
Optimization of Cancer Risk Assessment Models for PM2.5-Bound PAHs: Application in Jingzhong, Shanxi, China


Abstract
1. Introduction
2. Methods
2.1. Sample Collection
2.2. Extraction and Purification
2.3. Quantitative Analysis of PAHs
2.4. Quality Control and Quality Assurance
2.5. Cancer Risk Assessment
2.6. Statistical Analysis
3. Results and Discussion
3.1. Levels of PM2.5 and Their Bound PAHs
3.2. Selection of Models of Cancer Risk Assessment
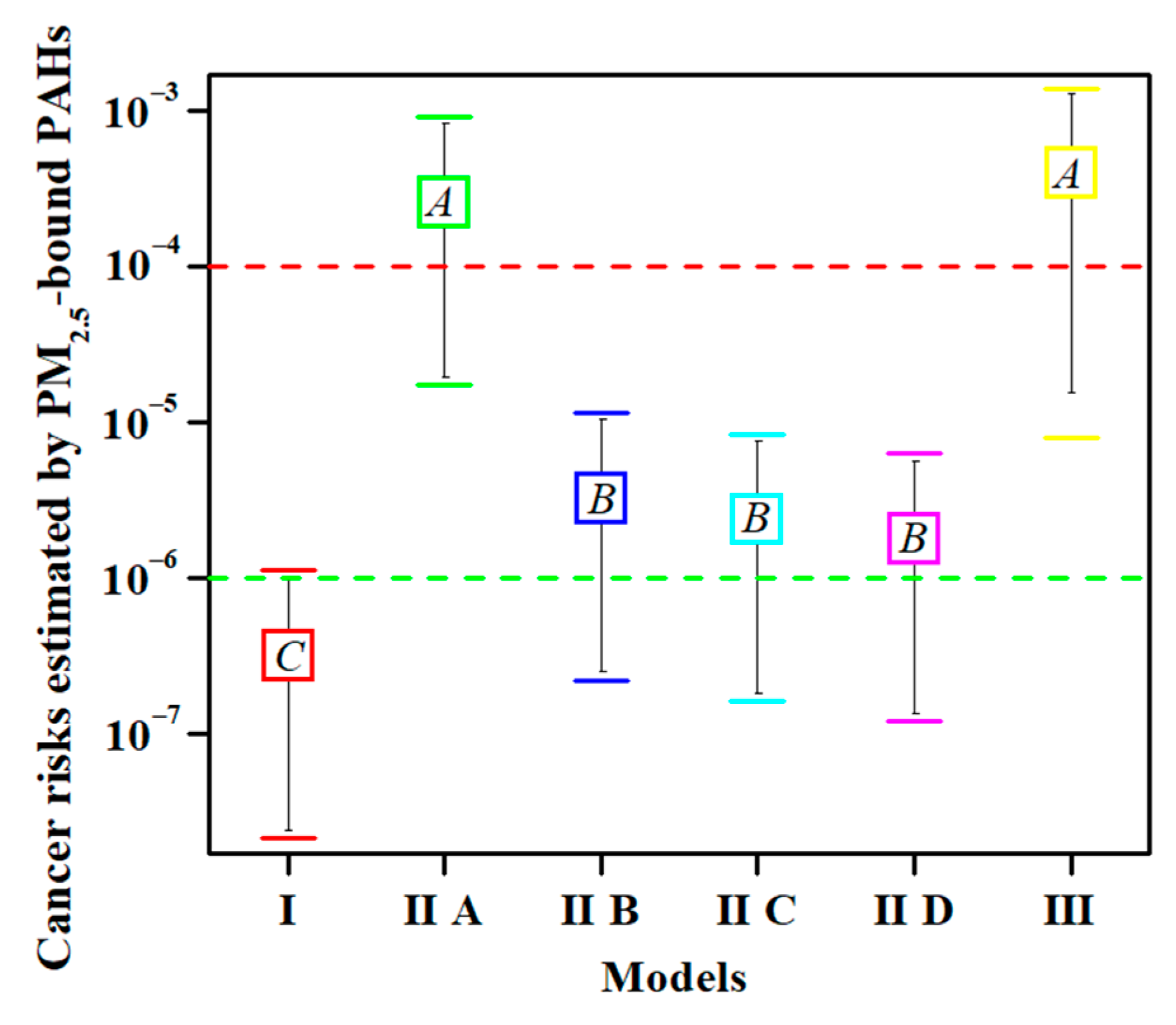
3.2.1. Statistical Differences among the Models of Cancer Risk Assessment
3.2.2. Advantages of Model I
3.2.3. Simple and Convenient Models IIB, IIC, and IID
3.2.4. Model IIA and Model III Overestimated Cancer Risk
3.3. Selection of Population Exposure Parameters in Model I
3.4. Limitations
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cohen, A.J.; Brauer, M.; Burnett, R.; Anderson, H.R.; Frostad, J.; Estep, K.; Balakrishnan, K.; Brunekreef, B.; Dandona, L.; Dandona, R.; et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: An analysis of data from the Global Burden of Diseases Study 2015. Lancet 2017, 389, 1907–1918. [Google Scholar] [CrossRef] [PubMed]
- Landrigan, P.J.; Fuller, R.; Acosta, N.J.R.; Adeyi, O.; Arnold, R.; Basu, N.; Balde, A.B.; Bertollini, R.; Bose-O’Reilly, S.; Boufford, J.I.; et al. The Lancet Commission on pollution and health. Lancet 2018, 391, 462–512. [Google Scholar] [CrossRef] [PubMed]
- Turner, M.C.; Krewski, D.; Diver, W.R.; Pope, C.A.; Burnett, R.T.; Jerrett, M.; Marshall, J.D.; Gapstur, S.M. Ambient air pollution and cancer mortality in the cancer prevention study II. Environ. Health Perspect. 2017, 125, 087013. [Google Scholar] [CrossRef] [PubMed]
- Yan, D.; Wu, S.; Zhou, S.; Tong, G.; Li, F.; Wang, Y.; Li, B. Characteristics, sources and health risk assessment of airborne particulate PAHs in Chinese cities: A review. Environ. Pollut. 2019, 248, 804–814. [Google Scholar] [CrossRef] [PubMed]
- Bai, X.; Tian, H.; Liu, X.; Wu, B.; Liu, S.; Hao, Y.; Luo, L.; Liu, W.; Zhao, S.; Lin, S. Spatial-temporal variation characteristics of air pollution and apportionment of contributions by different sources in Shanxi province of China. Atmos. Environ. 2021, 244, 117926. [Google Scholar] [CrossRef]
- Kim, K.H.; Jahan, S.A.; Kabir, E.; Brown, R. A review of airborne polycyclic aromatic hydrocarbons (PAHs) and their human health effects. Environ. Int. 2013, 60, 71–80. [Google Scholar] [CrossRef]
- Meng, Y.; Liu, X.; Lu, S.; Zhang, T.; Jin, B.; Wang, Q.; Tang, Z.; Liu, Y.; Guo, X.; Zhou, J. A review on occurrence and risk of polycyclic aromatic hydrocarbons (PAHs) in lakes of China. Sci. Total Environ. 2019, 651, 2497–2506. [Google Scholar] [CrossRef]
- Qi, H.; Chen, X.; Du, Y.-e.; Niu, X.; Guo, F.; Li, W. Cancer risk assessment of soils contaminated by polycyclic aromatic hydrocarbons in Shanxi, China. Ecotoxicol. Environ. Saf. 2019, 182, 109381. [Google Scholar] [CrossRef]
- Akhbarizadeh, R.; Dobaradaran, S.; Torkmahalleh, M.A.; Saeedi, R.; Aibaghi, R.; Ghasemi, F.F. Suspended fine particulate matter (PM2.5), microplastics (MPs), and polycyclic aromatic hydrocarbons (PAHs) in air: Their possible relationships and health implications. Environ. Res. 2021, 192, 110339. [Google Scholar] [CrossRef]
- Gong, X.S.; Shen, Z.X.; Zhang, Q.; Zeng, Y.L.; Sun, J.; Ho, S.S.H.; Le, Y.L.; Zhang, T.; Xu, H.M.; Cui, S.; et al. Characterization of polycyclic aromatic hydrocarbon (PAHs) source profiles in urban PM2.5 fugitive dust: A large-scale study for 20 Chinese cites. Sci. Total Environ. 2019, 687, 188–197. [Google Scholar] [CrossRef]
- Krumal, K.; Mikuska, P. Mass concentrations and lung cancer risk assessment of PAHs bound to PM1 aerosol in six industrial, urban and rural areas in the Czech Republic, Central Europe. Atmos. Pollut. Res. 2020, 11, 401–408. [Google Scholar] [CrossRef]
- Mehmood, T.; Zhu, T.L.; Ahmad, I.; Li, X.H. Ambient PM2.5 and PM10 bound PAHs in Islamabad, Pakistan: Concentration, source and health risk assessment. Chemosphere 2020, 257, 127187. [Google Scholar] [CrossRef]
- Ali-Taleshi, M.S.; Moeinaddini, M.; Bakhtiari, A.R.; Feiznia, S.; Squizzato, S.; Bourliva, A. A one-year monitoring of spatiotemporal variations of PM2.5-bound PAHs in Tehran, Iran: Source apportionment, local and regional sources origins and source-specific cancer risk assessment. Environ. Pollut. 2021, 274, 115883. [Google Scholar] [CrossRef]
- USEPA. Risk Assessment Guidance for Superfund: Volume I: Human Health Evaluation Manual (Part F, Supplemental Guidance for Inhalation Risk Assessment); EPA/540/R-070/002; U.S. Environmental Protection Agency: Washington, DC, USA, 2009.
- Ouyang, R.T.; Yang, S.D.; Xu, L.Y. Analysis and risk assessment of PM2.5-bound PAHs in a comparison of indoor and outdoor environments in a middle school: A case study in Beijing, China. Atmosphere 2020, 11, 904. [Google Scholar] [CrossRef]
- WHO (World Health Organization). Air Quality Guidelines for Europe, 2nd ed.; WHO Regional Office for Europe: Copenhagen, Denmark, 2000; Available online: https://www.euro.who.int/en/health-topics/environment-and-health/air-quality/publications/pre2009/air-quality-guidelines-for-europe (accessed on 22 August 2022).
- OEHHA. Air Toxics Hot Spots Program Risk Assessment Guidelines: The Air Toxics Hot Spots Program Guidance Manual for Preparation of Health Risk Assessments; Office of Environmental Health Hazard Assessment: Sacramento, CA, USA, 2003.
- Han, F.; Guo, H.; Hu, J.; Zhang, J.; Ying, Q.; Zhang, H. Sources and health risks of ambient polycyclic aromatic hydrocarbons in China. Sci. Total Environ. 2020, 698, 134229. [Google Scholar] [CrossRef]
- USEPA. IRIS (Integrated Risk Information System). Toxicological Review of Benzo[a]pyrene (Executive Summary); EPA/635/R-17/003Fc; Office of Research and Development, U.S. Environmental Protection Agency: Washington, DC, USA, 2017. [Google Scholar]
- Yabueng, N.; Wiriya, W.; Chantara, S. Influence of zero-burning policy and climate phenomena on ambient PM2.5 patterns and PAHs inhalation cancer risk during episodes of smoke haze in Northern Thailand. Atmos. Environ. 2020, 232, 117485. [Google Scholar] [CrossRef]
- MEPC (Ministry of Environmental Protection of China). Ambient Air and Stationary Source Emissions—Determination of Gas and Particle-Phase PAHs with Gas Chromatography/Mass Spectrometry (HJ 646-2013); China Environmental Science Press: Beijing, China, 2013. (In Chinese)
- USEPA. Exposure Factors Handbook 2011 Edition (Final Report); EPA/600/R-09/052F; Office of Emergency and Remedial Response, U.S. Environmental Protection Agency: Washington, DC, USA, 2011.
- Nisbet, I.C.T.; Lagoy, P.K. Toxic equivalency factors (TEFs) for polycyclic aromatic-hydrocarbons (PAHs). Regul. Toxicol. Pharmacol. 1992, 16, 290–300. [Google Scholar] [CrossRef]
- WHO (World Health Organization). WHO Global Air Quality Guidelines: Particulate Matter (PM2.5 and PM10), Ozone, Nitrogen Dioxide, Sulfur Dioxide and Carbon Monoxide: Executive Summary; WHO Regional Office for Europe: Copenhagen, Denmark, 2021; Available online: https://www.who.int/publications/i/item/9789240034433 (accessed on 25 August 2022).
- Zhang, Q.; Zheng, Y.; Tong, D.; Shao, M.; Wang, S.; Zhang, Y.; Xu, X.; Wang, J.; He, H.; Liu, W.; et al. Drivers of improved PM2.5 air quality in China from 2013 to 2017. Proc. Natl. Acad. Sci. USA 2019, 116, 24463–24469. [Google Scholar] [CrossRef]
- Li, Q.; Jiang, N.; Yu, X.; Dong, Z.; Duan, S.; Zhang, L.; Zhang, R. Sources and spatial distribution of PM2.5-bound polycyclic aromatic hydrocarbons in Zhengzhou in 2016. Atmos. Res. 2019, 216, 65–75. [Google Scholar] [CrossRef]
- Jia, J.; Deng, L.; Bi, C.; Jin, X.; Zeng, Y.; Chen, Z. Seasonal variations, gas-PM2. 5 partitioning and long-distance input of PM2.5-bound and gas-phase polycyclic aromatic hydrocarbons in Shanghai, China. Atmos. Environ. 2021, 252, 118335. [Google Scholar] [CrossRef]
- IARC (International Agency for Research on Cancer). Agents Classified by the IARC Monographs. 2021; Volumes 1–130. Available online: https://monographs.iarc.who.int/agents-classified-by-the-iarc/ (accessed on 20 August 2022).
- GB 3095-2012; Ambient Air Quality Standards. National Standards of the People’s Republic of China. China Environmental Press: Beijing, China, 2012. (In Chinese)
- WHO (World Health Organization). Principles for Evaluating Health Risks from Chemicals during Infancy and Early Childhood: The Need for a Special Approach [R]; World Health Organization, International Program on Chemical Safety: Geneva, Switzerland, 1986; Volume 59. [Google Scholar]
- Wang, S.B.; Ji, Y.Q.; Zhao, J.B.; Lin, Y.; Lin, Z. Source apportionment and toxicity assessment of PM2.5-bound PAHs in a typical iron-steel industry city in northeast China by PMF-ILCR. Sci. Total Environ. 2020, 713, 136428. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.L.; Morisaki, H.; Wei, Y.J.; Li, Z.G.; Yang, L.; Zhou, Q.Y.; Zhang, X.; Xing, W.L.; Hu, M.; Shima, M.; et al. PM2.5-bound polycyclic aromatic hydrocarbons and nitro-polycyclic aromatic hydrocarbons inside and outside a primary school classroom in Beijing: Concentration, composition, and inhalation cancer risk. Sci. Total Environ. 2020, 705, 135840. [Google Scholar] [CrossRef]
- Zeng, H.; Zhang, L.; Sun, F.Z.; Liu, J.J.; Fang, B.; Yang, W.Q.; Meng, C.Y.; Wang, M.M.; Wang, Q.; Hao, Y.L. Inhalation bioaccessibility, health risk assessment, and source appointment of ambient PM2.5-bound polycyclic aromatic hydrocarbons (PAHs) in Caofeidian, China. Environ. Sci. Pollut. R. 2021, 28, 47574–47587. [Google Scholar] [CrossRef] [PubMed]
- Shi, M.; Zhang, R.; Wang, Y.; Zhang, Y.; Zhang, Y. Health risk assessments of polycyclic aromatic hydrocarbons and chlorinated/brominated polycyclic aromatic hydrocarbons in urban air particles in a haze frequent area in China. Emerg. Contam. 2020, 6, 172–178. [Google Scholar] [CrossRef]
- Wang, G.Y.; Wang, Y.; Yin, W.J.; Xu, T.; Hu, C.; Cheng, J.; Hou, J.; He, Z.Y.; Yuan, J. Seasonal exposure to PM2.5-bound polycyclic aromatic hydrocarbons and estimated lifetime risk of cancer: A pilot study. Sci. Total Environ. 2020, 702, 135056. [Google Scholar] [CrossRef]
- Feng, B.H.; Li, L.J.; Xu, H.B.; Wang, T.; Wu, R.S.; Chen, J.; Zhang, Y.; Liu, S.; Ho, S.S.H.; Cao, J.J.; et al. PM2.5-bound polycyclic aromatic hydrocarbons (PAHs) in Beijing: Seasonal variations, sources, and risk assessment. J. Environ. Sci. 2019, 77, 11–19. [Google Scholar] [CrossRef]
- Gao, P.; Hu, J.; Song, J.; Chen, X.; Ou, C.Y.; Wang, H.; Sha, C.Y.; Hang, J.; Xing, B.S. Inhalation bioaccessibility of polycyclic aromatic hydrocarbons in heavy PM2.5 pollution days: Implications for public health risk assessment in northern China. Environ. Pollut. 2019, 255, 8. [Google Scholar] [CrossRef]
- Longoria-Rodriguez, F.E.; Gonzalez, L.T.; Mendoza, A.; Leyva-Porras, C.; Arizpe-Zapata, A.; Esneider-Alcala, M.; Acuna-Askar, K.; Gaspar-Ramirez, O.; Lopez-Ayala, O.; Alfaro-Barbosa, J.M.; et al. Environmental levels, sources, and cancer risk assessment of PAHs associated with PM2.5 and TSP in Monterrey metropolitan area. Arch. Environ. Contam. Toxicol. 2020, 78, 377–391. [Google Scholar] [CrossRef]
- Kermani, M.; Jafari, A.J.; Gholami, M.; Farzadkia, M.; Shahsavani, A.; Norzaee, S. Polycyclic aromatic hydrocarbons in PM2.5 atmospheric particles in Shiraz, a city in southwest Iran: Sources and risk assessment. Arabian J. Geosci. 2021, 14, 10. [Google Scholar] [CrossRef]
- Han, B.; You, Y.; Liu, Y.T.; Xu, J.; Zhou, J.; Zhang, J.F.; Niu, C.; Zhang, N.; He, F.; Ding, X.; et al. Inhalation cancer risk estimation of source-specific personal exposure for particulate matter-bound polycyclic aromatic hydrocarbons based on positive matrix factorization. Environ. Sci. Pollut. Res. 2019, 26, 10230–10239. [Google Scholar] [CrossRef]
- Zhang, M.; Li, Z.P.; Xu, M.; Yue, J.W.; Cai, Z.W.; Yung, K.K.L.; Li, R.J. Pollution characteristics, source apportionment and health risks assessment of fine particulate matter during a typical winter and summer time period in urban Taiyuan, China. Hum. Ecol. Risk Assess. 2019, 26, 2737–2750. [Google Scholar] [CrossRef]
- Sharma, D.; Jain, S. Carcinogenic risk from exposure to PM2.5 bound polycyclic aromatic hydrocarbons in rural settings. Ecotoxicol. Environ. Saf. 2020, 190, 10. [Google Scholar] [CrossRef]
- He, J.; Chen, W.Q.; China National Central. 2016 Chinese Tumor Registry Annual Report [M]; Tsinghua University Press: Beijing, China, 2017. (In Chinese) [Google Scholar]
- He, J.; Chen, W.Q.; China National Central. 2017 Chinese Tumor Registry Annual Report [M]; People’s Sanitary Publishing Press: Beijing, China, 2018. (In Chinese) [Google Scholar]
- He, J.; China National Central. 2018 Chinese Tumor Registry Annual Report [M]; People’s Sanitary Publishing Press: Beijing, China, 2019. (In Chinese) [Google Scholar]
- He, J.; Wei, W.Q.; China National Central. 2019 Chinese Tumor Registry Annual Report [M]; People’s Sanitary Publishing Press: Beijing, China, 2021. (In Chinese) [Google Scholar]
- Chen, W.; Xia, C.; Zheng, R.; Zhou, M.; Lin, C.; Zeng, H.; Zhang, S.; Wang, L.; Yang, Z.; Sun, K.; et al. Disparities by province, age, and sex in site-specific cancer burden attributable to 23 potentially modifiable risk factors in China: A comparative risk assessment. Lancet Glob. Health 2019, 7, 257–269. [Google Scholar] [CrossRef]
- Wang, J.; Jiang, Y.; Liang, H.; Li, P.; Xiao, H.; Ji, J.; Xiang, W.; Shi, J.; Fan, Y.; Li, L. Attributable causes of cancer in China. Ann. Oncol. 2012, 23, 2983–2989. [Google Scholar] [CrossRef]
- Zhang, Y.; Zheng, H.; Zhang, L.; Zhang, Z.Z.; Xing, X.L.; Qi, S.H. Fine particle-bound polycyclic aromatic hydrocarbons (PAHs) at an urban site of Wuhan, central China: Characteristics, potential sources and cancer risks apportionment. Environ. Pollut. 2019, 246, 319–327. [Google Scholar] [CrossRef]
- Shi, M.M.; Hu, T.P.; Mao, Y.; Cheng, C.; Liu, W.J.; Tian, Q.; Chen, Z.L.; Xing, X.L.; Qi, S.H. Polycyclic aromatic hydrocarbons in atmospheric PM2.5 during winter haze in Huang-gang, central China: Characteristics, sources and health risk assessment. Aerosol Air Qual. Res. 2021, 21, 19. [Google Scholar] [CrossRef]
- Xu, A.; Mao, Y.; Su, Y.; Shi, M.; Qi, S. Characterization, sources and risk assessment of PM2.5-bound polycyclic aromatic hydrocarbons (PAHs) in Huanggang city, central China. Atmos. Environ. 2021, 252, 118296. [Google Scholar] [CrossRef]
- Ma, W.-L.; Zhu, F.-J.; Liu, L.-Y.; Jia, H.-L.; Yang, M.; Li, Y.-F. PAHs in Chinese atmosphere Part II: Health risk assessment. Ecotoxicol. Environ. Saf. 2020, 200, 110774. [Google Scholar] [CrossRef]
- Xing, X.L.; Chen, Z.L.; Tian, Q.; Mao, Y.; Liu, W.J.; Shi, M.M.; Cheng, C.; Hu, T.P.; Zhu, G.H.; Li, Y.; et al. Characterization and source identification of PM2.5-bound polycyclic aromatic hydrocarbons in urban, suburban, and rural ambient air, central China during summer harvest. Ecotoxicol. Environ. Saf. 2020, 191, 10. [Google Scholar] [CrossRef]
- Wang, W.; Lin, Y.; Yang, H.; Ling, W.; Liu, L.; Zhang, W.; Lu, D.; Liu, Q.; Jiang, G. Internal exposure and distribution of airborne fine particles in the human body: Methodology, current understandings, and research needs. Environ. Sci. Technol. 2022, 56, 6857–6869. [Google Scholar] [CrossRef]
- Drew, R.; Frangos, J.; Hagen, T. Australian Exposure Factor Guidance; Toxikos Pty Ltd.: Melbourne, Australia, 2010. [Google Scholar]
- NIAIST (National Institute of Advanced Industrial Science and Technology). Japanese Exposure Factors Handbook [S], Japan. 2007. Available online: https://unit.aist.go.jp/riss/crm/exposurefactors/english_summary.html (accessed on 26 August 2022).
- Jang, J.; Jo, S.; Kim, S.; Cheong, H. Korean Exposure Factors Handbook [S]; Ministry of Environment: Seoul, Republic of Korea, 2007. [Google Scholar]
- MEPC (Ministry of Environmental Protection of China). Manual of Chinese Population Exposure Parameters (Children’s Volume 6–17 Years Old) [M]; China Environmental Press: Beijing, China, 2016. (In Chinese)
- MEPC (Ministry of Environmental Protection of China). Manual of Chinese Population Exposure Parameters (Adult Volume) [M]; China Environmental Press: Beijing, China, 2013. (In Chinese)
- Liu, Z.; Gao, W.; Yu, Y.; Hu, B.; Xin, J.; Sun, Y.; Wang, L.; Wang, G.; Bi, X.; Zhang, G. Characteristics of PM2.5 mass concentrations and chemical species in urban and background areas of China: Emerging results from the CARE-China network. Atmos. Chem. Phys. 2018, 18, 8849–8871. [Google Scholar] [CrossRef]
- Pushparajah, D.S.; Plant, K.E.; Plant, N.J.; Ioannides, C. Synergistic and antagonistic interactions of binary mixtures of polycyclic aromatic hydrocarbons in the upregulation of CYP1 activity and mRNA levels in precision-cut rat liver slices. Environ. Toxicol. 2017, 32, 764–775. [Google Scholar] [CrossRef] [PubMed]
- Pushparajah, D.S.; Ioannides, C. Antagonistic and synergistic interactions during the binding of binary mixtures of polycyclic aromatic hydrocarbons to the aryl hydrocarbon receptor. Toxicol. In Vitro 2018, 50, 54–61. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Model | Parameter | Abbreviation | Unit | Adult |
|---|---|---|---|---|
| I [22] | Carcinogenic slope factor | CSF | [mg/(kg·d)] −1 | 3.14 |
| Inhalation rate | IR | m3·d−1 | 20 | |
| Exposure time | ET | h·d−1 | 4 | |
| Exposure frequency | EF | d·a−1 | 350 | |
| Exposure duration | ED | a | 52 | |
| Conversion factor | CF | — | 10−6 | |
| Body weight | BW | kg | 70 | |
| Averaging time | AT | a | 70 | |
| IIA [16] | Inhalation unit risk | IURBaP | (ng·m−3)−1 | 8.7 × 10−5 |
| IIB [17] | 1.1 × 10−6 | |||
| IIC [18] | 8.0 × 10−7 | |||
| IID [19] | 6.0 × 10−7 | |||
| III [10] | Carcinogenic slope factor (inhalation) | CSF(inh) | [mg/(kg·d)] −1 | 3.85 |
| Exposure duration | ED | a | 24 | |
| Particulate emission factor | PEF | m3·kg−1 | 1.36 × 109 | |
| Exposed skin area | SA | cm2 | 5800 | |
| Skin attachment factor | AF | mg·cm−2·d | 0.07 | |
| Skin adherence factor | ABS | — | 0.13 | |
| Carcinogenic slope factor | CSF(dem) | [mg/(kg·d)] −1 | 25 | |
| Ingestion rate | IR(soil) | mg·d−1 | 100 | |
| Cancer slope factor (ingestion) | CSF(ing) | [mg/(kg·d)] −1 | 7.3 |
| Ring | Class a | TEF b | Detection Rate/% | Min | Median | Max | Mean | SD | ||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Naphthalene | 2 | 2B | 0.001 | 97 | 0.13 c | 3.25 | 70.7 | 6.91 | 12.2 |
| 2 | Acenaphthylene | 3 | — d | 0.001 | 82 | 0.04 | 0.72 | 16.1 | 1.58 | 3.02 |
| 3 | Fluorene | 3 | 3 | 0.001 | 62 | 0.07 | 0.34 | 1.51 | 0.48 | 0.38 |
| 4 | Acenaphthene | 3 | 3 | 0.001 | 74 | 0.06 | 1.63 | 14.4 | 2.98 | 3.56 |
| 5 | Phenanthrene | 3 | 3 | 0.001 | 59 | 0.06 | 0.71 | 6.13 | 1.56 | 1.71 |
| 6 | Anthracene | 3 | 3 | 0.01 | 85 | 0.09 | 3.81 | 19.5 | 6.28 | 6.17 |
| 7 | Fluoranthene | 4 | 3 | 0.001 | 97 | 0.09 | 3.99 | 21.4 | 6.11 | 6.33 |
| 8 | Pyrene | 4 | 3 | 0.001 | 100 | 0.06 | 4.33 | 20.7 | 5.83 | 6.14 |
| 9 | Benz[a]anthracene | 4 | 2B | 0.1 | 100 | 0.12 | 0.42 | 5.48 | 0.98 | 1.25 |
| 10 | Chrysene | 4 | 2B | 0.01 | 77 | 0.07 | 4.48 | 21.8 | 6.02 | 5.90 |
| 11 | Benzo[b]fluoranthene | 5 | 2B | 0.1 | 77 | 0.08 | 2.89 | 24.7 | 4.84 | 5.92 |
| 12 | Benzo[k]fluoranthene | 5 | 2B | 0.1 | 74 | 0.05 | 1.72 | 10.3 | 2.41 | 2.33 |
| 13 | Benzo[a]pyrene | 5 | 1 | 1.0 | 85 | 0.06 | 0.39 | 2.19 | 0.53 | 0.52 |
| 14 | Dibenzo[a,h]anthracene | 5 | 2A | 1.0 | 100 | 0.06 | 0.68 | 4.73 | 1.13 | 1.23 |
| 15 | Indeno[1,2,3-c,d]pyrene | 6 | 2B | 0.1 | 100 | 0.08 | 3.06 | 33.4 | 6.06 | 7.78 |
| 16 | Benzo[g,h,i]perylene | 6 | 3 | 0.01 | 64 | 0.07 | 1.00 | 5.32 | 1.65 | 1.48 |
| ∑PAH | 1.92 | 38.4 | 154 | 48.1 | 38.0 | |||||
| BaPeq (ng·m−3) | 0.16 | 2.59 | 11.1 | 2.85 | 2.62 | |||||
| BaPeq (mg·kg−1) | 0.74 | 20.4 | 138 | 31.9 | 34.6 | |||||
| PM2.5 (μg·m−3) | 21.4 | 61.1 | 183 | 70.2 | 33.1 |
| Model | Country | Area | Year | Samples | BaPeq (ng·m−3) | ILCR (×10−4) | Reference |
|---|---|---|---|---|---|---|---|
| Czech | Brno | 2017 | 15 | 3.47 (0.495–11.7) | 3.02 (0.43–10.16) | [11] | |
| Pakistan | Islamabad | 2017 | 160 | 4.45 | 6.39 | [12] | |
| Iran | Shahrrey, Tehran | 2019 | 45 | 7.09 ± 5.82 | 6.17 | [13] | |
| IIA | Thailand | Nan Province | 2018 | 40 | 1.54 ± 1.36 | 1.34 | [20] |
| China | Wuhan | 2015 | 115 | 3.48 ± 3.53 | 3.03 | [49] | |
| China | Jinzhong, Shanxi | 2021 | 39 | 2.96 ± 2.68 | 2.57 ± 2.33 | This study | |
| China | North China | 2015 | 90 | 2.94 | 1.99 | [10] | |
| III | China | Huanggang | 2018 | 28 | 4.08 ± 2.22 | 0.37 ± 0.20 | [50] |
| China | Jinzhong, Shanxi | 2021 | 39 | 2.85 ± 2.62 | 3.92 ± 3.98 | This study |
| CSF | IR | ET | EF | ED | BW | AT | CF | ADD (×10−8) | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Adults | 3.14 | 20 | 4 | 350 | 52 | 70 | 70 | 10−6 | 10.7 | |
| USEPA | Females | 3.14 | 14.7 | 4 | 350 | 52 | 73 | 80.4 | 10−6 | 6.54 |
| [22] | Males | 3.14 | 14.7 | 4 | 350 | 52 | 86 | 75.4 | 10−6 | 5.92 |
| Children | 3.14 | 10 | 4 | 350 | 6 | 15 | 70 | 10−6 | 2.87 | |
| Australia [55] | Adults | 3.14 | 16 | 3 | 350 | 52 | 75 | 81.5 | 10−6 | 5.12 |
| Japan [56] | Adults | 3.14 | 17.3 | 1.2 | 350 | 52 | 58.4 | 81.2 | 10−6 | 2.86 |
| Korea | Adults | 3.14 | 14.3 | 1.3 | 350 | 52 | 62.8 | 78.6 | 10−6 | 2.46 |
| [57] | Females | 3.14 | 12.8 | 1.3 | 350 | 52 | 56.4 | 81.9 | 10−6 | 2.35 |
| Males | 3.14 | 15.7 | 1.3 | 350 | 52 | 69.2 | 75.1 | 10−6 | 2.56 | |
| Adults | 3.14 | 15.7 | 3.68 | 350 | 52 | 60.6 | 74.8 | 10−6 | 8.32 | |
| China | Females | 3.14 | 14.5 | 3.48 | 350 | 52 | 56.8 | 77.4 | 10−6 | 7.49 |
| [58,59] | Males | 3.14 | 18 | 3.93 | 350 | 52 | 65 | 72.4 | 10−6 | 9.81 |
| Children (6–9) | 3.14 | 10.1 | 1.73 | 350 | 6 | 26.5 | 74.8 | 10−6 | 0.66 | |
| Children (9–12) | 3.14 | 13.2 | 1.77 | 350 | 9 | 36.8 | 74.8 | 10−6 | 0.96 | |
| Children (12–15) | 3.14 | 13.5 | 1.7 | 350 | 12 | 47.3 | 74.8 | 10−6 | 0.98 | |
| Children (15–18) | 3.14 | 14 | 1.3 | 350 | 15 | 54.8 | 74.8 | 10−6 | 1.03 |
| Country | Population | Mean ± SD | p < 0.05 |
|---|---|---|---|
| Adults | (3.15 ± 2.86) × 10−7 | A | |
| USA | Females | (1.93 ± 1.75) × 10−7 | AB |
| Males | (1.75 ± 1.59) × 10−7 | AB | |
| Australia | Adults | (1.51 ± 1.37) × 10−7 | AB |
| Japan | Adults | (8.44 ± 7.66) × 10−8 | B |
| Adults | (7.26 ± 6.59) × 10−8 | B | |
| Korea | Females | (6.95 ± 6.30) × 10−8 | B |
| Males | (7.57 ± 6.87) × 10−8 | B | |
| Adults | (2.46 ± 2.23) × 10−7 | A | |
| China | Females | (2.21 ± 2.01) × 10−7 | A |
| Males | (2.90 ± 2.63) × 10−7 | A |
| Country | Population | Mean ± SD | p < 0.01 |
|---|---|---|---|
| USA | Adults | (3.15 ± 2.86) × 10−7 | Aa |
| Children | (8.48 ± 7.69) × 10−8 | B | |
| Adults | (2.46 ± 2.23) × 10−7 | A | |
| China | Children (6–9) | (1.96 ± 1.78) × 10−8 | C |
| Children (9–12) | (2.83 ± 2.57) × 10−8 | C | |
| Children (12–15) | (2.89 ± 2.62) × 10−8 | C | |
| Children (15–18) | (3.04 ± 2.76) × 10−8 | C |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qi, H.; Liu, Y.; Li, L.; Zhao, B. Optimization of Cancer Risk Assessment Models for PM2.5-Bound PAHs: Application in Jingzhong, Shanxi, China. Toxics 2022, 10, 761. https://doi.org/10.3390/toxics10120761
Qi H, Liu Y, Li L, Zhao B. Optimization of Cancer Risk Assessment Models for PM2.5-Bound PAHs: Application in Jingzhong, Shanxi, China. Toxics. 2022; 10(12):761. https://doi.org/10.3390/toxics10120761
Chicago/Turabian StyleQi, Hongxue, Ying Liu, Lihong Li, and Bingqing Zhao. 2022. "Optimization of Cancer Risk Assessment Models for PM2.5-Bound PAHs: Application in Jingzhong, Shanxi, China" Toxics 10, no. 12: 761. https://doi.org/10.3390/toxics10120761
APA StyleQi, H., Liu, Y., Li, L., & Zhao, B. (2022). Optimization of Cancer Risk Assessment Models for PM2.5-Bound PAHs: Application in Jingzhong, Shanxi, China. Toxics, 10(12), 761. https://doi.org/10.3390/toxics10120761