4.1. Overview of Personal Exposure and Pollutant Uptake
Air quality in Dublin has improved significantly over the last 30 years and compared to the mean personal exposure of the study population, the average ambient outdoor PM
10 concentration during the sampling campaign was recorded as just 13 µg/m
3 at a fixed site monitor in Dublin City. Personal exposure studies of PM
10 and PM
2.5 in a number of other cities have found much higher concentrations [
10,
18] but such studies have been conducted in regions that are subject to greater ambient concentrations of PM. Improvements in air quality in this jurisdiction have been brought about by a number of measures including a ban on certain forms of coal combustion in major cities [
19], a number of EU directives limiting ambient concentrations and improving emissions standards, licensing of point emissions sources, taxation on fuels and carbon, tobacco control measures
etc. In addition, the geographic location of Ireland in North West Europe, with a prevailing wind travelling across the Atlantic Ocean results in little trans-boundary air pollution contributions to urban air quality in Dublin.
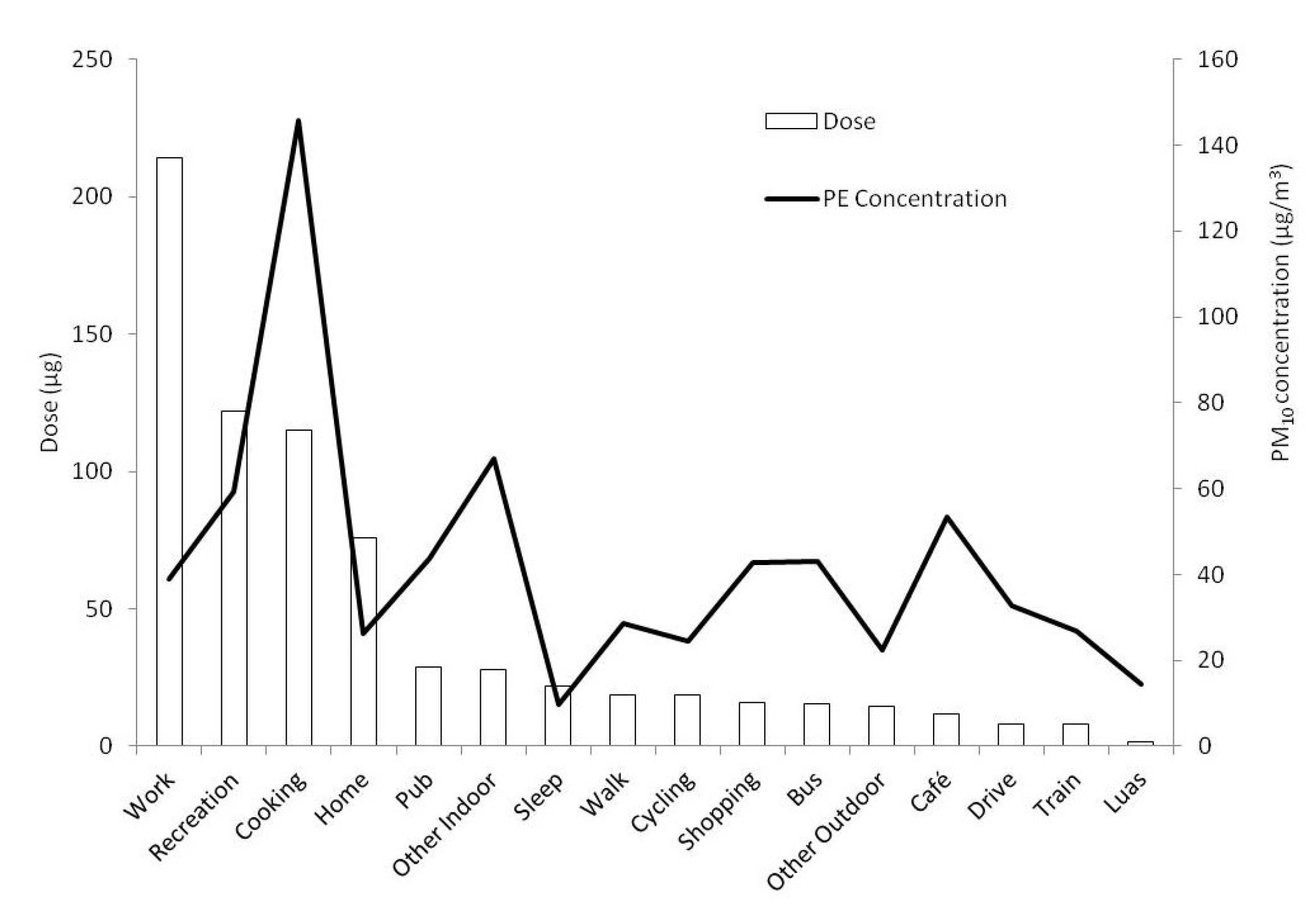
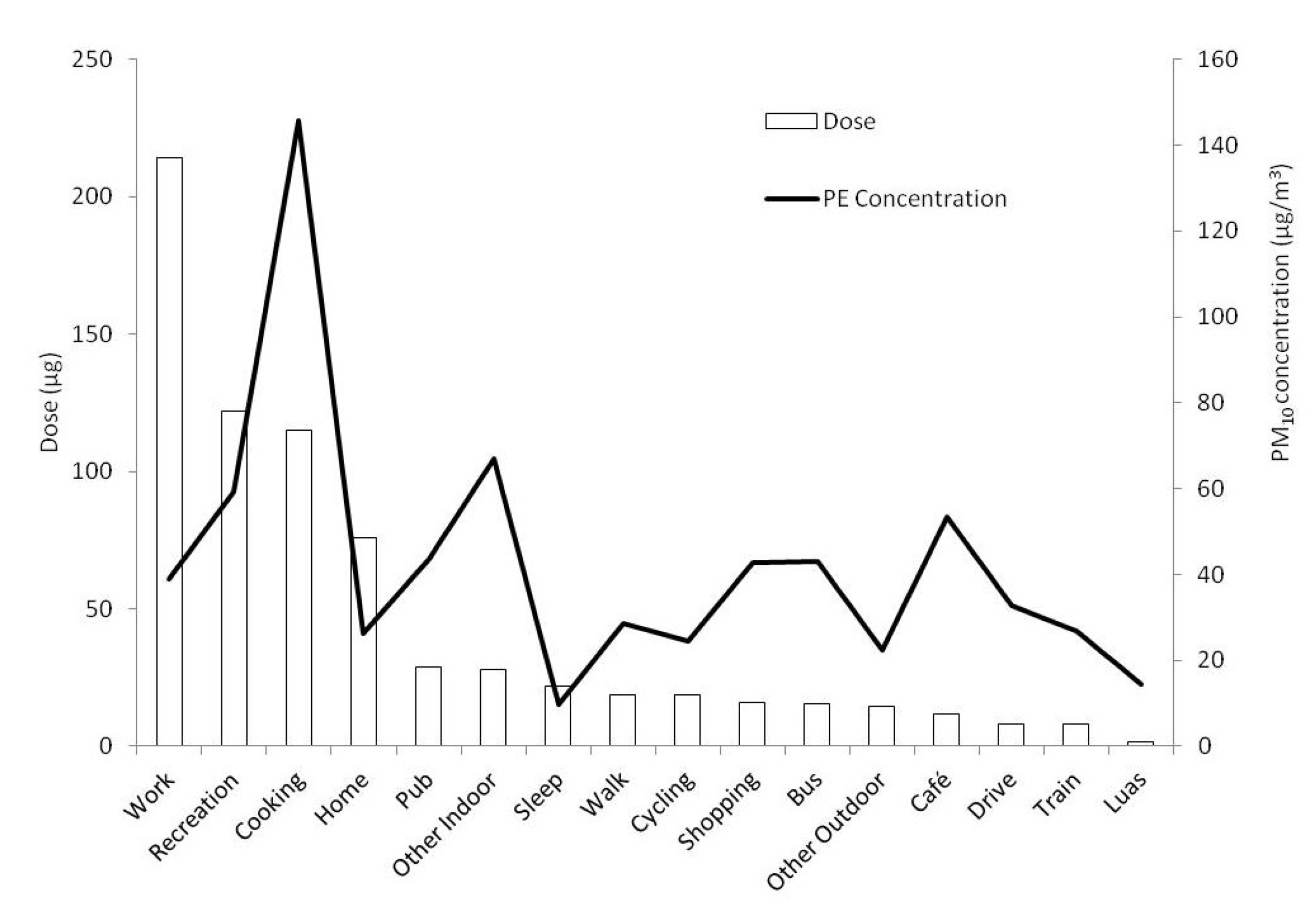
The largest uptake of PM10 among subjects was found to be in the office working environment, which had a mean uptake of 214.2 µg. This was followed by recreation or sport (122.0 µg) and cooking (115.2 µg). The mean uptake while each subject was classified as active at home was 75.9 µg. The mean uptake that subjects absorbed while sleeping fell to 22.9 µg. The commuting modes of subjects were observed to have some of the lowest mean uptake of all microenvironments for the study population.
Exposure and uptake of pollutants in the workplace was a common factor in all samples and clearly a key area through which improvements in health impact could be achieved using control measures. Sport and recreation activities were less common among the study population but were nonetheless surprisingly elevated in terms of both exposure and uptake. The majority of these activities were incidences of subjects attending a gym or playing indoor sports, and as such this is an area requiring further research into the reasons behind high exposure levels at a number of separate sports facilities in the city.
Cooking was also not universally undertaken across the sampling campaign with approximately 50% of sampling days including one or more cooking event. As the third highest source of pollutant uptake cooking activities were also a key determinant in overall exposure and uptake of PM10. A number of cooking events resulted in very high concentrations of particles being measured. Variations in these concentrations were present depending on cooking type and duration as well as ventilation conditions. However it was impractical to accurately determine the ventilation parameters for each cooking event during this study and it was also difficult to separate the impact of differing types of cooking as these were often carried out in combination (e.g., boiling and frying, etc.). Increased awareness among the public of the benefits of adequate ventilation during cooking on their environmental health would be an obvious step in reducing this component of exposure.
It is the view of the authors that there is limited awareness among the public or among policy makers of the relative importance of differing sources or air pollution for a large group of the population such as office workers. There is significant awareness and policy attention on the transport sector, but relative to cooking or the workplace this was not found to be an important microenvironment in the current study. However, it should be noted that the numerous types of air pollution emitted from transport sources such as VOCs, NOx, etc. may not be as prevalent in cooking emissions (i.e., the results and findings of this study are limited to particulate matter).
It is also worth highlighting that just under 50% of subjects did not cook and presumably either dined outside the home or ordered takeaway food. For numerous reasons relating to healthy diet, eating out and takeaway food are often highlighted for their negative health impacts, however as found here through the act of not cooking, subjects were not exposed to the third highest source of pollutant uptake found in this study.
4.2. Indoor Air Quality
The majority of the time was spent indoors by subject and this was predominantly in the subject’s residence. Time spent there was split almost two thirds in favour of the activity of sleeping, with one third of the time whereby the subject was active in the home. The activity of sleeping had a relatively low mean personal exposure concentration (10 µg/m3), and this was partially as a result of lack of activity in the residence. In contrast, the personal exposure concentrations when each individual was active at home were far greater. In addition to the home microenvironment, a large proportion of the study population’s day was also spent at work. Other microenvironments such as commuting, shopping, recreation etc. were responsible for only small portions of the daily routine of the study population. The mean occupational exposure (39 µg/m3) for the office workers in this study was found to be higher than the overall 24 hour mean personal exposure. This microenvironment played a key role in the day to day personal exposure concentrations of individuals as 30% of every weekday was found to be spent in work on average by the study subjects.
These findings highlight the importance of indoor air quality on the overall impacts of air pollution on the health of a typical office worker. Office workers in this study lived predominantly outside of the city centre while they worked in offices located in the city centre. This was also reflected in the fact that in-home concentrations were typically lower than at work. The control of air pollution in the workplace in Ireland has seen some improvement in recent years with the introductions of ban on smoking for example. This was evident in the elevated in-home concentrations found in the houses of smokers including the activity of sleeping in contrast to their workplace exposure concentration.
The extension of indoor air pollution control policy to the monitoring of air quality in the workplace and the enforcement of air quality standards indoors would bring about significant improvements in population health. The mean outdoor PM10 concentration recorded by the local authorities during the sampling period of 13 µg/m3 was less than half of the population’s mean personal exposure and was at a level which was of no cause for concern. However this clearly underestimated the exposure of a significant proportion of the population and the control of air quality in such locations does not directly target equivalent reductions in personal exposure. As outlined in the most recent European Directive for air quality (CAFÉ 2008/50/EC) national exposure reductions targets must be achieved for PM2.5 of 0%–20% depending on 2010 levels. The results of this investigation clearly demonstrate in which areas the most significant gains in personal exposure reduction can be achieved.
4.3. Transport Microenvironments and Commuting
The highest PM10 concentrations were found while travelling by bus (43 µg/m3), while travel by tram had the lowest personal exposure associated with it (14 µg/m3). However in the context of the overall daily average personal exposure these contributed only a small fraction. Significant research efforts have focused on personal exposure in the transport microenvironment, particularly during commuting. However, certainly in the case of Dublin, where air quality is generally good, exposure during transport activities was insignificant in comparison to the contribution of indoor air quality in the workplace and at home to overall daily exposure.
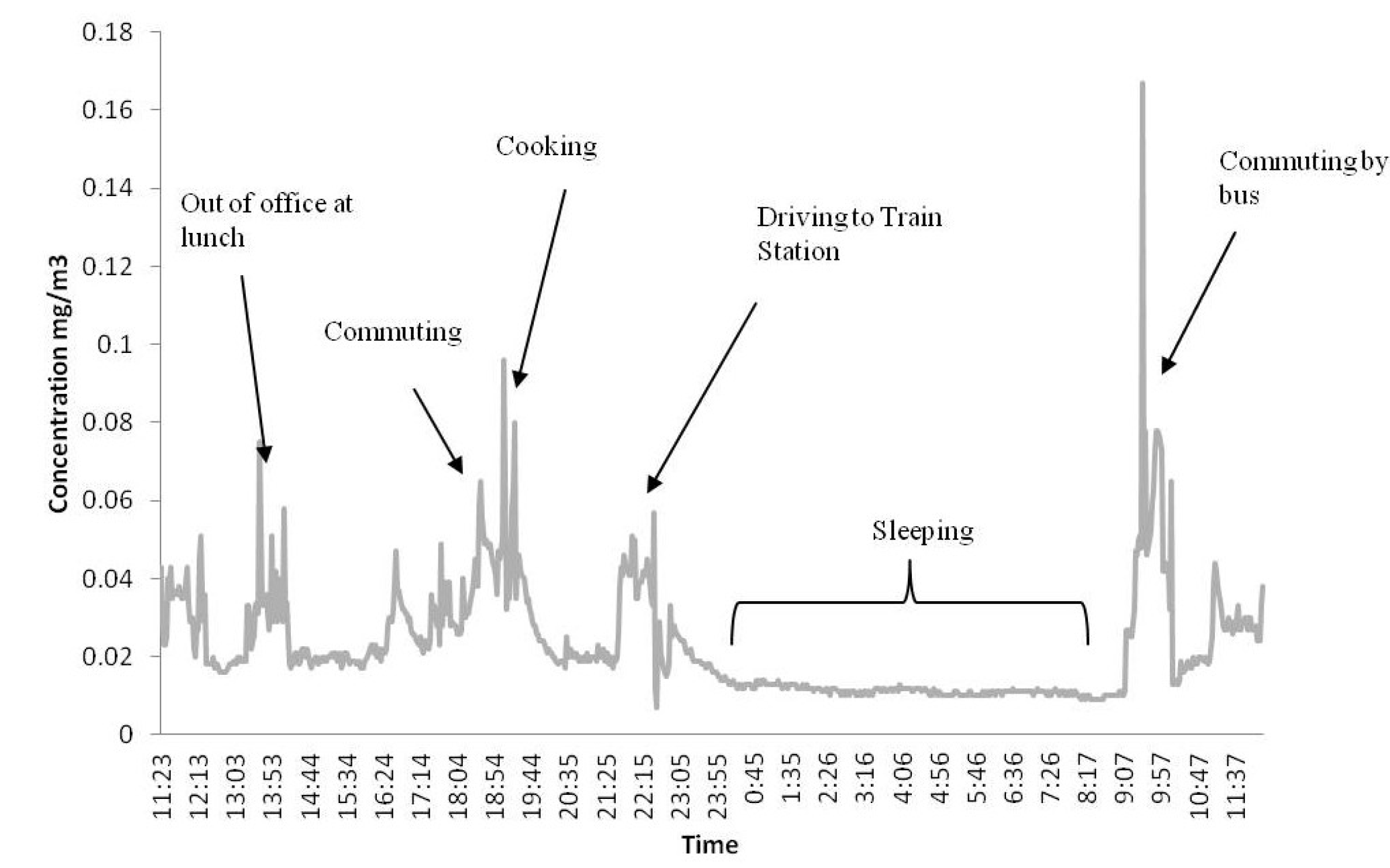
Michaels and Kleinman [
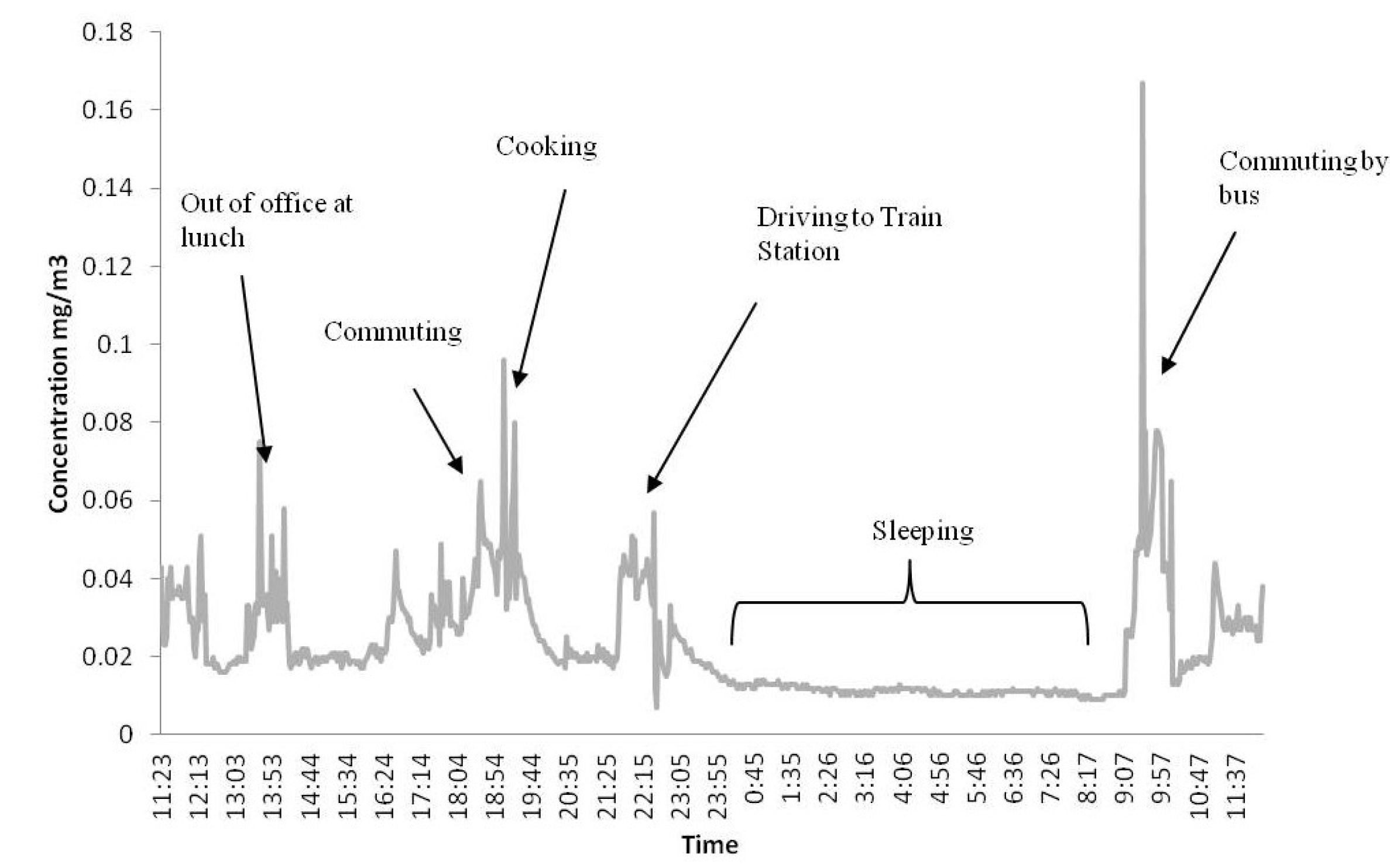
7] highlighted the significance of brief excursions in microenvironments with high 1-hour peak concentrations of particulate matter on the health of human and animal receptors. In this investigation such high peaks were predominantly found in the home associated with cooking or smoking as opposed to in outdoor transport microenvironments. In addition, much of the air quality legislation in place today and the monitoring of compliance focus on the outdoor environment. Given that over 90% of time was spent indoors by typical office workers in this study, it is clear that indoor air quality is the key factor influencing exposure and health impact among this population sub-group. Such findings highlight further the need for policy development in the area of indoor air quality to improve human health.
However it is also important to highlight that this does not suggest that transport emissions in Dublin had little impact on the environment or the public. The key contribution of transport emissions in this study was their likely elevation of urban background concentrations in general and their infiltration into city centre office buildings where workers spent significant amounts of time breathing elevated levels of pollutants. Previous investigations have shown that 50%–80% of particulate air pollution in buildings originated from external sources [
20]. As such it is too early to conclude that outdoor air pollution plays a minor role in the total uptake of particulate pollution among this population. Further work is needed to characterise the source of indoor air pollution (
i.e., indoor or outdoor sources).
4.4. Comparison of Personal Exposure and Uptake
Some of the microenvironments which were highlighted in
Section 3.1 as having the largest mean personal PM
10 concentrations associated with them, in fact contributed relatively little to the 24 hour uptake of subjects. This was particularly apparent in the case of the category “other indoor” along with cafés and restaurants. The impact of highest exposure category, cooking, was also shown to be lower when breathing rates and exposure duration were accounted for.
The activity category of “other indoor” was found to have a relatively high mean PM10 concentration (67 µg/m3) during the measurement campaign. However, due to the relatively infrequent and short amount of time spent in some of these microenvironments, the actual population uptake over 24 h was low (27.8 µg). A similar situation was seen with cafés and restaurants.
The uptake for the subjects while at work and active at home were, as expected, both large contributors to the 24 hour total uptake of subjects. This was due to the majority of each 24 hour sampling day being spent in either location. However, the greater activity levels while at work (40% sitting and 60% light exercise) amplified the difference in uptake even though the personal concentration population average was just 13 µg/m3 greater than “active at home”. For example, the uptake while at work (214.2 µg) was over 280% greater than that in the home (75.9 µg) on average, compared with the 49% difference between the two exposure concentrations.
The importance of considering both exposure and uptake of pollutants is clearly demonstrated here, however it is worth noting that the HRT models predictions of uptake took account of particle size, particle physics, the exhalation of particles, variations in physiology of subjects (sex, weight, height,
etc.), duration of exposure,
etc. As such the result of this model provide a more realistic estimate of air quality health impacts than the ‘inhaled dose technique’ used in a number of other studies e.g. [
5].
4.5. Transferability of Results
The transferability and limitations of the results of the current study are worth highlighting. Emphasis has been given to the importance of indoor air quality on the likely health impact of air pollution on office workers, particularly in the workplace. Clearly this may differ for those with differing workplace environments or those who are retired/unemployed etc. Exposure in predominantly outdoor or industrial settings is likely to differ from those found in the present study.
The transferability of the results of the present study to other locations is also worth noting. As mentioned, air quality in Dublin is generally quite good and perhaps the contribution of commuting may be more significant in cities with greater air quality problems. Branis and Kolomazikova [
10] performed a similar long term exposure assessment exercise using real time monitoring of one subject in the Czech Republic. Concentrations of PM
2.5 measured in various microenvironments during this study were typically higher than those found here for PM
10. However the relative importance of each microenvironment was similar. Furthermore the findings here in relation to PM
10 on the importance of the transport microenvironment do not necessarily translate to exposure to other traffic related pollutants e.g., NO
x, PM
2.5, VOCs,
etc.
The authors would like to thank the Environmental Protection Agency (STRIVE programme) for funding this research.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}