Factors Underlying Food Choice Motives in a Brazilian Sample: The Association with Socioeconomic Factors and Risk Perceptions about Chronic Diseases

 ,
,  ,
, 

Abstract
1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Evaluation of Food Choices
2.3. Evaluation of Risk and Control Perceptions
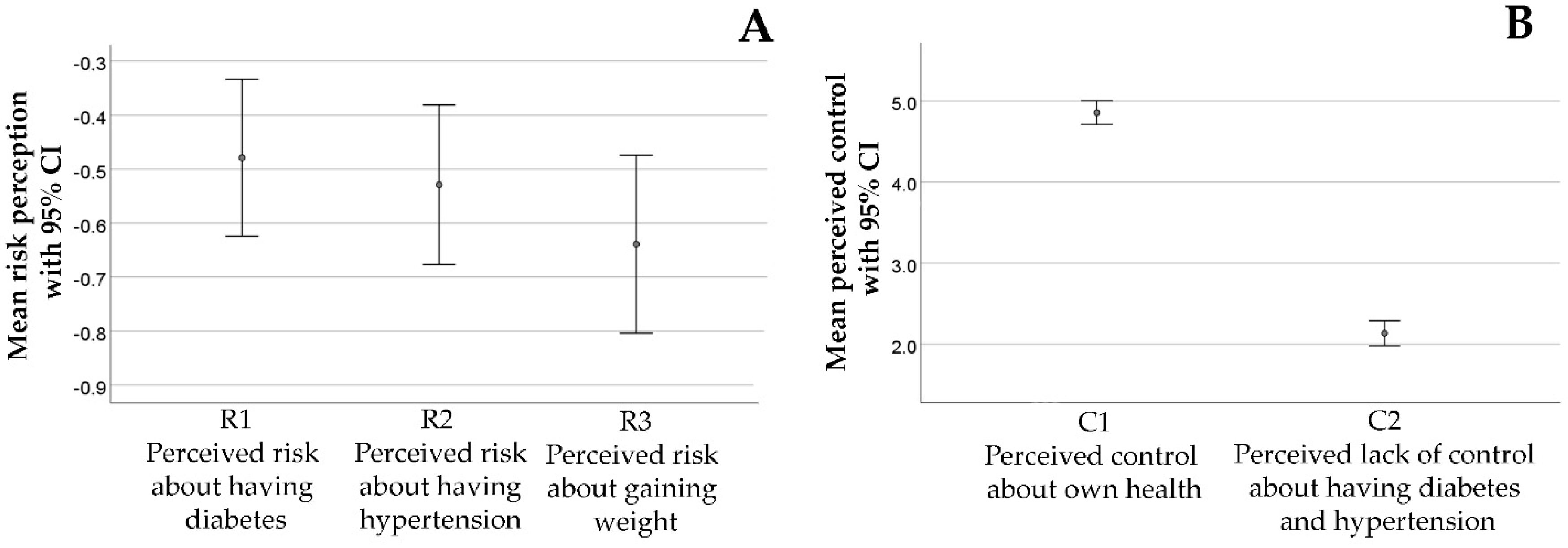
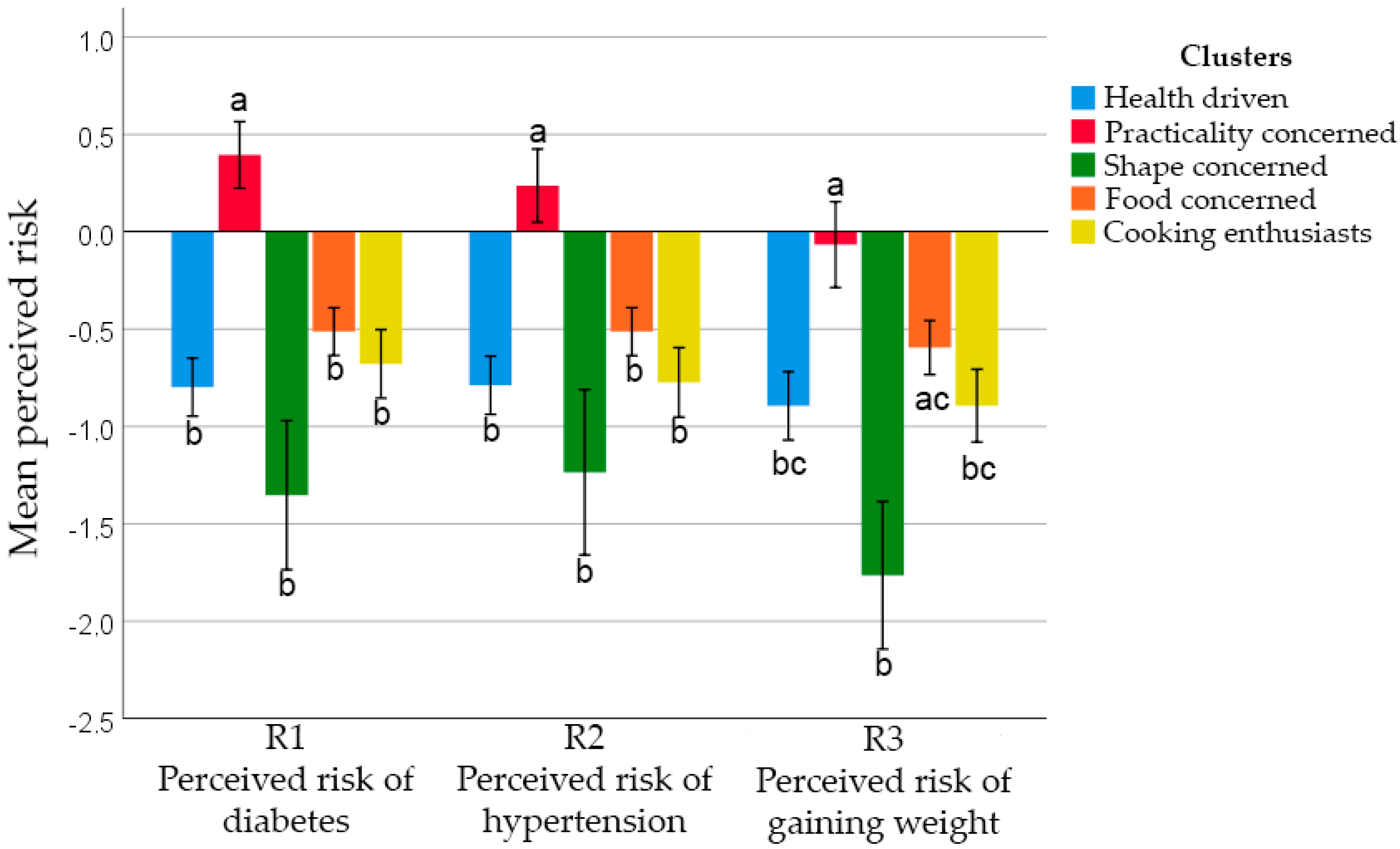
- R1—What is the chance of you developing diabetes, maintaining your current lifestyle?/Qual a chance de você desenvolver diabetes, mantendo seu estilo de vida atual?
- R2—What is the chance of you developing hypertension, maintaining your current lifestyle?/Qual a chance de você desenvolver hipertensão, mantendo seu estilo de vida atual?
- R3—What is the chance that you will gain 3 to 10 kg in the next 12 months, maintaining your current lifestyle?/Qual a chance de você engordar 3 a 10 kg nos próximos 12 meses, mantendo seus hábitos atuais?
- C1—“I believe I have control over my health”/Eu acredito que tenho controle sobre a minha saúde.
- C2—“There is not much I can do to prevent the development of diseases such as diabetes and hypertension”/Não existe muito o que eu possa fazer para evitar o desenvolvimento de doenças como diabetes e hipertensão.
2.4. Data Analysis
3. Results
3.1. Food Choice Questionnaire’s Structure
3.2. Food Choice Motives
3.3. Risk Perceptions and the Relationship with Food Choice Motives
4. Discussion
4.1. FCQ’s Structure
4.2. Food Choice Motives
4.3. Risk Perceptions and Food Choice Patterns
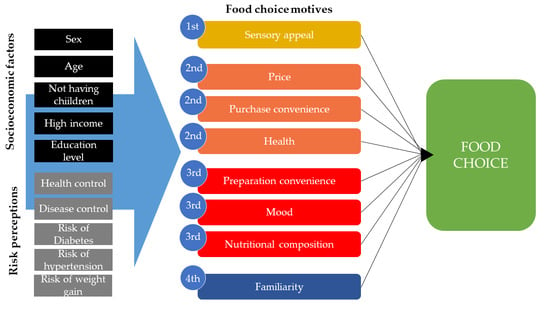
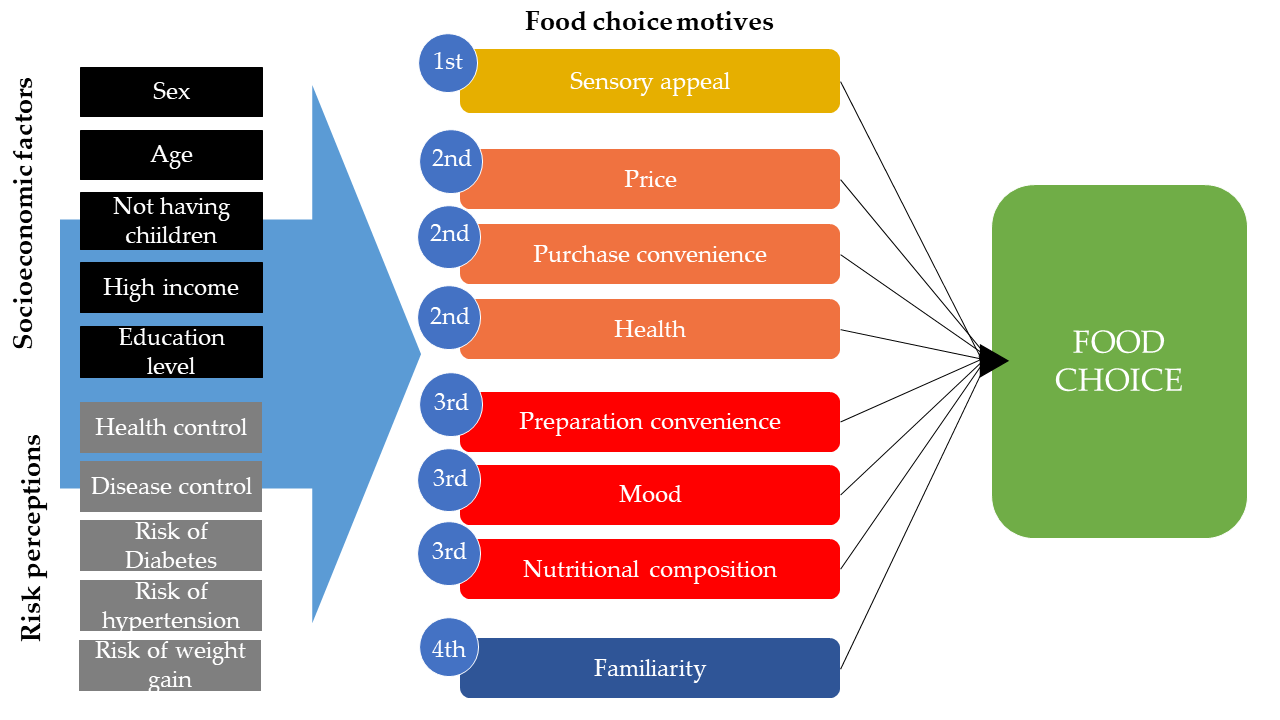
4.4. Modelling Food Choice Motives
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Alvarenga, M.; Figueiredo, M.; Timerman, F.; Antonaccio, C. Nutrição Comportamental, 1st ed.; Coutinho, W.L., Hosaka, A.M.d.S., Eds.; Editora Manole Ltda: Barueri, Brasil, 2015. [Google Scholar]
- Sobal, J.; Bisogni, C.A.; Devine, C.M.; Jastran, M. A Conptual Model of the Food Choice Progress over the Life Course. In The Psychology of Food Choice; Shepherd, R., Raats, M., Eds.; Biddles Ltd.: King’s Lynn, UK, 2006. [Google Scholar]
- Filho, M.B.; Rissin, A. Nutritional transition in Brazil: Geographic and temporal trends. Cad. Saude Publica 2003, 19, S181–S191. [Google Scholar]
- Brasíl Ministério da Saúde. Vigitel Brasil 2006: Vigilância de Fatores de Risco e Proteção Para Doenças Crônicas Por Inquérito Telefônico; Brasíl Ministério da Saúde: Brasília, Brazil.
- Brasil Ministério da Saúde. Vigitel Brasil 2018: Vigilância de Fatores de Risco e Proteção Para Doenças Crônicas Por Inquérito Telefônico. Brasil Ministério da Saúde: Brasília, Brazil, 2019. [Google Scholar]
- Lee, E.Y.; Yoon, K.-H. Epidemic obesity in children and adolescents: Risk factors and prevention. Front. Med. 2018, 12, 658–666. [Google Scholar] [CrossRef] [PubMed]
- Canella, D.S.; Levy, R.B.; Martins, A.P.B.; Claro, R.M.; Moubarac, J.C.; Baraldi, L.G.; Cannon, G.; Monteiro, C.A. Ultra-processed food products and obesity in Brazilian households (2008–2009). PLoS ONE 2014, 9, e92752. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, C.A.; Moubarac, J.-C.; Levy, R.B.; Canella, D.S.; da Costa Louzada, M.L.; Cannon, G. Household availability of ultra-processed foods and obesity in nineteen European countries. Public Health Nutr. 2018, 21, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Martins, A.P.B.; Levy, R.B.; Claro, R.M.; Moubarac, J.C.; Monteiro, C.A. Increased contribution of ultra-processed food products in the Brazilian diet (1987–2009). Rev. Saúde Pública 2013, 47, 656–665. [Google Scholar] [CrossRef]
- IBGE-Instituto Brasileiro de Geografia e Estatística. Pesquisa de Orçamentos Familiares—2008/2009; IBGE: Rio de Janeiro, Brazil, 2011.
- Sibai, A.M.; Nasreddine, L.; Mokdad, A.H.; Adra, N.; Tabet, M.; Hwalla, N. Nutrition Transition and Cardiovascular Disease Risk Factors in Middle East and North Africa Countries: Reviewing the Evidence. Ann. Nutr. Metab. 2010, 57, 193–203. [Google Scholar] [CrossRef]
- Popkin, B.M. The shift in stages of the nutrition transition in the developing world differs from past experiences! Public Health Nutr. 2002, 5, 205–214. [Google Scholar] [CrossRef]
- Sobal, J.; Bisogni, C.A.; Jastran, M. Food Choice Is Multifaceted, Contextual, Dynamic, Multilevel, Integrated, and Diverse. Mind Brain Educ. 2014, 8, 6–12. [Google Scholar] [CrossRef]
- Higgs, S. Social norms and their influence on eating behaviours. Appetite 2015, 86, 38–44. [Google Scholar] [CrossRef]
- Singh, M. Mood, food and obesity. Front. Psychol. 2014, 5, 1–35. [Google Scholar] [CrossRef]
- Chaya, C.; Eaton, C.; Hewson, L.; Vázquez, R.F.; Fernández-Ruiz, V.; Smart, K.A.; Hort, J. Developing a reduced consumer-led lexicon to measure emotional response to beer. Food Qual. Prefer. 2015, 45, 100–112. [Google Scholar] [CrossRef]
- Deliza, R.; Macfie, H.J.H. The generation of sensory expectation by external cues and its effect on sensory perception and hedonic ratings: A review. J. Sens. Stud. 1996, 11, 103–128. [Google Scholar] [CrossRef]
- Champion, V.L.; Skinner, C.S. The health belief model. In Health Behavior and Health Education: Theory, Research, and Practice; Glanz, K., Rimer, B.K., Viswanath, K., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 2008; pp. 45–65. [Google Scholar]
- McKenna, F.P. It won’t happen to me: Unrealistic optimism or illusion of control? Br. J. Psychol. 1993, 84, 39–50. [Google Scholar] [CrossRef]
- Steptoe, A.; Pollard, T.M.; Wardle, J. Development of a Measure of the Motives Underlying the Selection of Food: The Food Choice Questionnaire. Appetite 1995, 25, 267–284. [Google Scholar] [CrossRef] [PubMed]
- Cunha, L.M.; Cabral, D.; Moura, A.P.; de Almeida, M.D.V. Application of the Food Choice Questionnaire across cultures: Systematic review of cross-cultural and single country studies. Food Qual. Prefer. 2018, 64, 21–36. [Google Scholar] [CrossRef]
- Januszewska, R.; Pieniak, Z.; Verbeke, W. Food choice questionnaire revisited in four countries. Does it still measure the same? Appetite 2011, 57, 94–98. [Google Scholar] [CrossRef]
- Cabral, D.; de Almeida, M.D.V.; Cunha, L.M. Food Choice Questionnaire in an African country—Application and validation in Cape Verde. Food Qual. Prefer. 2017, 62, 90–95. [Google Scholar] [CrossRef]
- Knight, J.G.; Holdsworth, D.K.; Mather, D.W. Country-of-origin and choice of food imports: An in-depth study of European distribution channel gatekeepers. J. Int. Bus. Stud. 2007, 38, 107–125. [Google Scholar] [CrossRef]
- de Onis, J. Brazil’s Big Moment: A South American Giant Wakes Up. Foreign Aff. 2008, 87, 110–122. [Google Scholar]
- Heitor, S.F.D.; Estima, C.C.P.; Das Neves, F.J.; De Aguiar, A.S.; de Souza Castro, S.; de Souza Ferreira, J.E. Tradução e adaptação cultural do questionário sobre motivo das escolhas alimentares (Food Choice Questionnaire—FCQ) para a língua portuguesa. Cienc. Saude Coletiva 2015, 20, 2339–2346. [Google Scholar] [CrossRef]
- Heitor, S.F.D.; Reichenheim, M.E.; de Souza Ferreira, J.E.; de Souza Castro, S. Validity of the factorial structure of the brazilian version scale of the food choice questionnaire. Cienc. Saude Coletiva 2019, 24, 3551–3561. [Google Scholar] [CrossRef] [PubMed]
- Dean, A.G.; Sullivan, K.M.; Soe, M.M. Epi Info and OpenEpi in Epidemiology and Clinical Medicine: Health Applications of Free Software; CreateSpace: Scotts Valley, CA, USA, 2010. [Google Scholar]
- Pedhazur, E.J.; Schmelkin, L.P. Measurement, Design, and Analysis: An Integrated Approach; Lawrence Erlbaum Associates: Hillside, NJ, USA, 1991. [Google Scholar]
- Malhotra, N.K.; Nunan, D.; Birks, D.F. Marketing Research, 5th ed.; Pearson Education: Edinburgh, UK, 2017. [Google Scholar]
- Helweg-Larsen, M.; Shepperd, J.A. Do Moderators of the Optimistic Bias Affect Personal or Target Risk Estimates? A Review of the Literature. Personal. Soc. Psychol. Rev. 2001, 5, 74–95. [Google Scholar] [CrossRef]
- Raats, M.M.; Sparks, P.; Geekie, M.A.; Shepherd, R. The effects of providing personalized dietary feedback. A semi-computerized approach. Patient Educ. Couns. 1999, 37, 177–189. [Google Scholar] [CrossRef]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. A Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Milošević, J.; Žeželj, I.; Gorton, M.; Barjolle, D. Understanding the motives for food choice in Western Balkan Countries. Appetite 2012, 58, 205–214. [Google Scholar] [CrossRef] [PubMed]
- Szakály, Z.; Kontor, E.; Kovács, S.; Popp, J.; Pető, K.; Polereczki, Z. Adaptation of the Food Choice Questionnaire: The case of Hungary. Br. Food J. 2018, 120, 1474–1488. [Google Scholar] [CrossRef]
- Carrillo, E.; Varela, P.; Salvador, A.; Fiszman, S. Main Factors Underlying Consumers’ Food Choice: A First Step For The Understanding Of Attitudes Toward “Healthy Eating”. J. Sens. Stud. 2011, 26, 85–95. [Google Scholar] [CrossRef]
- Carvalho-Ferreira, J.P.d.; Finlayson, G.; da Cunha, D.T.; Caldas, G.; Bandoni, D.; de Rosso, V.V. Adiposity and binge eating are related to liking and wanting for food in Brazil: A cultural adaptation of the Leeds Food Preference Questionnaire. Appetite 2019, 133, 174–183. [Google Scholar] [CrossRef]
- Berthoud, H.-R. Homeostatic and Non-homeostatic Pathways Involved in the Control of Food Intake and Energy Balance. Obesity 2006, 14, 197S–200S. [Google Scholar] [CrossRef]
- Duerlund, M.; Andersen, B.V.; Grønbeck, M.S.; Byrne, D.V. Consumer reflections on post-ingestive sensations. A qualitative approach by means of focus group interviews. Appetite 2019, 142, 104350. [Google Scholar] [CrossRef]
- Monteiro, C.A.; Cannon, G.; Levy, R.B.; Moubarac, J.-C.; Louzada, M.L.; Rauber, F.; Khandpur, N.; Cediel, G.; Neri, D.; Martinez-Steele, E.; et al. Ultra-processed foods: What they are and how to identify them. Public Health Nutr. 2019, 22, 936–941. [Google Scholar] [CrossRef] [PubMed]
- Departamento de Atenção Básica, Secretaria de Atenção à Saúde, Ministério da Saúde. Guia Alimentar Para a População Brasileira; Ministério da saúde: Brasília, Brazil, 2014; ISBN 9788533421769.
- Monteiro, C.A.; Moubarac, J.C.; Cannon, G.; Ng, S.W.; Popkin, B. Ultra-processed products are becoming dominant in the global food system. Obes. Rev. 2013, 14, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Fiolet, T.; Srour, B.; Sellem, L.; Kesse-Guyot, E.; Allès, B.; Méjean, C.; Deschasaux, M.; Fassier, P.; Latino-Martel, P.; Beslay, M.; et al. Consumption of ultra-processed foods and cancer risk: Results from NutriNet-Santé prospective cohort. BMJ 2018, 360, k322. [Google Scholar] [CrossRef] [PubMed]
- Srour, B.; Fezeu, L.K.; Kesse-Guyot, E.; Allès, B.; Méjean, C.; Andrianasolo, R.M.; Chazelas, E.; Deschasaux, M.; Hercberg, S.; Galan, P.; et al. Ultra-processed food intake and risk of cardiovascular disease: Prospective cohort study (NutriNet-Santé). BMJ 2019, 365, 11451. [Google Scholar] [CrossRef] [PubMed]
- McCrickerd, K.; Forde, C.G. Sensory influences on food intake control: Moving beyond palatability. Obes. Rev. 2016, 17, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, N.D. Unrealistic optimism about future life events. J. Personal. Soc. Psychol. 1980, 39, 806–820. [Google Scholar]
- Gomes, D.C.K.; Sichieri, R.; Junior, E.V.; Boccolini, C.S.; de Moura Souza, A.; Cunha, D.B. Trends in obesity prevalence among Brazilian adults from 2002 to 2013 by educational level. BMC Public Health 2019, 19, 965. [Google Scholar] [CrossRef]
- Hartmann, C.; Dohle, S.; Siegrist, M. Importance of cooking skills for balanced food choices. Appetite 2013, 65, 125–131. [Google Scholar] [CrossRef]
- Pollard, T.M.; Steptoe, A.; Wardle, J. Motives underlying healthy eating: Using the food choice questionnaire to explain variation in dietary intake. J. Biosoc. Sci. 1998, 30, 165–179. [Google Scholar] [CrossRef]
- da Costa Louzada, M.L.; Martins, A.P.B.; Canella, D.S.; Baraldi, L.G.; Levy, R.B.; Claro, R.M.; Moubarac, J.C.; Cannon, G.; Monteiro, C.A. Ultra-processed foods and the nutritional dietary profile in Brazil. Rev. Saude Publica 2015, 49, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, C.A. Nutrition and health. The issue is not food, nor nutrients, so much as processing. Public Health Nutr. 2009, 12, 729–731. [Google Scholar] [CrossRef] [PubMed]
- Finkelstein, S.R.; Fishbach, A. When Healthy Food Makes You Hungry. J. Consum. Res. Inc. 2010, 37, 357–367. [Google Scholar] [CrossRef]
- Carvalho-Ferreira, J.P.d.; da Cunha, D.T.; Finlayson, G.; Caldas, G.; Jamar, G.; Bandoni, D.H.; Pisani, L.P.; de Rosso, V.V. Differential impact of consuming foods perceived to be high or low in fat on subsequent food reward. Food Qual. Prefer. 2020, 85, 103977. [Google Scholar] [CrossRef]
- Kuchkuntla, A.R.; Limketkai, B.; Nanda, S.; Hurt, R.T.; Mundi, M.S. Fad Diets: Hype or Hope? Curr. Nutr. Rep. 2018, 7, 310–323. [Google Scholar] [CrossRef]
- de Assis BRAGA, D.C.; Coletro, H.N.; de Freitas, M.T. Nutritional composition of fad diets published on websites and blogs. Rev. Nutr. 2019, 32, e170190. [Google Scholar] [CrossRef]
- Marangoni, J.S.; Maniglia, F.P. Nutrition analysis of diets published in magazines for women. Rev. Assoc. Bras. Nutr. 2017, 7894, 31–36. [Google Scholar]
- Barker, M.E.; Tandy, M.; Stookey, J.D. How are consumers of low-fat and high-fat diets perceived by those with lower and higher fat intake? Appetite 1999, 33, 309–317. [Google Scholar] [CrossRef]
- Silva, D.A.S.; Peres, K.G.; Boing, A.F.; González-Chica, D.A.; Peres, M.A. Clustering of risk behaviors for chronic noncommunicable diseases: A population-based study in southern Brazil. Prev. Med. (Baltim.) 2013, 56, 20–24. [Google Scholar] [CrossRef]
- Weinstein, N.D. Unrealistic optimism about susceptibility to health problems. J. Behav. Med. 1982, 5, 441–460. [Google Scholar] [CrossRef]
- Weinstein, N.D. Optimistic Biases About Personal Risks. Science 1989, 246, 1233–1234. [Google Scholar] [CrossRef]
- Slof-Op’t Landt, M.C.T.; van Furth, E.F.; van Beijsterveldt, C.E.M.; Bartels, M.; Willemsen, G.; de Geus, E.J.; Ligthart, L.; Boomsma, D.I. Prevalence of dieting and fear of weight gain across ages: A community sample from adolescents to the elderly. Int. J. Public Health 2017, 62, 911–919. [Google Scholar] [CrossRef] [PubMed]
- del Mar Bibiloni, M.; Coll, J.L.; Pich, J.; Pons, A.; Tur, J.A. Body image satisfaction and weight concerns among a Mediterranean adult population. BMC Public Health 2017, 17, 39. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, C.; Trindade, I.A.; Martinho, A. Explaining rigid dieting in normal-weight women: The key role of body image inflexibility. Eat. Weight Disord.-Stud. Anorex. Bulim. Obes. 2016, 21, 49–56. [Google Scholar]
- Brewer, N.T.; Weinstein, N.D.; Cuite, C.L.; Herrington, J.E. Risk Perceptions and Their Relation to Risk Behavior. Ann. Behav. Med. 2004, 27, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Assumpção, D.D.; Martins, S.; Domene, Á.; Fisberg, R.M.; Canesqui, A.M.; Barros, M.B.D.A. Differences between men and women in the quality of their diet: A study conducted on a population in Campinas, São Paulo, Brazil. Cienc. Saude Coletiva 2017, 22, 347–358. [Google Scholar] [CrossRef]
- Guibu, I.A.; Moraes, J.C.d.; Junior, A.A.G.; Costa, E.A.; Acurcio, F.d.A.; Costa, K.S.; Karnikowski, M.G.d.O.; Soeiro, O.M.; Leite, S.N.; Álvares, J. Características principais dos usuários dos serviços de atenção primária à saúde no Brasil. Rev. Saude Publica 2017, 51, 1s–13s. [Google Scholar]
- IBGE—Instituto Brasileiro de Geografia e Estatística. Pesquisa de Orçamentos Familiares 2017/2018, Primeiros Resultados; IBGE—Instituto Brasileiro de Geografia e Estatística: Rio de Janeiro, Brazil, 2019.



{kind=link}
{kind=link}
{kind=link}
| Variable | Frequency (n) | Valid Percentage (%) |
|---|---|---|
| Age (years old) | ||
| Young adults (18–34) | 301 | 57.3 |
| Adults (35–59) | 167 | 31.8 |
| Elderly (>60) | 57 | 10.9 |
| Marital status | ||
| Single | 298 | 56.8 |
| Married | 170 | 32.4 |
| Divorced | 33 | 6.3 |
| Widower | 24 | 4.6 |
| Have children | ||
| No | 314 | 59.9 |
| Yes | 210 | 40.1 |
| Education level | ||
| Incomplete primary education | 43 | 8.2 |
| Complete primary education | 30 | 5.7 |
| Incomplete high school | 21 | 4.0 |
| Complete high school | 67 | 12.8 |
| Incomplete higher education | 258 | 49.1 |
| Complete higher education | 106 | 20.2 |
| Family income | ||
| 1 to 2 times the minimum wage * | 99 | 19.1 |
| Between 2 and 3 times the minimum wage | 88 | 17.0 |
| Between 3 and 4 times the minimum wage | 70 | 13.5 |
| Between 4 and 5 times the minimum wage | 61 | 11.8 |
| More than 5 times the minimum wage | 199 | 38.5 |
| Factor | Items—“It Is Important to Me That the Food I Eat on a Typical Day...” | Loading | Mean (SD) * | Cronbach’s α |
|---|---|---|---|---|
| Factor 1 | Nutritional Composition | 5.46 c (1.23) | 0.863 | |
| Contains natural ingredients | 0.724 | 5.80 (1.37) | ||
| Contains no additives | 0.786 | 5.47 (1.60) | ||
| Contains no artificial ingredients | 0.761 | 5.37 (1.65) | ||
| Is low in fat | 0.612 | 5.51 (1.49) | ||
| Is low in calories | 0.574 | 5.16 (1.58) | ||
| Helps me control my weight | 0.544 | 5.57 (1.53) | ||
| Factor 2 | Mood | 5.48 c (1.15) | 0.794 | |
| Helps me cope with stress | 0.676 | 4.98 (1.78) | ||
| Helps me cope with life | 0.737 | 5.22 (1.78) | ||
| Helps me relax | 0.775 | 5.23 (1.58) | ||
| Makes me feel good | 0.521 | 6.21 (1.14) | ||
| Cheers me up | 0.710 | 5.76 (1.41) | ||
| Factor 3 | Health | 5.94 b (1.15) | 0.833 | |
| Is nutritious | 0.715 | 6.25 (1.19) | ||
| Is high in fibre and roughage | 0.537 | 5.62 (1.47) | ||
| Contains a lot of vitamins and minerals | 0.644 | 5.80 (1.34) | ||
| Is good for my skin/teeth/hair/nails etc. | 0.420 | 5.66 (1.61) | ||
| Keeps me healthy | 0.497 | 6.37 (1.00) | ||
| Factor 4 | Sensory Appeal | 6.19 a (0.90) | 0.778 | |
| Looks nice | 0.761 | 6.08 (1.27) | ||
| Has a pleasant texture | 0.766 | 5.96 (1.32) | ||
| Tastes good | 0.431 | 6.56 (0.82) | ||
| Smells nice | 0.679 | 6.16 (1.20) | ||
| Factor 5 | Price | 6.01 b (1.02) | 0.763 | |
| Is not expensive | 0.767 | 5.86 (1.36) | ||
| Is cheap | 0.803 | 5.79 (1.33) | ||
| Is good value for money | 0.549 | 6.38 (0.98) | ||
| Factor 6 | Preparation Convenience | 5.59 c (1.31) | 0.852 | |
| Is easy to prepare | 0.727 | 5.77 (1.43) | ||
| Takes no time to prepare | 0.899 | 5.47 (1.53) | ||
| Can be cooked very simply | 0.866 | 5.52 (1.51) | ||
| Factor 7 | Familiarity | 4.99 d (1.34) | 0.712 | |
| Is familiar to me | 0.537 | 5.48 (1.51) | ||
| Is what I usually eat | 0.710 | 5.45 (1.60) | ||
| Is like the food I ate when I was a child | 0.696 | 4.03 (1.94) | ||
| Factor 8 | Purchase Convenience | 5.95 b (1.18) | 0.625 | |
| Is easily available in shops and supermarkets | 0.660 | 5.91 (1.47) | ||
| Can be bought in shops close to where I live or work | 0.426 | 5.99 (1.30) |
| FCQ Factors | FCQ Factors | |||||||
|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
| Nutritional composition (1) | 1.000 | . | ||||||
| Mood (2) | 0.398 | 1.000 | ||||||
| Health (3) | 0.684 | 0.477 | 1.000 | |||||
| Sensory Appeal (4) | 0.487 | 0.353 | 0.400 | 1.000 | ||||
| Price (5) | 0.384 | 0.291 | 0.271 | 0.375 | 1.000 | |||
| Convenience of Preparation (6) | 0.192 | 0.258 | 0.226 | 0.191 | 0.422 | 1.000 | ||
| Familiarity (7) | 0.425 | 0.367 | 0.334 | 0.496 | 0.317 | 0.293 | 1.000 | |
| Convenience of Purchase (8) | 0.252 | 0.307 | 0.329 | 0.336 | 0.475 | 0.415 | 0.284 | 1.000 |
| FCQ Factors | Clusters | F-Value * | ||||
|---|---|---|---|---|---|---|
| 1—Health Driven (n = 106) | 2—Practicality Concerned (n = 77) | 3—Shape Concerned (n = 18) | 4—Food Concerned (n = 209) | 5—Cooking Enthusiasts (n = 88) | ||
| Sensory Appeal | 5.22 c,B (0.94) | 6.04 b,A (0.84) | 6.33 ab,A (1.10) | 6.69 a,A (0.42) | 6.24 b,A (0.73) | 72.70 |
| Price | 5.15 c,BC (1.03) | 5.91 b,A (0.90) | 6.01 b,AB (1.33) | 6.62 a,A (0.52) | 5.67 b,B (0.98) | 49.45 |
| Purchase Convenience | 5.18 c,B (1.15) | 5.96 b,A (0.92) | 3.38 d,C (1.74) | 6.58 a,A (0.63) | 5.84 b,B (0.99) | 89.24 |
| Health | 5.86 b,A (0.87) | 4.62 c,C (1.06) | 4.76 c,BC (1.26) | 6.58 a,A (0.48) | 5.84 b,B (0.77) | 50.93 |
| Preparation Convenience | 5.51 b,AB (1.00) | 6.07 a,A (0.90) | 4.42 c,BC (1.62) | 6.31 a,B (0.65) | 3.78 c,D (1.06) | 27.77 |
| Mood | 4.74 c,C (1.13) | 5.18 b,B (1.25) | 4.94 bc,BC (1.25) | 6.10 a,B (0.82) | 5.17b,C (0.92) | 102.01 |
| Nutritional Composition | 5.13 b,BC (0.99) | 3.92 d,D (0.91) | 5.80 a,AB (1.22) | 6.37 a,B (0.64) | 5.13 c,C (1.00) | 79.57 |
| Familiarity | 4.14 b,D (1.21) | 4.62 b,C (1.11) | 4.90 b,BC (1.43) | 5.77 a,C (1.06) | 4.29 b,D (1.26) | 38.00 |
| F-value ** | 115.21 | 19.78 | 32.07 | 118.10 | 42.15 | - |
| Independent Variables | Dependent Variables | ||||||
|---|---|---|---|---|---|---|---|
| Model 1—Nut Comp | Model 2—Sens App | Model 3—Health | Model 4—Price | Model 5—Fam | Model 6—Prep Conv | Model 7—Purch Conv | |
| Odds Ratio [CI 95%] | |||||||
| Sex (base value = female) | 0.32 (0.21–0.49) | 0.72 (0.62–0.84) | 0.66 (0.55–0.78) | 0.83 (0.69–0.99) | 0.72 (0.59–0.88) | - | - |
| Age (years) | 1.01 (1.00–1.02) | 1.01 (1.00–1.02) | 1.01 (1.00–1.02) | - | 1.00 * (0.99—1.01) | - | - |
| Children in household (base level = no) | 0.72 (0.54–0.94) | - | - | - | 0.31 (0.17–0.58) | 0.37 (0.20–0.67) | - |
| Income (base level = low income) | 0.88 * (0.73–1.06) | - | - | 0.62 (0.52–0.75) | - | 0.81 (0.68–0.97) | - |
| Perceived health control (scale from 1 to 7) | 1.10 (1.04–1.16) | - | 1.11 (1.06–1.17) | - | - | - | - |
| Education level (base level = high education level) | NS | 0.77 (0.63–0.93) | 0.80 (0.64–1.00) | - | 0.53 (0.41–0.69) | - | 0.54 (0.45–0.66) |
| Interaction (male sex and age) | 1.02 (1.01–1.03) | - | - | - | - | - | - |
| Interaction (high income and age) | - | - | - | - | 0.99 (0.99–1.00) | - | - |
| Interaction (have no children and age) | - | - | - | - | 1.02 (1.01–1.04) | 1.01 (1.00–1.02) | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marsola, C.d.M.; Cunha, L.M.; Carvalho-Ferreira, J.P.d.; da Cunha, D.T. Factors Underlying Food Choice Motives in a Brazilian Sample: The Association with Socioeconomic Factors and Risk Perceptions about Chronic Diseases. Foods 2020, 9, 1114. https://doi.org/10.3390/foods9081114
Marsola CdM, Cunha LM, Carvalho-Ferreira JPd, da Cunha DT. Factors Underlying Food Choice Motives in a Brazilian Sample: The Association with Socioeconomic Factors and Risk Perceptions about Chronic Diseases. Foods. 2020; 9(8):1114. https://doi.org/10.3390/foods9081114
Chicago/Turabian StyleMarsola, Camila de Mello, Luís Miguel Cunha, Joana Pereira de Carvalho-Ferreira, and Diogo Thimoteo da Cunha. 2020. "Factors Underlying Food Choice Motives in a Brazilian Sample: The Association with Socioeconomic Factors and Risk Perceptions about Chronic Diseases" Foods 9, no. 8: 1114. https://doi.org/10.3390/foods9081114
APA StyleMarsola, C. d. M., Cunha, L. M., Carvalho-Ferreira, J. P. d., & da Cunha, D. T. (2020). Factors Underlying Food Choice Motives in a Brazilian Sample: The Association with Socioeconomic Factors and Risk Perceptions about Chronic Diseases. Foods, 9(8), 1114. https://doi.org/10.3390/foods9081114