Relation between the Recipe of Yeast Dough Dishes and Their Glycaemic Indices and Loads


Abstract
1. Introduction
2. Materials and Methods
2.1. Characteristics of the Analysed Dishes
2.2. Characteristics of the Surveyed Participants
- Age—18–40 years;
- No cigarette smoking;
- Good self-perceived health status;
- Not taking drugs that affect carbohydrate metabolism;
- Not using any special diets and preference for diversified food rations;
- Moderate physical activity (no extreme sports activity);
- 10-h night fasting before the study.
2.3. Course of the Experiment
2.4. Calculation of GI and GL
2.5. Statistical Analysis
3. Results
3.1. Chemical Composition of Meals
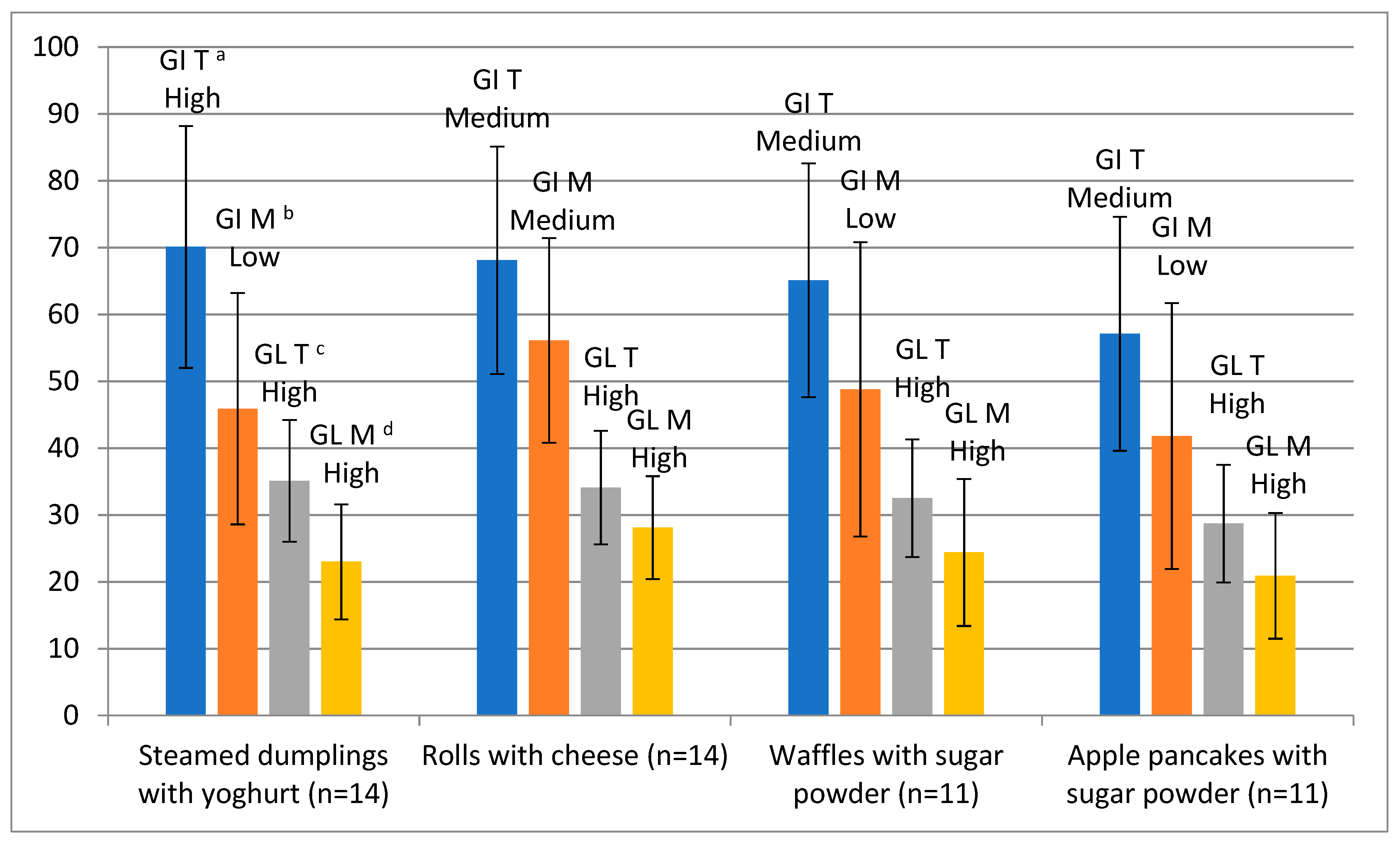
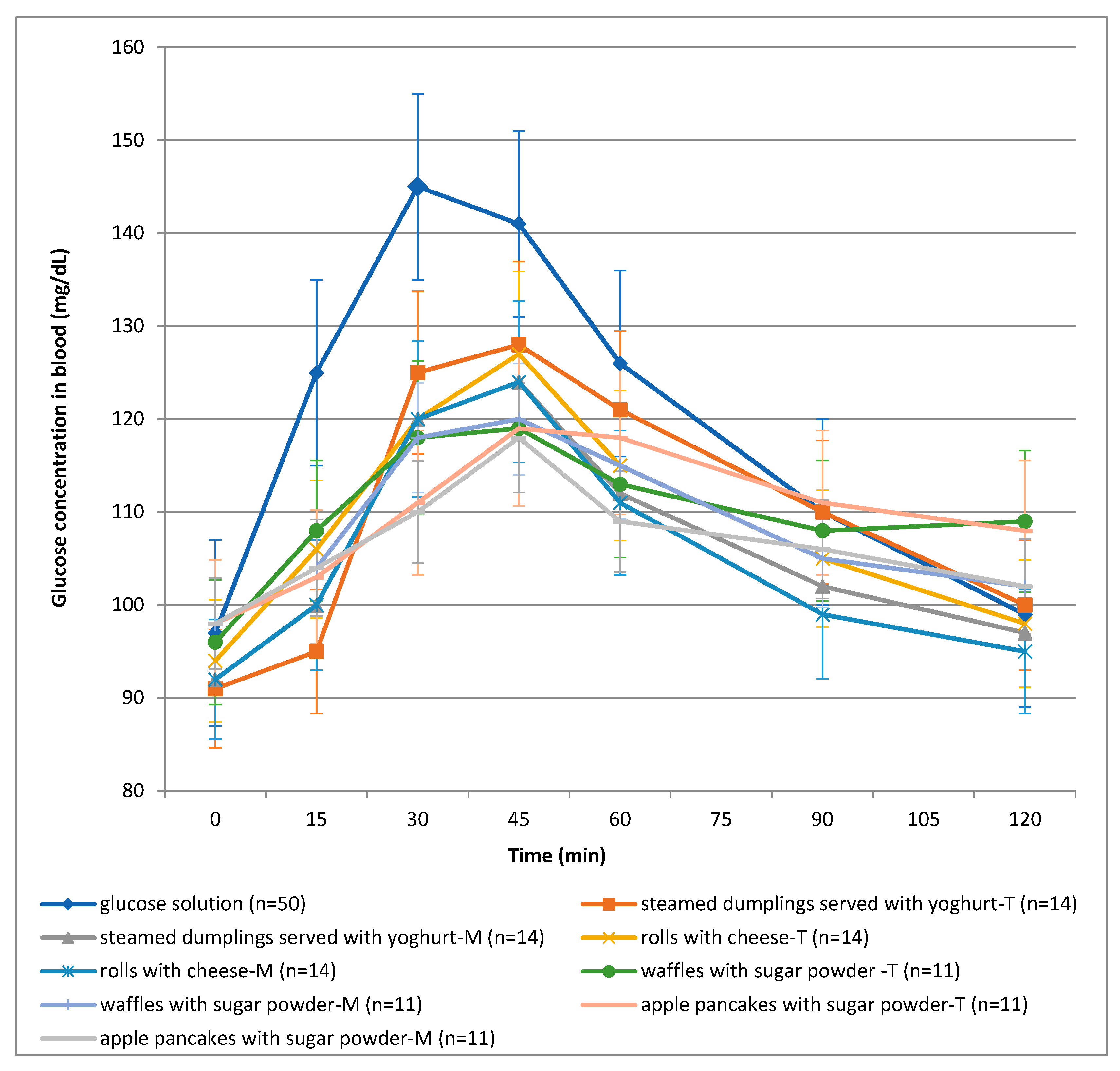
3.2. GI, GL and Glycaemic Response Curves of Test Meals
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Zamłyńska-Kowal, A.; Kusińska, E.; Sosińska-Leszczyńska, E.; Panasiewicz, M. Influence of pumpkin flour addition on textural properties of yeast dough. Acta Agroph. 2018, 25, 317–327. [Google Scholar] [CrossRef]
- Ali, A.; Shehzad, A.; Khan, M.R.; Shabbir, M.A.; Amjid, M.R. Yeast, its types and role in fermentation during bread making process—A review. Pak. J. Food Sci. 2012, 22, 171–179. [Google Scholar]
- Heitmann, M.; Zannini, E.; Arendt, E. Impact of Saccharomyces cerevisiae metabolites produced during fermentation on bread quality parameters: A review. Crit. Rev. Food Sci. 2018, 58, 1152–1164. [Google Scholar] [CrossRef]
- Struyf, N.; Van der Maelen, E.; Hemdane, S.; Verspreet, J.; Verstrepen, K.J.; Courtin, C.M. Bread Dough and Baker’s Yeast: An Uplifting Synergy. Compr. Rev. Food Sci. Food Safety 2017, 16, 850–867. [Google Scholar] [CrossRef]
- Sahin, B.; Schieberle, P. Characterization of the key aroma compounds in yeast dumplings by means of the sensonics concept. J. Agric. Food Chem. 2019, 67, 2973–2979. [Google Scholar] [CrossRef]
- Jaspreet, K.; Priya, K. Baker’s yeast. Industrial applications and health benefits. Appl. Biol. Res. 2019, 21, 105–113. [Google Scholar]
- Menezes, L.A.A.; Minervini, F.; Filannino, P.; Sardaro, M.L.S.; Gatti, M.; De Dea Lindner, J. Effects of Sourdough on FODMAPs in Bread and Potential Outcomes on Irritable Bowel Syndrome Patients and Healthy Subjects. Front. Microbiol. 2018, 9, 1972. [Google Scholar] [CrossRef]
- Struyf, N.; Laurent, J.; Verspreet, J.; Verstrepen, K.J.; Courtin, C.M. Saccharomyces cerevisiae and Kluyveromyces marxianus Cocultures Allow Reduction of Fermentable Oligo-, Di-, and Monosaccharides and Polyols Levels in Whole Wheat Bread. J. Agric. Food Chem. 2017, 65, 8704–8713. [Google Scholar] [CrossRef]
- Pushpangadan, P.; George, V.; Sreedevi, P.; Biney, A.J.; Anzar, S.; Aswany, T.; Ninawe, A.S.; Ijinu, T. Functional foods and nutraceuticals with special focus on mother and child care. Ann. Phytomed. 2014, 3, 4–24. [Google Scholar]
- Alkhatib, A.; Tsang, C.; Tiss, A.; Bahorun, T.; Arefanian, H.; Barake, R.; Khadir, A.; Tuomilehto, J. Functional Foods and Lifestyle Approaches for Diabetes Prevention and Management Nutrients. Nutrients 2017, 9, 1310. [Google Scholar] [CrossRef]
- Elmaliklis, N.; Liveri, A.; Ntelis, B.; Paraskeva, K.; Goulis, I.; Koutelidakis, A.E. Increased Functional Foods’ Consumption and Mediterranean Diet Adherence May Have a Protective Effect in the Appearance of Gastrointestinal Diseases: A Case⁻Control Study. Medicines 2019, 6, 50. [Google Scholar] [CrossRef]
- Del Castillo, M.D.; Iriondo-DeHond, A.; Martirosyan, D.M. Are Functional Foods Essential for Sustainable Health? Ann. Nutr. Food Sci. 2018, 2, 1015. [Google Scholar]
- GBD 2017 Diet Collaborators. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef]
- Zygler, A.; Wąsik, A.; Namieśnik, J. Analytical methodologies for determination of artificial sweeteners in foodstuffs. TrAc Trends Anal. Chem. 2009, 28, 1082–1102. [Google Scholar] [CrossRef]
- Gibney, M.J.; Barr, S.I.; Bellisle, F.; Drewnowski, A.; Fagt, S.; Livingstone, B.; Masset, G.; Moreiras, G.V.; Moreno, L.A.; Smith, J.; et al. Breakfast in Human Nutrition: The International Breakfast Research Initiative. Nutrients 2018, 10, 559. [Google Scholar] [CrossRef]
- Wolever, T.M.S.; Mehling, C. High-carbohydrate-low-glycaemic index dietary advice improves glucose disposition index in subjects with impaired glucose tolerance. Br. J. Nutr. 2002, 87, 477–487. [Google Scholar] [CrossRef]
- Wolever, T.M.S. Physiological mechanisms and observed health impacts related to the glycaemic index: Some observations. Int. J. Obes. 2006, 30, 72–78. [Google Scholar] [CrossRef]
- Venn, B.J.; Green, T.J. Glycemic index and glycemic load: measurement issues and their effect on diet–disease relationships. Eur. J. Clin. Nutr. 2007, 61, 122–131. [Google Scholar] [CrossRef]
- Bell, S.J.; Sears, B. Low-glycemic-load diets: Impact on obesity and chronic diseases. Crit. Rev. Food Sci. Nutr. 2003, 43, 357–377. [Google Scholar] [CrossRef]
- Lajous, M.; Boutron-Ruault, M.C.; Fabre, A.; Clavel-Chapelon, F.; Romieu, I. Carbohydrate intake, glycemic index, glycemic load, and risk of postmenopausal breast cancer in a prospective study of French women. Am. J. Clin. Nutr. 2008, 87, 1384–1391. [Google Scholar] [CrossRef]
- Esfahani, A.; Wong, J.M.W.; Mirrahimi, A.; Villa, C.R.; Kendall, C.W.C. The application of the glycemic index and glycemic load in weight loss: A review of the clinical evidence. Life 2011, 63, 7–13. [Google Scholar] [CrossRef]
- Marsh, K.; Barclay, A.; Colagiuri, S.; Brand-Miller, J. Glycemic index and glycemic load of carbohydrates in the diabetes diet. Curr. Diabetes Rep. 2011, 11, 120–127. [Google Scholar] [CrossRef]
- Sluijs, I.; van der Schouw, Y.T.; Spijkerman, A.M.; Hu, F.B.; Grobbee, D.E.; Beulens, J.W. Carbohydrate quantity and quality and risk of type 2 diabetes in the European Prospective Investigation into Cancer and Nutrition–Netherlands (EPIC-NL) study. Am. J. Clin. Nutr. 2010, 92, 905–911. [Google Scholar] [CrossRef]
- Dong, J.Y.; Zhang, Y.H.; Wang, P.; Qin, L.Q. Meta-analysis of dietary glycemic load and glycemic index in relation to risk of coronary heart disease. Am. J. Cardiol. 2012, 109, 1608–1613. [Google Scholar] [CrossRef]
- Murakami, K.; McCaffrey, T.A.; Livingstone, M.B.E. Associations of dietary glycaemic index and glycaemic load with food and nutrient intake and general and central obesity in British adults. Br. J. Nutr. 2013, 110, 2047–2057. [Google Scholar] [CrossRef]
- Bressiani, J.; Oro, T.; Santetti, G.S.; Almeida, J.L.; Bertolin, T.E.; Gómez, M.; Gutkoski, L.C. Properties of whole grain wheat flour and performance in bakery products as a function of particle size. J. Cereal Sci. 2017, 75, 269–277. [Google Scholar] [CrossRef]
- ISO 26642:2010. Food Products—Determination of the Glycaemic Index (GI) and Recommendation for Food Classification; International Standards Organisation: Geneva, Switzerland, 2010.
- Carbohydrates in Human Nutrition (FAO Food and Nutrition Paper No. 66). Report of a Joint FAO/WHO Expert Consultation; World Health Organisation, Food and Agriculture Organization of the United Nations: Rome, Italy, 1997.
- Gronowska-Senger, A. Analiza żywności. Zbiór ćwiczeń (Food analysis. Collection of exercises); Wydawnictwo SGGW: Warsaw, Poland, 2010. (In Polish) [Google Scholar]
- Association of Official Agricultural Chemists International. Methods of Analysis of AOAC International, 18th ed.; AOAC International: Rockville, MD, USA.
- Nadolna, I.; Przygoda, B.; Iwanow, K.; Kunachowicz, H. Tables of Composition and Nutritional Value of Food; PZWL: Warsaw, Poland, 2005. [Google Scholar]
- Berger, S.; Janik, K.; Kulzowa-Hawliczkowa, H.; Laskowska, M.; Nowicka, L.; Rościszewska-Stoyanow, A.; Rutkowski, A.; Stobnicka-Szczygłowa, H.; Szlęzakowa, I.; Witkowska, S. Kuchina Polska (Polish Cuisine); Państwowe Wydawnictwo Ekonomiczne: Warsaw, Poland, 1990. (In Polish) [Google Scholar]
- Foster-Powell, K.; Holt, S.H.A.; Brand-Miller, J.C. International table of glycemic index and glycemic load values: 2002. Am. J. Clin. Nutr. 2002, 76, 5–56. [Google Scholar] [CrossRef]
- Atkinson, F.S.; Foster-Powell, K.; Brand-Miller, J.C. International tables of glycemic index and glycemic load values: 2008. Diabetes Care 2008, 31, 2281–2283. [Google Scholar] [CrossRef]
- Alongi, M.; Melchior, S.; Anese, M. Reducing the glycemic index of short dough biscuits by using apple pomace as a functional ingredient. LWT 2019, 100, 300–305. [Google Scholar] [CrossRef]
- Scazzina, F.; Dall’Asta, M.; Casiraghi, M.C.; Sieri, S.; Del Rio, D.; Pellegrini, N.; Brighenti, F. Glycemic index and glycemic load of commercial Italian foods. Nutr. Metab. Cardiovas. 2016, 26, 419–429. [Google Scholar] [CrossRef]
- Jariyah, J.; Susiloningsih, E.K.B.; Nilasari, K. Glycemic Index Biscuits Formulation of Pedada Flour (Sonneratia caseolaris) with Tubers Starch. J. Phys. Conf. Ser. 2018, 953, 012246. [Google Scholar] [CrossRef]
- Avberšek Lužnik, I.; Lušnic Polak, M.; Demšar, L.; Gašperlin, L.; Polak, T. Does type of bread ingested for breakfast contribute to lowering of glycaemic index? J. Nutr. Intermed. Metab. 2019, 16, 100097. [Google Scholar] [CrossRef]
- Borczak, B.; Sikora, M.; Sikora, E.; Dobosz, A.; Kapusta-Duch, J. Glycaemic index of wheat bread. Starch/Stärke 2018, 70, 1700022. [Google Scholar] [CrossRef]
- Bae, I.Y.; Lee, H.I.; Ko, A.; Lee, H.G. Substituting whole grain flour for wheat flour: Impact on cake quality and glycemic index. Food Sci. Biotechnol. 2013, 22, 1–7. [Google Scholar] [CrossRef]
- Ferrer-Mairal, A.; Peñalva-Lapuente, C.; Iglesia, I.; Urtasun, L.; De Miguel-Etayo, P.; Remón, S.; Cortés, E.; Moreno, L.A. In vitro and in vivo assessment of the glycemic index of bakery products: Influence of the reformulation of ingredients. Eur. J. Nutr. 2012, 51, 947–954. [Google Scholar] [CrossRef]
- Taye, A.; Engidawork, E.; Urga, K. An in vitro estimation of glycemic index of white bread and improvement of the dietary fiber. Adv. Food Technol. Nutr. Sci. 2016, 2, 83–87. [Google Scholar] [CrossRef]
- Litwinek, D.; Gambuś, H.; Zięć, G.; Gambuś, F. Porównanie indeksu i ładunku glikemicznego herbatników owsianych oraz pszennych. Żywność: Nauka. Technologia. Jakość 2014, 5, 168–182. (In Polish) [Google Scholar]
- Marangoni, F.; Poli, A. The glycemic index of bread and biscuits is markedly reduced by the addition of a proprietary fiber mixture to the ingredients. Nutr. Metab. Cardiovas. Dis. 2008, 18, 602–605. [Google Scholar] [CrossRef]
- Henry, C.J.K.; Lightowler, H.J.; Kendall, F.L.; Storey, M. The impact of the addition of toppings/fillings on the glycaemic response to commonly consumed carbohydrate foods. Eur. J. Clin. Nutr. 2006, 60, 763–769. [Google Scholar] [CrossRef]
- Kouamé, C.A.; Kouassi, N.K.; Abodo, J.R.; Pereko, K.K.A.; Casiraghi, M.C.; N’dri, D.Y.; Amani, G.N. Glycemic responses, glycemic index, and glycemic load values of some street foods prepared from plantain (Musa spp., AAB genome) in Côte d’Ivoire. Foods 2017, 6, 83. [Google Scholar] [CrossRef]
- Gagné, L. The glycemic index and glycemic load in clinical practice. Explore 2008, 4, 66–69. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Recipe | Steamed Dumplings with Yoghurt | Rolls with Cheese | Waffles with Sugar Powder | Apple Pancakes with Sugar Powder | ||||
|---|---|---|---|---|---|---|---|---|
| T | M | T | M | T | M | T | M | |
| X ± SD | X ± SD | X ± SD | X ± SD | X ± SD | X ± SD | X ± SD | X ± SD | |
| Energy value (kcal/100 g) | 260.3 ± 8.3 | 244.7 ± 9.3 | 294.6 ± 15.9 | 260.2 ± 12.3 | 318.8 ± 7.9 | 308.7 ± 8.8 | 229.7 ± 11.5 | 212.6 ± 7.8 |
| Protein (g/100 g) | 7.5 ± 0.3 | 8.4 ± 0.6 | 10.7 ± 0.4 | 12.6 ± 0.5 | 9.9 ± 0.5 | 10.4 ± 0.7 | 6.5 ± 0.3 | 7.3 ± 0.3 |
| Total carbohydrates (g/100 g) | 38.9 ± 3.6 | 35.5 ± 3.8 | 43.8 ± 4.8 | 40.6 ± 5.1 | 41.5 ± 3.2 | 36.9 ± 3.5 | 39.5 ± 3.7 | 34.9 ± 3.2 |
| Fat (g/100 g) | 6.2 ± 0.4 | 5.9 ± 0.4 | 5.9 ± 0.6 | 6.6 ± 0.4 | 11.9 ± 0.7 | 11.7 ± 0.6 | 3.6 ± 0.4 | 3.8 ± 0.3 |
| Fibre (g/100 g) | 1.1 | 2.7 | 1.4 | 3.2 | 1.2 | 2.8 | 1.4 | 2.6 |
| Total ash (g/100 g) | 0.57 ± 0.03 | 0.93 ± 0.05 | 0.94 ± 0.05 | 1.48 ± 0.08 | 0.81 ± 0.04 | 1.18 ± 0.05 | 0.59 ± 0.03 | 0.78 ± 0.04 |
| Water (g/100 g) | 46.8 ± 2.3 | 49.3 ± 1.4 | 38.6 ± 1.3 | 38.7 ± 1.9 | 35.6 ± 1.7 | 39.8 ± 1.8 | 49.8 ± 2.2 | 53.2 ± 2.0 |
| Test portion size (g) 1 | 133.0 | 153.0 | 119.0 | 135.0 | 125.0 | 148.0 | 132.0 | 156.0 |
| Parameter | Sample | ||
|---|---|---|---|
| Mean | SEM | Range | |
| Age (years) | 21.7 | 1.1 | 21.0–27.0 |
| Gender (female/male) | 42/8 | ||
| Body weight (kg) | 60.3 | 8.5 | 49.2–87.0 |
| Height (m) | 1.68 | 0.1 | 1.6–1.9 |
| BMI (kg/m2) | 21.2 | 2.0 | 19.1–24.9 |
| Fasting glucose (mg/dL) | 93.0 | 0.1 | 81.0–98.0 |
| Correlation | Pearson’s Correlation Coefficient (r) |
|---|---|
| GI and energy value | 0.241 * |
| GI and protein content | 0.068 |
| GI and fat content | 0.057 |
| GI and total carbohydrate content | 0.410 * |
| GI and the ash content | −0.140 |
| GI and fibre content | −0.440 * |
| GI and water content | −0.271 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raczkowska, E.; Łoźna, K.; Bienkiewicz, M.; Jurczok, K.; Bronkowska, M. Relation between the Recipe of Yeast Dough Dishes and Their Glycaemic Indices and Loads. Foods 2019, 8, 377. https://doi.org/10.3390/foods8090377
Raczkowska E, Łoźna K, Bienkiewicz M, Jurczok K, Bronkowska M. Relation between the Recipe of Yeast Dough Dishes and Their Glycaemic Indices and Loads. Foods. 2019; 8(9):377. https://doi.org/10.3390/foods8090377
Chicago/Turabian StyleRaczkowska, Ewa, Karolina Łoźna, Maciej Bienkiewicz, Karolina Jurczok, and Monika Bronkowska. 2019. "Relation between the Recipe of Yeast Dough Dishes and Their Glycaemic Indices and Loads" Foods 8, no. 9: 377. https://doi.org/10.3390/foods8090377
APA StyleRaczkowska, E., Łoźna, K., Bienkiewicz, M., Jurczok, K., & Bronkowska, M. (2019). Relation between the Recipe of Yeast Dough Dishes and Their Glycaemic Indices and Loads. Foods, 8(9), 377. https://doi.org/10.3390/foods8090377