
Effects of Dietary Fiber Supplementation on Chronic Constipation in the Elderly: A Systematic Review and Meta-Analysis of Randomized Controlled Trials



Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Literature Searches
2.3. Eligibility Criteria
2.4. Data Extraction
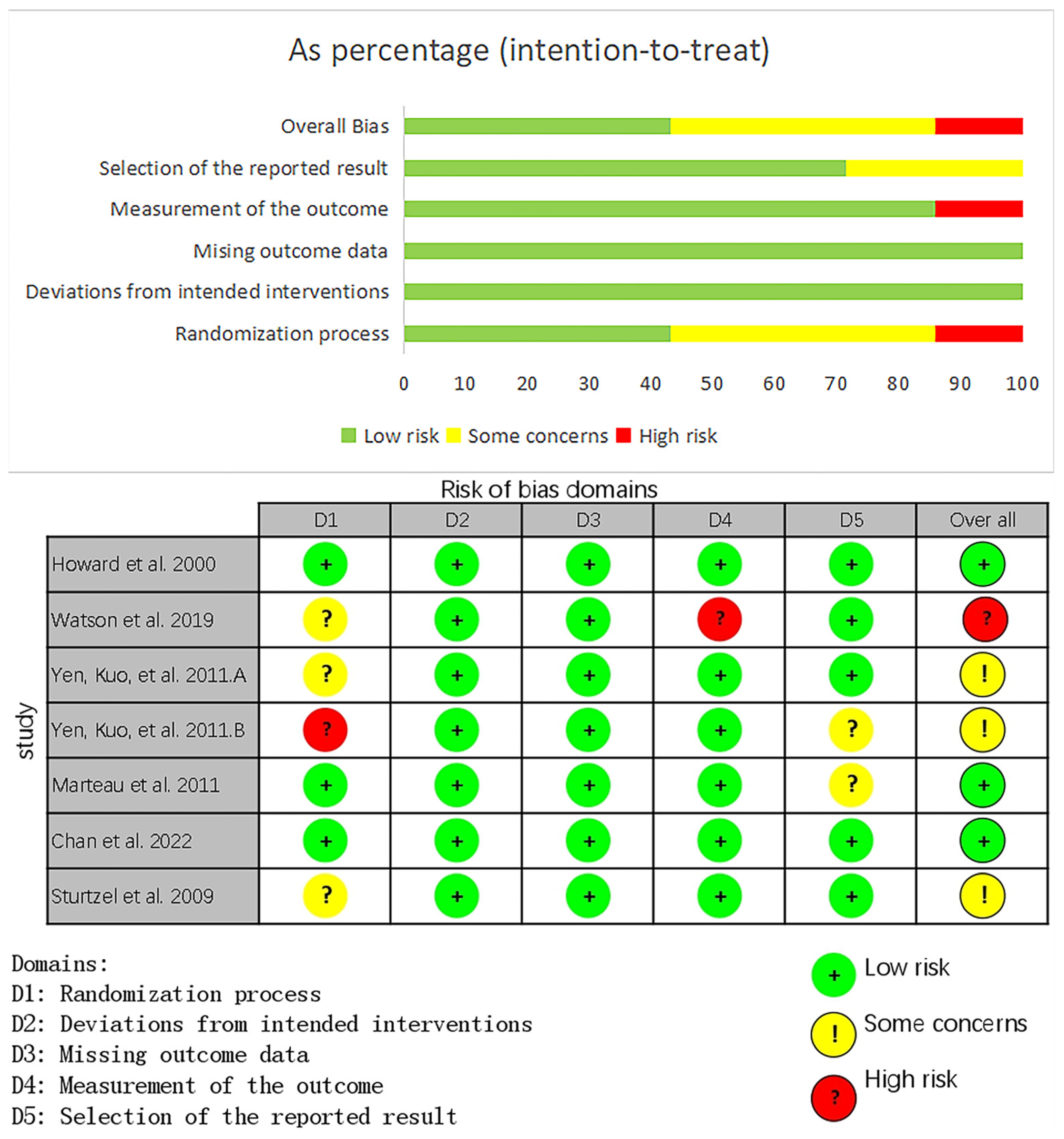
2.5. Assessment of Risk of Bias
2.6. Data Synthesis and Statistical Analysis
3. Results
3.1. Results of the Search
3.2. Study Characteristics
3.3. Risk of Bias
3.4. Outcomes
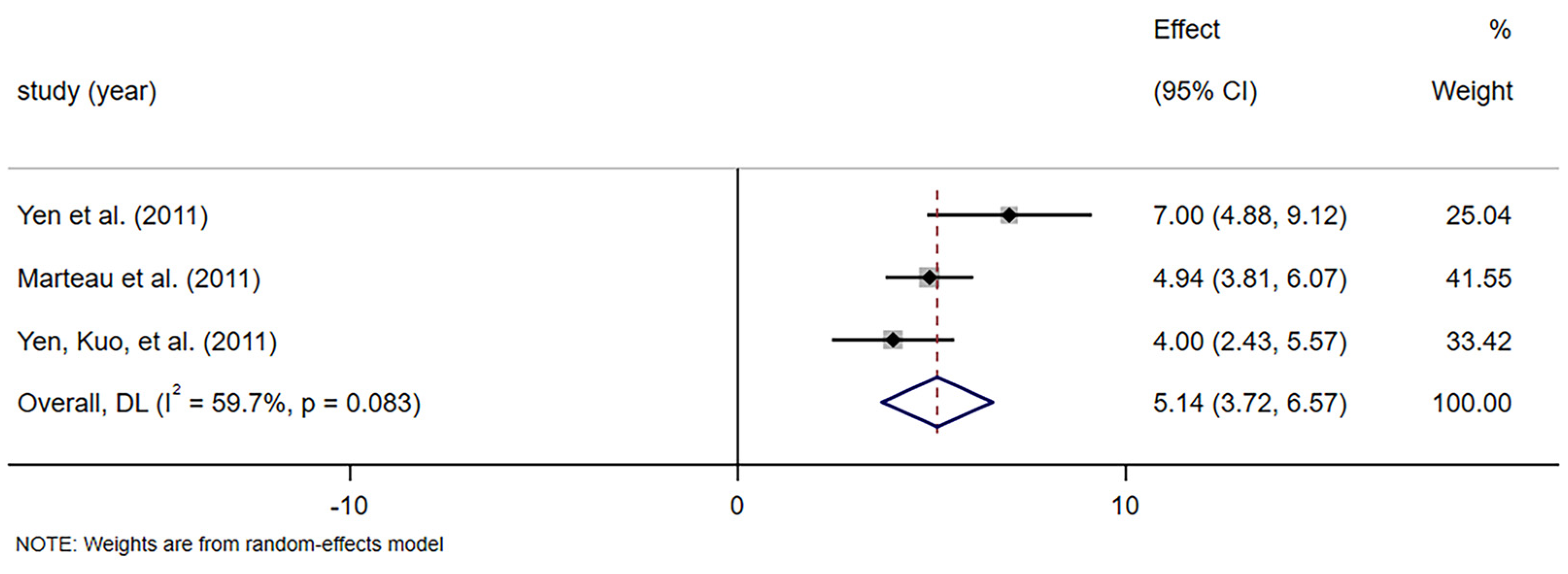
3.4.1. Stool Frequency
3.4.2. Stool Dry Weight
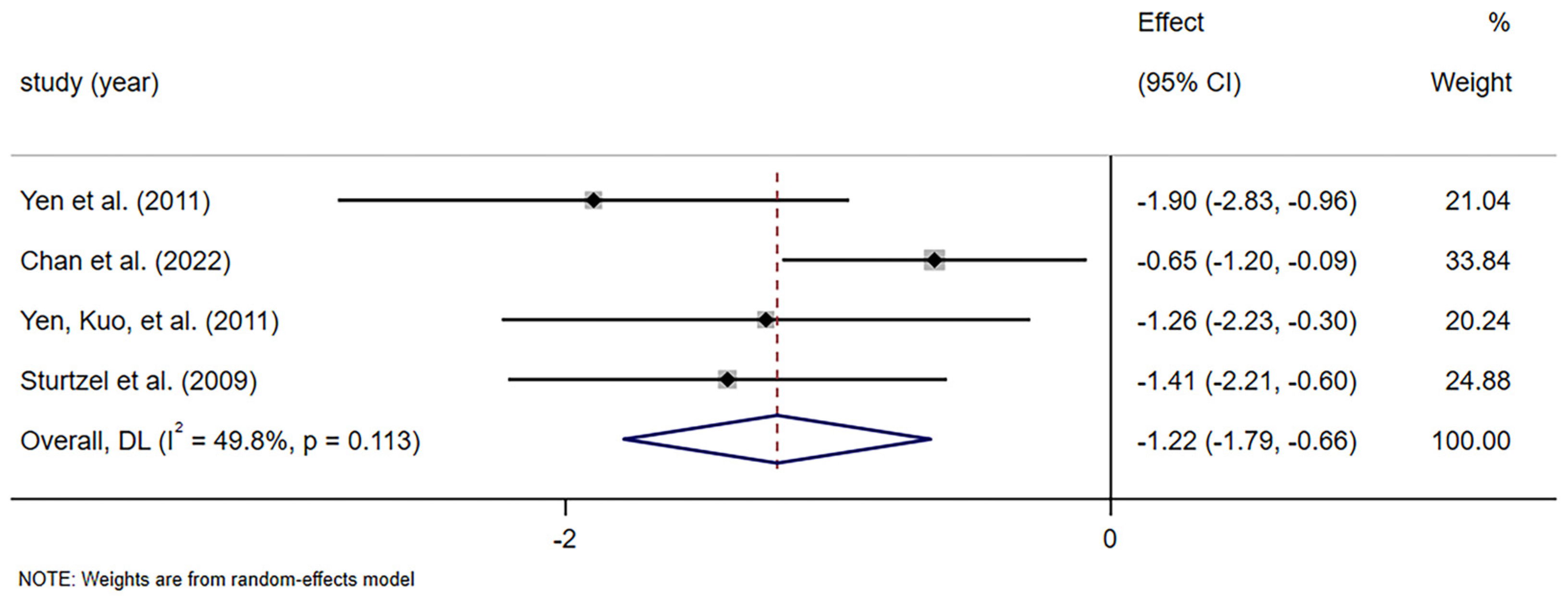
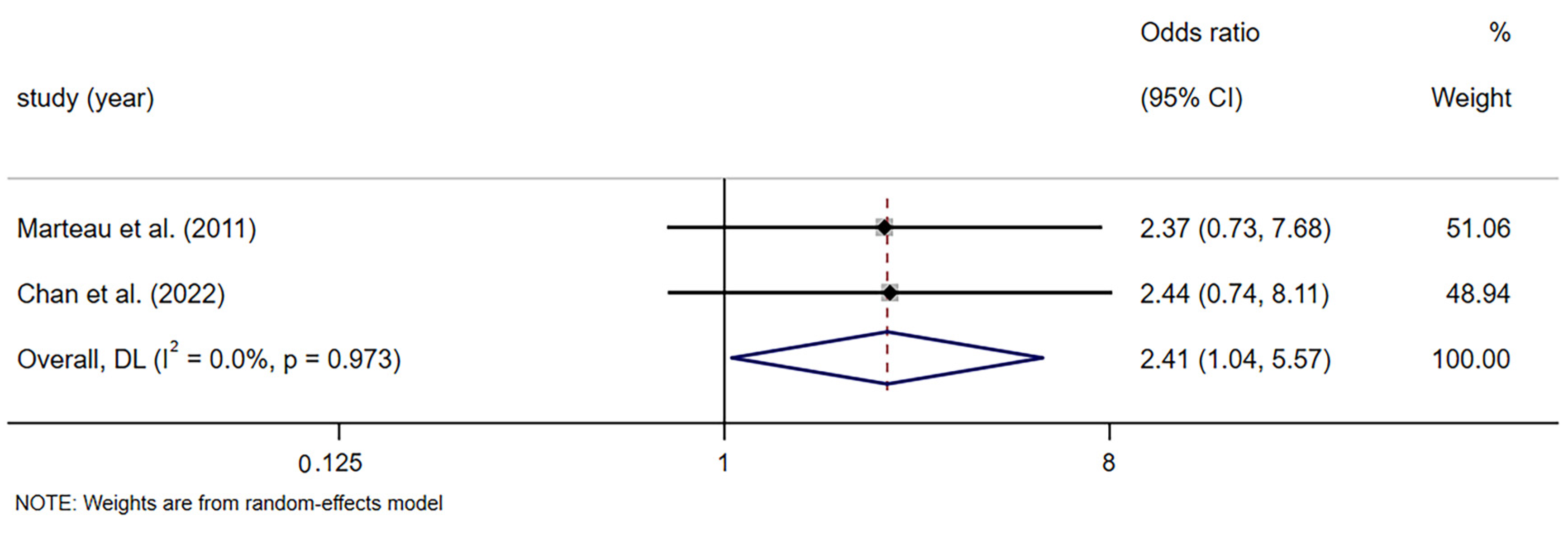
3.4.3. Frequency of Laxative or Enema Use
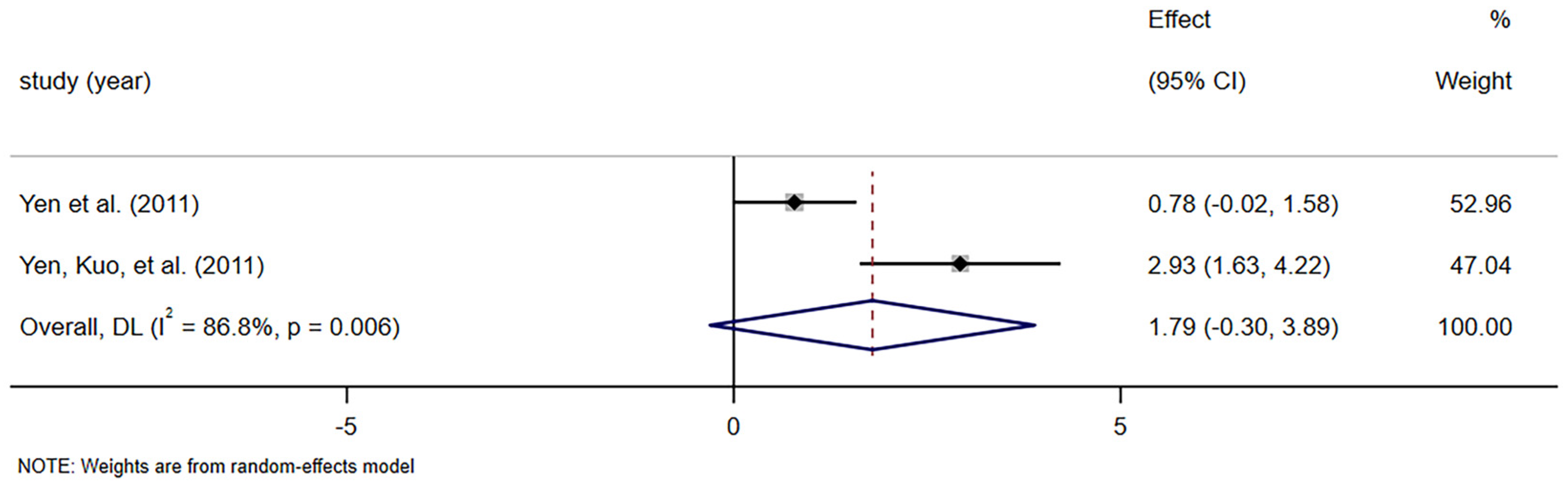
3.4.4. Intestinal Bifidobacteria Concentration
3.4.5. Adverse Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Masaoka, T. Current Management of Chronic Constipation in Japan. Keio J. Med. 2023, 72, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Kurniawan, I.; Simadibrata, M. Management of Chronic Constipation in the Elderly. Acta Med. Indones. 2011, 43, 195–205. [Google Scholar] [PubMed]
- Baffy, N.; Foxx-Orenstein, A.E.; Harris, L.A.; Sterler, S. Intractable Constipation in the Elderly. Curr. Treat. Options Gastroenterol. 2017, 15, 363–381. [Google Scholar] [CrossRef] [PubMed]
- Wlodarczyk, J.; Wasniewska, A.; Fichna, J.; Dziki, A.; Dziki, L.; Wlodarczyk, M. Current Overview on Clinical Management of Chronic Constipation. J. Clin. Med. 2021, 10, 1738. [Google Scholar] [CrossRef]
- Barberio, B.; Judge, C.; Savarino, E.V.; Ford, A.C. Global Prevalence of Functional Constipation according to the Rome Criteria: A Systematic Review and Meta-analysis. Lancet Gastroenterol. Hepatol. 2021, 6, 638–648. [Google Scholar] [CrossRef]
- De Giorgio, R.; Ruggeri, E.; Stanghellini, V.; Eusebi, L.H.; Bazzoli, F.; Chiarioni, G. Chronic Constipation in the Elderly: A Primer for the Gastroenterologist. BMC Gastroenterol. 2015, 15, 130. [Google Scholar] [CrossRef]
- Higgins, P.D.; Johanson, J.F. Epidemiology of Constipation in North America: A Systematic Review. Am. J. Gastroenterol. 2004, 99, 750–759. [Google Scholar] [CrossRef]
- Forootan, M.; Bagheri, N.; Darvishi, M. Chronic Constipation: A Review of Literature. Medicine 2018, 97, e10631. [Google Scholar] [CrossRef]
- Du, X.; Liu, S.; Jia, P.; Wang, X.; Gan, J.; Hu, W.; Zhu, H.; Song, Y.; Niu, J.; Ji, Y. Epidemiology of Constipation in Elderly People in Parts of China: A Multicenter Study. Front. Public Health 2022, 10, 823987. [Google Scholar] [CrossRef]
- Yang, D.Y.; Lupianez-Merly, C.; Jencks, K.; Burton, D.; Ryks, M.; Camilleri, M. Overall and Regional Colonic Transit Abnormalities in Elderly Patients with Constipation. Dig. Dis. Sci. 2025, 70, 1132–1141. [Google Scholar] [CrossRef]
- Vazquez Roque, M.; Bouras, E.P. Epidemiology and Management of Chronic Constipation in Elderly Patients. Clin. Interv. Aging 2015, 10, 919–930. [Google Scholar]
- Okuyan, C.B.; Bilgili, N. Determining the Prevalence of Constipation and Relating Factors in Elderly People: A Nursing Home Study. Florence Nightingale Hemsire Derg. 2019, 27, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Bouras, E.P.; Tangalos, E.G. Chronic Constipation in the Elderly. Gastroenterol. Clin. N. Am. 2009, 38, 463–480. [Google Scholar] [CrossRef] [PubMed]
- Bruce Wirta, S.; Hodgkins, P.; Joseph, A. Economic Burden associated with Chronic Constipation in Sweden: A Retrospective Cohort Study. Clinicoecon. Outcomes Res. 2014, 6, 369–379. [Google Scholar] [CrossRef] [PubMed]
- Harris, L.A.; Chang, C.H. Burden of Constipation: Looking Beyond Bowel Movements. Am. J. Gastroenterol. 2022, 117, S2–S5. [Google Scholar] [CrossRef]
- Sun, S.X.; DiBonaventura, M.; Purayidathil, F.W.; Wagner, J.S.; Dabbous, O.; Mody, R. Impact of Chronic Constipation on Health-Related Quality of Life, Work Productivity, and Healthcare Resource Use: An Analysis of the National Health and Wellness Survey. Dig. Dis. Sci. 2011, 56, 2688–2695. [Google Scholar] [CrossRef]
- Fleming, V.; Wade, W.E. A Review of Laxative Therapies for Treatment of Chronic Constipation in Older Adults. Am. J. Geriatr. Pharmacother. 2010, 8, 514–550. [Google Scholar] [CrossRef]
- Lucak, S.; Lunsford, T.N.; Harris, L.A. Evaluation and Treatment of Constipation in the Geriatric Population. Clin. Geriatr. Med. 2021, 37, 85–102. [Google Scholar] [CrossRef]
- Sbahi, H.; Cash, B.D. Chronic Constipation: A Review of Current Literature. Curr. Gastroenterol. Rep. 2015, 17, 47. [Google Scholar] [CrossRef]
- Johanson, J.F.; Kralstein, J. Chronic Constipation: A Survey of the Patient Perspective. Aliment. Pharmacol. Ther. 2007, 25, 599–608. [Google Scholar] [CrossRef]
- Kubota, Y.; Iso, H.; Tamakoshi, A. Bowel Movement Frequency, Laxative Use, and Mortality From Coronary Heart Disease and Stroke Among Japanese Men and Women: The Japan Collaborative Cohort (JACC) Study. J. Epidemiol. 2016, 26, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Gong, L.; Liu, F.; Liu, J.; Wang, J. Dietary Fiber (Oligosaccharide and Non-starch Polysaccharide) in Preventing and Treating Functional Gastrointestinal Disorders—Challenges and Controversies: A Review. Int. J. Biol. Macromol. 2024, 258 Pt 1, 128835. [Google Scholar] [CrossRef]
- Wang, Z.; Yang, Z.; Liu, J.; Hao, Y.; Sun, B.; Wang, J. Potential Health Benefits of Whole Grains: Modulation of Mitochondrial Biogenesis and Energy Metabolism. J. Agric. Food Chem. 2021, 69, 14065–14074. [Google Scholar] [CrossRef] [PubMed]
- Gill, S.K.; Rossi, M.; Bajka, B.; Whelan, K. Dietary Fibre in Gastrointestinal Health and Disease. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 101–116. [Google Scholar] [CrossRef] [PubMed]
- Topping, D.L.; Clifton, P.M. Short-chain Fatty Acids and Human Colonic Function: Roles of Resistant Starch and Nonstarch Polysaccharides. Physiol. Rev. 2001, 81, 1031–1064. [Google Scholar] [CrossRef]
- Soret, R.; Chevalier, J.; De Coppet, P.; Poupeau, G.; Derkinderen, P.; Segain, J.P.; Neunlist, M. Short-chain Fatty Acids Regulate the Enteric Neurons and Control Gastrointestinal Motility in Rats. Gastroenterology 2010, 138, 1772–1782. [Google Scholar] [CrossRef]
- Wang, H.; Huang, X.; Tan, H.; Chen, X.; Chen, C.; Nie, S. Interaction between Dietary Fiber and Bifidobacteria in Promoting Intestinal Health. Food Chem. 2022, 393, 133407. [Google Scholar] [CrossRef]
- Dahl, W.J.; Lockert, E.A.; Cammer, A.L.; Whiting, S.J. Effects of Flax Fiber on Laxation and Glycemic Response in Healthy Volunteers. J. Med. Food. 2005, 8, 508–511. [Google Scholar] [CrossRef]
- Rao, S.S.C.; Yu, S.; Fedewa, A. Systematic Review: Dietary Fibre and FODMAP-Restricted Diet in the Management of Constipation and Irritable Bowel Syndrome. Aliment. Pharmacol. Ther. 2015, 41, 1256–1270. [Google Scholar] [CrossRef]
- Huang, C.; Lyu, J.; Chu, C.; Ge, L.; Peng, Y.; Yang, Z.; Xiong, S.; Wu, B.; Chen, X.; Zhang, X. Dietary Fiber and Probiotics Based on Gut Microbiota Targeting for Functional Constipation in Children with Cerebral Palsy. Front. Pediatr. 2022, 10, 1001789. [Google Scholar]
- Pannemans, J.; Masuy, I.; Tack, J. Functional Constipation: Individualising Assessment and Treatment. Drugs 2020, 80, 947–963. [Google Scholar] [CrossRef] [PubMed]
- Eswaran, S.; Muir, J.; Chey, W.D. Fiber and Functional Gastrointestinal Disorders. Am. J. Gastroenterol. 2013, 108, 718–727. [Google Scholar] [CrossRef] [PubMed]
- Fuller, S.; Beck, E.; Salman, H.; Tapsell, L. New Horizons for the Study of Dietary Fiber and Health: A Review. Plant Foods Hum. Nutr. 2016, 71, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Vandeputte, D.; Falony, G.; Vieira-Silva, S.; Wang, J.; Sailer, M.; Theis, S.; Verbeke, K.; Raes, J. Prebiotic Inulin-type Fructans Induce Specific Changes in the Human Gut Microbiota. Gut 2017, 66, 1968–1974. [Google Scholar] [CrossRef]
- Black, C.J.; Ford, A.C. Chronic Idiopathic Constipation in Adults: Epidemiology, Pathophysiology, Diagnosis and Clinical Management. Med. J. Aust. 2018, 209, 86–91. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Syst Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, 4898. [Google Scholar] [CrossRef]
- Howard, L.V.; West, D.; Ossip-Klein, D.J. Chronic Constipation Management for Institutionalized Older Adults. Geriatr. Nur. 2000, 21, 78–82. [Google Scholar] [CrossRef]
- Sturtzel, B.; Mikulits, C.; Gisinger, C.; Elmadfa, I. Use of Fiber Instead of Laxative Treatment in a Geriatric Hospital to Improve the Wellbeing of Seniors. J. Nutr. Health Aging 2009, 13, 136–139. [Google Scholar] [CrossRef]
- Yen, C.H.; Kuo, Y.W.; Tseng, Y.H.; Lee, M.C.; Chen, H.L. Beneficial Effects of Fructo-oligosaccharides Supplementation on Fecal Bifidobacteria and Index of Peroxidation Status in Constipated Nursing-home Residents—A Placebo-controlled, Diet-controlled trial. Nutrition 2011, 27, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Yen, C.H.; Tseng, Y.H.; Kuo, Y.W.; Lee, M.C.; Chen, H.L. Long-term Supplementation of Isomalto-oligosaccharides Improved Colonic Microflora Profile, Bowel Function, and Blood Cholesterol Levels in Constipated Elderly People—A Placebo-controlled, Diet-controlled Trial. Nutrition 2011, 27, 445–450. [Google Scholar] [CrossRef] [PubMed]
- Marteau, P.; Jacobs, H.; Cazaubiel, M.; Signoret, C.; Prevel, J.M.; Housez, B. Effects of Chicory Inulin in Constipated Elderly People: A Double-blind Controlled Trial. Int. J. Food Sci. Nutr. 2011, 62, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Watson, A.W.; Houghton, D.; Avery, P.J.; Stewart, C.; Vaughan, E.E.; Meyer, P.D.; de Bos Kuil, M.J.J.; Weijs, P.J.M.; Brandt, K. Changes in Stool Frequency Following Chicory Inulin Consumption, and Effect on Stool Consistency, Quality of Life and Composition of Gut Microbiota. Food Hydrocoll. 2019, 96, 688–698. [Google Scholar] [CrossRef]
- Chan, T.C.; Yu, V.M.W.; Luk, J.K.H.; Chu, L.W.; Yuen, J.K.Y.; Chan, F.H.W. Effectiveness of Partially Hydrolyzed Guar Gum in Reducing Constipation in Long Term Care Facility Residents: A Randomized Single-blinded Placebo-controlled Trial. J. Nutr. Health Aging 2022, 26, 247–251. [Google Scholar] [CrossRef]
- Schoot, A.; Drysdale, C.; Whelan, K.; Dimidi, E. The Effect of Fiber Supplementation on Chronic Constipation in Adults: An Updated Systematic Review and Meta-analysis of Randomized Controlled Trials. Am. J. Clin. Nutr. 2022, 116, 953–969. [Google Scholar] [CrossRef]
- Christodoulides, S.; Dimidi, E.; Fragkos, K.C.; Farmer, A.D.; Whelan, K.; Scott, S.M. Systematic Review with Meta-analysis: Effect of Fibre Supplementation on Chronic Idiopathic Constipation in Adults. Aliment. Pharmacol. Ther. 2016, 44, 103–116. [Google Scholar] [CrossRef]
- Piccoli de Mello, P.; Eifer, D.A.; Daniel de Mello, E. Use of Fibers in Childhood Constipation Treatment: Systematic Review with Meta-analysis. J. Pediatr. 2018, 94, 460–470. [Google Scholar] [CrossRef]
- Tack, J.; Müller-Lissner, S.; Stanghellini, V.; Boeckxstaens, G.; Kamm, M.A.; Simren, M.; Galmiche, J.P.; Fried, M. Diagnosis and Treatment of Chronic Constipation—A European Perspective. Neurogastroenterol. Motil. 2011, 23, 697–710. [Google Scholar] [CrossRef]
- Suares, N.C.; Ford, A.C. Systematic Review: The Effects of Fibre in the Management of Chronic Idiopathic Constipation. Aliment. Pharmacol. Ther. 2011, 33, 895–901. [Google Scholar] [CrossRef]
- Mitsuhashi, S.; Ballou, S.; Jiang, Z.G.; Hirsch, W.; Nee, J.; Iturrino, J.; Cheng, V.; Lembo, A. Characterizing Normal Bowel Frequency and Consistency in a Representative Sample of Adults in the United States (NHANES). Am. J. Gastroenterol. 2018, 113, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Eun, S.J. Pharmacological Treatment of Chronic Constipation: Focused on Oral Laxatives. J. Korean Med. Assoc. 2018, 61, 57–61. [Google Scholar]
- Luthra, P.; Camilleri, M.; Burr, N.E.; Quigley, E.M.M.; Black, C.J.; Ford, A.C. Efficacy of Drugs in Chronic Idiopathic Constipation: A Systematic Review and Network Meta-analysis. Lancet Gastroenterol. Hepatol. 2019, 4, 831–844. [Google Scholar] [CrossRef]
- Komiya, H.; Umegaki, H.; Asai, A.; Kanda, S.; Maeda, K.; Nomura, H.; Kuzuya, M. Prevalence and Risk Factors of Constipation and Pollakisuria among Older Home-care Patients. Geriatr. Gerontol. Int. 2019, 19, 277–281. [Google Scholar] [CrossRef]
- Werth, B.L.; Williams, K.A.; Fisher, M.J.; Pont, L.G. Use of Over-the-counter Laxatives by Community-dwelling Adults to Treat and Prevent Constipation: A National Cross-sectional Study. Eur. J. Clin. Pharmacol. 2020, 76, 1003–1010. [Google Scholar] [CrossRef]
- O’Brien, L.; Wilkinson, T.J.; Frampton, C.; Gearry, R.B.; Wall, C. A Systematic Review and Meta-analysis of the Dietary Fiber Menu Provision and Consumption for Older Adults Living in Residential Care Facilities. Am. J. Clin Nutr. 2024, 120, 431–441. [Google Scholar] [CrossRef] [PubMed]
- Atsushi, N.; Hiroki, T.; Yukikazu, K.; Seigo, S.; Masaki, I.; Ataru, I. High-fiber Liquid Diet for Chronic Constipation: An Exploration from Healthcare Providers’ Survey Results. CNO 2023, 52, 34–48. [Google Scholar]
- Nellesen, D.; Yee, K.; Chawla, A.; Lewis, B.E.; Carson, R.T. A Systematic Review of the Economic and Humanistic Burden of Illness in Irritable Bowel Syndrome and Chronic Constipation. J. Manag. Care Pharm. 2013, 19, 755–764. [Google Scholar] [CrossRef]
- Abreu, Y.; Abreu, A.T.; Milke-Garcia, M.P.; Arguello-Arevalo, G.A.; Calderón-de la Barca, A.M.; Carmona-Sánchez, R.I.; Consuelo-Sánchez, A.; Coss-Adame, E.; García-Cedillo, M.F.; Hernández-Rosiles, V.; et al. Dietary Fiber and the Microbiota: A Narrative Review by a Group of Experts from the Asociacion Mexicana de Gastroenterologia. Rev. Gastroenterol. Mex. (Engl. Ed.) 2021, 86, 287–304. [Google Scholar] [CrossRef]
- Zhen, H.; Qian, H.; Liu, X.; Tan, C. Fructooligosaccharides for Relieving Functional Constipation: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Foods. 2024, 13, 3993. [Google Scholar] [CrossRef]
- Abdulqadir, R.; Engers, J.; Al Sadi, R. Role of Bifidobacterium in Modulating the Intestinal Epithelial Tight Junction Barrier: Current Knowledge and Perspectives. Curr. Dev. Nutr. 2023, 7, 102026. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, M.J.; Sharp, R.; Macfarlane, G.T. Age and Disease Related Changes in Intestinal Bacterial Populations Assessed by Cell Culture, 16S rRNA Abundance, and Community Cellular Fatty Acid Profiles. Gut 2001, 48, 198–205. [Google Scholar] [CrossRef] [PubMed]
- Tawfick, M.M.; Xie, H.; Zhao, C.; Shao, P.; Farag, M.A. Inulin Fructans in Diet: Role in Gut Homeostasis, Immunity, Health Outcomes and Potential Therapeutics. Int. J. Biol. Macromol. 2022, 208, 948–961. [Google Scholar] [CrossRef]
- Ionita Mindrican, C.B.; Ziani, K.; Mititelu, M.; Oprea, E.; Neacșu, S.M.; Moroșan, E.; Dumitrescu, D.E.; Roșca, A.C.; Drăgănescu, D.; Negrei, C. Therapeutic Benefits and Dietary Restrictions of Fiber Intake: A State of the Art Review. Nutrients 2022, 14, 2641. [Google Scholar] [CrossRef]
- Mysonhimer, A.R.; Holscher, H.D. Gastrointestinal Effects and Tolerance of Nondigestible Carbohydrate Consumption. Adv. Nutr. 2022, 13, 2237–2276. [Google Scholar] [CrossRef]
- Richardson, M.; Garner, P.; Donegan, S. Interpretation of Subgroup Analyses in Systematic Reviews: A Tutorial. Clin. Epidemiol. Glob. Health 2019, 7, 192–198. [Google Scholar] [CrossRef]
- So, D.; Whelan, K.; Rossi, M.; Morrison, M.; Holtmann, G.; Kelly, J.T.; Shanahan, E.R.; Staudacher, H.M.; Campbell, K.L. Dietary Fiber Intervention on Gut Microbiota Composition in Healthy Adults: A Systematic Review and Meta-analysis. Am. J. Clin. Nutr. 2018, 107, 965–983. [Google Scholar] [CrossRef]
- Takaoka, M.; Igarashi, A.; Ninomiya, A.; Ishibashi, T.; Yamamoto-Mitani, N. Continuous Laxative Use and its Relationship to Defecation among Residents of Nursing Homes: A Longitudinal Observational Study Using the InterRAI. Geriatr. Gerontol. Int. 2024, 24, 133–139. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Criteria |
|---|---|
| Participants (P) | Constipated patients over the age of 50 of any ethnicity and geographic area |
| Interventions (I) | Any type of dietary fiber supplement |
| Comparisons (C) | Placebo or habitual diet or any pharmacological or non-pharmacological interventions |
| Outcomes (O) | Stool frequency, stool consistency, stool weight, gastrointestinal symptoms, use of laxatives or enemas, and adverse events |
| Study design (S) | Randomized controlled trials (RCTs) in either parallel or crossover design |
| First Author/ Year | Study Design | Number of Participants | Age (Range) (Years) | Diagnostic Criteria | Duration of Therapy | Intervention/Dose | Form | Outcomes |
|---|---|---|---|---|---|---|---|---|
| Sturtzel 2009 [40] | Double-blind, parallel | 30 | 57–98 | Not mentioned | Twelve weeks | Ordinary oat flakes vs habitual diet; 7–8 g oat-bran/d | Solid | The usage of laxatives; bodyweight; stool frequency |
| Yen 2011 [42] | Double-blind, crossover | 13 | 82.5 ± 1.9 | Not mentioned | Eight weeks | Isomalto-oligosaccharide vs. Placebo; 5 g/d for the first 7 d 22 g/d for the rest of time | Liquid | Fecal bacteria; bowel function; fecal short-chain fatty acids; biochemical indices |
| Marteau 2011 [43] | Double-blind, parallel | 50 | 50–70 | Rome definition | Four weeks | Native inulin vs. Placebo; 15 g/d | Sachet | Microbiological analyses; bowel symptoms; bowel motor function parameters |
| Chan 2022 [45] | Single-blind, parallel | 52 | 83.9 ± 7.6 | Rome III criteria | Four weeks | PHGG vs. Placebo; 5 g PHGG/d | Liquid | Frequency of laxative use; fecal consistency; fecal frequency; fecal |
| Howard, 2000 [39] | Double-blind, parallel | 12 | 61–80 | Two or fewer stools/week | Five months | Bran mixture vs. Placebo; ≥3 tablespoons/d | Liquid | Number of bowel movements; number of bowel medications |
| Watson 2019 [44] | Double-blind, crossover | 20 | 62 (from 51 to 74) | Self-reported | Five weeks | Inulin vs. placebo; 10 g/day | Sachet | Stool frequency; consistency; fecal microbiota |
| Yen 2011 [41] | Double-blind, crossover | 10 | 74.0 ± 3.3 | Taking medication for constipation or ≤3 spontaneous bowel movements/week or straining with a bowel movement without medication | Four weeks | FOS vs. placebo; 5 g/d for the first 7 d 10 g/d for 8–28 days | Liquid | Fecal bifidobacteria; lipid peroxidation index; indices of nutritional status |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xi, N.; Yang, X.; Liu, J.; Yue, H.; Wang, Z. Effects of Dietary Fiber Supplementation on Chronic Constipation in the Elderly: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Foods 2025, 14, 2315. https://doi.org/10.3390/foods14132315
Xi N, Yang X, Liu J, Yue H, Wang Z. Effects of Dietary Fiber Supplementation on Chronic Constipation in the Elderly: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Foods. 2025; 14(13):2315. https://doi.org/10.3390/foods14132315
Chicago/Turabian StyleXi, Na, Xiao Yang, Jie Liu, Hao Yue, and Ziyuan Wang. 2025. "Effects of Dietary Fiber Supplementation on Chronic Constipation in the Elderly: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Foods 14, no. 13: 2315. https://doi.org/10.3390/foods14132315
APA StyleXi, N., Yang, X., Liu, J., Yue, H., & Wang, Z. (2025). Effects of Dietary Fiber Supplementation on Chronic Constipation in the Elderly: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Foods, 14(13), 2315. https://doi.org/10.3390/foods14132315