
Prevalence of Metabolic Syndrome Based on the Dietary Habits and Physical Activity of Korean Women Cancer Survivors



Abstract
1. Introduction
2. Materials and Methods
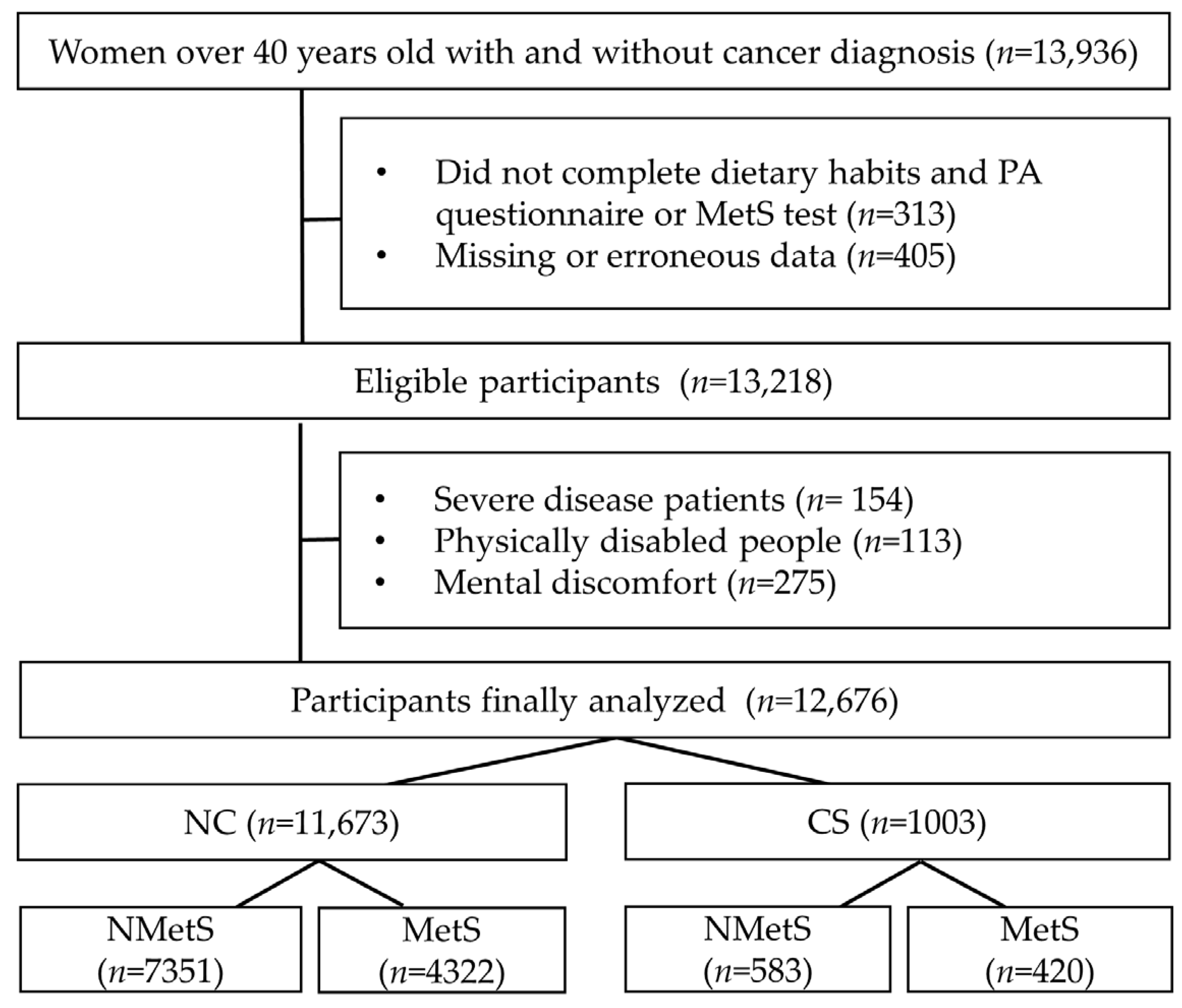
2.1. Participants
2.2. Health Questionnaire
2.3. Dietary Habits
2.4. Physical Activity
2.5. Diagnosis of Metabolic Syndrome
2.6. Data Analysis
3. Results
3.1. General Characteristics
3.2. Odds Ratio for MetS and Factors According to Cancer Type
3.3. MetS Odds Ratio According to Dietary Habits
3.4. MetS Odds Ratio According to Physical Activity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| PA | physical activity |
| CS | cancer survivors |
| MetS | metabolic syndrome |
| NC | non-cancer |
| CI | confidence interval |
| BP | blood pressure |
| WHO | World Health Organization |
References
- Jung, K.-W.; Won, Y.-J.; Kang, M.J.; Kong, H.-J.; Im, J.-S.; Seo, H.G. Prediction of cancer incidence and mortality in Korea, 2022. Cancer Res. Treat. Off. J. Korean Cancer Assoc. 2022, 54, 345–351. [Google Scholar] [CrossRef]
- Suh, Y.S.; Lee, J.; Woo, H.; Shin, D.; Kong, S.H.; Lee, H.J.; Shin, A.; Yang, H.K. National cancer screening program for gastric cancer in Korea: Nationwide treatment benefit and cost. Cancer 2020, 126, 1929–1939. [Google Scholar] [CrossRef]
- Kweon, S.-S. Updates on cancer epidemiology in Korea, 2018. Chonnam Med. J. 2018, 54, 90–100. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Johansen, S.; Cvancarova, M.; Ruland, C. The effect of cancer patients’ and their family caregivers’ physical and emotional symptoms on caregiver burden. Cancer Nurs. 2018, 41, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Schirrmacher, V. From chemotherapy to biological therapy: A review of novel concepts to reduce the side effects of systemic cancer treatment. Int. J. Oncol. 2019, 54, 407–419. [Google Scholar] [CrossRef] [PubMed]
- Peddie, N.; Agnew, S.; Crawford, M.; Dixon, D.; MacPherson, I.; Fleming, L. The impact of medication side effects on adherence and persistence to hormone therapy in breast cancer survivors: A qualitative systematic review and thematic synthesis. Breast 2021, 58, 147–159. [Google Scholar] [CrossRef]
- Shapiro, C.L. Cancer survivorship. N. Engl. J. Med. 2018, 379, 2438–2450. [Google Scholar] [CrossRef]
- Jung, H.-S.; Myung, S.-K.; Kim, B.-S.; Seo, H.G. Metabolic syndrome in adult cancer survivors: A meta-analysis. Diabetes Res. Clin. Pract. 2012, 95, 275–282. [Google Scholar] [CrossRef]
- Bellastella, G.; Scappaticcio, L.; Esposito, K.; Giugliano, D.; Maiorino, M.I. Metabolic syndrome and cancer:“The common soil hypothesis”. Diabetes Res. Clin. Pract. 2018, 143, 389–397. [Google Scholar] [CrossRef]
- Rock, C.L.; Thomson, C.A.; Sullivan, K.R.; Howe, C.L.; Kushi, L.H.; Caan, B.J.; Neuhouser, M.L.; Bandera, E.V.; Wang, Y.; Robien, K. American Cancer Society nutrition and physical activity guideline for cancer survivors. CA Cancer J. Clin. 2022, 72, 230–262. [Google Scholar] [CrossRef]
- Jones, L.M.; Stoner, L.; Baldi, J.C.; McLaren, B. Circuit resistance training and cardiovascular health in breast cancer survivors. Eur. J. Cancer Care 2020, 29, e13231. [Google Scholar] [CrossRef]
- de Paulo, T.R.; Winters-Stone, K.M.; Viezel, J.; Rossi, F.E.; Simões, R.R.; Tosello, G.; Junior, I.F.F. Effects of resistance plus aerobic training on body composition and metabolic markers in older breast cancer survivors undergoing aromatase inhibitor therapy. Exp. Gerontol. 2018, 111, 210–217. [Google Scholar] [CrossRef]
- Garcia-Unciti, M.; Palacios Samper, N.; Méndez-Sandoval, S.; Idoate, F.; Ibáñez-Santos, J. Effect of Combining Impact-Aerobic and Strength Exercise, and Dietary Habits on Body Composition in Breast Cancer Survivors Treated with Aromatase Inhibitors. Int. J. Environ. Res. Public Health 2023, 20, 4872. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-Y.; Park, N.H.; Song, Y.-S.; Park, S.M.; Lee, H.-W.; Kim, K.H.; Choi, K.-H. Prevalence of the metabolic syndrome and associated factors in Korean cancer survivors. Asian Pac. J. Cancer Prev. 2013, 14, 1773–1780. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Yun, Y.H.; Kim, Y.; Lee, M.K.; Sim, J.A.; Nam, B.-H.; Kim, S.; Lee, E.S.; Noh, D.-Y.; Lim, J.-Y.; Kim, S. A randomized controlled trial of physical activity, dietary habit, and distress management with the Leadership and Coaching for Health (LEACH) program for disease-free cancer survivors. BMC Cancer 2017, 17, 298. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. International Guide for Monitoring Alcohol Consumption and Related Harm; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Jung, H. Validation of Food Frequency Questionnaire for Korea National Health and Nutrition Examination Survey; Korea Center for Diease Control and Prevention: Osong, Republic of Korea, 2010.
- Yun, S.H.; Shim, J.-S.; Kweon, S.; Oh, K. Development of a food frequency questionnaire for the Korea National Health and Nutrition Examination Survey: Data from the fourth Korea National Health and Nutrition Examination Survey (KNHANES IV). Korean J. Nutr. 2013, 46, 186–196. [Google Scholar] [CrossRef]
- Hong, H.-S.; Park, S.-J.; Lee, D.-K.; Lee, H.-J. Comparison of the portion sizes of Korean adults across eating places: Korea National Health and Nutrition Examination Survey (2012–2016). J. Nutr. Health 2020, 53, 676–687. [Google Scholar] [CrossRef]
- Tee, E.S.; Nurliyana, A.R.; Karim, N.A.; Jan Mohamed, H.J.B.; Tan, S.Y.; Appukutty, M.; Hopkins, S.; Thielecke, F.; Ong, M.K.; Ning, C. Breakfast consumption among Malaysian primary and secondary school children and relationship with body weight status-Findings from the MyBreakfast Study. Asia Pac. J. Clin. Nutr. 2018, 27, 421–432. [Google Scholar]
- Adolphus, K.; Lawton, C.L.; Dye, L. The relationship between habitual breakfast consumption frequency and academic performance in British adolescents. Front. Public Health 2015, 3, 68. [Google Scholar] [CrossRef]
- Craig, C.; Marshall, A.; Sjostrom, M.; Bauman, A.; Lee, P.; Macfarlane, D.; Lam, T.; Stewart, S. International physical activity questionnaire-short form. J. Am. Coll. Health 2017, 65, 492–501. [Google Scholar]
- Oh, J.Y.; Yang, Y.J.; Kim, B.S.; Kang, J.H. Validity and reliability of Korean version of International Physical Activity Questionnaire (IPAQ) short form. J. Korean Acad. Fam. Med. 2007, 28, 532–541. [Google Scholar]
- Liguori, G.; American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2020. [Google Scholar]
- Huang, P.L. A comprehensive definition for metabolic syndrome. Dis. Models Mech. 2009, 2, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Nam, G.E.; Kim, Y.-H.; Han, K.; Jung, J.-H.; Park, Y.G.; Lee, K.-W.; Rhee, E.-J.; Son, J.W.; Lee, S.-S.; Kwon, H.-S. Obesity fact sheet in Korea, 2018: Data focusing on waist circumference and obesity-related comorbidities. J. Obes. Metab. Syndr. 2019, 28, 236–245. [Google Scholar] [CrossRef] [PubMed]
- Ostchega, Y.; Seu, R.; Isfahani, N.S.; Zhang, G.; Hughes, J.P.; Miller, I.M. Waist Circumference Measurement Methodology Study: National Health and Nutrition Examination Survey, 2016; U.S. Department of Health and Human Services: Hyattsville, MD, USA, 2019.
- Lee, J.; Lee, K.S.; Kim, H.; Jeong, H.; Choi, M.-J.; Yoo, H.-W.; Han, T.-H.; Lee, H. The relationship between metabolic syndrome and the incidence of colorectal cancer. Environ. Health Prev. Med. 2020, 25, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Han, F.; Wu, G.; Zhang, S.; Zhang, J.; Zhao, Y.; Xu, J. The association of metabolic syndrome and its components with the incidence and survival of colorectal cancer: A systematic review and meta-analysis. Int. J. Biol. Sci. 2021, 17, 487–497. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Kim, I.-H.; Lim, M.K.; Kim, Y.; Park, B. Increased prevalence of metabolic syndrome in adult cancer survivors: Asian first report in community setting. Cancer Epidemiol. 2019, 58, 130–136. [Google Scholar] [CrossRef] [PubMed]
- De Haas, E.C.; Oosting, S.F.; Lefrandt, J.D.; Wolffenbuttel, B.H.; Sleijfer, D.T.; Gietema, J.A. The metabolic syndrome in cancer survivors. Lancet Oncol. 2010, 11, 193–203. [Google Scholar] [CrossRef] [PubMed]
- da Silva Almeida, G.; de Souza, M.O.; Pereira, L.M.R.N. Relationship between omitting breakfast and late eating with obesity and metabolic disorders: A review focusing on chrononutrition. J. Arch. Health 2023, 4, 466–483. [Google Scholar] [CrossRef]
- Salas-González, M.D.; Lozano-Estevan, M.d.C.; Aparicio, A.; Bermejo, L.M.; Loria-Kohen, V.; Ortega, R.M.; López-Sobaler, A.M. Breakfast quality and insulin resistance in Spanish schoolchildren: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2023, 20, 1181. [Google Scholar] [CrossRef]
- Blom, W.A.; Stafleu, A.; de Graaf, C.; Kok, F.J.; Schaafsma, G.; Hendriks, H.F. Ghrelin response to carbohydrate-enriched breakfast is related to insulin. Am. J. Clin. Nutr. 2005, 81, 367–375. [Google Scholar] [CrossRef]
- Welton, S.; Minty, R.; O’Driscoll, T.; Willms, H.; Poirier, D.; Madden, S.; Kelly, L. Intermittent fasting and weight loss: Systematic review. Can. Fam. Physician 2020, 66, 117–125. [Google Scholar] [PubMed]
- Patterson, R.E.; Sears, D.D. Metabolic effects of intermittent fasting. Annu. Rev. Nutr. 2017, 37, 371–393. [Google Scholar] [CrossRef] [PubMed]
- Sievert, K.; Hussain, S.M.; Page, M.J.; Wang, Y.; Hughes, H.J.; Malek, M.; Cicuttini, F.M. Effect of breakfast on weight and energy intake: Systematic review and meta-analysis of randomised controlled trials. BMJ 2019, 364, l42. [Google Scholar] [CrossRef] [PubMed]
- Titan, S.M.; Bingham, S.; Welch, A.; Luben, R.; Oakes, S.; Day, N.; Khaw, K.-T. Frequency of eating and concentrations of serum cholesterol in the Norfolk population of the European prospective investigation into cancer (EPIC-Norfolk): Cross sectional study. BMJ 2001, 323, 1286. [Google Scholar] [CrossRef] [PubMed]
- Alkhulaifi, F.; Darkoh, C. Meal timing, meal frequency and metabolic syndrome. Nutrients 2022, 14, 1719. [Google Scholar] [CrossRef] [PubMed]
- Laguzzi, F.; Salleber, S.; Gigante, B.; De Faire, U.; Hellenius, M.; Leander, K. 4948 Irregular eating behavior and incidence of cardiovascular disease: Results from a Swedish 60-year-old cohort of men and women. Eur. Heart J. 2019, 40, ehz746-0018. [Google Scholar] [CrossRef]
- Pastor, R.; Bouzas, C.; Tur, J.A. Beneficial effects of dietary supplementation with olive oil, oleic acid, or hydroxytyrosol in metabolic syndrome: Systematic review and meta-analysis. Free Radic. Biol. Med. 2021, 172, 372–385. [Google Scholar] [CrossRef]
- Tsai, C.-H.; Chen, E.C.-F.; Tsay, H.-S.; Huang, C.-J. Wild bitter gourd improves metabolic syndrome: A preliminary dietary supplementation trial. Nutr. J. 2012, 11, 1–9. [Google Scholar] [CrossRef]
- Liu, S.; Willett, W.C.; Manson, J.E.; Hu, F.B.; Rosner, B.; Colditz, G. Relation between changes in intakes of dietary fiber and grain products and changes in weight and development of obesity among middle-aged women. Am. J. Clin. Nutr. 2003, 78, 920–927. [Google Scholar] [CrossRef]
- Lee, K.; Ko, D.H.; Lee, J.Y. Prevalence of metabolic syndrome according to causes of physical activity limitation. Diabetes Metab. Syndr. Obes. 2020, 13, 2455–2463. [Google Scholar] [CrossRef]
- Amin, M.; Kerr, D.; Atiase, Y.; Samir, M.M.; Driscoll, A. Improving Metabolic Syndrome in Ghanaian Adults with Type 2 Diabetes through a Home-Based Physical Activity Program: A Feasibility Randomised Controlled Trial. Int. J. Environ. Res. Public Health 2023, 20, 5518. [Google Scholar] [CrossRef] [PubMed]
- Farmanfarma, K.K.; Kaykhaei, M.A.; Adineh, H.A.; Mohammadi, M.; Dabiri, S.; Ansari-Moghaddam, A. Prevalence of metabolic syndrome in Iran: A meta-analysis of 69 studies. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 792–799. [Google Scholar] [CrossRef] [PubMed]
- Fong, D.Y.; Ho, J.W.; Hui, B.P.; Lee, A.M.; Macfarlane, D.J.; Leung, S.S.; Cerin, E.; Chan, W.Y.; Leung, I.P.; Lam, S.H. Physical activity for cancer survivors: Meta-analysis of randomised controlled trials. BMJ 2012, 344, e70. [Google Scholar] [CrossRef] [PubMed]
- Friedenreich, C.M.; Stone, C.R.; Cheung, W.Y.; Hayes, S.C. Physical activity and mortality in cancer survivors: A systematic review and meta-analysis. JNCI Cancer Spectr. 2020, 4, pkz080. [Google Scholar] [CrossRef] [PubMed]
- Micucci, C.; Valli, D.; Matacchione, G.; Catalano, A. Current perspectives between metabolic syndrome and cancer. Oncotarget 2016, 7, 38959. [Google Scholar] [CrossRef]
- Huang, D.; Shin, W.-K.; De la Torre, K.; Lee, H.-W.; Min, S.; Shin, A.; Lee, J.-K.; Kang, D. Association between metabolic syndrome and gastric cancer risk: Results from the Health Examinees Study. Gastric Cancer 2023, 26, 481–492. [Google Scholar] [CrossRef]
- Murphy, R.A. Diet, Physical Activity, and Cancer Prevention. In Nutrition Guide for Physicians and Related Healthcare Professions; Springer: Cham, Switzerland, 2022; pp. 149–158. [Google Scholar]
- Coro, D.G.; Hutchinson, A.D.; Banks, S.; Coates, A.M. Dietary Drivers and Challenges of Australian Breast Cancer Survivors: A Qualitative Study. Women’s Health Rep. 2022, 3, 563–572. [Google Scholar] [CrossRef]
- Aldossari, A.; Sremanakova, J.; Sowerbutts, A.M.; Jones, D.; Hann, M.; Burden, S.T. Do people change their eating habits after a diagnosis of cancer? A systematic review. J. Hum. Nutr. Diet. 2023, 36, 566–579. [Google Scholar] [CrossRef]


{kind=link}
| Variables | NC (n = 11,673) | p | CS (n = 1003) | p | ||
|---|---|---|---|---|---|---|
| NMetS (n = 7351) | MetS (n = 4322) | NMetS (n = 583) | MetS (n = 420) | |||
| NMetS or MetS, % | 63.0% | 37.0% | 58.1 | 41.9% | ||
| Age, years | 57.9 ± 10.9 | 63.6 ± 9.1 | <0.001 | 58.5 ± 10.6 | 65.8 ± 9.9 | <0.001 |
| Height, cm | 156.5 ± 6.2 | 153.8 ± 5.8 | <0.001 | 156.6 ± 6.0 | 154.9 ± 5.9 | <0.001 |
| Weight, kg | 55.7 ± 7.6 | 60.9 ± 9.0 | <0.001 | 55.4 ± 8.0 | 61.7 ± 9.2 | <0.001 |
| BMI, kg/m2 | 22.7 ± 2.7 | 25.7 ± 3.3 | <0.001 | 22.5 ± 2.8 | 25.7 ± 3.2 | <0.001 |
| WC, cm | 77.4 ± 7.6 | 87.6 ± 8.2 | <0.001 | 77.4 ± 7.3 | 87.6 ± 8.2 | <0.001 |
| SBP, mmHg | 116.2 ± 16.6 | 130.6 ± 16.7 | <0.001 | 117.2 ± 17.2 | 128.3 ± 16.1 | <0.001 |
| DBP, mmHg | 73.7 ± 9.1 | 75.7 ± 10.2 | <0.001 | 73.5 ± 8.7 | 76.1 ± 9.7 | <0.001 |
| HDL, mg/dL | 57.6 ± 12.2 | 46.6 ± 10.1 | <0.001 | 57.5 ± 12.2 | 46.4 ± 10.0 | <0.001 |
| TG, mg/dL | 98.3 ± 50.5 | 160.2 ± 96.3 | <0.001 | 96.8 ± 43.8 | 159.9 ± 84.0 | <0.001 |
| Glucose, mg/dL | 94.3 ± 13.9 | 113.2 ± 29.8 | <0.001 | 95.2 ± 17.2 | 111.2 ± 26.3 | <0.001 |
| Household income | ||||||
| High | 3771 (51.3%) | 2018 (46.7%) | <0.001 | 312 (53.5%) | 187 (44.6%) | <0.001 |
| Medium | 1286 (17.5%) | 821 (19.0%) | 92 (15.8%) | 74 (17.5%) | ||
| Low | 2294 (31.2%) | 1482 (34.3%) | 179 (30.7%) | 159 (37.9%) | ||
| School | ||||||
| Middle school | 897 (12.2%) | 562 (13.0%) | 0.410 | 86 (14.7%) | 60 (14.2%) | 0.459 |
| High school | 3359 (45.7%) | 2036 (47.1%) | 282 (48.3%) | 201 (47.9%) | ||
| College | 3095 (42.1%) | 1724 (39.9%) | 216 (37.0%) | 159 (37.9%) | ||
| Smoking | ||||||
| Current | 221 (3.0%) | 186 (4.3%) | 0.007 | 20 (3.5%) | 13 (3.2%) | 0.373 |
| Stopping | 257 (3.5%) | 190 (4.4%) | 41 (7.1%) | 36 (8.6%) | ||
| Never | 6873 (93.5%) | 3946 (91.3%) | 521 (89.4%) | 370 (88.2%) | ||
| Alcohol | ||||||
| Low | 4359 (59.3%) | 2282 (52.8%) | <0.001 | 374 (64.1%) | 247 (58.8%) | <0.001 |
| Medium | 1742 (23.7%) | 1145 (26.5%) | 134 (22.9%) | 103 (24.5%) | ||
| High | 1250 (17.0%) | 895 (20.7%) | 76 (13.0%) | 70 (16.7%) | ||
| Survivor year | ||||||
| 1–5 | - | - | 273 (40.9%) | 131 (39.1%) | 0.054 | |
| 6–10 | - | - | 187 (28.0%) | 96 (28.7%) | ||
| 11–20 | - | - | 208 (31.1%) | 108 (32.2%) | ||
| Cancer number | ||||||
| 1 | - | - | - | 562 (96.4%) | 396 (94.3%) | 0.178 |
| 2 | - | - | - | 21 (3.6%) | 23 (5.5%) | |
| 3 | - | - | - | 0 (0.0%) | 1 (0.2%) | |
| NC | Total (n = 1003) | Stomach (n = 111) | Colorectal (n = 80) | Breast (n = 229) | Cervical (n = 190) | Lung (n = 17) | Thyroid (n = 301) | Other (n = 120) | |
|---|---|---|---|---|---|---|---|---|---|
| MetS | 1.00 (ref) | 1.22 (1.07–1.39) | 0.98 (0.69–1.45) | 1.77 (1.14–2.74) | 0.99 (0.75–1.29) | 1.72 (1.29–2.30) | 3.07 (1.14–5.31) | 1.02 (0.89–1.29) | 1.45 (1.01–2.07) |
| WC | 1.00 (ref) | 1.10 (0.97–1.26) | 0.67 (0.43–1.02) | 1.64 (1.05–2.55) | 0.92 (0.70–1.22) | 1.33 (1.01–1.78) | 2.14 (0.82–5.54) | 1.16 (0.92–1.47) | 1.17 (0.81–1.69) |
| BP | 1.00 (ref) | 1.09 (0.96–1.24) | 1.27 (0.99–2.14) | 1.8 (1.14–2.83) | 0.83 (0.64–1.08) | 1.39 (1.04–1.86) | 3.02 (1.44–5.49) | 0.91 (0.72–1.14) | 1.06 (0.74–1.51) |
| HDL | 1.00 (ref) | 1.16 (1.02–1.32) | 1.17 (0.80–1.70) | 1.34 (0.87–2.09) | 0.81 (0.62–1.06) | 1.62 (1.21–2.16) | 1.13 (0.44–2.94) | 1.07 (0.85–1.34) | 1.44 (1.01–2.06) |
| TG | 1.00 (ref) | 1.14 (1.00–1.30) | 0.84 (0.57–1.25) | 1.55 (1.00–2.40) | 0.99 (0.76–1.30) | 1.41 (1.05–1.87) | 1.44 (0.56–3.74) | 1.05 (0.83–1.32) | 1.31 (0.91–1.88) |
| GLU | 1.00 (ref) | 1.15 (1.01–1.31) | 0.95 (0.65–1.40) | 1.08 (0.69–1.69) | 1.07 (0.82–1.40) | 1.44 (1.08–1.92) | 2.98 (1.10–7.06) | 1.06 (0.84–1.34) | 1.45 (1.01–2.08) |
| Variables | NC | OR (95%CI) | CS | OR (95%CI) | ||
|---|---|---|---|---|---|---|
| NMetS (n = 7351) | MetS (n = 4322) | NMetS (n = 583) | MetS (n = 420) | |||
| Calorie intake | ||||||
| Low | 3367 (45.8%) | 1733 (40.1%) | 0.74 (0.68–0.81) | 255 (43.7%) | 166 (39.6%) | 0.77 (0.56–1.05) |
| Recommended | 2323 (31.6%) | 1366 (31.6%) | Reference | 143 (24.5%) | 97 (23.1%) | Reference |
| High | 1661 (22.6%) | 1223 (28.3%) | 1.43 (1.09–1.79) | 185 (31.8%) | 157 (37.3%) | 1.31 (1.02–1.89) |
| Three meals per day | ||||||
| High | 4586 (62.4%) | 3252 (75.2%) | Reference | 430 (69.1%) | 314 (74.8%) | Reference |
| Low | 2765 (37.6%) | 1070 (24.8%) | 1.83 (1.68–1.99) | 180 (30.9%) | 106 (25.2%) | 1.32 (1.03–1.75) |
| Eating out frequency | ||||||
| Low | 5418 (73.7%) | 3177 (73.5%) | Reference | 511 (87.7%) | 316 (75.2%) | Reference |
| Medium | 1110 (15.1%) | 514 (11.9%) | 1.01 (0.69–1.07) | 39 (6.7%) | 51 (12.2%) | 1.25 (1.03–1.52) |
| High | 823 (11.2%) | 631 (14.6%) | 1.11 (1.01–1.64) | 33 (5.6%) | 53 (12.6%) | 2.65 (2.29–3.07) |
| Breakfast frequency | ||||||
| High, | 5888 (80.1%) | 3380 (78.2%) | Reference | 513 (88%) | 305 (72.6%) | Reference |
| Medium | 750 (10.2%) | 445 (10.3%) | 1.02 (0.54–1.25) | 33 (5.6%) | 39 (9.4%) | 1.66 (1.36–2.02) |
| Low | 713 (9.7%) | 497 (11.5%) | 1.17 (0.77–1.76) | 37 (6.4%) | 76 (18%) | 3.37 (2.95–3.86) |
| Diet supplement | ||||||
| Yes | 4661 (63.4%) | 2775 (64.2%) | Reference | 461 (79.1%) | 342 (81.4%) | Reference |
| No | 2690 (36.6%) | 1547 (35.8%) | 0.88 (0.72–1.02) | 122 (20.9%) | 78 (18.6%) | 1.09 (0.74–2.35) |
| Diet therapy | ||||||
| Yes | 2411 (32.8%) | 1405 (32.5%) | Reference | 183 (31.4%) | 113 (26.9%) | Reference |
| No | 4940 (67.2%) | 2917 (67.5%) | 1.01 (0.77–1.32) | 400 (68.6%) | 307 (73.1%) | 1.24 (1.05–1.85) |
| Nutrition education | ||||||
| Yes | 515 (7.0%) | 229 (5.3%) | Reference | 47 (8.1%) | 32 (7.5%) | Reference |
| No | 6836 (93.0%) | 4093 (94.7%) | 1.36 (1.17–1.59) | 536 (91.9%) | 389 (92.5%) | 1.28 (1.08–2.36) |
| NC | OR (95%CI) | CS | OR (95%CI) | |||
|---|---|---|---|---|---|---|
| Variables | NMetS (n = 7351) | MetS (n = 4322) | NMetS (n = 583) | MetS (n = 420) | ||
| Aerobic PA | ||||||
| High | 1775 (24.2%) | 921 (21.3%) | 0.98 (0.79–1.14) | 244 (36.6%) | 102 (30.5%) | 0.88 (0.67–0.98) |
| Recommended level | 3082 (41.9%) | 1616 (37.4%) | Reference | 224 (33.5%) | 105 (31.3%) | Reference |
| Low | 2494 (33.9%) | 1785 (41.3%) | 1.37 (1.13–1.71) | 200 (29.9%) | 128 (38.2%) | 1.36 (1.10–1.87) |
| Strength PA | ||||||
| High | 860 (11.7%) | 454 (10.5%) | 0.92 (0.74–2.01) | 57 (8.6%) | 19 (5.7%) | 0.78 (0.52–0.96) |
| Recommended level | 515 (7.0%) | 294 (6.8%) | Reference | 45 (6.7%) | 23 (6.8%) | Reference |
| No | 5976 (81.3%) | 3574 (82.7%) | 1.36 (1.08–1.70) | 566 (84.7%) | 293 (87.5%) | 1.49 (1.07–2.57) |
| Sedentary time | ||||||
| Low | 3279 (44.6%) | 1539 (35.6%) | Reference | 268 (40.1%) | 139 (41.5%) | Reference |
| Medium | 2744 (37.3%) | 1595 (36.9%) | 1.24 (1.04–1.45) | 256 (38.3%) | 108 (32.2%) | 1.24 (0.91–1.79) |
| High | 1328 (18.1%) | 1188 (27.5%) | 1.90 (1.23–3.10) | 144 (21.6%) | 88 (26.3%) | 1.85 (1.39–2.91) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, P.; Kim, Y.; Lee, J. Prevalence of Metabolic Syndrome Based on the Dietary Habits and Physical Activity of Korean Women Cancer Survivors. Foods 2023, 12, 3554. https://doi.org/10.3390/foods12193554
Zhou P, Kim Y, Lee J. Prevalence of Metabolic Syndrome Based on the Dietary Habits and Physical Activity of Korean Women Cancer Survivors. Foods. 2023; 12(19):3554. https://doi.org/10.3390/foods12193554
Chicago/Turabian StyleZhou, Peng, Yonghwan Kim, and Jiseol Lee. 2023. "Prevalence of Metabolic Syndrome Based on the Dietary Habits and Physical Activity of Korean Women Cancer Survivors" Foods 12, no. 19: 3554. https://doi.org/10.3390/foods12193554
APA StyleZhou, P., Kim, Y., & Lee, J. (2023). Prevalence of Metabolic Syndrome Based on the Dietary Habits and Physical Activity of Korean Women Cancer Survivors. Foods, 12(19), 3554. https://doi.org/10.3390/foods12193554