
An Evaluation of a Virtual Food Safety Program for Low-Income Families: Applying the Theory of Planned Behavior


Abstract
:1. Introduction
2. Materials and Methods
2.1. Survey Design
- The knowledge constructs were adapted from Barrett et al. [17], and the TPB constructs were developed based on Ajzen’s guidelines for developing the TPB questionnaire [33]. The knowledge section included eight multiple-choice questions evaluating participants’ knowledge of (a) recommended handwashing, (b) chilling, and (c) storage practices, as well as (d) recommended meat cooking temperatures and refrigerator temperatures.
- The attitudes toward the behavior construct included seven questions measuring participants’ attitudes toward the core four food safety practices (clean, separate, cook, and chill), the importance of participants’ children washing their hands, and the risk of their children contracting foodborne illness.
- The PBC construct contained seven questions measuring participants’ confidence in their ability to comply with the core four food safety practices, ensure their children washed their hands, and prepare safe foods for their children.
- The subjective norms construct had eight questions measuring the perceived beliefs of participants’ family and friends on the core four food safety practices, the importance of ensuring the handwashing practices of participants’ children, participants’ children’s risk of contracting foodborne illnesses, and the ability of participants to prepare safe foods for their children.
- The behavior change intentions construct included six questions evaluating participants’ intentions to adopt the core four food safety practices, ensure participants’ children washed their hands, and follow recommended practices to prepare safe foods for their children.
- The self-reported safe food practice behaviors had seven questions evaluating participants’ current compliance with the core four food safety practices and ensuring participants’ children washed their hands.
2.2. Participant Recruitment
2.3. Procedure
2.4. Data Analysis
3. Results and Discussion
3.1. Sociodemographic Characteristics
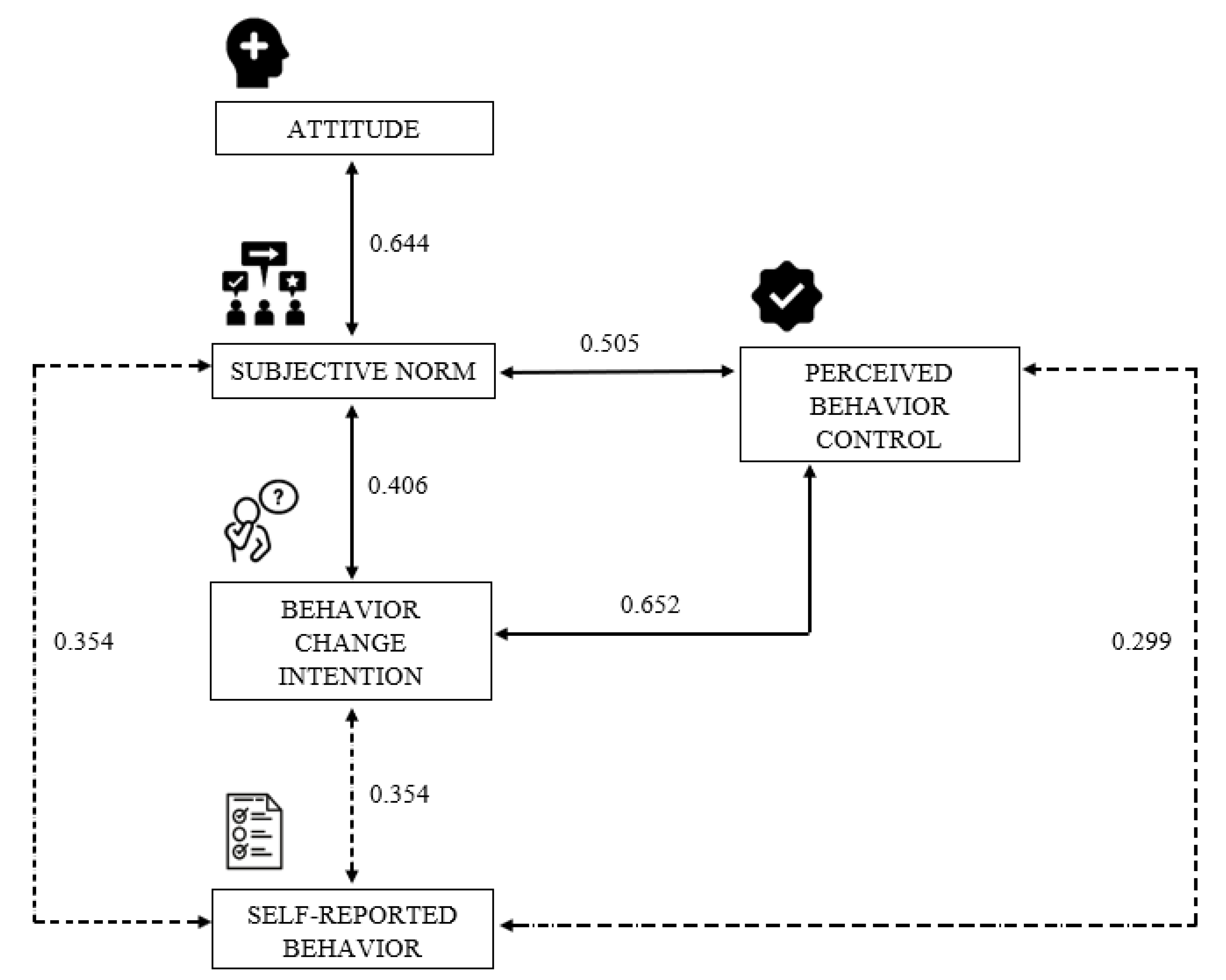
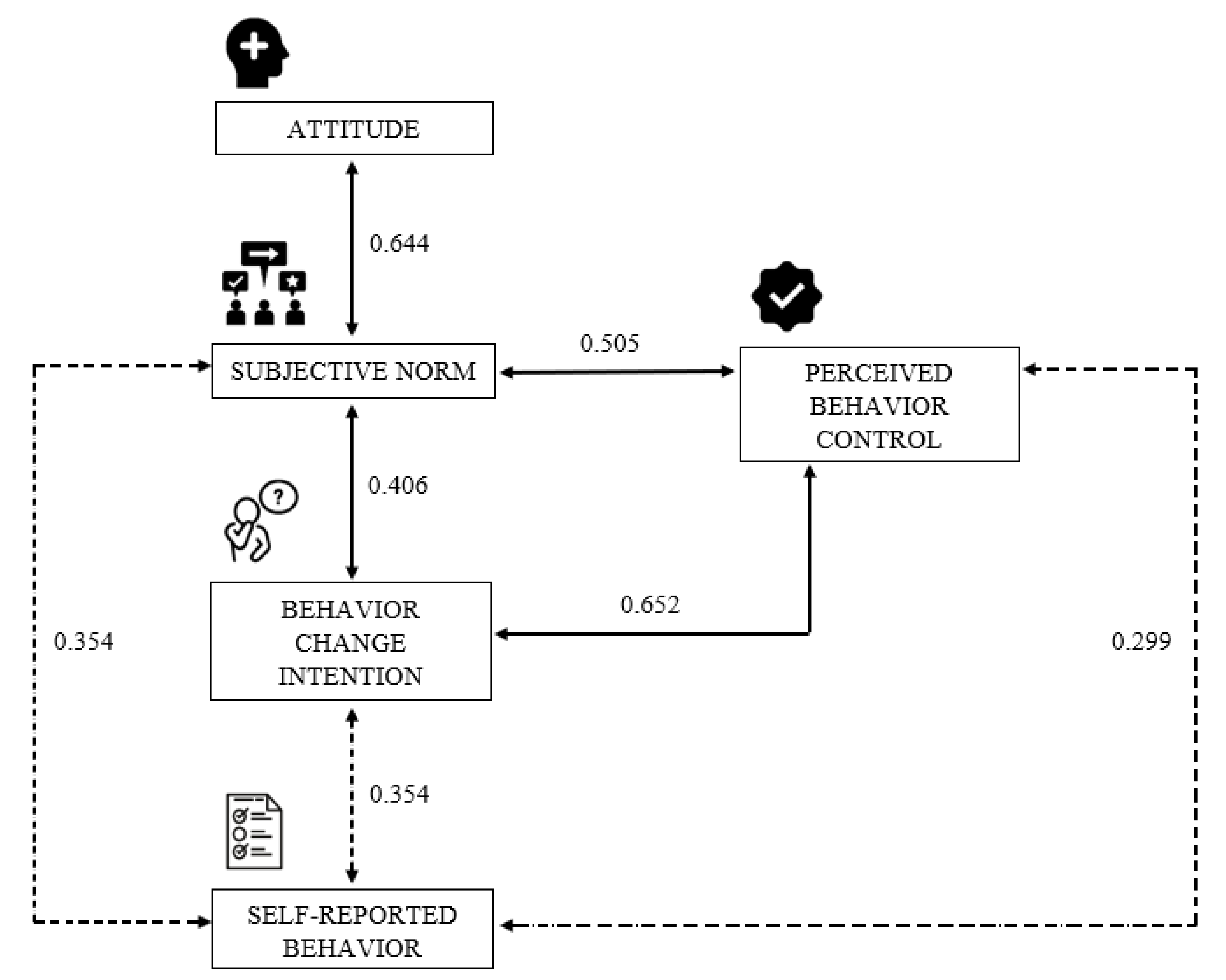
3.2. Theory of Planned Behavior
3.3. Knowledge Assessment
3.4. Differences between English and Spanish participants
3.5. Dialogue-Based Program Evaluation
3.6. Advantages of the Virtual Program for Low-Income Families
4. Limitations and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Center for Disease Control and Prevention. Foodborne Germs and Illnesses. Available online: https://www.cdc.gov/foodsafety/foodborne-germs.html (accessed on 17 May 2021).
- Center for Disease Control and Prevention. People with a Higher Risk of Food Poisoning. Available online: https://www.cdc.gov/foodsafety/people-at-risk-food-poisoning.html (accessed on 11 September 2021).
- Quinlan, J.J. Foodborne illness incidence rates and food safety risks for populations of low socioeconomic status and minority race/ethnicity: A review of the literature. Int. J. Environ. Res. Public Health 2013, 10, 3634–3652. [Google Scholar] [CrossRef] [PubMed]
- Creamer, J. Inequalities Persist Despite Decline in Poverty for All Major Race and Hispanic Origin Groups. Available online: https://www.census.gov/library/stories/2020/09/poverty-rates-for-blacks-and-hispanics-reached-historic-lows-in-2019.html (accessed on 17 May 2021).
- Zenk, S.N.; Schulz, A.J.; Israel, B.A.; James, S.A.; Bao, S.; Wilson, M.L. Neighborhood racial composition, neighborhood poverty, and the spatial accessibility of supermarkets in metropolitan Detroit. Am. J. Public Health 2005, 95, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Henley, S.C.; Stein, S.E.; Quinlan, J.J. Identification of unique food handling practices that could represent food safety risks for minority consumers. J. Food Prot. 2012, 75, 2050–2054. [Google Scholar] [CrossRef] [PubMed]
- Koro, M.E.; Anandan, S.; Quinlan, J.J. Microbial quality of food available to populations of differing socioeconomic status. Am. J. Prev. Med. 2010, 38, 478–481. [Google Scholar] [CrossRef] [PubMed]
- Darcey, V.L.; Quinlan, J.J. Use of geographic information systems technology to track critical health code violations in retail facilities available to populations of different socioeconomic status and demographics. J. Food Prot. 2011, 74, 1524–1530. [Google Scholar] [CrossRef]
- Jackson, K.A.; Gould, L.H.; Hunter, J.C.; Kucerova, Z.; Jackson, B. Listeriosis outbreaks associated with soft cheeses, United States, 1998–2014. Emerg. Infect. Dis. 2018, 24, 1116. [Google Scholar] [CrossRef]
- Lee, L.A.; Gerber, A.R.; Lonsway, D.R.; Smith, J.D.; Carter, G.P.; Puhr, N.D.; Parrish, C.M.; Sikes, R.K.; Finton, R.J.; Tauxe, R.V. Yersinia enterocolitica O: 3 infections in infants and children, associated with the household preparation of chitterlings. N. Engl. J. Med. 1990, 322, 984–987. [Google Scholar] [CrossRef]
- Bermudez-Millan, A.; Perez-Escamilla, R.; Damio, G.; Gonzalez, A.; Segura-Perez, S. Food safety knowledge, attitudes, and behaviors among Puerto Rican caretakers living in Hartford, Connecticut. J. Food Prot. 2004, 67, 512–516. [Google Scholar] [CrossRef]
- Kwon, J.; Wilson, A.N.; Bednar, C.; Kennon, L. Food safety knowledge and behaviors of women, infant, and children (WIC) program participants in the United States. J. Food Prot. 2008, 71, 1651–1658. [Google Scholar] [CrossRef] [Green Version]
- Trepka, M.J.; Murunga, V.; Cherry, S.; Huffman, F.G.; Dixon, Z. Food safety beliefs and barriers to safe food handling among WIC program clients, Miami, Florida. J. Nutr. Educ. Behav. 2006, 38, 371–377. [Google Scholar] [CrossRef]
- Milton, A.; Mullan, B. Consumer food safety education for the domestic environment: A systematic review. Br. Food J. 2010. 112, 1003–1022. [CrossRef] [Green Version]
- Henley, S. Kitchen Kaizen: Preliminary Findings of a Hands-on Consumer Food Safety Workshop. In Proceedings of the International Association of Food Protection Annual Meeting, Lousiville, KY, USA, 22 July 2019. [Google Scholar]
- Yardley, L.; Miller, S.; Schlotz, W.; Little, P. Evaluation of a Web-based intervention to promote hand hygiene: Exploratory randomized controlled trial. J. Med. Internet Res. 2011, 13, e107. [Google Scholar] [CrossRef] [PubMed]
- Barrett, T.; Feng, Y.; Chen, H.; Chuang, E.; Feist, S.; Choate, M. Evaluation of the Fight BAC! The Story of Your Dinner Campaign video: A multistate study. J. Food Prot. 2020, 83, 584–598. [Google Scholar] [CrossRef] [PubMed]
- Losasso, C.; Cibin, V.; Cappa, V.; Roccato, A.; Vanzo, A.; Andrighetto, I.; Ricci, A. Food safety and nutrition: Improving consumer behaviour. Food Control 2012, 26, 252–258. [Google Scholar] [CrossRef]
- Sivaramalingam, B.; Young, I.; Pham, M.T.; Waddell, L.; Greig, J.; Mascarenhas, M.; Papadopoulos, A. Scoping review of research on the effectiveness of food-safety education interventions directed at consumers. Foodborne Pathog. Dis. 2015, 12, 561–570. [Google Scholar] [CrossRef]
- Takeuchi, M.T.; Edlefsen, M.; McCurdy, S.M.; Hillers, V.N. Educational intervention enhances consumers’ readiness to adopt food thermometer use when cooking small cuts of meat: An application of the Transtheoretical Model. J. Food Prot. 2005, 68, 1874–1883. [Google Scholar] [CrossRef]
- Henley, S.C.; Gleason, J.; Quinlan, J.J. Don’t wash your chicken!: A food safety education campaign to address a common food mishandling practice. Food Prot. Trends 2016, 36, 43–53. [Google Scholar]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Ajzen, I.; Cote, N.G. Attitudes and the prediction of behavior. In Attitudes and Attitude Change; Crano, W.D., Prislin, R., Eds.; Psychology Press: New York, NY, USA, 2008; pp. 289–311. [Google Scholar]
- Husain, N.R.N.; Muda, W.M.W.; Jamil, N.I.N.; Hanafi, N.N.N.; Rahman, R.A. Effect of food safety training on food handlers’ knowledge and practices: A randomized controlled trial. Br. Food J. 2016, 118, 795–808. [Google Scholar] [CrossRef]
- Shapiro, M.A.; Porticella, N.; Jiang, L.C.; Gravani, R.B. Predicting intentions to adopt safe home food handling practices. Applying the theory of planned behavior. Appetite 2011, 56, 96–103. [Google Scholar] [CrossRef]
- Milton, A.C.; Mullan, B.A. An application of the theory of planned behavior—A randomized controlled food safety pilot intervention for young adults. Health Psychol. 2012, 31, 250–259. [Google Scholar] [CrossRef] [Green Version]
- Mullan, B.A.; Wong, C.; Kothe, E.J. Predicting adolescents’ safe food handling using an extended theory of planned behavior. Food Control 2013, 31, 454–460. [Google Scholar] [CrossRef] [Green Version]
- Pampel, F.C.; Krueger, P.M.; Denney, J.T. Socioeconomic disparities in health behaviors. Annu. Rev. Sociol. 2010, 36, 349–370. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.; Archila-Godínez, J.C.; Klinestiver, L.; Rosa, L.; Barrett, T.; Zabala, V.; Feng, Y. Development of a virtual food safety program for low-income families with young children: A dialogue-based learning approach. J. Food Prot. 2021. submitted. [Google Scholar]
- Sanford, R.C. Caring through relation and dialogue: A nursing perspective for patient education. Adv. Nur. Sci. 2000, 22, 1–15. [Google Scholar] [CrossRef]
- Feng, Y.; Bruhn, C.; Health Management and Education. Food safety education for people with diabetes and pregnant women: A positive deviance approach. Food Control 2016, 66, 107–115. [Google Scholar] [CrossRef] [Green Version]
- Jensen, N.K.; Pals, R.A.; Willaing, I. The use of dialogue tools to promote dialogue-based and person-centred patient education for people with type 2 diabetes. Chronic Illn. 2016, 12, 145–156. [Google Scholar] [CrossRef]
- Ajzen, I. Constructing a Theory of Planned Behavior Questionnaire. Available online: https://www.researchgate.net/publication/235913732_Constructing_a_Theory_of_Planned_Behavior_Questionnaire (accessed on 12 September 2021).
- Taber, K.S. The use of Cronbach’s alpha when developing and reporting research instruments in science education. Res. Sci. Educ. 2018, 48, 1273–1296. [Google Scholar] [CrossRef]
- Department of Housing and Urban Development’s Office of Policy Development and Research. Tables for Section 8 Income Limits. Available online: https://www.huduser.gov/portal/datasets/il/il19/Section8-IncomeLimits-FY19.pdf (accessed on 1 April 2021).
- Smith, L.; Sirsat, S.A.; Neal, J.A. Does food safety training for non-profit food service volunteers improve food safety knowledge and behavior. Food Prot. Trends 2014, 34, 156–163. [Google Scholar]
- Gold, A.; Yu, N.; Buro, B.; Garden-Robinson, J. Discussion Map and Cooking Classes: Testing the effectiveness of teaching food safety to immigrants and refugees. J. Nutr. Educ. Behav. 2014, 46, 547–553. [Google Scholar] [CrossRef]
- King, A.; Eckersley, R. Chapter 5. Inferential statistics II: Parametric hypothesis testing. Stat. Biomed. Eng. Sci. 2019, 91–117. [Google Scholar] [CrossRef]
- Pathak, R.P. Chapter 3. Significance of diference of means. In Statistics in Education and Psychology; Pearson Education: Noida, India, 2011. [Google Scholar]
- Akoglu, H. User’s guide to correlation coefficients. Turk. J. Emerg. Med. 2018, 18, 91–93. [Google Scholar] [CrossRef]
- Taillie, L.S. Who’s cooking? Trends in US home food preparation by gender, education, and race/ethnicity from 2003 to 2016. Nutr. J. 2018, 17, 41. [Google Scholar] [CrossRef] [Green Version]
- Flagg, L.A.; Sen, B.; Kilgore, M.; Locher, J.L. The influence of gender, age, education and household size on meal preparation and food shopping responsibilities. Public Health Nutr. 2014, 17, 2061–2070. [Google Scholar] [CrossRef] [Green Version]
- Miller, A.J.; Carlson, D.L. Great expectations? Working-and middle-class cohabitors’ expected and actual divisions of housework. J. Marriage Fam. 2016, 78, 346–363. [Google Scholar] [CrossRef]
- Dudeja, P.; Singh, A.; Sahni, N.; Kaur, S.; Goel, S. Effectiveness of an intervention package on knowledge, attitude, and practices of food handlers in a tertiary care hospital of north India: A before and after comparison study. Med. J. Armed Forces India 2017, 73, 49–53. [Google Scholar] [CrossRef] [Green Version]
- Barrett, T.; Feng, Y. Evaluation of food safety curriculum effectiveness: A longitudinal study of high-school-aged youths’ knowledge retention, risk-perception, and perceived behavioral control. Food Control 2021, 121, 107587. [Google Scholar] [CrossRef]
- Diplock, K.J.; Jones-Bitton, A.; Leatherdale, S.T.; Rebellato, S.; Hammond, D.; Majowicz, S.E. Food safety education needs of high-school students: Leftovers, lunches, and microwaves. J. Sch. Health 2019, 89, 578–586. [Google Scholar] [CrossRef]
- Yiannas, F. Make food safety the social norm. In Food Safety = Behavior: 30 Proven Techniques to Enhance Employee Compliance; Yiannas, F., Ed.; Springer: New York, NY, USA, 2016; pp. 31–33. [Google Scholar]
- Mullan, B.; Wong, C. Using the Theory of Planned Behaviour to design a food hygiene intervention. Food Control 2010, 21, 1524–1529. [Google Scholar] [CrossRef] [Green Version]
- Hajivandi, L.; Noroozi, M.; Mostafavi, F.; Ekramzadeh, M. Assessing the impact of an educational intervention program based on the theory of planned behavior on the nutritional behaviors of adolescents and young adults with PCOS in Iran: A field trial study. BMC Pediatr. 2021, 21, 316. [Google Scholar] [CrossRef]
- Taghdis, M.H.; Babazadeh, T.; Moradi, F.; Shariat, F. Effect of educational intervention on the fruit and vegetables consumption among the students: Applying theory of planned behavior. J. Res. Health Sci. 2016, 16, 195–199. [Google Scholar]
- Zhang, J.; Shi, L.; Chen, D.; Wang, J.; Wang, Y. Using the theory of planned behavior to examine effectiveness of an educational intervention on infant feeding in China. Prev. Med. 2009, 49, 529–534. [Google Scholar] [CrossRef]
- Stenger, K.M.; Ritter-Gooder, P.K.; Perry, C.; Albrecht, J.A. A mixed methods study of food safety knowledge, practices and beliefs in Hispanic families with young children. Appetite 2014, 83, 194–201. [Google Scholar] [CrossRef] [Green Version]
- Feng, Y.; Bruhn, C. Motivators and barriers to cooking and refrigerator thermometer use among consumers and food workers: A review. J. Food Prot. 2019, 82, 128–150. [Google Scholar] [CrossRef]
- Elshahat, S.; Woodside, J.V.; McKinley, M.C. Meat thermometer usage amongst European and North American consumers: A scoping review. Food Control 2019, 106, 106692. [Google Scholar] [CrossRef]
- James, C.; Onarinde, B.A.; James, S.J. The use and performance of household refrigerators: A review. Compr. Rev. Food Sci. Food Saf. 2017, 16, 160–179. [Google Scholar] [CrossRef]
- Koidis, T.; Cairnduff, V.; Dean, M. A Study of Domestic Fridges on Island of Ireland. Available online: https://www.safefood.net/research-reports/domestic-fridges-ireland (accessed on 29 August 2021).
- Towns, R.E.; Cullen, R.W.; Memken, J.A.; Nnakwe, N.E. Food safety–related refrigeration and freezer practices and attitudes of consumers in Peoria and surrounding counties. J. Food Prot. 2006, 69, 1640–1645. [Google Scholar] [CrossRef]
- Borrusso, P.A.; Henley, S.; Quinlan, J.J. Visual audit of food safety hazards present in homes in an urban environment. Food Prot. Trends 2015, 35, 290–301. [Google Scholar]
- Feng, Y.; Bruhn, C.; Marx, D. Evaluation of different food safety education interventions. Br. Food J. 2016, 118, 762–776. [Google Scholar] [CrossRef]
- Partnership for Food Safety Education. The Core Four Practices. Available online: https://www.fightbac.org/food-safety-basics/the-core-four-practices/ (accessed on 15 August 2021).
- U.S. Food & Drug Administration. Food Safety at Home. Available online: https://www.fda.gov/consumers/free-publications-women/food-safety-home (accessed on 18 May 2021).
- Ajzen, I. The theory of planned behavior: Frequently asked questions. Hum. Behav. Emerg. Technol. 2020, 2, 314–324. [Google Scholar] [CrossRef]
- Maxwell, S.E. Sample size and multiple regression analysis. Psychol. Methods 2000, 5, 434–458. [Google Scholar] [CrossRef]
- Clayton, D.A.; Griffith, C.J. Efficacy of an extended theory of planned behaviour model for predicting caterers’ hand hygiene practices. Int. J. Environ. Health Res. 2008, 18, 83–98. [Google Scholar] [CrossRef]
- Soon, J.; Baines, R. Food safety training and evaluation of handwashing intention among fresh produce farm workers. Food Control 2012, 23, 437–448. [Google Scholar] [CrossRef]
- Lin, N.; Roberts, K.R. Using the theory of planned behavior to predict food safety behavioral intention: A systematic review and meta-analysis. Int. J. Hosp. Manag. 2020, 90, 102612. [Google Scholar] [CrossRef]
- Egan, M.; Raats, M.; Grubb, S.; Eves, A.; Lumbers, M.; Dean, M.; Adams, M. A review of food safety and food hygiene training studies in the commercial sector. Food Control 2007, 18, 1180–1190. [Google Scholar] [CrossRef]
- Yeung, H.F.; Bruhn, C.; Blackburn, M.; Ganthavorn, C.; Martin, A.; Mendoza, C.; Neelon, M.; Smith, D.; Soule, K.; Spezzano, T.M.; et al. Evaluation of in-person and on-line food safety education programs for community volunteers. Food Control 2019, 99, 34–39. [Google Scholar] [CrossRef]
- Medeiros, L.; Hillers, V.; Kendall, P.; Mason, A. Evaluation of food safety education for consumers. J. Nutr. Educ. 2001, 33, S27–S34. [Google Scholar] [CrossRef]
- Nieto-Montenegro, S.; Brown, J.L.; LaBorde, L.F. Development and assessment of pilot food safety educational materials and training strategies for Hispanic workers in the mushroom industry using the Health Action Model. Food Control 2008, 19, 616–633. [Google Scholar] [CrossRef]
- Liu, P. Food safety knowledge and practice in low-income families in the United States: An exploratory study. Food Prot. Trends 2020, 40, 80–94. [Google Scholar]
- Wenrich, T.; Cason, K.; Lv, N.; Kassab, C. Food safety knowledge and practices of low income adults in Pennsylvania. Food Prot. Trends 2003, 23. Available online: https://agris.fao.org/agris-search/search.do?recordID=US201400167450 (accessed on 15 December 2021).
- Panchal, P.K.; Liu, L.; Dworkin, M.S. Food safety knowledge is lower among Spanish-speaking than among English-speaking restaurant food handlers in Chicago. Food Prot. Trends 2012, 32, 16–25. [Google Scholar]
- Brown, L.G.; Le, B.; Wong, M.R.; Reimann, D.; Nicholas, D.; Faw, B.; Davis, E.; Selman, C.A. Restaurant manager and worker food safety certification and knowledge. Foodborne Pathog. Dis. 2014, 11, 835–843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hann, K.E.; Freeman, M.; Fraser, L.; Waller, J.; Sanderson, S.C.; Rahman, B.; Side, L.; Gessler, S.; Lanceley, A. Awareness, knowledge, perceptions, and attitudes towards genetic testing for cancer risk among ethnic minority groups: A systematic review. BMC Public Health 2017, 17, 503. [Google Scholar] [CrossRef]
- Bai, L.; Tang, J.; Yang, Y.; Gong, S. Hygienic food handling intention. An application of the Theory of Planned Behavior in the Chinese cultural context. Food Control 2014, 42, 172–180. [Google Scholar] [CrossRef]
- Li, J.; Zhang, X.-A.; Sun, G. Effects of “face” consciousness on status consumption among Chinese consumers: Perceived social value as a mediator. Psychol. Rep. 2015, 116, 280–291. [Google Scholar] [CrossRef]
- Landale, N.S.; Oropesa, R.S.; Bradatan, C. Hispanic Families in the United States: Family Structure and Process in an Era of Family Change; National Academies Press: Washington, DC, USA, 2006; pp. 138–178. [Google Scholar]
- American Psychological Association. APA Dictionary of Psychology. Available online: https://dictionary.apa.org/familism (accessed on 9 September 2021).
- Vella, J. On Teaching and Learning: Putting the Principles and Practices of Dialogue Education into Action; Jossey-Bass: San Francisco, CA, USA, 2008. [Google Scholar]
- Smith, J.M.; Hayes, R. Integrating philosophy, sociology, and dialog-based instruction in the social & criminal justice classroom. Contemp. Justice Rev. 2016, 19, 3–18. [Google Scholar] [CrossRef]
- Witschel, H.F.; Diwanji, P.; Hinkelmann, K. A Dialog-Based Tutoring System for Project-Based Learning in Information Systems Education; Springer International Publishing: Cham, Switzerland, 2020; pp. 81–95. [Google Scholar]
- Afzal, S.; Dhamecha, T.; Mukhi, N.; Sindhgatta Rajan, R.; Marvaniya, S.; Ventura, M.; Yarbro, J. Development and deployment of a large-scale dialog-based intelligent tutoring system. In Proceedings of the Conference of the North American Chapter of the Association for Computational Linguistics: Human Language Technologies, Minneapolis, MN, USA, 2–7 June 2019; Association for Computational Linguistics: Stroudsburg, PA, USA, 2019. [Google Scholar]
- Wambsganss, T.; Kueng, T.; Soellner, M.; Leimeister, J.M. ArgueTutor: An adaptive dialog-based learning system for argumentation skills. In Proceedings of the Conference on Human Factors in Computing Systems, Yokohama, Japan, 8–13 May 2021; ACM Digital Library: New York, NY, USA, 2021. [Google Scholar]
- Csapo, N.; Hayen, R. The role of learning styles in the teaching/learning process. Issues Inf. Syst. 2006, 7, 129–133. [Google Scholar]
- Clemons, S.A. Developing on-line courses for visual/kinesthetic learners: A case study. Int. J. Instr. Technol. Distance Learn. 2004, 1, 51. [Google Scholar]
- Craig, M.A.; Richeson, J.A. Hispanic population growth engenders conservative shift among non-Hispanic racial minorities. Soc. Psychol. Pers. Sci. 2018, 9, 383–392. [Google Scholar] [CrossRef] [Green Version]
- Beary, M.A.; DiCaprio, E.; Feng, Y.; Chang, E.; Dunn, L.L.; Padilla-Zakour, O.I.; Snyder, A.B. Virtual food safety trainings during the COVID-19 pandemic reveals significant opportunities for future distance education in food safety extension. Food Saf. Manag. Pract. 2021. submitted. [Google Scholar]
- Egalite, A.J.; Kisida, B. The effects of teacher match on students’ academic perceptions and attitudes. Educ. Eval. Policy Anal. 2018, 40, 59–81. [Google Scholar] [CrossRef] [Green Version]
- Larson, A.L.; Cycyk, L.M.; Carta, J.J.; Hammer, C.S.; Baralt, M.; Uchikoshi, Y.; An, Z.G.; Wood, C. A systematic review of language-focused interventions for young children from culturally and linguistically diverse backgrounds. Early Child. Res. Q. 2020, 50, 157–178. [Google Scholar] [CrossRef]
- Curtis, M.E.; Clingan, S.E.; Guo, H.; Zhu, Y.; Mooney, L.J.; Hser, Y.I. Disparities in digital access among American rural and urban households and implications for telemedicine-based services. J. Rural. Health 2021. [Google Scholar] [CrossRef] [PubMed]
- Zuo, G.W. Wired and hired: Employment effects of subsidized broadband Internet for low-income Americans. Am. Econ. J. Econ. Policy 2021, 13, 447–482. [Google Scholar] [CrossRef]
- Rosston, G.L.; Wallsten, S.J. Increasing low-income broadband adoption through private incentives. Telecommun. Policy 2020, 44, 102020. [Google Scholar] [CrossRef]
- Comcast NBCUniversal. Ready for Anything. Available online: https://update.comcast.com/wp-content/uploads/sites/33/dlm_uploads/2018/08/Internet-Essentials-2018-Progress-Report.pdf (accessed on 9 November 2021).
- Baranowski, T.; Cullen, K.W.; Nicklas, T.; Thompson, D.; Baranowski, J. Are current health behavioral change models helpful in guiding prevention of weight gain efforts? Obes. Res. 2003, 11, 23S–43S. [Google Scholar] [CrossRef]
- Rezaei, R.; Mianaji, S.; Ganjloo, A. Factors affecting farmers’ intention to engage in on-farm food safety practices in Iran: Extending the theory of planned behavior. J. Rural. Stud. 2018, 60, 152–166. [Google Scholar] [CrossRef]
- Bonanno, A.; Li, J. Food insecurity and food access in US metropolitan areas. Appl. Econ. Perspect. Policy 2015, 37, 177–204. [Google Scholar] [CrossRef]
- Sharpe, P.A.; Liese, A.D.; Bell, B.A.; Wilcox, S.; Hutto, B.E.; Stucker, J. Household food security and use of community food sources and food assistance programs among food shoppers in neighborhoods of low income and low food access. J. Hunger Environ. Nutr. 2018, 13, 482–496. [Google Scholar] [CrossRef]
- Seligman, H.K.; Berkowitz, S.A. Aligning programs and policies to support food security and public health goals in the United States. Annu. Rev. Public Health 2019, 40, 319–337. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Correlation Coefficient | Interpretation | |
|---|---|---|
| +1 | −1 | Perfect |
| +0.9 | −0.9 | Strong |
| +0.8 | −0.8 | Strong |
| +0.7 | −0.7 | Strong |
| +0.6 | −0.6 | Moderate |
| +0.5 | −0.5 | Moderate |
| +0.4 | −0.4 | Moderate |
| +0.3 | −0.3 | Weak |
| +0.2 | −0.2 | Weak |
| +0.1 | −0.1 | Weak |
| 0 | 0 | Zero |
| Characteristics | English Program n (%) (n = 30) | Spanish Program n (%) (n = 30) | Total n (%) (n = 60) |
|---|---|---|---|
| Gender | |||
| Female | 30 (100) | 28 (93) | 58 (97) |
| Male | - | 2 (7) | 2 (3) |
| Prefer not to answer | - | - | - |
| Age | |||
| 18–24 | 1 (3) | 5 (17) | 6 (10) |
| 25–34 | 16 (54) | 8 (27) | 24 (40) |
| 35–54 | 12 (40) | 16 (53) | 28 (47) |
| 55 and above | 1 (3) | 1 (3) | 2 (3) |
| Prefer not to answer | - | - | - |
| Ethnicity | |||
| White | 14 (47) | 2 (7) | 16 (26) |
| Hispanic American | 1 (3) | 23 (77) | 24 (40) |
| Asian American | 1 (3) | - | 1 (2) |
| Native American | 1 (3) | - | 1 (2) |
| African American | 10 (34) | - | 10 (17) |
| Others | 3 (10) | 5 (16) | 8 (13) |
| Children (<10 years old) in household | |||
| 1 | 5 (17) | 11 (37) | 16 (26) |
| 2 | 10 (33) | 9 (30) | 19 (32) |
| 3 | 11 (37) | 2 (7) | 13 (22) |
| 4 | 4 (13) | 1 (3) | 5 (9) |
| 5 | - | - | - |
| 6 and above | - | - | - |
| Prefer not to answer | - | 7 (23) | 7 (11) |
| Meal preparation frequency | |||
| All the time | 12 (40) | 16 (53) | 28 (47) |
| Nearly all the time | 16 (53) | 9 (30) | 25 (42) |
| Some of the time | 2 (7) | 5 (17) | 7 (11) |
| Never | - | - | - |
| Household income | |||
| Less than 10,000USD | 3 (10) | 3 (10) | 6 (10) |
| 10,001USD–30,000USD | 8 (27) | 8 (27) | 16 (27) |
| 30,001USD–50,000USD | 16 (53) | 4 (13) | 20 (34) |
| 50,001USD–80,000USD | 3 (10) | 5 (16) | 8 (13) |
| 80,001USD and above | - | 2 (7) a | 2 (3) |
| Prefer not to answer | - | 8 (27) | 8 (13) |
| Education | |||
| High school/GED degree | 15 (50) | 6 (20) | 21 (35) |
| Associate degree | 4 (13) | 9 (30) | 13 (22) |
| Bachelor’s degree | 8 (27) | 14 (47) | 22 (36) |
| Post-graduate degree | 3 (10) | 1 (3) | 4 (7) |
| English Program (n = 30) | Spanish Program (n = 30) | Total (n = 60) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre-Survey (Mean ± SD) | Post-Survey (Mean ± SD) | p Value (Paired Samples t-Test) | Pre-Survey (Mean ± SD) | Post-Survey (Mean ± SD) | p Value (Paired Samples t-Test) | Pre-Survey (Mean ± SD) | Post-Survey (Mean ± SD) | p Value (paired Samples t-Test) | |
| Knowledge a | 5.80 ± 1.32 | 7.70 ± 0.75 | <0.001 | 4.83 ± 1.76 d | 7.17 ± 0.87 e | <0.001 | 5.32 ± 1.62 | 7.43 ± 0.85 | <0.001 |
| Attitudes toward the behavior b | 30.50 ± 2.61 | 33.03 ± 1.75 | <0.001 | 29.73 ± 3.83 | 33.00 ± 1.98 | <0.001 | 30.12 ± 3.27 | 33.02 ± 1.85 | <0.001 |
| Perceived behavioral control (PBC) b | 31.67 ± 2.45 | 34.47 ± 1.31 | <0.001 | 31.57 ± 3.78 | 34.37 ± 1.19 | <0.001 | 31.62 ± 3.16 | 34.42 ± 1.24 | <0.001 |
| Subjective norms b | 31.90 ± 4.59 | 35.10 ± 4.21 | <0.001 | 34.53 ± 4.15 d | 36.00 ± 3.64 | 0.086 | 33.22 ± 4.54 | 35.55 ± 3.93 | <0.001 |
| Behavior change intentions b | 27.73 ± 1.74 | 29.67 ± 0.84 | <0.001 | 28.13 ± 2.06 | 29.70 ± 0.60 | <0.001 | 27.93 ± 1.90 | 29.68 ± 0.72 | <0.001 |
| Self-reported safe food practice behaviors c | 25.80 ± 4.44 | 30.17 ± 4.07 | <0.001 | 23.77 ± 3.53 d | 28.43 ± 4.10 | <0.001 | 24.78 ± 4.10 | 29.30 ± 4.14 | <0.001 |
| Practice | TPB Constructs | Behavior Change Intentions | Self-Reported Safe Food Practice Behaviors | ||
|---|---|---|---|---|---|
| Attitudes toward the Behavior | PBC | Subjective Norms | |||
| Chilling and storing procedures for a large pot of soup. a | pre: 4.17 ± 0.91 post: 4.90 ± 0.35 p value: ≤0.05 | pre: 4.38 ± 0.76 post: 4.88 ± 0.37 p value: ≤0.05 | pre: 3.98 ± 1.10 post: 4.48 ± 0.77 p value: ≤0.05 | NA b | NA b |
| Using thermometer to check the safe cooking temperature of ground beef. a | pre: 3.92 ± 0.98 post: 4.87 ± 0.34 p value: ≤0.05 | pre: 4.13 ± 1.00 post: 4.88 ± 0.37 p value: ≤0.05 | pre: 3.38 ± 1.35 post: 4.32 ± 0.83 p value: ≤0.05 | pre: 4.07 ± 0.97 post: 4.92 ± 0.28 p value: ≤0.05 | pre: 2.20 ± 1.39 post: 3.93 ± 1.12 p value: ≤0.05 |
| Checking the temperature of the refrigerator and freezer. a | pre: 4.23 ± 1.16 post: 4.93 ± 0.31 p value: ≤0.05 | pre: 4.37 ± 0.80 post: 4.92 ± 0.28 p value: ≤0.05 | pre: 4.12 ± 0.99 post: 4.55 ± 0.70 p value: ≤0.05 | pre: 4.53 ± 0.60 post: 4.97 ± 0.18 p value: ≤0.05 | pre: 2.65 ± 1.54 post: 4.17 ± 1.26 p value: ≤0.05 |
| English Program (n = 30) | Spanish Program (n = 30) | Total (n = 60) | |
|---|---|---|---|
| Statements a | Evaluation (Mean ± SD) | ||
| My expectations were met. | 5.00 ± 0.00 | 4.90 ± 0.40 | 4.95 ± 0.29 |
| I would recommend this course to my friends and family. | 5.00 ± 0.00 | 4.83 ± 0.38 | 4.92 ± 0.28 |
| I have practiced what I have learned in my daily food preparation routine. | 4.90 ± 0.31 | 4.97 ± 0.18 | 4.93 ± 0.25 |
| This course will have a significant impact on the safety of my food handling practices. | 4.93 ± 0.25 | 4.83 ± 0.46 | 4.88 ± 0.37 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Archila-Godínez, J.C.; Chen, H.; Klinestiver, L.; Rosa, L.; Barrett, T.; Henley, S.C.; Feng, Y. An Evaluation of a Virtual Food Safety Program for Low-Income Families: Applying the Theory of Planned Behavior. Foods 2022, 11, 355. https://doi.org/10.3390/foods11030355
Archila-Godínez JC, Chen H, Klinestiver L, Rosa L, Barrett T, Henley SC, Feng Y. An Evaluation of a Virtual Food Safety Program for Low-Income Families: Applying the Theory of Planned Behavior. Foods. 2022; 11(3):355. https://doi.org/10.3390/foods11030355
Chicago/Turabian StyleArchila-Godínez, Juan C., Han Chen, Leah Klinestiver, Lia Rosa, Tressie Barrett, Shauna C. Henley, and Yaohua Feng. 2022. "An Evaluation of a Virtual Food Safety Program for Low-Income Families: Applying the Theory of Planned Behavior" Foods 11, no. 3: 355. https://doi.org/10.3390/foods11030355