
The Blood-Pressure-Lowering Effect of Food-Protein-Derived Peptides: A Meta-Analysis of Recent Clinical Trials

 ,
,  ,
, 

Abstract
1. Introduction
2. Materials and Methods
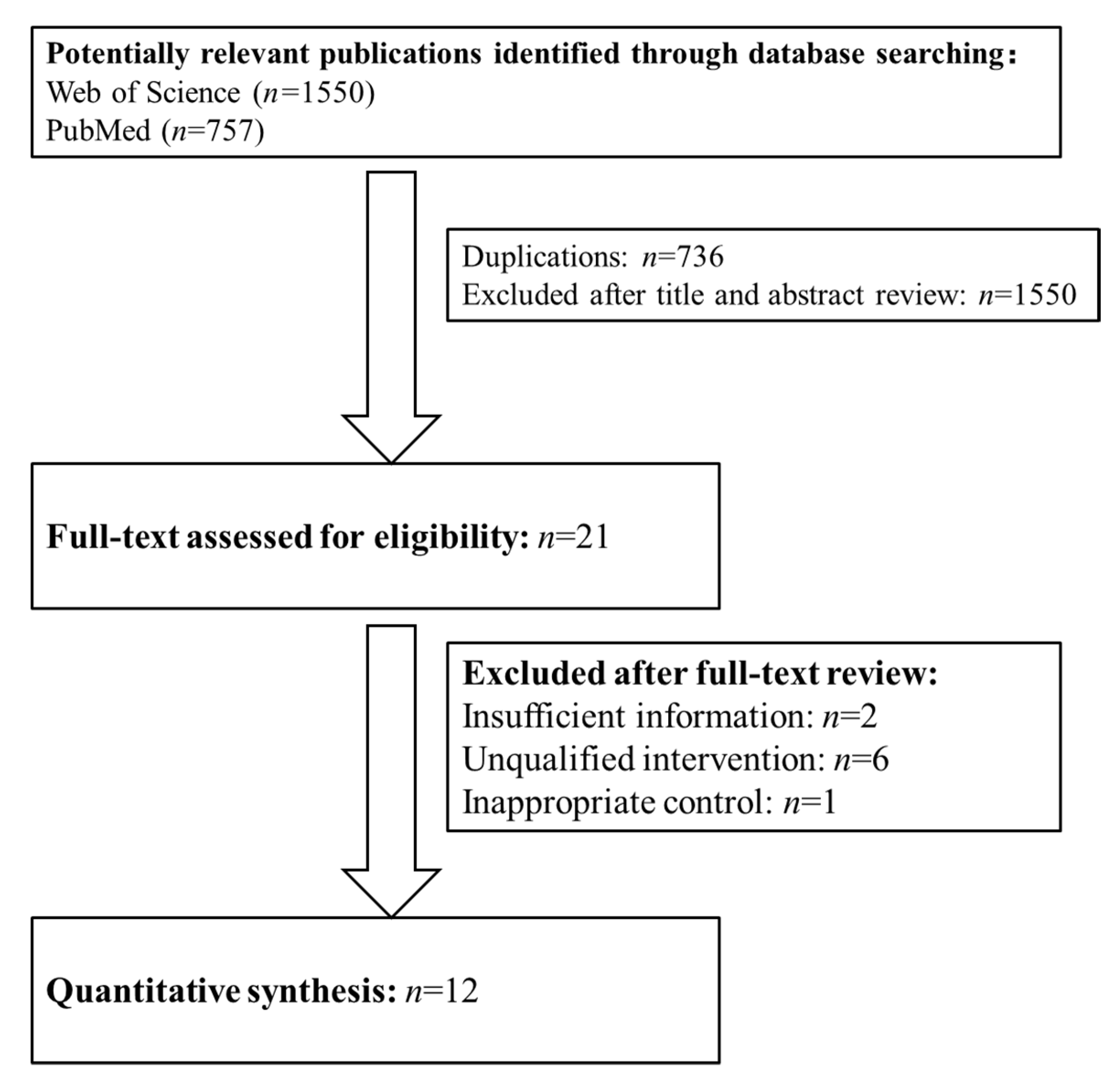
2.1. Search Strategy and the Inclusion and Exclusion Criteria
2.2. Data Extraction
2.3. Statistical Analyses
3. Results
3.1. Study Characteristics
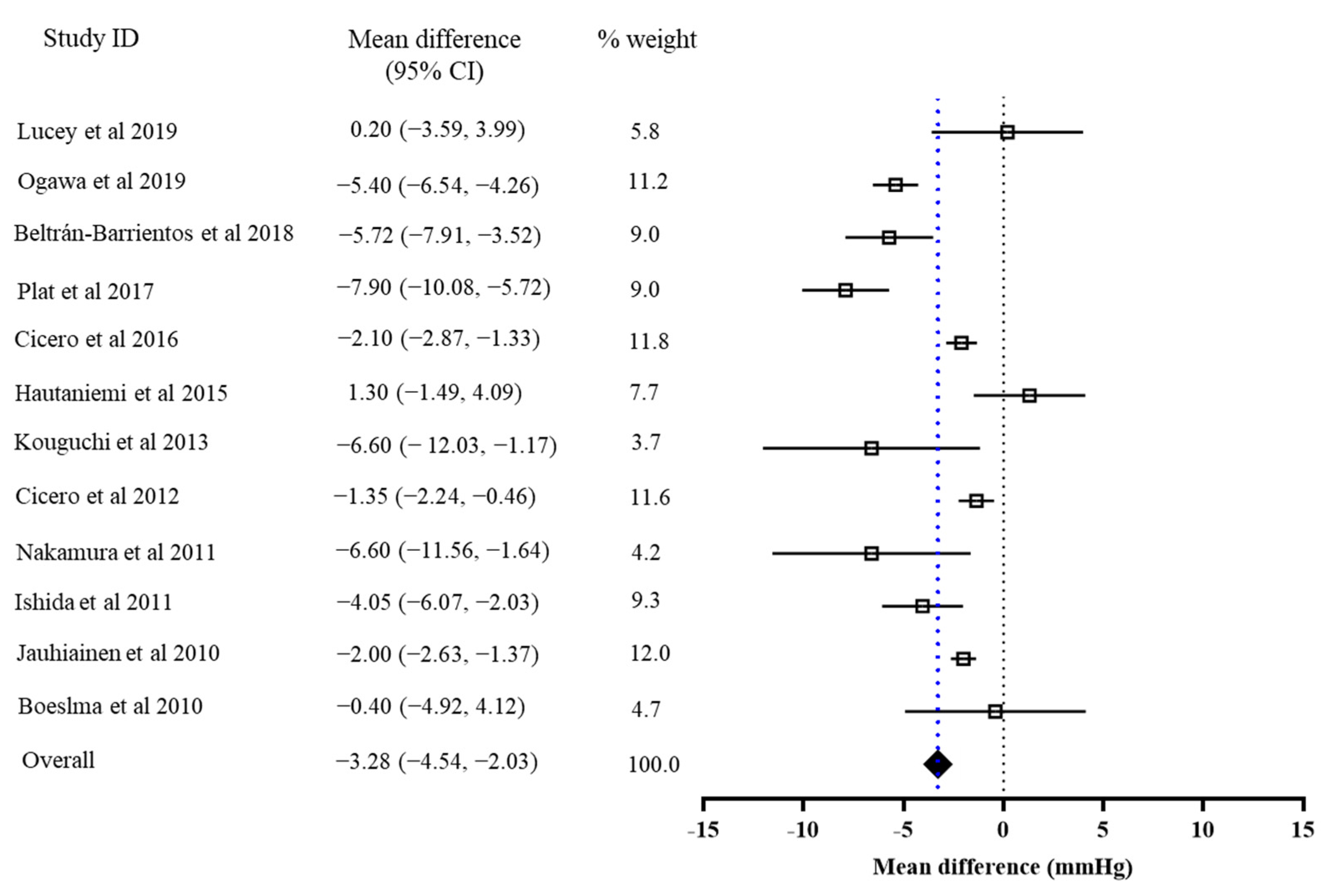
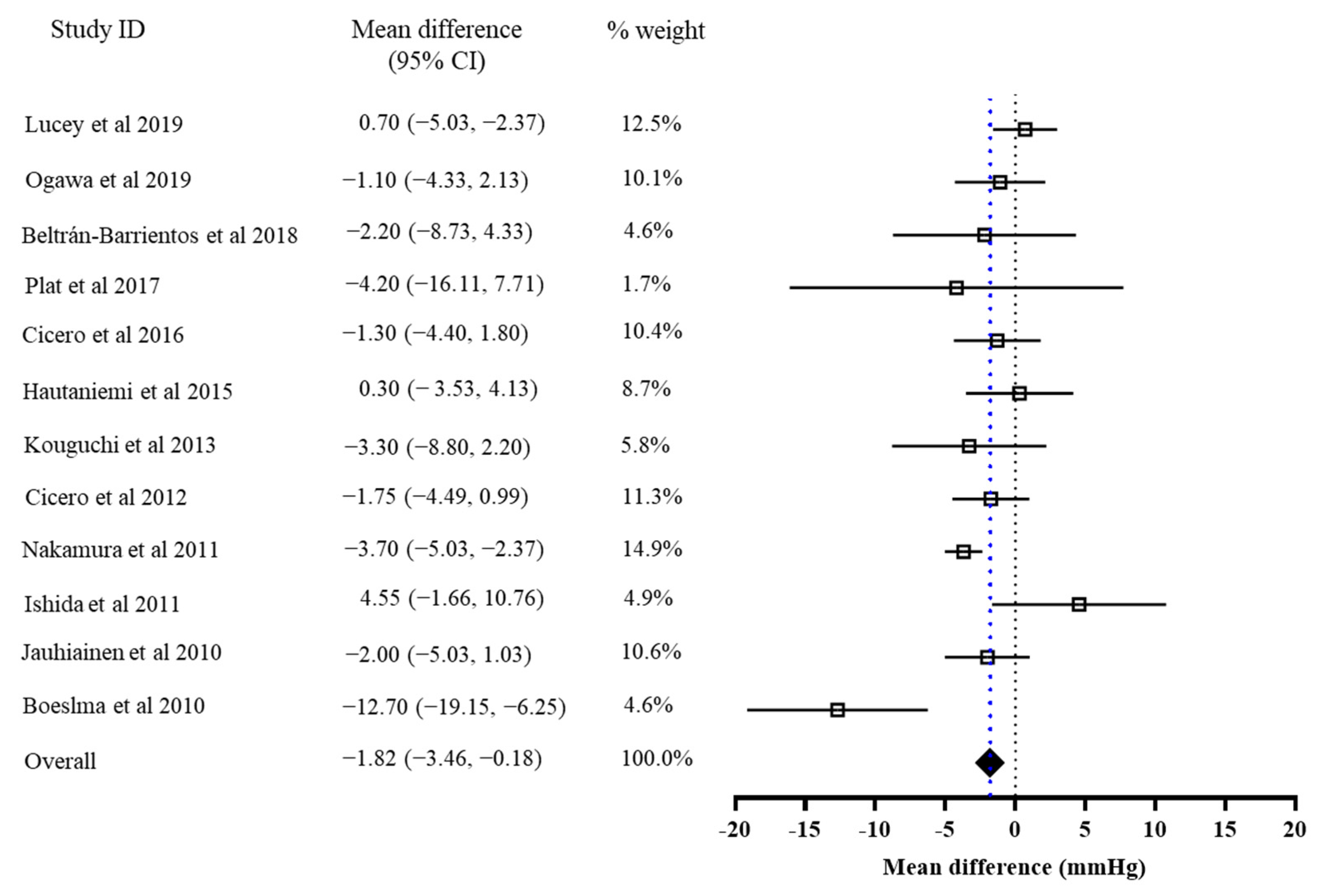
3.2. The Effects of Bioactive Peptide Intervention
3.3. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Mills, K.T.; Stefanescu, A.; He, J. The global epidemiology of hypertension. Nat. Rev. Nephrol. 2020, 16, 223–237. [Google Scholar] [CrossRef] [PubMed]
- Song, P.; Zhang, Y.; Yu, J.; Zha, M.; Zhu, Y.; Rahimi, K.; Rudan, I. Global prevalence of hypertension in children: A systematic review and meta-analysis. JAMA Pediatr. 2019, 173, 1154–1163. [Google Scholar] [CrossRef] [PubMed]
- Dahlöf, B. Cardiovascular disease risk factors: Epidemiology and risk assessment. Am. J. Cardiol. 2010, 105 (Suppl. 1), 3A–9A. [Google Scholar] [CrossRef] [PubMed]
- Borghi, C.; Tsioufis, K.; Agabiti-Rosei, E.; Burnier, M.; Cicero, A.F.G.; Clement, D.; Coca, A.; Desideri, G.; Grassi, G.; Lovic, D.; et al. Nutraceuticals and blood pressure control: A European Society of Hypertension position document. J. Hypertens. 2020, 38, 799–812. [Google Scholar] [CrossRef] [PubMed]
- Cicero, A.F.G.; Grassi, D.; Tocci, G.; Galletti, F.; Borghi, C.; Ferri, C. Nutrients and nutraceuticals for the management of high normal blood pressure: An evidence-based consensus document. High Blood Press. Cardiovasc. Prev. 2019, 26, 9–25. [Google Scholar] [CrossRef]
- Liao, W.; Wu, J. The ACE2/Ang (1–7)/MasR axis as an emerging target for antihypertensive peptides. Crit. Rev. Food Sci. Nutr. 2021, 61, 2572–2586. [Google Scholar] [CrossRef]
- Wu, J.; Liao, W.; Udenigwe, C.C. Revisiting the mechanisms of ACE inhibitory peptides from food proteins. Trends Food Sci. Technol. 2017, 69, 214–219. [Google Scholar] [CrossRef]
- Chakrabarti, S.; Guha, S.; Majumder, K. Food-derived bioactive peptides in human health: Challenges and opportunities. Nutrients 2018, 10, 1738. [Google Scholar] [CrossRef]
- Cicero, A.F.G.; Aubin, F.; Azais-Braesco, V.; Borghi, C. Do the lactotripeptides Isoleucine–Proline–Proline and Valine–Proline–Proline reduce systolic blood pressure in European Subjects? A Meta-analysis of randomized controlled trials. Am. J. Hypertens. 2013, 26, 442–449. [Google Scholar] [CrossRef]
- Fekete, Á.A.; Givens, D.I.; Lovegrove, J.A. Casein-derived lactotripeptides reduce systolic and diastolic blood pressure in a meta-analysis of randomised clinical trials. Nutrients 2015, 7, 659–681. [Google Scholar] [CrossRef]
- Majumder, K.; Wu, J. Molecular targets of antihypertensive peptides: Understanding the mechanisms of action based on the pathophysiology of hypertension. Int. J. Mol. Sci. 2015, 16, 256–283. [Google Scholar] [CrossRef]
- van der Zander, K.; Bots, M.L.; Bak, A.A.; Koning, M.M.; de Leeuw, P.W. Enzymatically hydrolyzed lactotripeptides do not lower blood pressure in mildly hypertensive subjects. Am. J. Clin. Nutr. 2008, 88, 1697–1702. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults. J Am Coll Cardiol. 2018, 71, e127–e248. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Jauhiainen, T.; Rönnback, M.; Vapaatalo, H.; Wuolle, K.; Kautiainen, H.; Groop, P.H.; Korpela, R. Long-term intervention with Lactobacillus helveticus fermented milk reduces augmentation index in hypertensive subjects. Eur. J. Clin. Nutr. 2010, 64, 424–431. [Google Scholar] [CrossRef] [PubMed]
- Boelsma, E.; Kloek, J. IPP-rich milk protein hydrolysate lowers blood pressure in subjects with stage 1 hypertension, a randomized controlled trial. Nutr. J. 2010, 9, 52. [Google Scholar] [CrossRef]
- Ishida, Y.; Shibata, Y.; Fukuhara, I.; Yano, Y.; Takehara, I.; Kaneko, K. Effect of an excess intake of casein hydrolysate containing Val-Pro-Pro and Ile-Pro-Pro in subjects with normal blood pressure, high-normal blood pressure, or mild hypertension. Biosci. Biotechnol. Biochem. 2011, 75, 427–433. [Google Scholar] [CrossRef]
- Nakamura, T.; Mizutani, J.; Ohki, K.; Yamada, K.; Yamamoto, N.; Takeshi, M.; Takazawa, K. Casein hydrolysate containing Val-Pro-Pro and Ile-Pro-Pro improves central blood pressure and arterial stiffness in hypertensive subjects: A randomized, double-blind, placebo-controlled trial. Atherosclerosis 2011, 219, 298–303. [Google Scholar] [CrossRef]
- Cicero, A.F.G.; Rosticci, M.; Ferroni, A.; Bacchelli, S.; Veronesi, M.; Strocchi, E.; Borghi, C. Predictors of the short-term effect of Isoleucine–Proline–Proline/Valine–Proline–Proline Lactotripeptides from casein on office and ambulatory blood pressure in subjects with pharmacologically untreated high-normal blood pressure or first-degree hypertension. Clin. Exp. Hypertens. 2012, 34, 601–605. [Google Scholar]
- Hautaniemi, E.J.; Tikkakoski, A.J.; Tahvanainen, A.; Nordhausen, K.; Kähönen, M.; Mattsson, T.; Luhtala, S.; Turpeinen, A.M.; Niemelä, O.; Vapaatalo, H.; et al. Effect of fermented milk product containing lactotripeptides and plant sterol esters on haemodynamics in subjects with the metabolic syndrome—A randomised, double-blind, placebo-controlled study. Br. J. Nutr. 2015, 114, 376–386. [Google Scholar] [CrossRef]
- Arrigo, F.G.; Cicero, A.C.; Martina, R.; Marcella, C.; Riccardo, U.; Marina, G.; Claudio, B.; D’Addato, S. Effect of lactotripeptides (Isoleucine–Proline–Proline/Valine–Proline–Proline) on blood pressure and arterial stiffness changes in subjects with suboptimal blood pressure control and metabolic syndrome: A double-blind, randomized, crossover clinical trial. Metab. Syndr. Relat. Disord. 2016, 14, 161–166. [Google Scholar]
- Beltrán-Barrientos, L.M.; González-Córdova, A.F.; Hernández-Mendoza, A.; Torres-Inguanzo, E.H.; Astiazarán-García, H.; Esparza-Romero, J.; Vallejo-Cordoba, B. Randomized double-blind controlled clinical trial of the blood pressure–lowering effect of fermented milk with Lactococcus lactis: A pilot study. J. Dairy Sci. 2018, 101, 2819–2825. [Google Scholar] [CrossRef]
- Plat, J.; Severins, N.; Morrison, S.; Mensink, R.P. Effects of NWT-03, an egg-protein hydrolysate, on blood pressure in normotensive, high-normotensive and mild-hypertensive men and women: A dose-finding study. Br. J. Nutr. 2017, 117, 942–950. [Google Scholar] [CrossRef][Green Version]
- Lucey, A.J.; Heneghan, C.; Manning, E.; Kroon, P.A.; Kiely, M.E. Effect of an egg ovalbumin-derived protein hydrolysate on blood pressure and cardiovascular risk in adults with a mildly elevated blood pressure: A randomized placebo-controlled crossover trial. Eur. J. Nutr. 2019, 58, 2823–2833. [Google Scholar] [CrossRef] [PubMed]
- Kouguchi, T.; Ohmori, T.; Shimizu, M.; Takahata, Y.; Maeyama, Y.; Suzuki, T.; Morimatsu, F.; Tanabe, S. Effects of a chicken collagen hydrolysate on the circulation system in subjects with mild hypertension or high-normal blood pressure. Biosci. Biotechnol. Biochem. 2013, 77, 691–696. [Google Scholar] [CrossRef]
- Ogawa, Y.; Shobako, N.; Fukuhara, I.; Satoh, H.; Kobayashi, E.; Kusakari, T.; Suwa, M.; Matsumoto, M.; Ishikado, A. Rice bran supplement containing a functional substance, the novel peptide Leu-Arg-Ala, has anti-hypertensive effects: A double-blind, randomized, placebo-controlled study. Nutrients 2019, 11, 726. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Prairie, N.; Udenigwe, C.C.; Adebiyi, A.P.; Tappia, P.S.; Aukema, H.M.; Jones, P.J.H.; Aluko, R.E. Blood pressure lowering effect of a pea protein hydrolysate in hypertensive rats and humans. J. Agric. Food Chem. 2011, 59, 9854–9860. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.-M.; Ho, S.C.; Chen, Y.-M.; Woo, J. Effect of soy protein and isoflavones on blood pressure and endothelial cytokines: A 6-month randomized controlled trial among postmenopausal women. J. Hypertens. 2013, 31, 384–392. [Google Scholar] [CrossRef]
- Zhu, C.F.; Li, G.Z.; Peng, H.B.; Zhang, F.; Chen, Y.; Li, Y. Therapeutic effects of marine collagen peptides on Chinese patients with type 2 diabetes mellitus and primary hypertension. Am. J. Med Sci. 2010, 340, 360–366. [Google Scholar] [CrossRef]
- Qin, L.Q.; Xu, J.Y.; Dong, J.Y.; Zhao, Y.; van Bladeren, P.; Zhang, W. Lactotripeptides intake and blood pressure management: A meta-analysis of randomised controlled clinical trials. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Chanson-Rolle, A.; Aubin, F.; Braesco, V.; Hamasaki, T.; Kitakaze, M. Influence of the lactotripeptides Isoleucine–Proline–Proline and Valine–Proline–Proline on systolic blood pressure in Japanese subjects: A systematic review and meta-analysis of randomized controlled trials. PLoS ONE 2015, 10, e014223. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Wheeler, C.T.; Alberico, T.; Sun, X.; Seeberger, J.; Laslo, M.; Spangler, E.; Kern, B.; de Cabo, R.; Zou, S. The effect of resveratrol on lifespan depends on both gender and dietary nutrient composition in Drosophila melanogaster. AGE 2013, 35, 69–81. [Google Scholar] [CrossRef] [PubMed]
- Shiina, K.; Tomiyama, H.; Matsumoto, C.; Komatsu, S.; Natsume, M.; Oba, C.; Ohshiba, Y.; Yamaji, T.; Chikamori, T.; Yamashina, A. Gender difference in the effects of cacao polyphenols on blood pressure and glucose/lipid metabolism in prediabetic subjects: A double-blinded, randomized, placebo-controlled crossover trial. Hypertens. Res. 2019, 42, 1083–1085. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Number of Participants (M/F), Average Age | Study Design | Duration | Treatment | Daily Dosage | Placebo | Basal BP | BP Measurement | |
|---|---|---|---|---|---|---|---|---|---|
| Systolic BP | Diastolic BP | ||||||||
| Jauhiainen et al., 2010 [16] | 121 (54/67), 49 ± 5 | R, D, PAL, P | 12 weeks | IPP and VPP in fermented milk | 50 mg IPP and VPP | Placebo milk without peptides | T: 151.3 ± 14.8 C: 154.6 ± 13.9 | T: 95.2 ± 12.2 C: 94.2 ± 8.8 | ABPM |
| Boeslma et al., 2010 [17] | 26 (17/9), 59 ± 7.3 | R, D, PAL, P, CR | 4 weeks | Casein hydrolysate | 1 g hydrolysate in 2 capsules | 2 capsules filled with cellulose | T: 146.6 ± 10.8 C: 150.4 ± 8.9 | T: 89.7 ± 8.7 C: 92.0 ± 8.5 | Office |
| Ishida et al., 2011 [18] | 32 (16/16), 51.9 ± 9.3 | R, D, PAL, P | 6 weeks | IPP and VPP in casein hydrolysate | 7.5 mg VPP and 9.6 mg IPP in tablets | Tablets filled with sodium caseinate | T: 141.4 ± 3.5 C: 141.3 ± 3 | T: 84.7 ± 5.1 C: 86.1 ± 5.1 | Office |
| Nakamura et al., 2011 [19] | 70 (47/23), 57.8 ± 5.4 | R, D, PAL, P | 8 weeks | IPP and VPP in casein hydrolysate | 1.5 mg VPP/day and 1.9 mg IPP in tablets | Tablets filled with sodium caseinate | T: 146.8 ± 4.4 C: 87.5 ± 7.1 | T: 146.9 ± 4.3 C: 88.0 ± 7.7 | Office |
| Cicero et al., 2012 [20] | 164 (101/63), 43.85 ± 11.1 | R, D, PAL, P | 4 weeks | IPP and VPP in milk protein hydrolysate | 2 mg VPP/day and 1 mg IPP with 250 mL fruit juice | 250 mL fruit juice without peptides | T: 133.49 ± 12.92 C: 83.28 ± 8.75 | T: 132.69 ± 12.46 C: 82.78 ± 8.33 | ABPM |
| Kouguchi et al., 2013 [26] | 58 (30/28), 52.8 ± 8.5 | R, D, PAL, P | 12 weeks | Chicken collagen hydrolysate | 4.4 g hydrolysate in 120 mL of lactic acid drink | 120 mL of lactic acid drink without hydrolysate | T: 139.2 ± 9.1 C: 85 ± 7.6 | T: 137.9 ± 11.1 C: 85.5 ± 7.4 | Office |
| Hautaniemi et al., 2015 [19] | 58 (30/28), 52.3 ± 6.6 | R, D, PAL, P | 12 weeks | IPP and VPP in fermented milk | 50 mg IPP and VPP in 125 mL fermented milk | 125 mL fermented milk without peptides | T: 168 ± 20 C: 162 ± 15 | T: 102 ± 10 C: 100 ± 10 | Office |
| Cicero et al., 2016 [21] | 40 (26/14), 50.1 ± 9.9 | R, D, PAL, P, CR | 4 weeks | IPP and VPP in casein hydrolysate | 10.2 mg IPP and VPP in 12 tablets | 12 tablets filled without peptides | T: 142.1 ± 11.5 C: 139.2 ± 8.3 | T: 86.2 ± 8.6 C: 85.2 ± 7.2 | ABPM |
| Plat et al., 2017 [24] | 10 | R, D, PAL, P, CR | 1 week | Egg protein hydrolysate | 2 g hydrolysate | Erythritol | T: 148.1 ± 12.9 C: 143.6 ± 9.3 | T: 87.9 ± 10.0 C: 85.3 ± 9.2 | Office |
| Beltrán-Barrientos et al., 2018 [23] | 36 (20/16), 42.55 ± 10.45 | R, D, PAL, P | 5 weeks | Fermented milk | 150 mL | Control milk | T: 131.8 ± 5.6 C: 134.3 ± 7 | T: 87.7 ± 5.1 C: 89.3 ± 5.8 | Office |
| Lucey et al., 2019 [25] | 65 (37/28), 56.9 ± 5.2 | R, D, PAL, P, CR | 12 weeks | Ovalbumin hydrolysate | 3 g hydrolysate in 150 mL fruit juice | Maltodextrin in 150 mL fruit juice | T: 135.5 ± 12.3 C: 133.8 ± 10.6 | T: 75.9 ± 6.3 C: 76.1 ± 7 | Office |
| Ogawa et al., 2019 [27] | 71 (31/40), 53.9 ± 5.85 | R, D, PAL, P | 12 weeks | Rice bran peptide LRA | 43 μg peptide in 4 tablets | 4 tablets without peptides | T: 141 ± 8.5 C: 141.9 ± 8.5 | T: 89.4 ± 7 C: 88.9 ± 6.4 | Office |
| Sub-Group Title | No. of Trials | Mean Difference (95% ci) | |
|---|---|---|---|
| SBP | DBP | ||
| Basal BP | |||
| ≤140/85 mmHg | 4 | −1.97 (−2.77, −1.18) | −0.25 (−2.67, 2.17) |
| >140/85 mmHg | 8 | −2.74 (−3.16, −2.32) | −2.69 (−3.69, −1.69) |
| p value | 0.007 | 0.01 | |
| Ratio of male to female | |||
| ≤0.5 | 6 | −4.29 (−6.39, −2.19) | −0.36 (−1.92, 1.20) |
| >0.5 | 6 | −1.75 (−3.08, −0.42) | −2.96 (−5.20, −0.71) |
| p value | 0.04 | 0.06 | |
| Age | |||
| ≤50 | 4 | −2.02 (−2.44, −1.60) | −1.73 (−3.37, −0.09) |
| >50 | 8 | −4.62 (−5.42, −3.81) | −1.96 (−4.55, 0.63) |
| p value | 0.001 | 0.88 | |
| Country of the study | |||
| Asia (Japan) | 4 | −1.19 (−1.45, −0.94) | −3.04 (−4.22, −1.87) |
| Others (Europe and Mexico) | 8 | −0.45 (−0.64, −0.26) | −2.18 (−3.03, −1.33) |
| p value | 0.01 | 0.04 | |
| Trial size | |||
| ≤50 | 5 | −4.06 (−6.54, −1.57) | −0.10 (−1.59, 1.79) |
| >50 | 7 | −2.62 (−4.33, −0.91) | −2.68 (−4.74, −0.63) |
| p value | 0.35 | 0.04 | |
| Parent protein | |||
| Milk protein | 8 | −2.37 (−3.38, −1.36) | −2.13 (−4.22, −0.04) |
| Other protein sources | 4 | −5.11 (−7.89, −2.34) | −0.33 (−2.09, 1.42) |
| p value | 0.07 | 0.20 | |
| Intervention duration | |||
| ≤6 weeks | 6 | −3.67 (−5.49, −1.84) | −2.53 (−6.16, 1.09) |
| >6 weeks | 6 | −2.86 (−5.17, −0.55) | −1.38 (−2.92, 0.15) |
| p value | 0.59 | 0.57 | |
| Delivery vehicle | |||
| Liquid | 6 | −2.07 (−3.53, −0.61) | −0.82 (−2.16, 0.52) |
| Non-liquid | 6 | −4.46 (−6.60, −2.32) | −2.70 (−5.69, 0.30) |
| p value | 0.07 | 0.26 | |
| Study | Random Sequence Generation | Allocation Concealment | Blinding of Participants and Personnel | Blinding of Outcome Assessment | Incomplete Outcome Data | Selective Reporting | Other Sources of Bias |
|---|---|---|---|---|---|---|---|
| Jauhiainen et al., 2010 [16] | U | U | L | L | L | L | L |
| Boeslma et al., 2010 [17] | U | U | L | L | H | L | L |
| Ishida et al., 2011 [18] | U | U | L | U | L | L | L |
| Nakamura et al., 2011 [19] | U | U | L | U | L | L | L |
| Cicero et al., 2012 [20] | U | U | L | L | L | L | L |
| Kouguchi et al., 2013 [26] | U | U | L | U | L | L | L |
| Hautaniemi et al., 2015 [21] | U | U | L | U | L | L | L |
| Cicero et al., 2016 [22] | U | U | L | L | L | L | L |
| Plat et al., 2017 [24] | U | H | H | U | H | L | L |
| Beltrán-Barrientos et al., 2018 [23] | U | U | L | U | L | L | L |
| Lucey et al., 2019 [25] | U | U | L | U | H | L | L |
| Ogawa et al., 2019 [27] | U | U | L | U | L | L | L |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liao, W.; Sun, G.; Xu, D.; Wang, Y.; Lu, Y.; Sun, J.; Xia, H.; Wang, S. The Blood-Pressure-Lowering Effect of Food-Protein-Derived Peptides: A Meta-Analysis of Recent Clinical Trials. Foods 2021, 10, 2316. https://doi.org/10.3390/foods10102316
Liao W, Sun G, Xu D, Wang Y, Lu Y, Sun J, Xia H, Wang S. The Blood-Pressure-Lowering Effect of Food-Protein-Derived Peptides: A Meta-Analysis of Recent Clinical Trials. Foods. 2021; 10(10):2316. https://doi.org/10.3390/foods10102316
Chicago/Turabian StyleLiao, Wang, Guiju Sun, Dengfeng Xu, Yuanyuan Wang, Yifei Lu, Jihan Sun, Hui Xia, and Shaokang Wang. 2021. "The Blood-Pressure-Lowering Effect of Food-Protein-Derived Peptides: A Meta-Analysis of Recent Clinical Trials" Foods 10, no. 10: 2316. https://doi.org/10.3390/foods10102316
APA StyleLiao, W., Sun, G., Xu, D., Wang, Y., Lu, Y., Sun, J., Xia, H., & Wang, S. (2021). The Blood-Pressure-Lowering Effect of Food-Protein-Derived Peptides: A Meta-Analysis of Recent Clinical Trials. Foods, 10(10), 2316. https://doi.org/10.3390/foods10102316