Tobacco Products, Periodontal Health and Education Level: Cohort Study from Sweden

 , ,
, ,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
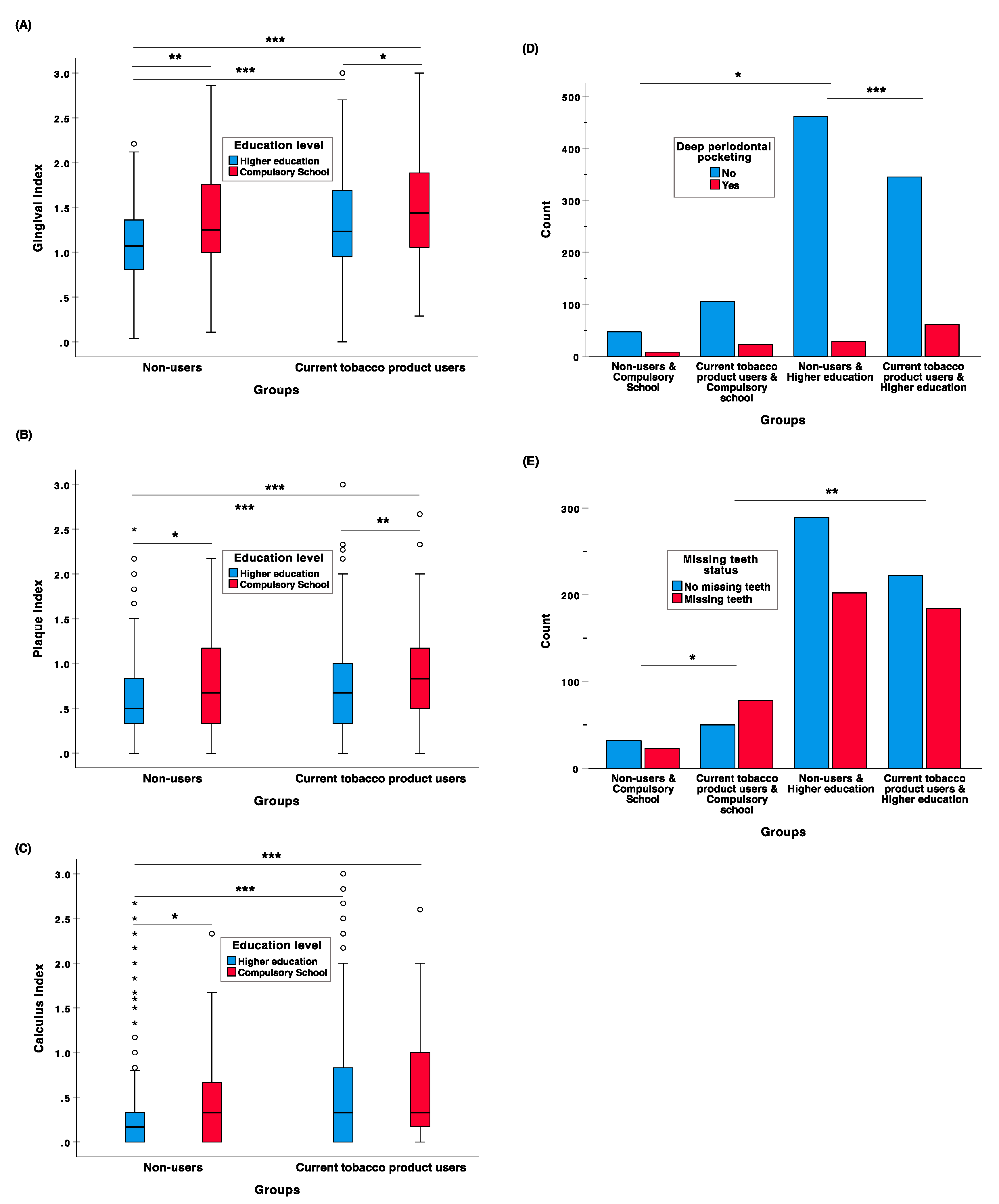
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lang, N.P.; Bartold, P.M. Periodontal health. J. Periodontol. 2018, 89, S9–S16. [Google Scholar] [CrossRef]
- Pihlstrom, B.; Michalowicz, B.; Johnson, N. Periodontal diseases. Lancet 2005, 366, 1809–1820. [Google Scholar] [CrossRef]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 world workshop on the classification of periodontal and peri-implant diseases and conditions. J. Periodontol. 2018, 89, S173–S182. [Google Scholar] [CrossRef] [PubMed]
- Seymour, G.; Taylor, J. Shouts and whispers: An introduction to immunoregulation in periodontal disease. Periodontol. 2000 2004, 35, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Genco, R.J.; Borgnakke, W.S. Risk factors for periodontal disease. Periodontol. 2000 2013, 62, 59–94. [Google Scholar] [CrossRef] [PubMed]
- Heikkinen, A.M.; Pajukanta, R.; Pitkaniemi, J.; Broms, U.; Sorsa, T.; Koskenvuo, M.; Meurman, J.H. The effect of smoking on periodontal health of 15-to 16-year-old adolescents. J. Periodontol. 2008, 79, 2042–2047. [Google Scholar] [CrossRef]
- Warnakulasuriya, S.; Dietrich, T.; Bornstein, M.M.; Casals Peidro, E.; Preshaw, P.M.; Walter, C.; Wennstrom, J.L.; Bergstrom, J. Oral health risks of tobacco use and effects of cessation. Int. Dent. J. 2010, 60, 7–30. [Google Scholar]
- Bao, X.; Liu, F.; Chen, Q.; Chen, L.; Lin, J.; Chen, F.; Wang, J.; Qiu, Y.; Shi, B.; Pan, L.; et al. Propensity score analysis exploring the impact of smoking and drinking on the prognosis of patients with oral cancer. Head Neck 2020, 42, 1837–1847. [Google Scholar] [CrossRef]
- Benowitz, N. Nicotine and smokeless tobacco. CA Cancer J. Clin. 1988, 38, 244–247. [Google Scholar] [CrossRef]
- Norderhaug, I.N.; Dybing, E.; Gilljam, H.; Lind, P.O.; Lund, K.E.; Mørland, J.; Stegmayr, B.; Hofmann, B.; Elvsaas, I.K.Ø. Health Effects and Dependency Associated with Snuff Consumption; NIPH: Oslo, Norway, 2005. [Google Scholar]
- Bergstrom, J.; Keilani, H.; Lundholm, C.; Radestad, U. Smokeless tobacco (snuff) use and periodontal bone loss. J. Clin. Periodontol. 2006, 33, 549–554. [Google Scholar] [CrossRef]
- Carlsson, S.; Andersson, T.; Araghi, M.; Galanti, R.; Lager, A.; Lundberg, M.; Nilsson, P.; Norberg, M.; Pedersen, N.L.; Trolle-Lagerros, Y.; et al. Smokeless tobacco (snus) is associated with an increased risk of type 2 diabetes: Results from five pooled cohorts. J. Intern. Med. 2017, 281, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Siddiqi, K.; Shah, S.; Abbas, S.M.; Vidyasagaran, A.; Jawad, M.; Dogar, O.; Sheikh, A. Global burden of disease due to smokeless tobacco consumption in adults: Analysis of data from 113 countries. BMC Med. 2015, 13, 194. [Google Scholar] [CrossRef] [PubMed]
- Hugoson, A.; Rolandsson, M. Periodontal disease in relation to smoking and the use of swedish snus: Epidemiological studies covering 20 years (1983-2003). J. Clin. Periodontol. 2011, 38, 809–816. [Google Scholar] [CrossRef]
- Borrell, L.N.; Crawford, N.D. Socioeconomic position indicators and periodontitis: Examining the evidence. Periodontol. 2000 2012, 58, 69–83. [Google Scholar] [CrossRef]
- Almerich-Silla, J.M.; Alminana-Pastor, P.J.; Boronat-Catala, M.; Bellot-Arcis, C.; Montiel-Company, J.M. Socioeconomic factors and severity of periodontal disease in adults (35—44 years). A cross sectional study. J. Clin. Exp. Dent. 2017, 9, e988–e994. [Google Scholar] [CrossRef]
- Timberlake, D.S.; Nikitin, D.; Johnson, N.J.; Altekruse, S.F. A longitudinal study of smokeless tobacco use and mortality in the United States. Int. J. Cancer 2017, 141, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Inoue-Choi, M.; Shiels, M.S.; McNeel, T.S.; Graubard, B.I.; Hatsukami, D.; Freedman, N.D. Contemporary associations of exclusive cigarette, cigar, pipe, and smokeless tobacco use with overall and cause-specific mortality in the united states. JNCI Cancer Spectr. 2019, 3, pkz036. [Google Scholar] [CrossRef]
- Eke, P.I.; Page, R.C.; Wei, L.; Thornton-Evans, G.; Genco, R.J. Update of the case definitions for population-based surveillance of periodontitis. J. Periodontol. 2012, 83, 1449–1454. [Google Scholar] [CrossRef]
- Greene, J.; Vermillion, J. Simplified oral hygiene index. J. Am. Dent. Assoc. 1964, 68, 7. [Google Scholar] [CrossRef]
- Loe, H. The gingival index, the plaque index and the retention index systems. J. Periodontol. 1967, 38, 610–616. [Google Scholar] [CrossRef]
- Soder, B.; Jin, L.; Soder, P.; Winker, S. Clinical characteristics of destructive periodontitis in a risk group of swedish urban adults. Swed. Dent. J. 1995, 19, 9–15. [Google Scholar] [PubMed]
- Soder, P.; Jin, L.; Soder, B.; Winker, S. Periodontal status in an urban adult-population in Sweden. Community Dent. Oral Epidemiol. 1994, 22, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Katuri, K.K.; Alluri, J.K.; Chintagunta, C.; Tadiboina, N.; Borugadda, R.; Loya, M.; Marella, Y.; Bollepalli, A.C. Assessment of periodontal health status in smokers and smokeless tobacco users: A cross-sectional study. J. Clin. Diagn. Res. 2016, 10, ZC143–ZC146. [Google Scholar] [CrossRef] [PubMed]
- An, N.; Andrukhov, O.; Tang, Y.; Falkensammer, F.; Bantleon, H.; Ouyang, X.; Rausch-Fan, X. Effect of nicotine and porphyromonas gingivalis lipopolysaccharide on endothelial cells in vitro. PLoS ONE 2014, 9, e96942. [Google Scholar] [CrossRef]
- Gomes, M.S.; Chagas, P.; Pereira Padilha, D.M.; Caramori, P.; Hugo, F.N.; Augustin Schwanke, C.H.; Hilgert, J.B. Association between self-reported oral health, tooth loss and atherosclerotic burden. Braz. Oral Res. 2012, 26, 436–442. [Google Scholar] [CrossRef]
- Holmlund, A.; Holm, G.; Lind, L. Number of teeth as a predictor of cardiovascular mortality in a cohort of 7674 subjects followed for 12 years. J. Periodontol. 2010, 81, 870–876. [Google Scholar] [CrossRef]
- Desvarieux, M.; Demmer, R.; Rundek, T.; Boden-Albala, B.; Jacobs, D.; Papapanou, P.; Sacco, R. Relationship between periodontal disease, tooth loss, and carotid artery plaque—The oral infections and vascular disease epidemiology study (INVEST). Stroke 2003, 34, 2120–2125. [Google Scholar] [CrossRef]
- Siukosaari, P.; Ajwani, S.; Ainamo, A.; Wolf, J.; Narhi, T. Periodontal health status in the elderly with different levels of education: A 5-year follow-up study. Gerodontology 2012, 29, E170–E178. [Google Scholar] [CrossRef]
- Norberg, M.; Malmberg, G.; Ng, N.; Brostrom, G. Who is using snus?—Time trends, socioeconomic and geographic characteristics of snus users in the ageing swedish population. BMC Public Health 2011, 11, 929. [Google Scholar] [CrossRef]
- Henley, S.; Thun, M.; Connell, C.; Calle, E. Two large prospective studies of mortality among men who use snuff or chewing tobacco (united states). Cancer Causes Control 2005, 16, 347–358. [Google Scholar] [CrossRef]
- Berkowitz, L.; Schultz, B.M.; Salazar, G.A.; Pardo-Roa, C.; Sebastian, V.P.; Alvarez-Lobos, M.M.; Bueno, S.M. Impact of cigarette smoking on the gastrointestinal tract inflammation: Opposing effects in crohn’s disease and ulcerative colitis. Front. Immunol. 2018, 9, 74. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Current Tobacco Product Users | Non-Users | Total | p Value | |
|---|---|---|---|---|
| N = 534 | N = 546 | N = 1080 | ||
| Sex N (%) | 0.503 | |||
| Male | 267 (50.0) | 261 (47.8) | 528 (48.9) | |
| Female | 267 (50.0) | 285 (52.2) | 552 (51.1) | |
| Total | 534 (100.0) | 546 (100.0) | 1080 (100.0) | |
| Age (Mean, SD) | 35.96 (2.83) | 35.44 (2.86) | 35.70 (2.86) | 0.004 |
| Working status N (%) | 0.601 | |||
| Employed | 481 (90.2) | 498 (91.2) | 979 (90.6) | |
| Unemployed | 52 (9.8) | 48 (8.8) | 100 (9.4) | |
| Total | 533 (100.0) | 546 (100.0) | 1079 (100) | |
| Education N (%) | <0.001 | |||
| Compulsory School | 128 (24.0) | 55 (10.1) | 183 (16.9) | |
| Higher education | 406 (76.0) | 491 (89.9) | 897 (83.1) | |
| Total | 534 (100.0) | 546 (100.0) | 1080 (100.0) | |
| Marital status N (%) | <0.001 | |||
| Single | 211 (40.7) | 174 (32.8) | 385 (36.7) | |
| Married 1 | 218 (42.0) | 298 (56.1) | 516 (49.1) | |
| Divorced 2 | 90 (17.3) | 59 (11.1) | 149 (14.2) | |
| Total | 519 (100.0) | 531 (100.0) | 1050 (100) | |
| Income (Mean, SD) | 1776.44 (927.10) | 1998.32 (1157.62) | 1888.65 (1055.38) | <0.001 |
| Dental visits once a year | 0.01 | |||
| N (%) | ||||
| Yes | 156 (29.2) | 121 (22.2) | 277 (25.6) | |
| No | 378 (70.8) | 425 (77.8) | 803 (0.74) | |
| Total | 534 (100.0) | 546 (100.0) | 1080 (100.0) |
| Groups | Age at the End of the Study | Age of Death | Survival Time | Survival Analysis (Overall Comparisons) | p Value |
|---|---|---|---|---|---|
| Median (IQR) | Median (IQR) | Mean (95% CI) | Test | ||
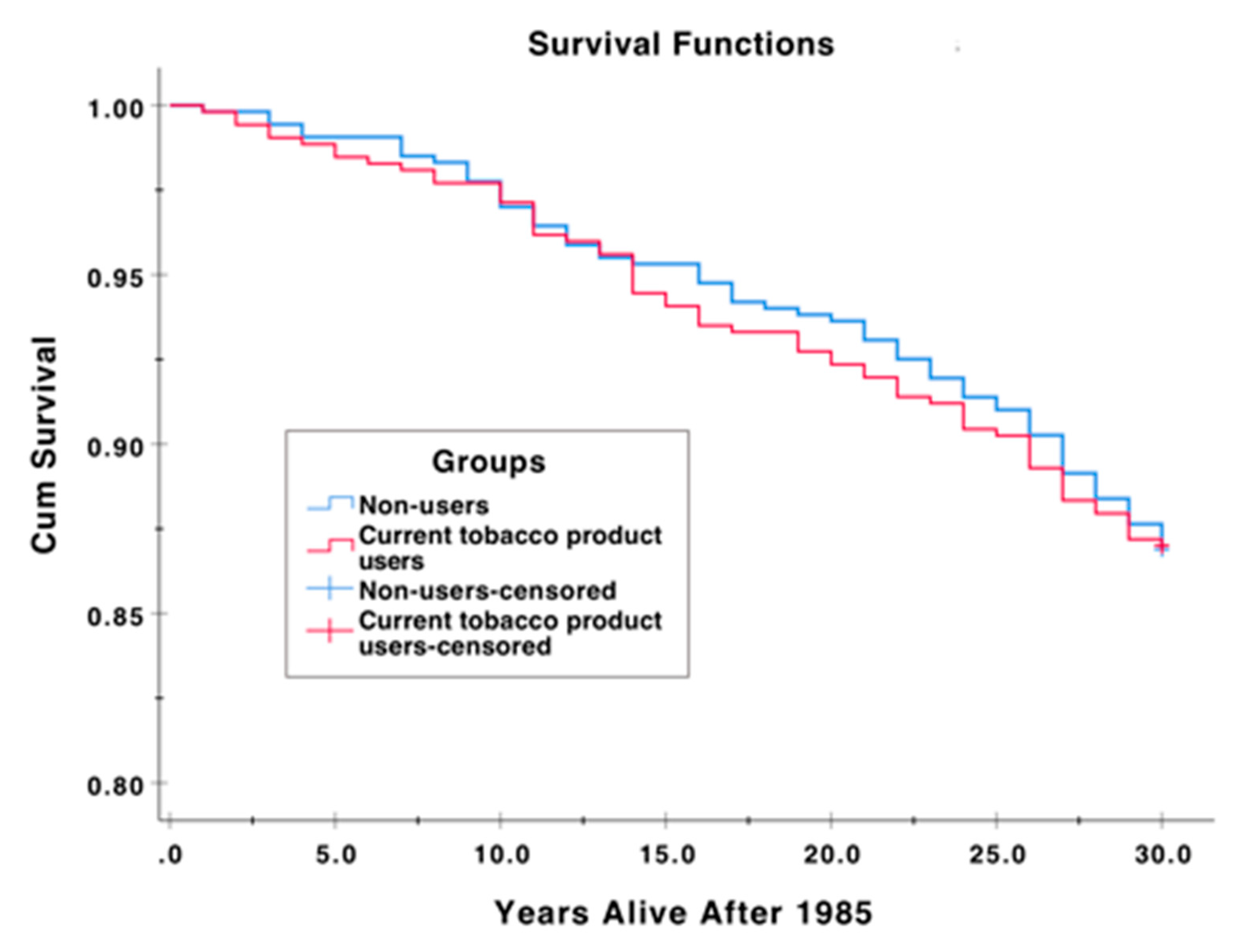
| Current tobacco product users | 66.00 (64.00–68.00) | 55.00 (46.00–60.00) | 28.34 (27.89–28.79) | Log Rank (Mantel-Cox) | 0.993 |
| Non-users | 65.00 (63.00–68.00) | 55.00 (48.50–62.00) | 28.52 (28.10–28.94) | Breslow (Generalized Wilcoxon) | 0.974 |
| Overall | 66.00 (63.00–68.00) | 55.00 (47.00–61.75) | 28.43 (28.13–28.74) | Tarone-Ware | 0.991 |
| Current Tobacco Product Users ICD Codes | Non-Users of Tobacco Products ICD Codes |
|---|---|
| 162x, 205A, 214X, 234, 296X, 303X, 401.99, 401X, 413X, 427.99, 427A, 427D, 431X, 454X, 585X, 615.2, 969E, 996W, A151, A410, C155, C229, C240, C249, C450, C509, C549, C619, C669, C679, C739, D333, E119, I120, I200, I209, I212, K269, K439, K572, K823, K830, K838, M161, R074, R119, R568. | 233.99, 428X, 428X, 450.01, 454.99,456B, 493X, A469, C509, C509, C509, C787, F019, F101, G408, G473, G479, I209, I214, I269, I420, I420, I471, I509, I509, I802, I803, I872, K253, K620, M165, R060, R061, R519, R568. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Julkunen-Iivari, A.; Heikkinen, A.M.; Räisänen, I.T.; Ruokonen, H.; Meurman, J.H.; Toppila-Salmi, S.; Söder, P.-Ö.; Söder, B. Tobacco Products, Periodontal Health and Education Level: Cohort Study from Sweden. Dent. J. 2020, 8, 90. https://doi.org/10.3390/dj8030090
Julkunen-Iivari A, Heikkinen AM, Räisänen IT, Ruokonen H, Meurman JH, Toppila-Salmi S, Söder P-Ö, Söder B. Tobacco Products, Periodontal Health and Education Level: Cohort Study from Sweden. Dentistry Journal. 2020; 8(3):90. https://doi.org/10.3390/dj8030090
Chicago/Turabian StyleJulkunen-Iivari, Anna, Anna Maria Heikkinen, Ismo T. Räisänen, Hellevi Ruokonen, Jukka H. Meurman, Sanna Toppila-Salmi, Per-Östen Söder, and Birgitta Söder. 2020. "Tobacco Products, Periodontal Health and Education Level: Cohort Study from Sweden" Dentistry Journal 8, no. 3: 90. https://doi.org/10.3390/dj8030090
APA StyleJulkunen-Iivari, A., Heikkinen, A. M., Räisänen, I. T., Ruokonen, H., Meurman, J. H., Toppila-Salmi, S., Söder, P.-Ö., & Söder, B. (2020). Tobacco Products, Periodontal Health and Education Level: Cohort Study from Sweden. Dentistry Journal, 8(3), 90. https://doi.org/10.3390/dj8030090