Effect of Decontamination and Cleaning on the Shear Bond Strength of High Translucency Zirconia

Abstract
1. Introduction
2. Results
3. Discussion
4. Materials and Methods
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Blatz, M.B.; Alvarez, M.; Sawyer, K.; Brindis, M. How to bond zirconia: The APC Concept. Compend. Cont. Educ. Dent. 2016, 37, 611–617. [Google Scholar]
- Tzanakakis, E.G.; Tzoutzas, I.G.; Koidis, P.T. Is there a potential for durable adhesion to zirconia restorations? A systematic review. J. Prosthet. Dent. 2016, 115, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Xie, H.; Li, Q.; Zhang, F.; Lu, Y.; Tay, F.R.; Qian, M.; Chen, C. Comparison of resin bonding improvements to zirconia between one-bottle universal adhesives and tribochemical silica coating, which is better? Dent. Mater. 2016, 32, 403–441. [Google Scholar] [CrossRef] [PubMed]
- El-Damanhoury, H.M.; Gaintantzopoulou, M.D. Self-etching ceramic primer versus hydrofluoric acid etching: Etching efficacy and bonding performance. J. Prosthodont. Res. 2017. [Google Scholar] [CrossRef] [PubMed]
- Román-Rodríguez, J.L.; Perez-Barquero, J.A.; Gonzalez-Angulo, E.; Fons-Font, A.; Bustos-Salvador, J.L. Bonding to silicate ceramics: Conventional technique compared with a simplified technique. J. Clin. Exp. Dent. 2017, 9, 384–386. [Google Scholar] [CrossRef] [PubMed]
- Bielen, V.; Inokoshi, M.; Munck, J.D.; Zhang, F.; Vanmeensel, K.; Minakuchi, S.; Vleugels, J.; Naert, I.; Van Meerbeek, B. Bonding Effectiveness to Differently Sandblasted Dental Zirconia. J. Adhes. Dent. 2015, 17, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Elsaka, S.E. Influence of Surface Treatments on the Bond Strength of Resin Cements to Monolithic Zirconia. J. Adhes. Dent. 2016, 18, 387–395. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.A.; Al Kheraif, A.A.; Jamaluddin, S.; Elsharawy, M.; Divakar, D.D. Recent Trends in Surface Treatment Methods for Bonding Composite Cement to Zirconia: A Review. J. Adhes. Dent. 2017, 19, 7–19. [Google Scholar] [CrossRef] [PubMed]
- Aladağ, A.; Elter, B.; Çömlekoğlu, E.; Kanat, B.; Sonugelen, M.; Kesercioğlu, A.; Özcan, M. Effect of different cleaning regimens on the adhesion of resin to saliva-contaminated ceramics. J. Prosthodont. 2015, 24, 136–145. [Google Scholar] [CrossRef] [PubMed]
- Angkasith, P.; Burgess, J.O.; Bottino, M.C.; Lawson, N.C. Cleaning Methods for Zirconia Following Salivary Contamination. J. Prosthodont. 2016, 25, 375–379. [Google Scholar] [CrossRef] [PubMed]
- Fraga, S.; Oliveira, S.C.; Pereira, G.K.; Beekman, P.; Rippe, M.P.; Kleverlaan, C.J. Silicone Disclosing Material used after Ceramic Surface Treatment Reduces Bond Strength. J. Adhes. Dent. 2016, 18, 545–554. [Google Scholar] [CrossRef] [PubMed]
- Feitosa, S.A.; Pater, D.; Borges, A.L.S.; Alshehri, E.Z.; Bottino, M.A.; Özcan, M.; Valandro, L.F.; Bottino, M.C. Effect of cleansing methods on saliva-contaminated Zirconia—An evaluation of resin bond durability. Oper. Dent. 2015, 40, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Son, J.S.; Jeong, S.H.; Kim, Y.K.; Kim, K.H.; Kwon, T.Y. Efficacy of various cleaning solutions on saliva-contaminated zirconia for improved resin bonding. J. Adv. Prosthodont. 2015, 7, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.; Lange-Jansen, H.; Scharnberg, M.; Wolfart, S.; Ludwig, K.; Adelung, R.; Kern, M. Influence of saliva contamination on zirconia ceramic bonding. Dent. Mater. 2008, 24, 508–513. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Niu, L.; Wang, Y.; Jiao, K.; Liu, Y.; Zhou, W.; Shen, L.; Fang, M.; Li, M.; Zhang, X.; et al. Bonding of Resin Cement to Zirconia with High Pressure Primer Coating. PLoS ONE 2014, 9, e101174. [Google Scholar] [CrossRef] [PubMed]
- Attia, A. Bond strength of three luting agents to zirconia ceramic—Influence of surface treatment and thermocycling. J. Appl. Oral. Sci. 2011, 19, 388–395. [Google Scholar] [CrossRef] [PubMed]
- Prasad, H.A.; Pasha, N.; Hilal, M.; Amarnath, G.S.; Kundapur, V.; Anand, M.; Singh, S. To Evaluate Effect of Airborne Particle Abrasion using Different Abrasives Particles and Compare Two Commercial Available Zirconia on Flexural Strength on Heat Treatment. Int. J. Biomed. Sci. 2017, 13, 93–112. [Google Scholar] [PubMed]
- Scribante, A.; Contreras-Bulnes, R.; Montasser, M.A.; Vallittu, P.K. Orthodontics: Bracket Materials, Adhesives Systems, and Their Bond Strength. Biomed. Res. Int. 2016, 2016, 1329814. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, I.R. A review of direct orthodontic bonding. Br. J. Orthod. 1975, 2, 171–178. [Google Scholar] [CrossRef]
- Giannini, M.; Soares, C.J.; de Carvalho, R.M. Ultimate tensile strength of tooth structures. Dent. Mater. 2004, 20, 322–329. [Google Scholar] [CrossRef]
- Hannig, C.; Hannig, M.; Attin, T. Enzymes in the acquired enamel pellicle. Eur. J. Oral. Sci. 2005, 113, 2–13. [Google Scholar] [CrossRef] [PubMed]
- Nagaoka, N.; Yoshihara, K.; Feitosa, V.P.; Tamada, Y.; Irie, M.; Yoshida, Y.; Van Meerbeek, B.; Hayakawa, S. Chemical interaction mechanism of 10-MDP with zirconia. Sci. Rep. 2017, 7, 45563. [Google Scholar] [CrossRef] [PubMed]
- Pitta, J.; Branco, T.C.; Portugal, J. Effect of saliva contamination and artificial aging on different primer/cement systems bonded to zirconia. J. Prosthet. Dent. 2017. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, F.; Cardenas, A.M.; Gutierrez, M.F.; Malaquias, P.; Hass, V.; Reis, A.; Loguercio, A.D.; Perdigão, J. Laboratory Performance of Universal Adhesive Systems for Luting CAD/CAM Restorative Materials. J. Adhes. Dent. 2016, 18, 331–340. [Google Scholar] [CrossRef] [PubMed]
- Behr, M.; Proff, P.; Kolbeck, C.; Langrieger, S.; Kunze, J.; Handel, G.; Rosentritt, M. The bond strength of the resin-to-zirconia interface using different bonding concepts. J. Mech. Behav. Biomed. Mater. 2011, 4, 2–8. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
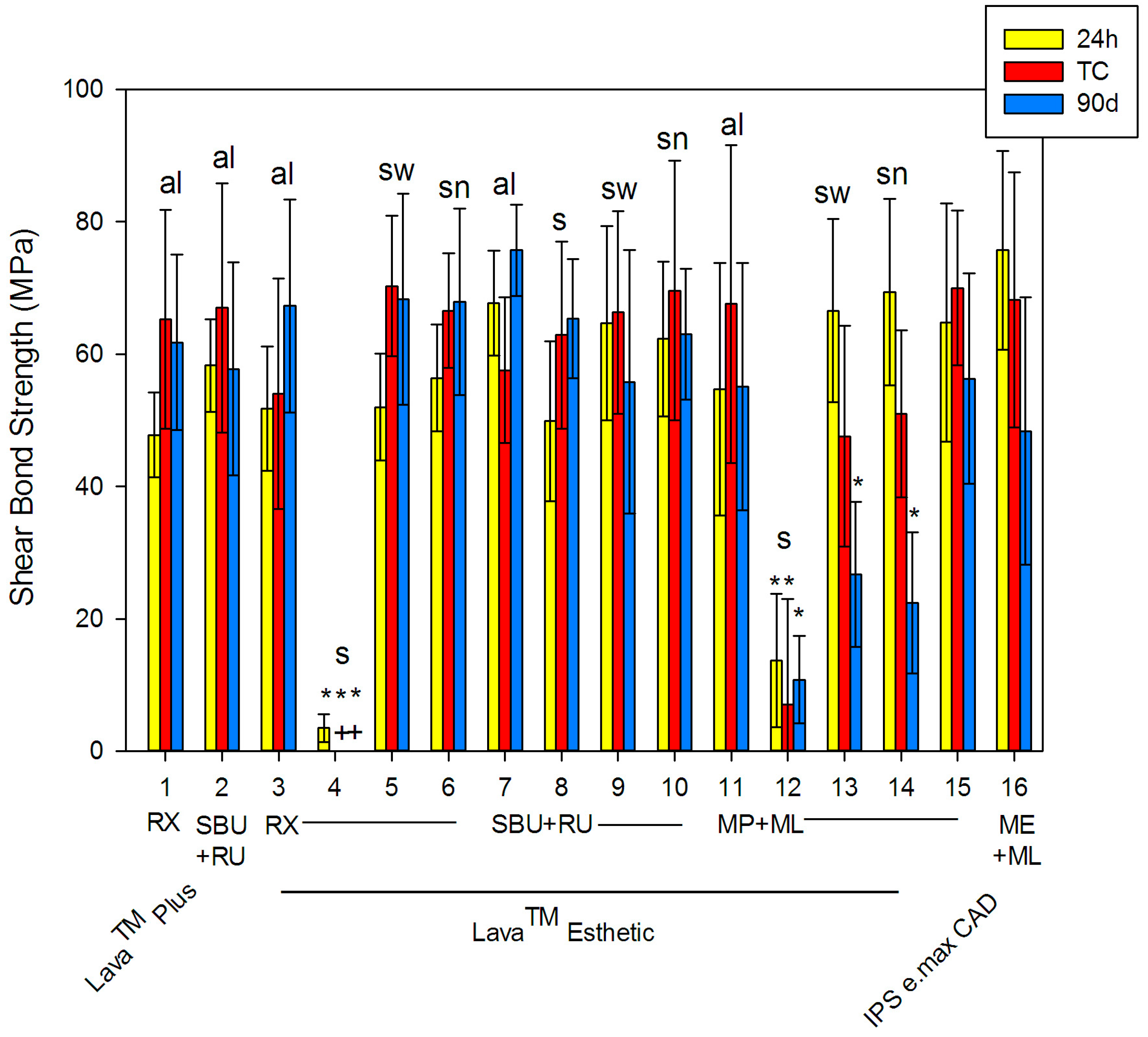
| # | Ceramic | Pre-Treatment | Procedure | Primer | Cement | Mean (SD) | ||
|---|---|---|---|---|---|---|---|---|
| 24 h | TC | 90 days | ||||||
| 1 | Lava™ Plus | sandblasting | al | none | RX | 47.8 (6.4) | 65.3 (16.5) | 61.8 (13.3) |
| 2 | SBU | RU | 58.3 (7.0) | 67.0 (18.8) | 57.8 (16.1) | |||
| 3 | Lava™ Esthetic | al | none | RX | 51.8 (9.4) | 54.0 (17.4) | 67.3 (16.1) | |
| 4 | s | 3.5 * (2.1) | 0 * (0) | 0 * (0) | ||||
| 5 | sw | 52.0 (8.1) | 70.3 (10.6) | 68.3 (15.9) | ||||
| 6 | sn | 56.4 (8.1) | 66.6 (8.7) | 67.9 (14.1) | ||||
| 7 | al | SBU | RU | 67.7 (7.9) | 57.6 (11.0) | 75.7 (6.9) | ||
| 8 | s | 49.9 (12.1) | 62.9 (14.1) | 65.4 (9.0) | ||||
| 9 | sw | 64.7 (14.7) | 66.3 (15.3) | 55.8 (19.9) | ||||
| 10 | sn | 62.3 (11.7) | 69.6 (19.6) | 63.0 (9.9) | ||||
| 11 | al | MP | ML | 54.7 (19.1) | 67.6 (24.0) | 55.1 (18.7) | ||
| 12 | s | 13.7 * (10.1) | 7.0 * (16.0) | 10.8 * (6.6) | ||||
| 13 | sw | 66.6 (13.8) | 47.6 (16.7) | 26.7 * (11.0) | ||||
| 14 | sn | 69.4 (14.1) | 51.0 (12.6) | 22.4 * (10.7) | ||||
| 15 | IPS e.max CAD | 5% HF | none | MP | 64.8 (18.0) | 70.0 (11.7) | 56.3 (15.9) | |
| 16 | none | ME | 75.7 (15.0) | 68.2 (19.3) | 48.4 (20.2) | |||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krifka, S.; Preis, V.; Rosentritt, M. Effect of Decontamination and Cleaning on the Shear Bond Strength of High Translucency Zirconia. Dent. J. 2017, 5, 32. https://doi.org/10.3390/dj5040032
Krifka S, Preis V, Rosentritt M. Effect of Decontamination and Cleaning on the Shear Bond Strength of High Translucency Zirconia. Dentistry Journal. 2017; 5(4):32. https://doi.org/10.3390/dj5040032
Chicago/Turabian StyleKrifka, Stephanie, Verena Preis, and Martin Rosentritt. 2017. "Effect of Decontamination and Cleaning on the Shear Bond Strength of High Translucency Zirconia" Dentistry Journal 5, no. 4: 32. https://doi.org/10.3390/dj5040032
APA StyleKrifka, S., Preis, V., & Rosentritt, M. (2017). Effect of Decontamination and Cleaning on the Shear Bond Strength of High Translucency Zirconia. Dentistry Journal, 5(4), 32. https://doi.org/10.3390/dj5040032