
Longitudinal Assessment of Dental Erosion in a Romanian Cohort of Young Adults: A Ten-Year Follow-Up Pilot Study

Abstract
1. Introduction
- To assess the ten-year incidence of dental erosion in a cohort of healthy young adults using the BEWE index.
- To investigate whether gender or other demographic factors are associated with the development of new erosive lesions.
- To evaluate the sensitivity of the digital surface analysis in detecting early or localized erosive changes not captured by BEWE.
- To validate clinical findings through 3D digital surface loss analysis using intraoral scanning and quantitative measurement of enamel wear.
2. Materials and Methods
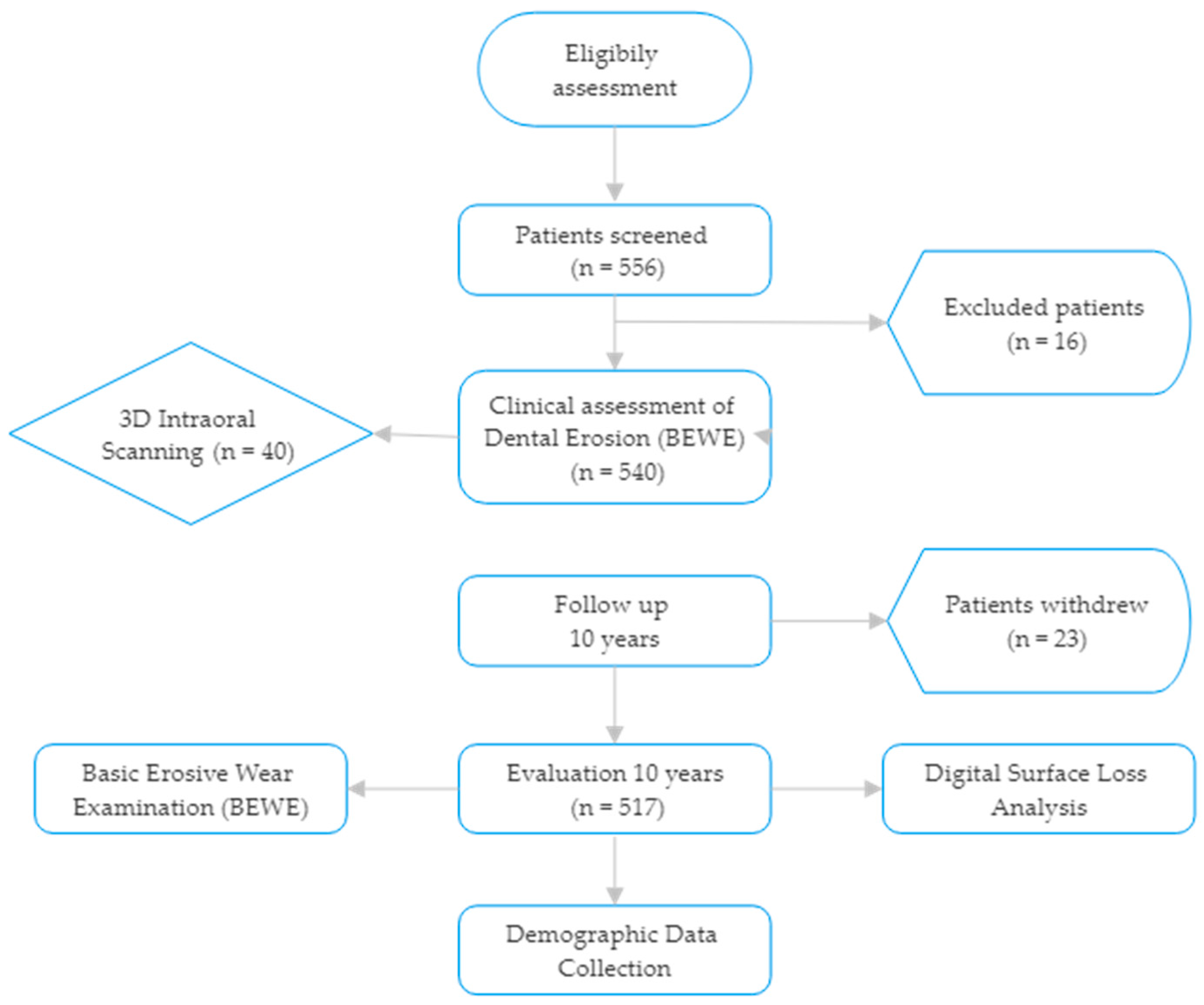
2.1. Study Design and Ethical Approval
Participant Selection and Follow-Up
- Diagnosed with gastroesophageal reflux disease (GERD) or eating disorders.
- Use of medications causing xerostomia.
- Fixed orthodontic appliances or extensive restorations affecting enamel integrity.
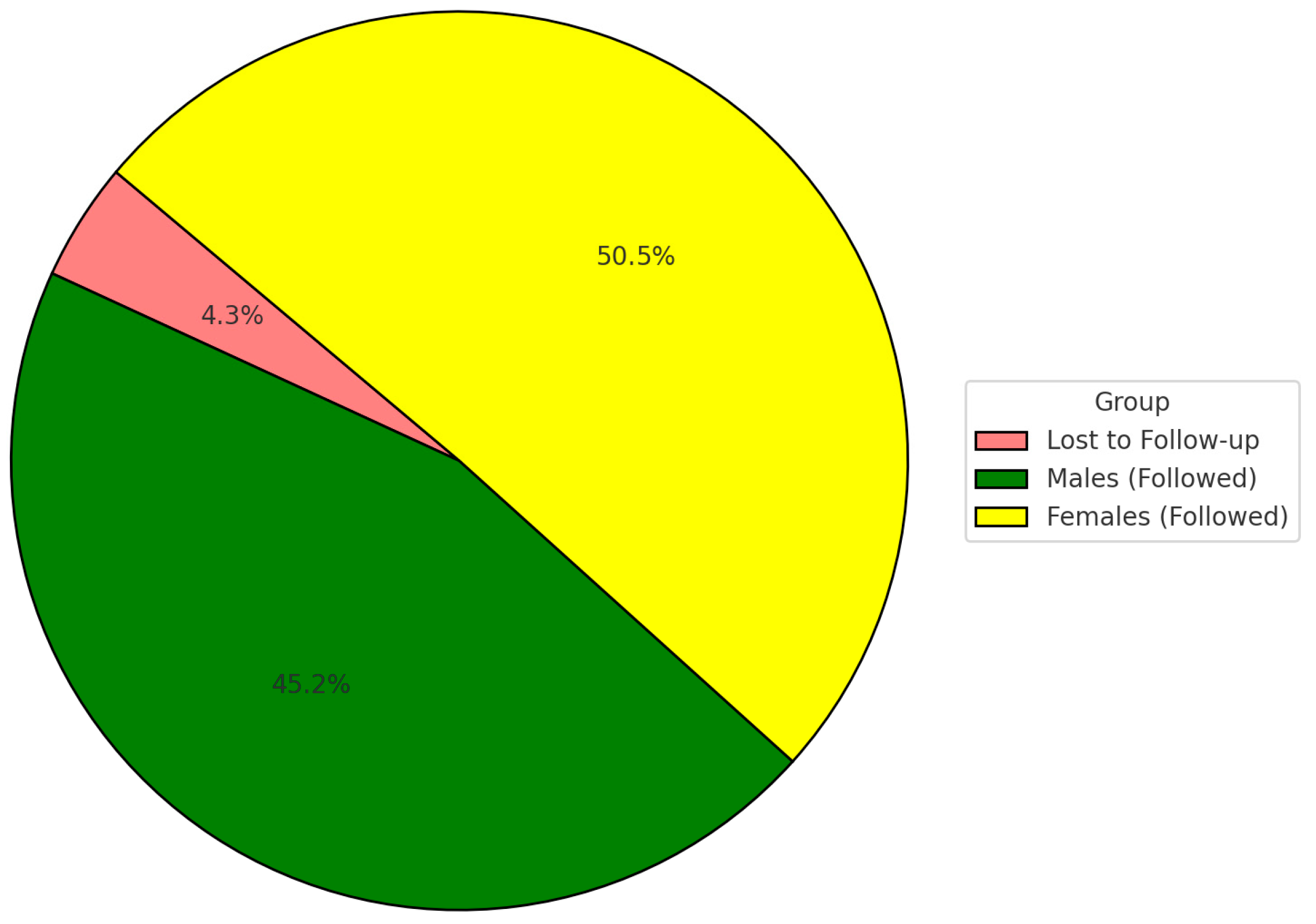
- At the 2024 follow-up, 517 participants (95.7%) were successfully re-examined; 23 participants were lost to follow-up.
2.2. Clinical Assessment of Dental Erosion
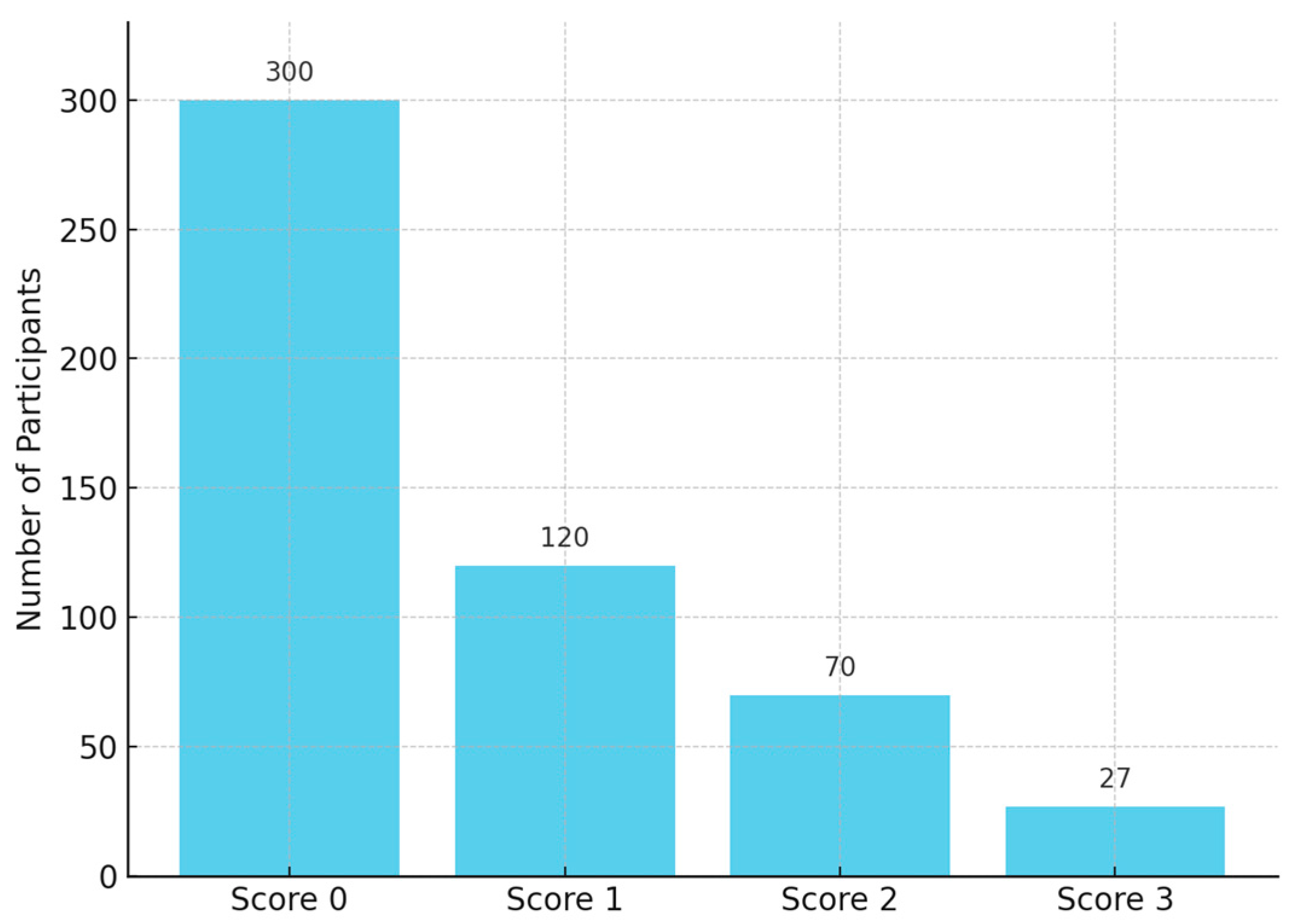
2.2.1. Basic Erosive Wear Examination (BEWE)
2.2.2. Digital Surface Loss Analysis (3D Intraoral Scanning)
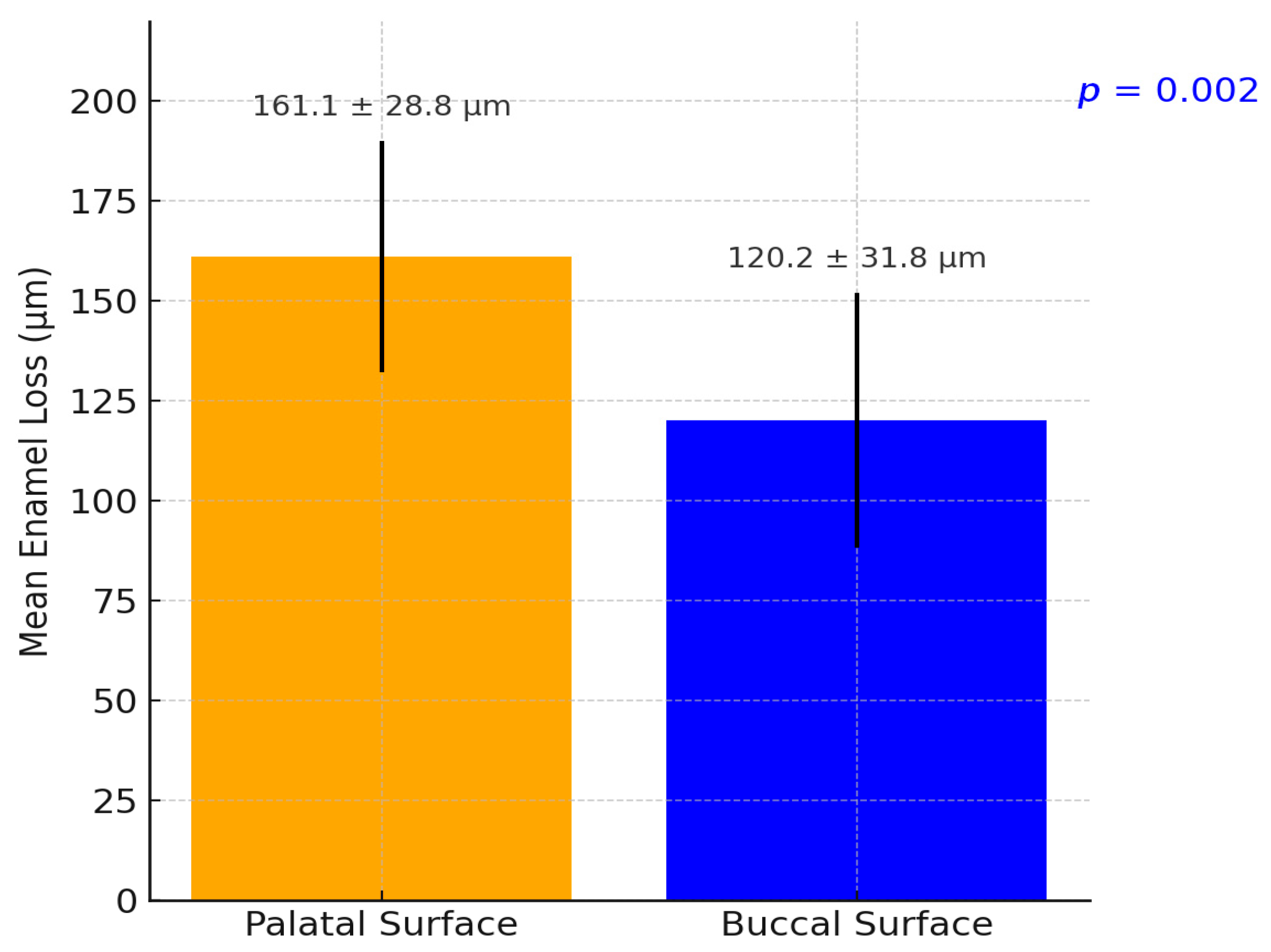
- Mean enamel loss per participant (in microns);
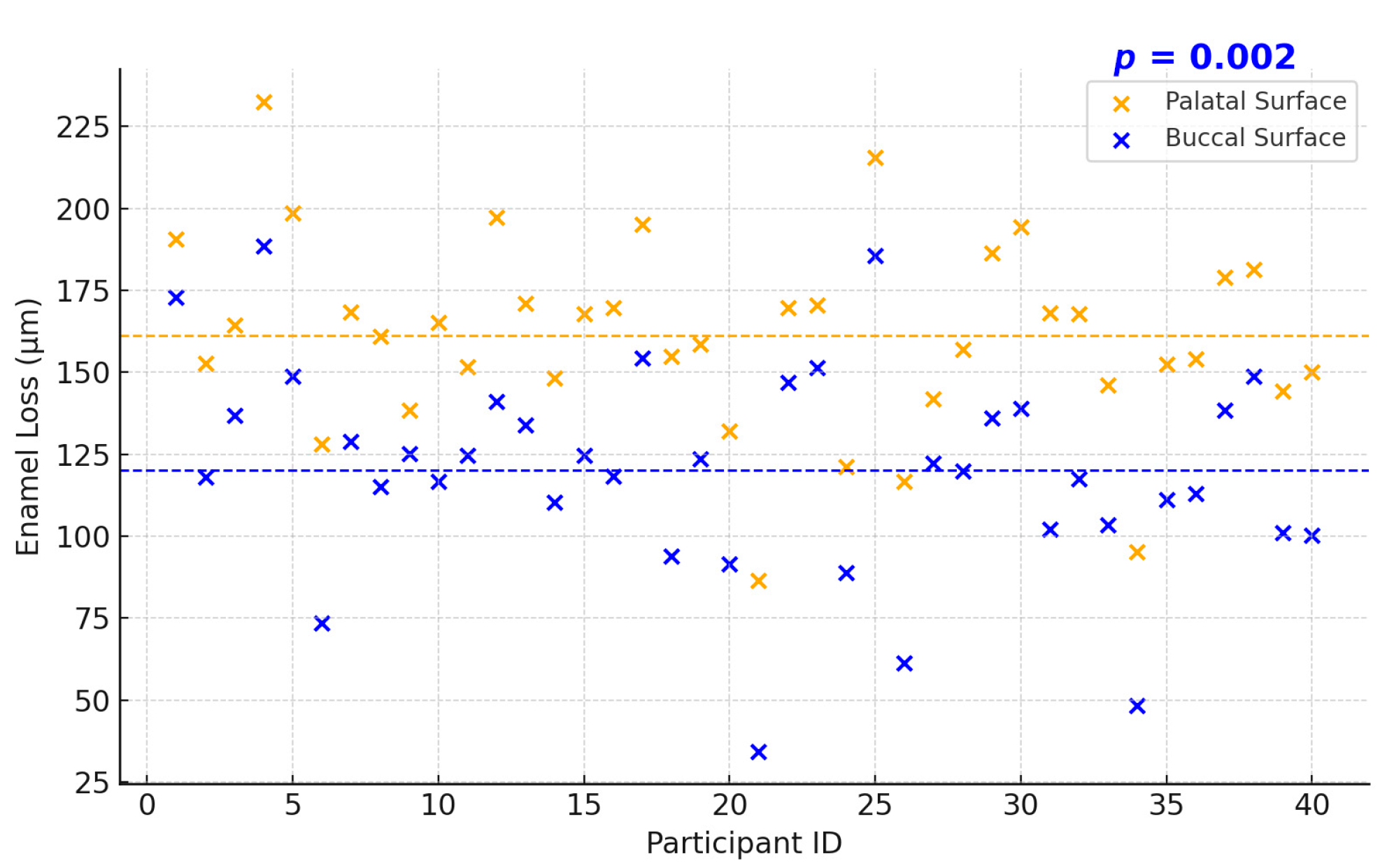
- Localization of wear (palatal vs. buccal surfaces);
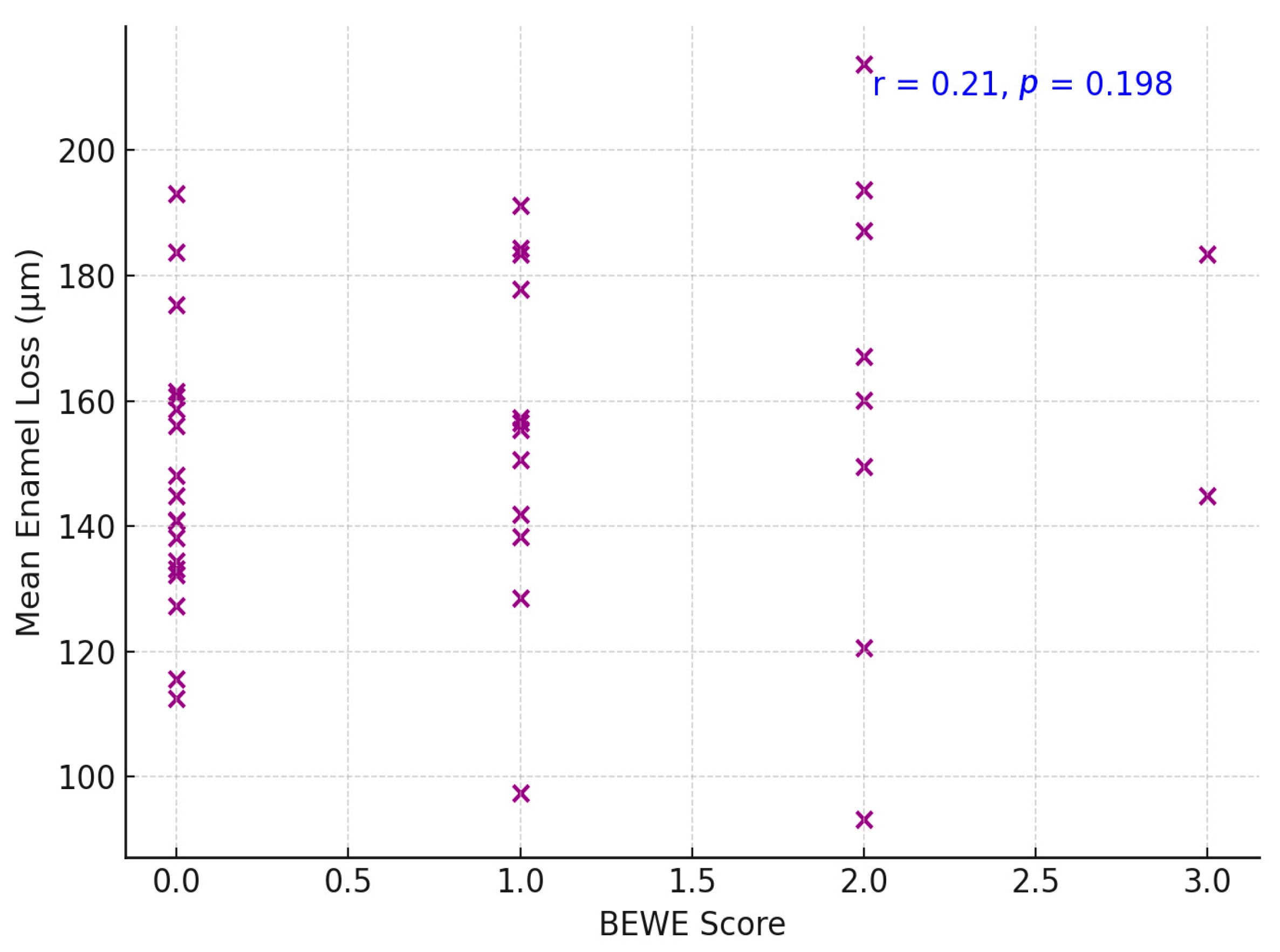
- Correlation with BEWE score and intraoral scanning.
2.2.3. Demographic Data Collection
2.2.4. Statistical Analysis
- Chi-square tests for gender differences in erosion incidence;
- Relative risk (RR) with 95% confidence intervals (CI);
- Pearson’s correlation coefficient to evaluate the relationship between clinical scores and 3D enamel loss;
- Statistical significance was set at p < 0.05.
3. Results
3.1. Participant Characteristics
Dental Erosion Incidence
3.2. Localization of Enamel Loss: Palatal vs. Buccal Surfaces
4. Discussion
4.1. Gender Differences in Erosion Risk and Severity
4.2. BEWE Index vs. Three-Dimensional Scanning: Diagnostic Accuracy and Correlation
5. Conclusions
- Longitudinal Erosion Rates: The Romanian 10-year study confirms that dental erosion accumulates appreciably in young adults over time, in line with global data. International longitudinal studies report a substantial 5–10 year incidence of erosive wear in this age group (on the order of tens of percent), with prevalence often rising from around one-quarter in the late teens to over one-third or more by the late twenties.
- Gender Differences: Males consistently show higher susceptibility to dental erosion than females. Romanian findings and worldwide evidence concur that young men experience higher incidence and greater severity of erosive tooth wear than women of similar age. Behavioral factors (e.g., more acidic drink consumption) and possible biological differences likely contribute to this male predominance.
- Diagnostic Methodologies: There is a meaningful difference between clinical index scoring and digital detection of erosion. The BEWE index is practical for in vivo assessment but may underestimate early or localized erosions, whereas 3D intraoral scanning can detect and measure very initial enamel wear with high sensitivity. Studies show only moderate agreement between BEWE scores and digital measurements, implying that combining traditional and digital methods provides a more complete picture of erosive wear status.
- In summary, 3D scanning offers superior accuracy in quantifying erosion progression, while BEWE remains a valuable, validated tool for quick clinical evaluation—the two should be viewed as complementary in monitoring dental erosion.
- Additionally, advancements in 3D-printing technologies offer promising opportunities for the digital rehabilitation of dentitions affected by advanced erosive tooth wear, supporting the integration of additive manufacturing in restorative workflows. Furthermore, 3D-printing technologies may play an important role in the digital rehabilitation of erosively worn dentitions, offering additive manufacturing solutions for customized restorative treatment [28].
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schlueter, N.; Luka, B. Erosive tooth wear—A review on global prevalence and on its prevalence in risk groups. Br. Dent. J. 2018, 224, 364–370. [Google Scholar] [CrossRef] [PubMed]
- Avila, V.; Betlrán, E.O.; Cortés, A.; Usuga-Vacca, M.; Castellanos Parras, J.E.; Diaz-Baez, D.; Martignon, S. Prevalence of erosive tooth wear and associated risk factors in Colombian adolescents. Braz. Oral Res. 2024, 38, e050. [Google Scholar] [CrossRef]
- de la Parte-Serna, A.C.; Monticelli, F.; Pradas, F.; Lecina, M.; García-Giménez, A. Gender-Based Analysis of Oral Health Outcomes Among Elite Athletes. Sports 2025, 13, 133. [Google Scholar] [CrossRef]
- Quinchiguano Caraguay, M.A.; Amoroso Calle, E.E.; Idrovo Tinta, T.S.; Gil Pozo, J.A. Non-carious cervical lesions (NCCL): A review of the literature. RSD [Internet] 2023, 12, e26612541876. [Google Scholar] [CrossRef]
- Hasselkvist, A.; Arnrup, K. Prevalence and progression of erosive tooth wear among children and adolescents in a Swedish county, as diagnosed by general practitioners during routine dental practice. Heliyon 2021, 7, e07977. [Google Scholar] [CrossRef]
- Chan, A.S.; Tran, T.T.K.; Hsu, Y.H.; Liu, S.Y.S.; Kroon, J. A systematic review of dietary acids and habits on dental erosion in adolescents. Int. J. Paediatr. Dent. 2020, 30, 713–733. [Google Scholar] [CrossRef] [PubMed]
- Kong, W.; Ma, H.; Qiao, F.; Xiao, M.; Wang, L.; Zhou, L.; Chen, Y.; Liu, J.; Wang, Y.; Wu, L. Risk factors for noncarious cervical lesions: A case-control study. J. Oral Rehabil. 2024, 51, 1684–1691. [Google Scholar] [CrossRef] [PubMed]
- Methuen, M.; Kangasmaa, H.; Alaraudanjoki, V.K.; Suominen, A.L.; Anttonen, V.; Vähänikkilä, H.; Karjalainen, P.; Väistö, J.; Lakka, T.; Laitala, M.L. Prevalence of Erosive Tooth Wear and Associated Dietary Factors among a Group of Finnish Adolescents. Caries Res. 2022, 56, 477–487. [Google Scholar] [CrossRef]
- Jász, M.; Szőke, J. Dental Erosion and Its Relation to Potential Influencing Factors among 12-year-old Hungarian Schoolchildren. Oral Health Prev. Dent. 2022, 20, 95–102. [Google Scholar]
- Piórecka, B.; Jamka-Kasprzyk, M.; Niedźwiadek, A.; Jagielski, P.; Jurczak, A. Fluid Intake and the Occurrence of Erosive Tooth Wear in a Group of Healthy and Disabled Children from the Małopolska Region (Poland). Int. J. Environ. Res. Public Health 2023, 20, 4585. [Google Scholar] [CrossRef]
- West, N.X.; Davies, M.; Sculean, A.; Jepsen, S.; Faria-Almeida, R.; Harding, M.; Graziani, F.; Newcombe, R.G.; Creeth, J.E.; Herrera, D. Prevalence of dentine hypersensitivity, erosive tooth wear, gingival recession and periodontal health in seven European countries. J. Dent. 2024, 150, 105364. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, F.; Dipalma, G.; Azzollini, D.; Trilli, I.; Carpentiere, V.; Hazballa, D.; Bordea, I.R.; Palermo, A.; Inchingolo, A.D.; Inchingolo, A.M. Advances in Preventive and Therapeutic Approaches for Dental Erosion: A Systematic Review. Dent. J. 2023, 11, 274. [Google Scholar] [CrossRef] [PubMed]
- Tapalaga, G.; Bumbu, B.A.; Reddy, S.R.; Vutukuru, S.D.; Nalla, A.; Bratosin, F.; Fericean, R.M.; Dumitru, C.; Crisan, D.C.; Nicolae, N.; et al. The Impact of Prenatal Vitamin D on Enamel Defects and Tooth Erosion: A Systematic Review. Nutrients 2023, 15, 3863. [Google Scholar] [CrossRef]
- Aránguiz, V.; Lara, J.S.; Marró, M.L.; O’Toole, S.; Ramírez, V.; Bartlett, D. Recommendations and guidelines for dentists using the basic erosive wear examination index (BEWE). Br. Dent. J. 2020, 228, 153–157. [Google Scholar] [CrossRef]
- Bartlett, D.W.; Ganss, C.; Lussi, A. Basic Erosive Wear Examination (BEWE): A new scoring system for scientific and clinical needs. Clin. Oral Investig. 2008, 12 (Suppl. S1), S65–S68. [Google Scholar] [CrossRef]
- O’Toole, S.; Bartlett, D.; Keeling, A.; McBride, J.; Bernabe, E.; Crins, L.; Loomans, B. Influence of Scanner Precision and Analysis Software in Quantifying Three-Dimensional Intraoral Changes: Two-Factor Factorial Experimental Design. J. Med. Internet Res. 2020, 22, e17150. [Google Scholar] [CrossRef]
- Skalsky Jarkander, M.; Grindefjord, M.; Carlstedt, K. Dental erosion: Prevalence and risk factors among a group of adolescents in Stockholm County. Eur. Arch. Paediatr. Dent. 2018, 19, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Stenhagen, K.R.; Berntsen, I.; Ødegaard, M.; Mulic, A.; Tveit, A.B. Has the prevalence and severity of dental erosion in Norwegian adolescents changed over 30 years? Eur. J. Paediatr. Dent. 2017, 18, 178–184. [Google Scholar]
- Hasselkvist, A.; Johansson, A.; Johansson, A.K. A 4-year longitudinal study of progression of dental erosion in Swedish adolescents. J. Dent. 2016, 47, 55–62. [Google Scholar] [CrossRef]
- Bratu, D.C.; Mihali, S.G.; Popa, G.; Dragoş, B.; Bratu, R.C.; Matichescu, A.; Loloș, D.; Boloș, O. The Prevalence of Dental Erosion in Young Adults—A Quantitative Approach. Med. Evol. 2024, 30, 40–50. [Google Scholar] [CrossRef]
- Søvik, J.B.; Skudutyte-Rysstad, R.; Tveit, A.B.; Sandvik, L.; Mulic, A. Sour Sweets and Acidic Beverage Consumption Are Risk Indicators for Dental Erosion. Caries Res. 2015, 49, 243–250. [Google Scholar] [CrossRef]
- Uhlen, M.M.; Stenhagen, K.R.; Dizak, P.M.; Holme, B.; Mulic, A.; Tveit, A.B.; Vieira, A.R. Genetic variation may explain why females are less susceptible to dental erosion. Eur. J. Oral Sci. 2016, 124, 426–432. [Google Scholar] [CrossRef] [PubMed]
- Avila, V.; Beltrán, E.O.; Cortés, A.; Usuga-Vacca, M.; Castellanos Parras, J.E.; Díaz-Báez, D.; Martignon, S. Prevalence of erosive tooth wear and associated risk factors in Colombian adolescents. Braz. Oral Res. 2024, 38, e050. [Google Scholar]
- Alaraudanjoki, V.; Saarela, H.; Pesonen, R.; Laitala, M.L.; Kiviahde, H.; Tjäderhane, L.; Lussi, A.; Pesonen, P.; Anttonen, V. Is a Basic Erosive Wear Examination (BEWE) reliable for recording erosive tooth wear on 3D models? J. Dent. 2017, 59, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Mitrirattanakul, S.; Neoh, S.P.; Chalarmchaichaloenkit, J.; Limthanabodi, C.; Trerayapiwat, C.; Pipatpajong, N.; Taechushong, N.; Chintavalakorn, R. Accuracy of the Intraoral Scanner for Detection of Tooth Wear. Int. Dent. J. 2023, 73, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Al-Seelawi, Z.; Hermann, N.V.; Peutzfeldt, A.; Baram, S.; Bakke, M.; Sonnesen, L.; Tsakanikou, A.; Rahiotis, C.; Benetti, A.R. Clinical and digital assessment of tooth wear. Sci. Rep. 2024, 14, 592. [Google Scholar] [CrossRef]
- Margaritis, V.; Mamai-Homata, E.; Koletsi-Kounari, H. Novel methods of balancing covariates for the assessment of dental erosion: A contribution to validation of a synthetic scoring system for erosive wear. J. Dent. 2011, 39, 361–367. [Google Scholar] [CrossRef]
- Patrício, T.; Domingos, M.; Gloria, A.; Bartolo, P.J. Advanced Additive Manufacturing Technologies for the Production of Oral and Maxillofacial Implants. Materials 2012, 17, 1380. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gender | Participants (n) | With Erosion (n %) | Without Erosion (n %) |
|---|---|---|---|
| Males | 244 | 73 (29.9%) | 171 (70.1%) |
| Females | 273 | 47 (17.2%) | 226 (82.8%) |
| Total | 517 | 120 (23.2%) | 397 (76.8%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bors, A.; Beresescu, F.G.; Szekely, M. Longitudinal Assessment of Dental Erosion in a Romanian Cohort of Young Adults: A Ten-Year Follow-Up Pilot Study. Dent. J. 2025, 13, 302. https://doi.org/10.3390/dj13070302
Bors A, Beresescu FG, Szekely M. Longitudinal Assessment of Dental Erosion in a Romanian Cohort of Young Adults: A Ten-Year Follow-Up Pilot Study. Dentistry Journal. 2025; 13(7):302. https://doi.org/10.3390/dj13070302
Chicago/Turabian StyleBors, Andrea, Felicia Gabriela Beresescu, and Melinda Szekely. 2025. "Longitudinal Assessment of Dental Erosion in a Romanian Cohort of Young Adults: A Ten-Year Follow-Up Pilot Study" Dentistry Journal 13, no. 7: 302. https://doi.org/10.3390/dj13070302
APA StyleBors, A., Beresescu, F. G., & Szekely, M. (2025). Longitudinal Assessment of Dental Erosion in a Romanian Cohort of Young Adults: A Ten-Year Follow-Up Pilot Study. Dentistry Journal, 13(7), 302. https://doi.org/10.3390/dj13070302