
In Vitro Comparison of Three Intraoral Scanners for Implant—Supported Dental Prostheses


 , ,
, ,  and
and 
Abstract
:1. Introduction
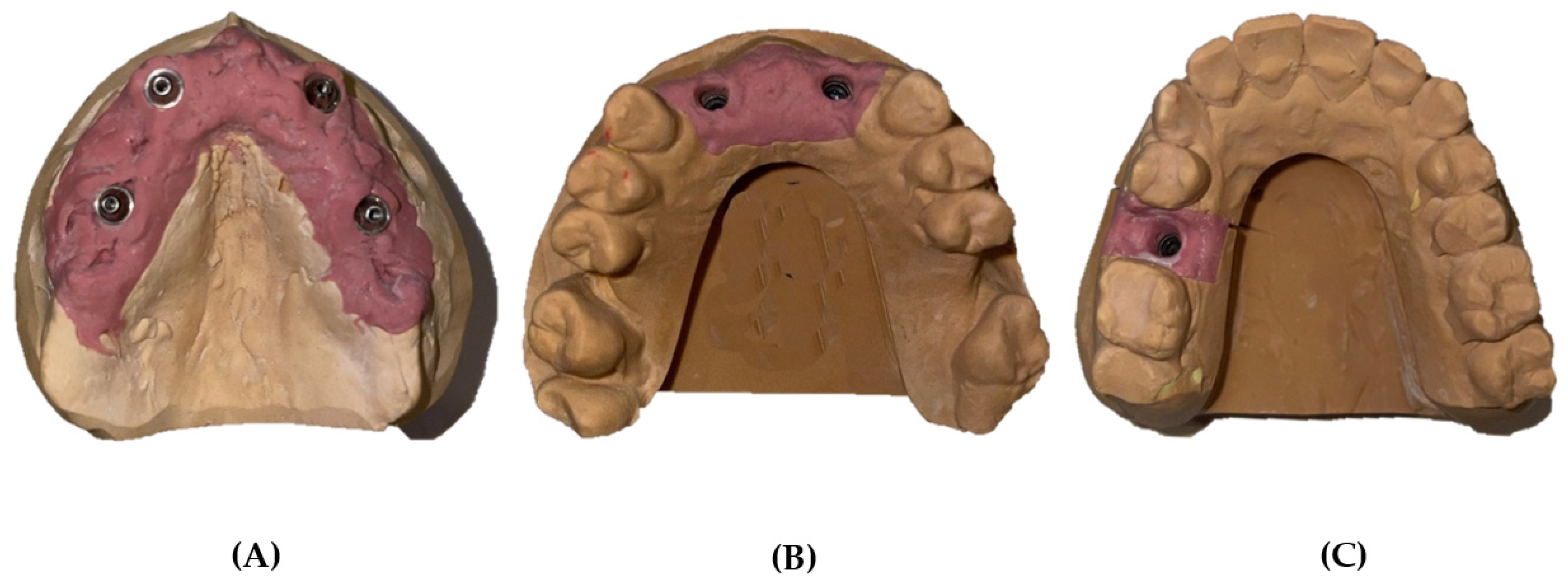
2. Materials and Methods
2.1. S6OO ARTI Extraoral Scanner
2.2. Intraoral Scanners
2.2.1. iTero® Element Plus Series
2.2.2. Medit® i500
2.2.3. Planmeca® PlanScan
2.3. Alignment and Measurement Procedures
2.4. Datasets and Statistical Analysis
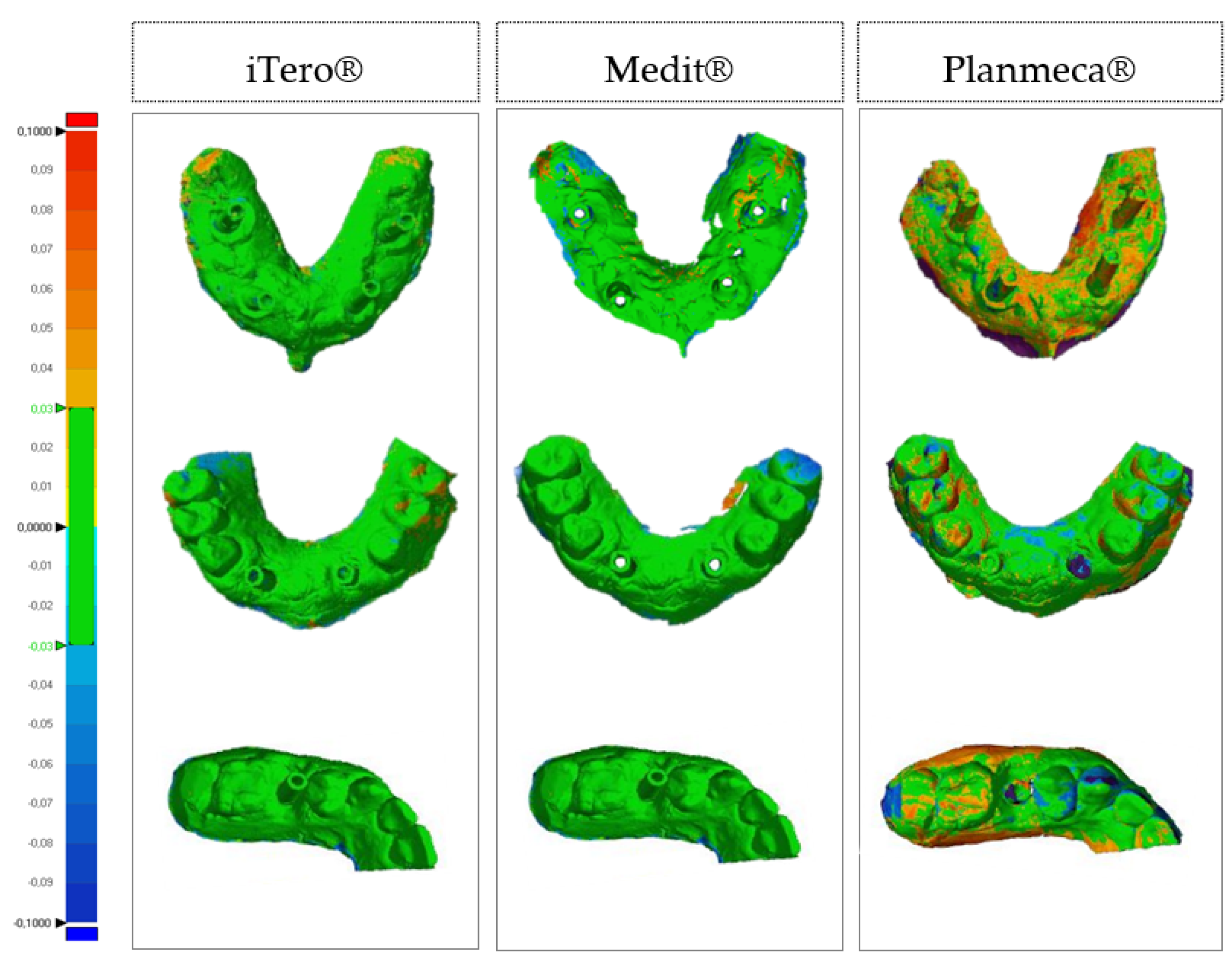
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Joda, T.; Zarone, F.; Ferrari, M. The complete digital workflow in fixed prosthodontics: A systematic review. BMC Oral Health 2017, 17, 124. [Google Scholar] [CrossRef] [PubMed]
- Medina-Sotomayor, P.; Pascual-Moscardo, A.; Camps, I. Accuracy of four digital scanners according to scanning strategy in complete-arch impressions. PLoS ONE 2018, 13, e0202916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mangano, F.G.; Hauschild, U.; Veronesi, G.; Imburgia, M.; Mangano, C.; Admakin, O. Trueness and precision of 5 intraoral scanners in the impressions of single and multiple implants: A comparative in vitro study. BMC Oral Health 2018, 2018, 5325032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mangano, F.; Veronesi, G. Digital versus analog procedures for the prosthetic restoration of single implants: A randomized controlled trial with 1 year of follow-up. Biomed Res. Int. 2018, 2018, 5325032. [Google Scholar] [CrossRef] [Green Version]
- Güth, J.F.; Keul, C.; Stimmelmayr, M.; Beuer, F.; Edelhoff, D. Accuracy of digital models obtained by direct and indirect data capturing. Clin. Oral Investig. 2013, 17, 1201–1208. [Google Scholar] [CrossRef]
- Logozzo, S.; Zanetti, E.M.; Franceschini, G.; Kilpelä, A.; Mäkynen, A. Recent advances in dental optics—Part I: 3D intraoral scanners for restorative dentistry. Opt. Lasers Eng. 2014, 54, 203–221. [Google Scholar] [CrossRef]
- Galhano, G.A.P.; Pellizzer, E.P.; Mazaro, J.V.Q. Optical impression systems for CAD-CAM restorations. J. Craniofac. Surg. 2012, 23, e575–e579. [Google Scholar] [CrossRef]
- Sawase, T.; Kuroshima, S. The current clinical relevancy of intraoral scanners in implant dentistry. Dent. Mater. J. 2020, 39, 57–61. [Google Scholar] [CrossRef] [Green Version]
- Infante, L.; Yilmaz, B.; McGlumphy, E.; Finger, I. Fabricating complete dentures with CAD/CAM technology. J. Prosthet. Dent. 2014, 111, 351–355. [Google Scholar] [CrossRef]
- Patzelt, S.B.M.; Lamprinos, C.; Stampf, S.; Att, W. The time efficiency of intraoral scanners: An in vitro comparative study. J. Am. Dent. Assoc. 2014, 145, 542–551. [Google Scholar] [CrossRef] [Green Version]
- Suese, K. Progress in digital dentistry: The practical use of intraoral scanners. Dent. Mater. J. 2020, 39, 52–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Meer, W.J.; Andriessen, F.S.; Wismeijer, D.; Ren, Y. Application of intra-oral dental scanners in the digital workflow of implantology. PLoS ONE 2012, 7, e43312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ender, A.; Mehl, A. Accuracy of complete-arch dental impressions: A new method of measuring trueness and precision. J. Prosthet. Dent. 2012, 109, 121–128. [Google Scholar] [CrossRef] [Green Version]
- Ajioka, H.; Kihara, H.; Odaira, C.; Kobayashi, T.; Kondo, H. Examination of the position accuracy of implant abutments reproduced by intra-oral optical impression. PLoS ONE 2016, 11, e0164048. [Google Scholar] [CrossRef]
- Nedelcu, R.G.; Persson, A.S.K. Scanning accuracy and precision in 4 intraoral scanners: An in vitro comparison based on 3-dimensional analysis. J. Prosthet. Dent. 2014, 112, 1461–1471. [Google Scholar] [CrossRef]
- Van Noort, R. The future of dental devices is digital. Dent. Mater. 2012, 28, 3–12. [Google Scholar] [CrossRef]
- Ahlholm, P.; Sipilä, K.; Vallittu, P.; Jakonen, M.; Kotiranta, U. Digital versus conventional impressions in fixed prosthodontics: A review. J. Prosthodont. 2018, 27, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Ting-shu, S.; Jian, S. Intraoral digital impression technique: A review. J. Prosthodont. 2015, 24, 313–321. [Google Scholar] [CrossRef]
- Imburgia, M.; Logozzo, S.; Hauschild, U.; Veronesi, G.; Mangano, C.; Mangano, F.G. Accuracy of four intraoral scanners in oral implantology: A comparative in vitro study. BMC Oral Health 2017, 17, 92. [Google Scholar] [CrossRef]
- Mizumoto, R.M.; Yilmaz, B. Intraoral scan bodies in implant dentistry: A systematic review. J. Prosthet. Dent. 2018, 120, 343–352. [Google Scholar] [CrossRef]
- Bolding, S.L. Advanced Digital Implant Dentistry. 2012. Available online: https://dentalacademyofce.com/courses/2264/pdf/1206cei_implant_web.pdf (accessed on 6 January 2022).
- Mangano, F.G.; Veronesi, G.; Hauschild, U.; Mijiritsk, E.; Mangano, C. Trueness and precision of four intraoral scanners in oral implantology: A comparative in vitro study. PLoS ONE 2016, 11, e0163107. [Google Scholar] [CrossRef] [PubMed]
- Mutwalli, H.; Braian, M.; Mahmood, D.; Larsson, C. Trueness and precision of three-dimensional digitizing intraoral devices. Int. J. Dent. 2018, 2018, 5189761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- iTero Elemento 5D Plus. Available online: https://guides.itero.com/product/itero-Element-5D-plus?locale=pt (accessed on 8 July 2021).
- Medit i500. Available online: https://www.cad-ray.com/wp-content/uploads/2019/01/Medit-i500-User-Guide.pdf (accessed on 28 August 2021).
- Planmeca PlanScan the Ultimate Scanning Experience. Available online: http://publications.planmeca.com/Brochures/CAD_CAM/PlanScan_integrated_en_low.pdf (accessed on 2 September 2021).
- Marques, S.; Ribeiro, P.; Falcão, C.; Lemos, B.F.; Ríos-Carrasco, B.; Ríos-Santos, J.V.; Herrero-Climent, M. Digital impressions in implant dentistry: A literature review. Int. J. Environ. Res. Public Health 2021, 18, 1020. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Betensky, R.A.; Gianneschi, G.E.; Gallucci, G.O. Accuracy of digital versus conventional implant impressions. Clin. Oral Implants Res. 2015, 26, 715–719. [Google Scholar] [CrossRef] [PubMed]
- Flügge, T.; van der Meer, W.J.; Gonzalez, B.G.; Vach, K.; Wismeijer, D.; Wang, P. The accuracy of different dental impression techniques for implant-supported dental prostheses: A systematic review and meta-analysis. Clin. Oral Implants Res. 2018, 29 (Suppl. 16), 374–392. [Google Scholar] [CrossRef] [Green Version]
- ISO. International Standard CAD/CAM systems for indirect dental. Int. Organ. Stand. 2015, 2012, 1–8. [Google Scholar]
- Mangano, F.; Margiani, B.; Admakin, O. A novel full-digital protocol (SCAN-PLAN-MAKE-DONE®) for the design and fabrication of implant-supported monolithic translucent zirconia crowns cemented on customized hybrid abutments: A retrospective clinical study on 25 patients. Int. J. Environ. Res. Public Health 2019, 16, 317. [Google Scholar] [CrossRef] [Green Version]
- Porter, J.L.; Carrico, C.K.; Lindauer, S.J.; Tüfekçi, E. Comparison of intraoral and extraoral scanners on the accuracy of digital model articulation. J. Orthod. 2018, 45, 275–282. [Google Scholar] [CrossRef] [Green Version]
- Cicciù, M.; Fiorillo, L.; D’Amico, C.; Gambino, D.; Amantia, E.M.; Laino, L.; Crimi, S.; Campagna, P.; Bianchi, A.; Herford, A.S.; et al. 3D digital impression systems compared with traditional techniques in dentistry: A recent data systematic review. Materials 2020, 13, 1982. [Google Scholar] [CrossRef]
- Abduo, J.; Elseyoufi, M. Accuracy of intraoral scanners: A systematic review of influencing factors. Eur. J. Prosthodont. Restor. Dent. 2018, 26, 101–121. [Google Scholar]
- Fukazawa, S.; Odaira, C.; Kondo, H. Investigation of accuracy and reproducibility of abutment position by intraoral scanners. J. Prosthodont. Res. 2017, 61, 450–459. [Google Scholar] [CrossRef] [PubMed]
- Mangano, F.; Gandolfi, A.; Luongo, G.; Logozzo, S. Intraoral scanners in dentistry: A review of the current literature. BMC Oral Health 2017, 17, 149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kihara, H.; Hatakeyama, W.; Komine, F.; Takafuji, K.; Takahashi, T.; Yokota, J.; Oriso, K.; Kondo, H. Accuracy and practicality of intraoral scanner in dentistry: A literature review. J. Prosthodont. Res. 2020, 64, 109–113. [Google Scholar] [CrossRef] [PubMed]
- Giménez, B.; Pradíes, G.; Martínez-Rus, F.; Özcan, M. Accuracy of two digital implant impression systems based on confocal microscopy with variations in customized software and clinical parameters. Int. J. Oral Maxillofac. Implants 2015, 30, 56–64. [Google Scholar] [CrossRef] [Green Version]
- Gimenez-Gonzalez, B.; Hassan, B.; Özcan, M.; Pradíes, G. An in vitro study of factors influencing the performance of digital intraoral impressions operating on active wavefront sampling technology with multiple implants in the edentulous maxilla. J. Prosthodont. 2017, 26, 650–655. [Google Scholar] [CrossRef]
- Müller, P.; Ender, A.; Joda, T.; Katsoulis, J. Impact of digital intraoral scan strategies on the impression accuracy using the TRIOS Pod scanner. Quintessence Int. 2016, 47, 343–349. [Google Scholar]
- Flugge, T.V.; Att, W.; Metzger, M.C.; Nelson, K. Precision of dental implant digitization using intraoral scanners. Int. J. Prosthodont. 2016, 29, 277–283. [Google Scholar] [CrossRef] [Green Version]
- Papaspyridakos, P.; Chen, Y.W.; Alshawaf, B.; Kang, K.; Finkelman, M.; Chronopoulos, V. Digital workflow: In vitro accuracy of 3D printed casts generated from complete-arch digital implant scans. J. Prosthet. Dent. 2020, 124, 589–593. [Google Scholar] [CrossRef]
- Ender, A.; Mehl, A. In-vitro evaluation of the accuracy of conventional and digital methods of obtaining full-arch dental impressions. Quintessence Int. 2015, 46, 9–17. [Google Scholar]
- Yuzbasioglu, E.; Kurt, H.; Turunc, R.; Bilir, H. Comparison of digital and conventional impression techniques: Evaluation of patients’ perception, treatment comfort, effectiveness and clinical outcomes. BMC Oral Health 2014, 14, 10. [Google Scholar] [CrossRef] [Green Version]
- Wismeijer, D.; Mans, R.; van Genuchten, M.; Reijers, H.A. Patients’ preferences when comparing analogue implant impressions using a polyether impression material versus digital impressions (Intraoral Scan) of dental implants. Clin. Oral Implants Res. 2014, 25, 113–118. [Google Scholar] [CrossRef]
- Joda, T.; Lenherr, P.; Dedem, P.; Kovaltschuk, I.; Bragger, U.; Zitzmann, N.U. Time efficiency, difficulty, and operator’s preference comparing digital and conventional implant impressions: A randomized controlled trial. Clin. Oral Implants Res. 2017, 28, 1318–1323. [Google Scholar] [CrossRef]
- Ender, A.; Zimmermann, M.; Attin, T.; Mehl, A. In vivo precision of conventional and digital methods for obtaining quadrant dental impressions. Clin. Oral Investig. 2016, 20, 1495–1504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joda, T.; Brägger, U. Digital vs. conventional implant prosthetic workflows: A cost/time analysis. Clin. Oral Implants Res. 2015, 26, 1430–1435. [Google Scholar] [CrossRef] [PubMed]
- Joda, T.; Brägger, U. Complete digital workflow for the production of implant-supported single-unit monolithic crowns. Clin. Oral Implants Res. 2014, 25, 1304–1306. [Google Scholar] [CrossRef] [PubMed]
- Rutkunas, V.; Geciauskaite, A.; Jegelevicius, D.; Vaitiekunas, M. Accuracy of digital implant impressions with intraoral scanners. A systematic review. Eur. J. Oral Implants 2017, 10 (Suppl. 1), 101–120. [Google Scholar]
- Mühlemann, S.; Kraus, R.D.; Hämmerle, C.H.; Thoma, D.S. Is the use of digital technologies for the fabrication of implant-supported reconstructions more efficient and / or more effective than conventional techniques: A systematic review. Clin. Oral Implants Res. 2018, 29 (Suppl. 18), 184–195. [Google Scholar] [CrossRef]
- Kim, R.J.Y.; Benic, G.I.; Park, J.M. Trueness of digital intraoral impression in reproducing multiple implant position. PLoS ONE 2019, 14, e0222070. [Google Scholar] [CrossRef] [Green Version]
- Andriessen, F.S.; Rijkens, D.R.; Van Der Meer, W.J.; Wismeijer, D.W. Applicability and accuracy of an intraoral scanner for scanning multiple implants in edentulous mandibles: A pilot study. J. Prosthet. Dent. 2014, 111, 186–194. [Google Scholar] [CrossRef]
- Chochlidakis, K.; Papaspyridakos, P.; Tsigarida, A.; Romeo, D.; Chen, Y.-W.; Natto, Z.; Ercoli, C. Digital versus conventional full-arch implant impressions: A prospective study on 16 edentulous maxillae. J. Prosthodont. 2020, 29, 281–286. [Google Scholar] [CrossRef]
- Mühlemann, S.; Greter, E.A.; Park, J.-M.; Hämmerle, C.H.F.; Thoma, D.S. Precision of digital implant models compared to conventional implant models for posterior single implant crowns: A within-subject comparison. Clin. Oral Implants Res. 2018, 29, 931–936. [Google Scholar] [CrossRef] [PubMed]
- Koch, G.K.; Gallucci, G.O.; Lee, S.J. Accuracy in the digital workflow: From data acquisition to the digitally milled cast. J. Prosthet. Dent. 2016, 115, 749–764. [Google Scholar] [CrossRef] [PubMed]
- Chia, V.A.; Esguerra, R.J.; Teoh, K.H.; Teo, J.W.; Wong, K.M.; Tan, K.B. In vitro three-dimensional accuracy of digital implant impressions: The effect of implant angulation. Int. J. Oral Maxillofac. Implants 2017, 32, 313–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marghalani, A.; Weber, H.P.; Finkelman, M.; Kudara, Y.; El Rafie, K.; Papaspyridakos, P. Digital versus conventional implant impressions for partially edentulous arches: An evaluation of accuracy. J. Prosthet. Dent. 2017, 119, 574–579. [Google Scholar] [CrossRef]
- Chew, A.A.; Esguerra, R.J.; Teoh, K.H.; Wong, K.M.; Ng, S.D.; Tan, K.B. Three-dimensional accuracy of digital implant impressions: Effects of different scanners and implant level. Int. J. Oral Maxillofac. Implants 2017, 32, 70–80. [Google Scholar] [CrossRef]
- Basaki, K.; Alkumru, H.; De Souza, G.; Finer, Y. Accuracy of digital vs. conventional implant impression approach: A three-dimensional comparative in vitro analysis. Int. J. Oral Maxillofac. Implants 2017, 32, 792–799. [Google Scholar] [CrossRef] [Green Version]
- Lin, W.-S.; Harris, B.T.; Elathamna, E.N.; Abdel-Azim, T.; Morton, D. Effect of implant divergence on the accuracy of definitive casts created from traditional and digital implant-level impressions: An in vitro comparative study. Int. J. Oral Maxillofac. Implants 2015, 30, 102–109. [Google Scholar] [CrossRef] [Green Version]
- Giménez, B.; Özcan, M.; Martínez-Rus, F.; Pradíes, G. Accuracy of a digital impression system based on active triangulation technology with blue light for implants: Effect of clinically relevant parameters. Implant. Dent. 2015, 24, 498–504. [Google Scholar] [CrossRef]
- Vandeweghe, S.; Vervack, V.; Dierens, M.; De Bruyn, H. Accuracy of digital impressions of multiple dental implants: An in vitro study. Clin. Oral Implants Res. 2016, 28, 648–653. [Google Scholar] [CrossRef]
- Giménez, B.; Özcan, M.; Martínez-Rus, F.; Pradíes, G. Accuracy of a digital impression system based on active wavefront sampling technology for implants considering operator experience, implant angulation, and depth. Clin. Implant. Dent. Relat. Res. 2015, 17 (Suppl. 1), e54–e64. [Google Scholar] [CrossRef]
- Papaspyridakos, P.; Gallucci, G.O.; Chen, C.J.; Hanssen, S.; Naert, I.; Vandenberghe, B. Digital versus conventional implant impressions for edentulous patients: Accuracy outcomes. Clin. Oral Implants Res. 2016, 27, 465–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amin, S.; Weber, H.P.; Finkelman, M.; Rafie, K.; Kudara, Y.; Papaspyridakos, P. Digital vs. conventional full-arch implant impressions: A comparative study. Clin. Oral Implants Res. 2017, 28, 1360–1367. [Google Scholar] [CrossRef] [PubMed]
- Alikhasi, M.; Siadat, H.; Nasirpour, A.; Hasanzade, M. Three-dimensional accuracy of digital impression versus conventional method: Effect of implant angulation and connection type. Int. J. Dent. 2018, 2018, 3761750. [Google Scholar] [CrossRef] [PubMed]
- Patzelt, S.B.M.; Vonau, S.; Stampf, S.; Att, W. Assessing the feasibility and accuracy of digitizing edentulous jaws. J. Am. Dent. Assoc. 2013, 144, 914–920. [Google Scholar] [CrossRef] [PubMed]
- Malik, J.; Rodriguez, J.; Weisbloom, M.; Petridis, H. Comparison of accuracy between a conventional and two digital intraoral impression techniques. Int. J. Prosthodont. 2018, 31, 107–113. [Google Scholar] [CrossRef]
- Mangano, F.G.; Admakin, O.; Bonacina, M.; Lerner, H.; Rutkunas, V.; Mangano, C. Trueness of 12 intraoral scanners in the full-arch implant impression: A comparative in vitro study. BMC Oral Health 2020, 20, 263. [Google Scholar] [CrossRef]
- Di Fiore, A.; Meneghello, R.; Graiff, L.; Savio, G.; Vigolo, P.; Monaco, C.; Stellini, E. Full arch digital scanning systems performances for implant-supported fixed dental prostheses: A comparative study of 8 intraoral scanners. J. Prosthodont. Res. 2019, 63, 396–403. [Google Scholar] [CrossRef]
- Miyoshi, K.; Tanaka, S.; Yokoyama, S.; Sanda, M.; Baba, K. Effects of different types of intraoral scanners and scanning ranges on the precision of digital implant impressions in edentulous maxilla: An in vitro study. Clin. Oral Implants Res. 2019, 31, 74–83. [Google Scholar] [CrossRef]
- Kim, K.R.; Seo, K.Y.; Kim, S. Conventional open-tray impression versus intraoral digital scan for implant-level complete-arch impression. J. Prosthet. Dent. 2019, 122, 543–549. [Google Scholar] [CrossRef]
- Huang, R.; Liu, Y.; Huang, B.; Zhang, C.; Chen, Z.; Li, Z. Improved scanning accuracy with newly designed scan bodies: An in vitro study comparing digital versus conventional impression techniques for complete-arch implant rehabilitation. Clin. Oral Implants Res. 2020, 31, 625–633. [Google Scholar] [CrossRef]
- Alsharbaty, M.M.M.; Alikhasi, M.; Zarrati, S.; Shamshiri, A.R. A clinical comparative study of 3-dimensional accuracy between digital and conventional implant impression techniques. J. Prothodont. 2019, 28, e902–e908. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| System | Manufacturer | Scanning Technology | Scan Protocol | Acquisition | Powder Application | Export |
|---|---|---|---|---|---|---|
| iTero- Element Plus Series | Align Technology | Parallel confocal microscopy | OPB | Video Sequence | No | STL/OBJ/PLY |
| i500 | Medit | Triangulation technique | OPB | Video Sequence | No | STL/OBJ/PLY |
| Planscan | Planmecca | Confocal microscopy and optical coherence tomography | OPB | Video Sequence | No | STL/OBJ/PLY |
| Two-Way Analysis of Variance | ||||||
|---|---|---|---|---|---|---|
| Model A | Model B | Model C | Scanner | Model | Interaction | |
| iTero® | 0.0244 (0.0017) | 0.0244 (0.0047) | 0.0249 (0.0012) | F(2,126) = 675.53 p < 0.001 η2 = 0.92 | F(2,126) = 58.13 p < 0.001 η2 = 0.48 | F(4,126) = 17.77 p < 0.001 η2 = 0.36 |
| Medit® | 0.0379 (0.0028) | 0.0329 (0.0041) | 0.0264 (0.0030) | |||
| Planmeca® | 0.0507 (0.0028) | 0.0469 (0.0017) | 0.0421 (0.0019) | |||
| t-Test, H0: μ = 0 | |||
|---|---|---|---|
| Model A | Model B | Model C | |
| iTero® | t(14) = 56.92 (p < 0.001) d = 14.70 | t(14) = 20.22 (p < 0.001) d = 5.22 | t(14) = 80.19 (p < 0.001) d = 20.71 |
| Medit® | t(14) = 52.91 (p < 0.001) d = 13.66 | t(14) = 30.89 (p < 0.001) d = 7.98 | t(14) = 34.34 (p < 0.001) d = 8.87 |
| Planmeca® | t(14) = 69.32 (p < 0.001) d = 17.90 | t(14) = 108.10 (p < 0.001) d = 27.91 | t(14) = 84.03 (p < 0.001) d = 21.70 |
| Two-Way Analysis of Variance | ||||||
|---|---|---|---|---|---|---|
| Model A | Model B | Model C | Scanner | Model | Interaction | |
| iTero® | 0.0260 (0.0039) | 0.0250 (0.0025) | 0.0192 (0.0042) | F(2,117) = 593.52 p < 0.001 η2 = 0.91 | F(2,117) = 218.95 p < 0.001 η2 = 0.79 | F(4,117) = 24.01 p < 0.001 η2 = 0.45 |
| Medit® | 0.0359 (0.0052) | 0.0268 (0.0052) | 0.0180 (0.0020) | |||
| Planmeca® | 0.0573 (0.0034) | 0.0530 (0.0018) | 0.0343 (0.0027) | |||
| t-Test, H0: μ = 0 | |||
|---|---|---|---|
| Model A | Model B | Model C | |
| iTero® | t(13) = 24.76 (p < 0.001) d = 6.62 | t(13) = 36.84 (p < 0.001) d = 9.85 | t(13) = 17.28 (p < 0.001) d = 4.62 |
| Medit® | t(13) = 25.86 (p < 0.001) d = 6.91 | t(13) = 21.11 (p < 0.001) d = 5.64 | t(13) = 32.90 (p < 0.001) d = 8.79 |
| Planmeca® | t(13) = 63.08 (p < 0.001) d = 16.86 | t(13) = 110.81 (p < 0.001) d = 29.62 | t(13) = 48.52 (p < 0.001) d = 12.97 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costa, V.; Silva, A.S.; Costa, R.; Barreiros, P.; Mendes, J.; Mendes, J.M. In Vitro Comparison of Three Intraoral Scanners for Implant—Supported Dental Prostheses. Dent. J. 2022, 10, 112. https://doi.org/10.3390/dj10060112
Costa V, Silva AS, Costa R, Barreiros P, Mendes J, Mendes JM. In Vitro Comparison of Three Intraoral Scanners for Implant—Supported Dental Prostheses. Dentistry Journal. 2022; 10(6):112. https://doi.org/10.3390/dj10060112
Chicago/Turabian StyleCosta, Vitória, António Sérgio Silva, Rosana Costa, Pedro Barreiros, Joana Mendes, and José Manuel Mendes. 2022. "In Vitro Comparison of Three Intraoral Scanners for Implant—Supported Dental Prostheses" Dentistry Journal 10, no. 6: 112. https://doi.org/10.3390/dj10060112
APA StyleCosta, V., Silva, A. S., Costa, R., Barreiros, P., Mendes, J., & Mendes, J. M. (2022). In Vitro Comparison of Three Intraoral Scanners for Implant—Supported Dental Prostheses. Dentistry Journal, 10(6), 112. https://doi.org/10.3390/dj10060112