
Influence on Implant Bone Healing of a Collagen Membrane Placed Subjacent the Sinus Mucosa—A Randomized Clinical Trial on Sinus Floor Elevation





Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Statement
2.2. Study Population
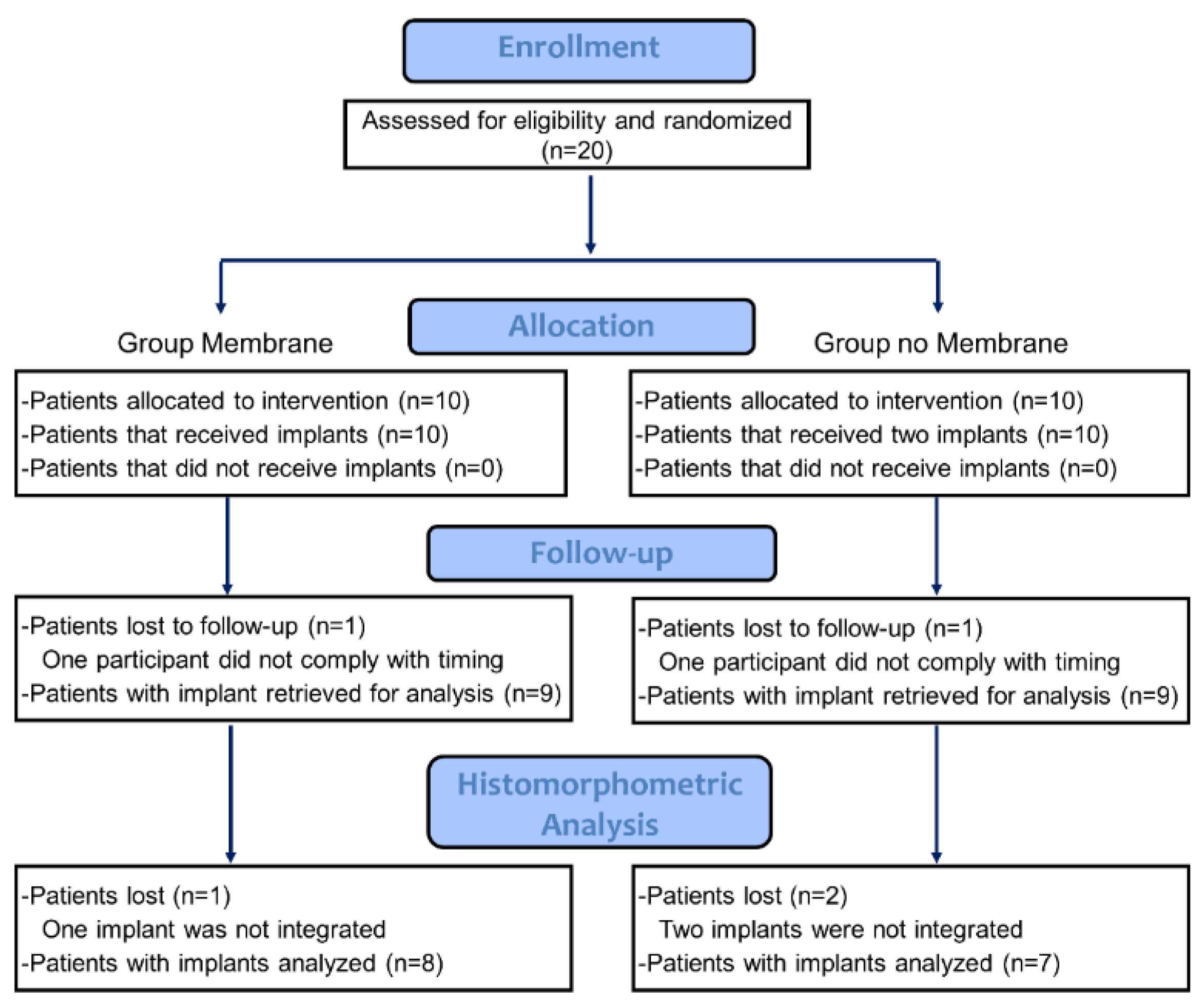
2.3. Study Design
2.4. Devices and Biomaterials
2.5. Sample Size
2.6. Randomization and Allocation Concealment
2.7. Clinical Procedures
2.8. Histological Preparation of the Biopsies
2.9. Histomorphometric Evaluation
2.10. Data Analysis
3. Results
3.1. Clinical Outcomes
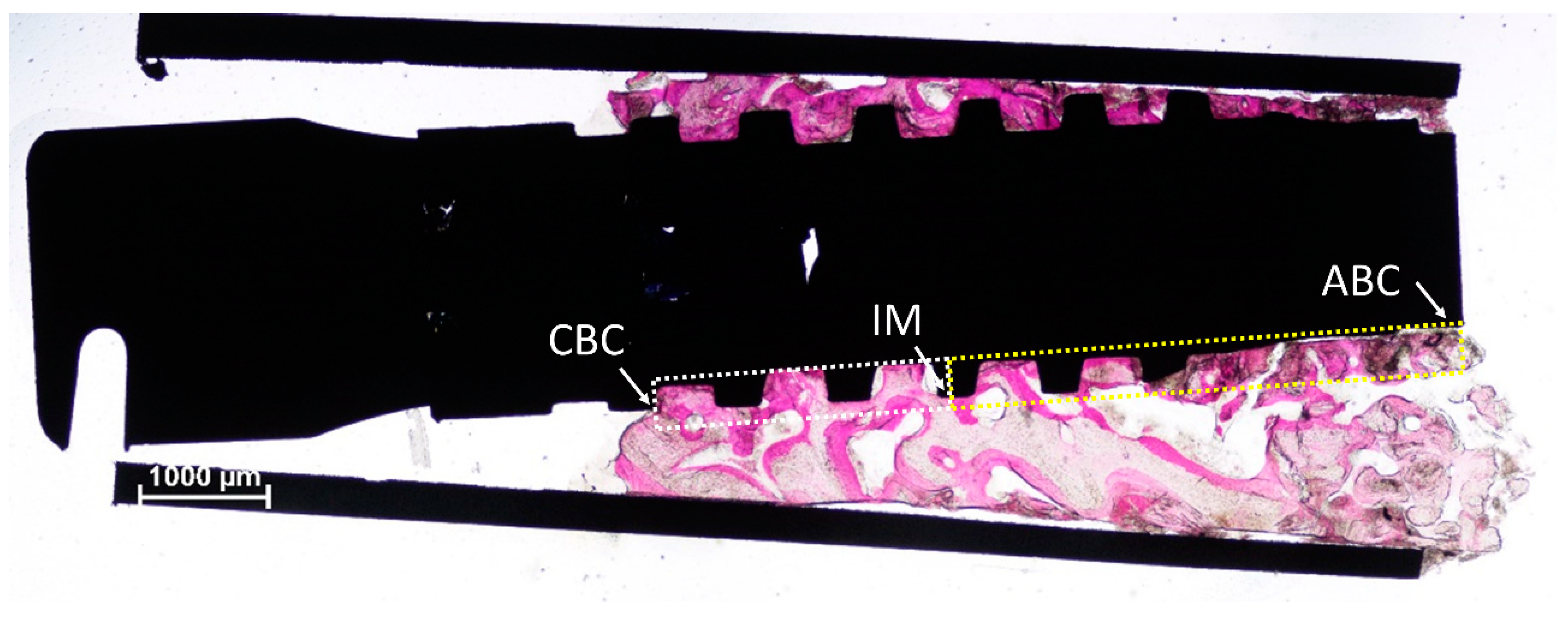
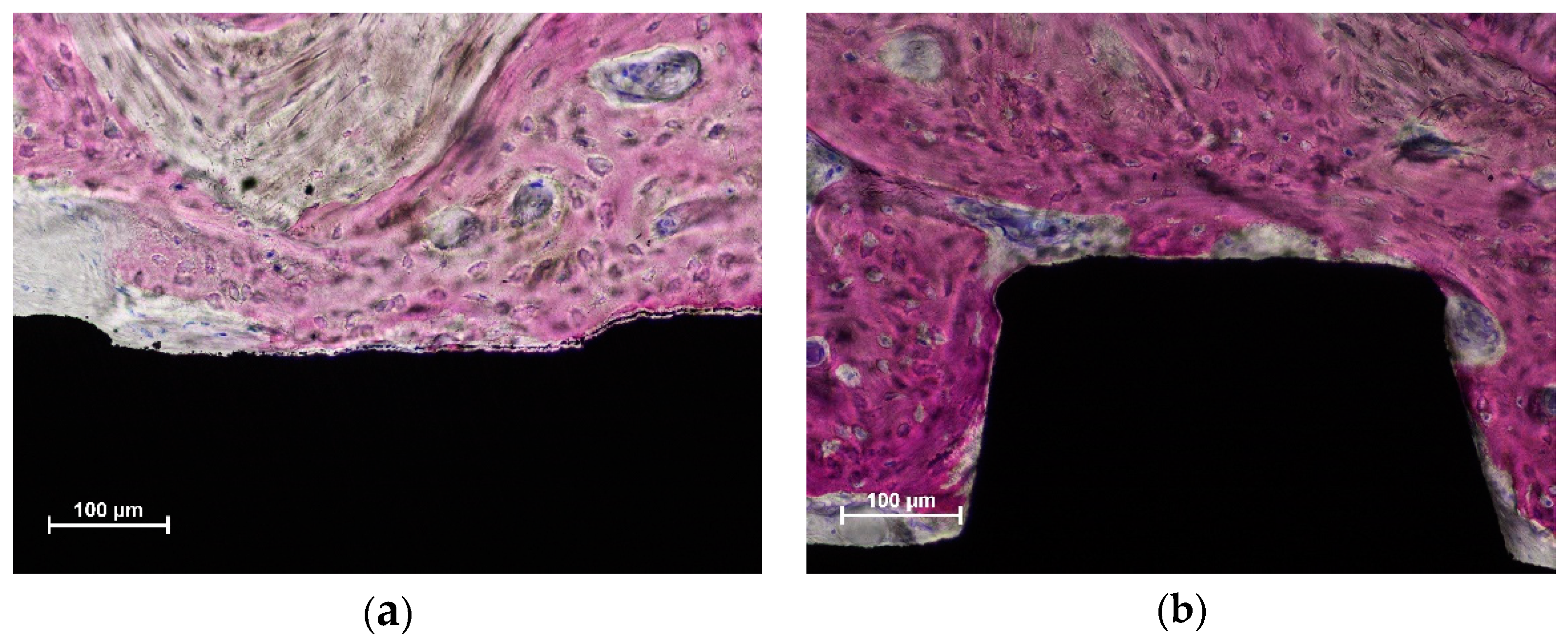
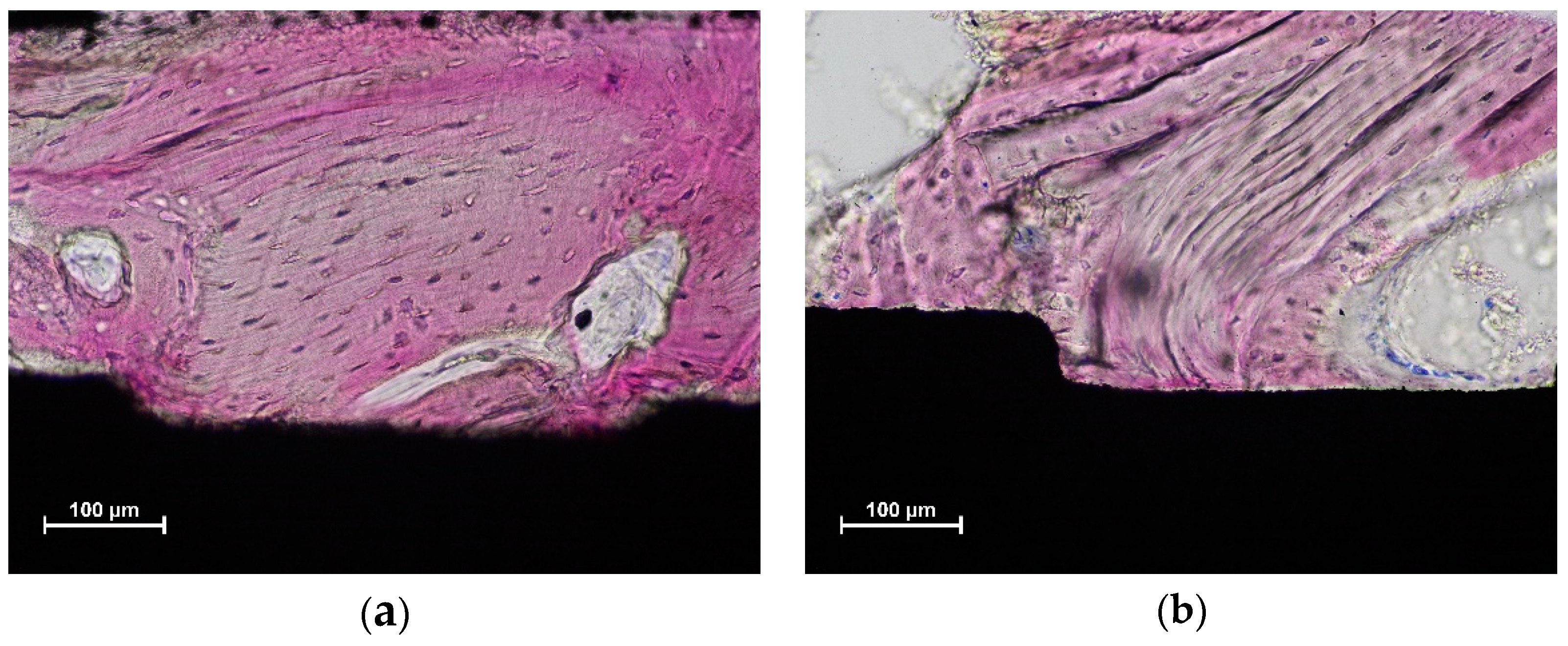
3.2. Histomorphometric Description
3.3. Histometric Evaluations—Tissues in Contact with the Implant Surface
3.4. Morphometric Evaluations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pjetursson, B.E.; Tan, W.C.; Zwahlen, M.; Lang, N.P. A systematic review of the success of sinus floor elevation and survival of implants inserted in combination with sinus floor elevation. J. Clin. Periodontol. 2008, 35 (Suppl. 8), 216–240. [Google Scholar] [CrossRef] [PubMed]
- Starch-Jensen, T.; Aludden, H.; Hallman, M.; Dahlin, C.; Christensen, A.E.; Mordenfeld, A. A systematic review and meta-analysis of long-term studies (five or more years) assessing maxillary sinus floor augmentation. Int. J. Oral Maxillofac. Surg. 2018, 47, 103–116. [Google Scholar] [CrossRef] [PubMed]
- Hirota, A.; Lang, N.P.; Ferri, M.; Mesa, N.F.; Alccayhuaman, K.A.A.; Botticelli, D. Tomographic evaluation of the influence of the placement of a collagen membrane subjacent to the sinus mucosa during maxillary sinus floor augmentation: A randomized clinical trial. Int. J. Implant Dent. 2019, 5, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Schwartz-Arad, D.; Herzberg, R.; Dolev, E. The prevalence of surgical complications of the sinus graft procedure and their impact on implant survival. J. Periodontol. 2004, 75, 511–516. [Google Scholar] [CrossRef]
- Nolan, P.J.; Freeman, K.; Kraut, R.A. Correlation between Schneiderian membrane perforation and sinus lift graft outcome: A retrospective evaluation of 359 augmented sinus. J. Oral Maxillofac. Surg. 2014, 72, 47–52. [Google Scholar] [CrossRef]
- Kawakami, S.; Lang, N.P.; Iida, T.; Ferri, M.; Apaza Alccayhuaman, K.A.; Botticelli, D. Influence of the position of the antrostomy in sinus floor elevation assessed with cone-beam computed tomography: A randomized clinical trial. J. Investig. Clin. Dent. 2018, 9, e12362. [Google Scholar] [CrossRef]
- Kawakami, S.; Lang, N.P.; Ferri, M.; Apaza Alccayhuaman, K.A.; Botticelli, D. Influence of the height of the antrostomy in sinus floor elevation assessed by cone beam computed tomography—a randomized clinical trial. Int. J. Oral Maxillofac. Implant. 2019, 34, 223–232. [Google Scholar] [CrossRef]
- Aimetti, M.; Massei, G.; Morra, M.; Cardesi, E.; Romano, F. Correlation between gingival phenotype and Schneiderian membrane thickness. Int. J. Oral Maxillofac. Implant. 2008, 23, 1128–1132. [Google Scholar]
- Khoury, F. Augmentation of the sinus floor with mandibular bone block and simultaneous implantation: A 6-year clinical investigation. Int. J. Oral Maxillofac. Implant. 1999, 14, 557–564. [Google Scholar]
- Lundgren, S.; Andersson, S.; Gualini, F.; Sennerby, L. Bone reformation with sinus membrane elevation: A new surgical technique for maxillary sinus floor augmentation. Clin. Implant Dent. Relat. Res. 2004, 6, 165–173. [Google Scholar] [CrossRef]
- Choi, K.S.; Kan, J.Y.; Boyne, P.J.; Goodacre, C.J.; Lozada, J.L.; Rungcharassaeng, K. The effects of resorbable membrane on human maxillary sinus graft: A pilot study. Int. J. Oral Maxillofac. Implant. 2009, 24, 73–80. [Google Scholar]
- Kim, J.; Jang, H. A review of complications of maxillary sinus augmentation and available treatment methods. J. Korean Assoc. Oral Maxillofac. Surg. 2019, 45, 220–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gruber, R.; Kandler, B.; Fuerst, G.; Fischer, M.B.; Watzek, G. Porcine sinus mucosa holds cells that respond to bone morphogenetic protein (BMP)-6 and BMP-7 with increased osteogenic differentiation in vitro. Clin. Oral Implant. Res. 2004, 15, 575–580. [Google Scholar] [CrossRef] [PubMed]
- Srouji, S.; Ben-David, D.; Lotan, R.; Riminucci, M.; Livne, E.; Bianco, P. The innate osteogenic potential of the maxillary sinus (Schneiderian) membrane: An ectopic tissue transplant model simulating sinus lifting. Int. J. Oral Maxillofac. Surg. 2010, 39, 793–801. [Google Scholar] [CrossRef] [PubMed]
- Scala, A.; Lang, N.P.; Velez, J.U.; Favero, R.; Bengazi, F.; Botticelli, D. Effects of a collagen membrane positioned between augmentation material and the sinus mucosa in the elevation of the maxillary sinus floor. An experimental study in sheep. Clin. Oral Implant. Res. 2016, 27, 1454–1461. [Google Scholar] [CrossRef] [PubMed]
- Favero, V.; Lang, N.P.; Canullo, L.; Urbizo Velez, J.; Bengazi, F.; Botticelli, D. Sinus floor elevation outcomes following perforation of the Schneiderian membrane. An experimental study in sheep. Clin. Oral Implant. Res. 2015, 27, 233–240. [Google Scholar] [CrossRef]
- Iida, T.; Carneiro Martins Neto, E.; Botticelli, D.; Apaza Alccayhuaman, K.A.; Lang, N.P.; Xavier, S.P. Influence of a collagen membrane positioned subjacent the sinus mucosa following the elevation of the maxillary sinus. A histomorphometric study in rabbits. Clin. Oral Implant. Res. 2017, 28, 1567–1576. [Google Scholar] [CrossRef]
- Scala, A.; Botticelli, D.; Faeda, R.S.; Garcia Rangel, I., Jr.; Américo de Oliveira, J.; Lang, N.P. Lack of influence of the Schneiderian membrane in forming new bone apical to implants simultaneously installed with sinus floor elevation: An experimental study in monkeys. Clin. Oral Implant. Res. 2013, 23, 175–181. [Google Scholar] [CrossRef]
- Hirota, A.; Iezzi, G.; Piattelli, A.; Ferri, M.; Tanaka, K.; Apaza Alccayhuaman, K.A.; Botticelli, D. Influence of the position of the antrostomy in sinus floor elevation on the healing of mini-implants: A randomized clinical trial. Oral Maxillofac. Surg. 2020, 24, 299–308. [Google Scholar] [CrossRef]
- Imai, H.; Iezzi, G.; Piattelli, A.; Ferri, M.; Apaza Alccayhuaman, K.A.; Botticelli, D. Influence of the Dimensions of the Antrostomy on Osseointegration of Mini-implants Placed in the Grafted Region After Sinus Floor Elevation: A Randomized Clinical Trial. Int. J. Oral Maxillofac. Implant. 2020, 35, 591–598. [Google Scholar] [CrossRef]
- Ferri, M.; Lang, N.P.; Alfonso, E.E.A.; Quintero, I.D.B.; Burgos, E.M.; Botticelli, D. Use of sonic instruments for implant biopsy retrieval. Clin. Oral Implant. Res. 2014, 26, 1237–1243. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, H.E.; Münzel-Pedrazzoli, S. Correlated morphometric and biochemical analysis of gingival tissue. Morphometric model, tissue sampling and test of stereologic procedures. J. Microsc. 1973, 99, 301–329. [Google Scholar] [CrossRef] [PubMed]
- Temmerman, A.; Van Dessel, J.; Cortellini, S.; Jacobs, R.; Teughels, W.; Quirynen, M. Volumetric changes of grafted volumes and the Schneiderian membrane after transcrestal and lateral sinus floor elevation procedures: A clinical, pilot study. J. Clin. Periodontol. 2017, 44, 660–671. [Google Scholar] [CrossRef] [PubMed]
- Nosaka, Y.; Nosaka, H.; Arai, Y. Complications of postoperative swelling of the maxillary sinus membrane after sinus floor augmentation. J. Oral Sci. Rehabil. 2015, 1, 26–33. [Google Scholar]
- Imai, H.; Lang, N.; Ferri, M.; Hirota, A.; Alccayhuaman, K. Tomographic Assessment on the Influence of the Use of a Collagen Membrane on Dimensional Variations to Protect the Antrostomy After Maxillary Sinus Floor Augmentation: A Randomized Clinical Trial. Int. J. Oral Maxillofac. Implant. 2020, 35, 350–356. [Google Scholar] [CrossRef]
- Makary, C.; Rebaudi, A.; Menhall, A.; Naaman, N. Changes in Sinus Membrane Thickness After Lateral Sinus Floor Elevation: A Radiographic Study. Int. J. Oral Maxillofac. Implant. 2016, 31, 331–337. [Google Scholar] [CrossRef] [Green Version]
- Scala, A.; Botticelli, D.; Rangel Garcia, I., Jr.; de Oliveira, J.A.; Okamoto, R.; Lang, N.P. Early healing after elevation of the maxillary sinus floor applying a lateral access: A histological study in monkeys. Clin. Oral Implant. Res. 2010, 21, 1320–1326. [Google Scholar] [CrossRef]
- Asai, S.; Shimizu, Y.; Ooya, K. Maxillary sinus augmentation model in rabbits: Effect of occluded nasal ostium on new bone formation. Clin. Oral Implant. Res. 2002, 13, 405–409. [Google Scholar] [CrossRef]
- Xu, H.; Shimizu, Y.; Asai, S.; Ooya, K. Grafting of deproteinized bone particles inhibits bone resorption after maxillary sinus floor elevation. Clin. Oral Implant. Res. 2004, 15, 126–133. [Google Scholar] [CrossRef]
- Xu, H.; Shimizu, Y.; Ooya, K. Histomorphometric study of the stability of newly formed bone after elevation of the floor of the maxillary sinus. Br. J. Oral Maxillofac. Surg. 2005, 43, 493–499. [Google Scholar] [CrossRef]
- Caneva, M.; Lang, N.P.; Garcia Rangel, I.J.; Ferreira, S.; Caneva, M.; De Santis, E.; Botticelli, D. Sinus mucosa elevation using Bio-Oss(®) or Gingistat(®) collagen sponge: An experimental study in rabbits. Clin. Oral Implant. Res. 2017, 28, e21–e30. [Google Scholar] [CrossRef] [PubMed]
- De Santis, E.; Lang, N.P.; Ferreira, S.; Rangel Garcia, I., Jr.; Caneva, M.; Botticelli, D. Healing at implants installed concurrently to maxillary sinus floor elevation with Bio-Oss(®) or autologous bone grafts. A histo-morphometric study in rabbits. Clin. Oral Implant. Res. 2017, 28, 503–511. [Google Scholar] [CrossRef] [PubMed]
- Godoy, E.P.; Alccayhuaman, K.A.A.; Botticelli, D.; Amaroli, A.; Balan, V.F.; Silva, E.R.; Xavier, S.P. Osteoconductivity of Bovine Xenograft Granules of Different Sizes in Sinus Lift: A Histomorphometric Study in Rabbits. Dent. J. 2021, 9, 61. [Google Scholar] [CrossRef]
- Miki, M.; Botticelli, D.; Silva, E.R.; Xavier, S.P.; Baba, S. Incidence of Sinus Mucosa Perforations During Healing After Sinus Elevation Using Deproteinized Bovine Bone Mineral as Grafting Material: A Histologic Evaluation in a Rabbit Model. Int. J. Oral Maxillofac. Implant. 2021, 36, 660–668. [Google Scholar] [CrossRef] [PubMed]
- Favero, R.; Apaza Alccayhuaman, K.A.; Botticelli, D.; Xavier, S.P.; Ferreira Balan, V.; Macchi, V.; De Caro, R. Sinus Mucosa Thinning and Perforations after Sinus Lifting Performed with Different Xenografts: A Histological Analysis in Rabbits. Dent. J. 2021, 10, 2. [Google Scholar] [CrossRef] [PubMed]
- Kato, S.; Botticelli, D.; De Santis, E.; Kanayama, M.; Ferreira, S.; Rangel-Garcia, I., Jr. Sinus mucosa thinning and perforation after sinus augmentation. A histological study in rabbits. Oral Maxillofac. Surg. 2021, 25, 477–485. [Google Scholar] [CrossRef]
- Omori, Y.; Botticelli, D.; Ferri, M.; Delgado-Ruiz, R.; Ferreira Balan, V.; Porfirio Xavier, S. Argon Bioactivation of Implants Installed Simultaneously to Maxillary Sinus Lifting without Graft. An Experimental Study in Rabbits. Dent. J. 2021, 9, 105. [Google Scholar] [CrossRef]
- Kotsu, M.; Apaza Alccayhuaman, K.A.; Ferri, M.; Iezzi, G.; Piattelli, A.; Fortich Mesa, N.; Botticelli, D. Osseointegration at implants installed in composite bone. A randomized clinical trial on sinus floor elevation. J. Funct. Biomater. 2022, 13, 22. [Google Scholar] [CrossRef]
- Melcher, A.H. On the repair potential of periodontal tissues. J. Periodontol. 1976, 47, 256–260. [Google Scholar] [CrossRef]
- Botticelli, D.; Berglundh, T.; Persson, L.G.; Lindhe, J. Bone regeneration at implants with turned or rough surfaces in self-contained defects. An experimental study in the dog. J. Clin. Periodontol. 2005, 32, 448–455. [Google Scholar] [CrossRef]
- Díaz-Olivares, L.A.; Cortés-Bretón Brinkmann, J.; Martínez-Rodríguez, N.; Martínez-González, J.M.; López-Quiles, J.; Leco-Berrocal, I.; Meniz-García, C. Management of Schneiderian membrane perforations during maxillary sinus floor augmentation with lateral approach in relation to subsequent implant survival rates: A systematic review and meta-analysis. Int. J. Implant Dent. 2021, 7, 91. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gender | Age | Smokers | |
|---|---|---|---|
| Mb | 6 females; 4 males | 56.0 ± 7.5 | None |
| Non-Mb | 7 females; 3 males | 54.7 ± 11.8 | None |
| Whole Surface | New Bone | Old Bone | Tot Bone | Debris | Graft | Soft Tissues | |
| Mb | Mean ± SD Median (25%; 75%) | 51.3 ± 14.0 53.0 (44.7; 56.9) | 3.8 ± 3.4 3.2 (2.3; 4.6) | 55.1 ± 16.6 58.3 (45.6; 60.2) | 1.8 ± 2.8 0.0 (0.0; 3.1) | 3.6 ± 2.5 4.0 (1.6; 5.2) | 39.5 ± 15.7 36.7 (33.6; 43.5) |
| Non-Mb | Mean ± SD Median (25%; 75%) | 52.5 ± 16.8 50.8 (41.2; 66.0) | 3.9 ± 4.8 2.2 (0.0; 6.5) | 56.5 ± 16.1 53.0 (50.2; 69.7) | 0.3 ± 0.9 0.0 (0.0; 0.0) | 4.8 ± 5.0 4.4 (0.0; 8.5) | 38.4 ± 17.2 34.8 (25.0; 48.6) |
| Apical Region | New Bone | Old Bone | Tot Bone | Debris | Graft | Soft Tissues | |
| Mb | Mean ± SD Median (25%; 75%) | 44.3 ± 21.2 36.4 (31.6; 56.1) | 1.5 ± 2.8 0.0 (0.0; 1.0) | 45.8 ± 23.7 36.4 (31.6; 57.1) | 1.1 ± 2.2 0.0 (0.0; 0.9) | 7.2 ± 5.5 7.4 (2.7; 10.9) | 45.8 ± 22.0 49.1 (32.6; 58.3) |
| Non-Mb | Mean ± SD Median (25%; 75%) | 44.9 ± 16.5 # 40.6 (37.2; 57.1) | 0.0 ± 0.0 0.0 (0.0; 0.0) | 44.9 ± 16.5 # 40.6 (37.2; 57.1) | 0.3 ± 0.8 0.0 (0.0; 0.0) | 8.7 ± 8.7 12.1 (0.0; 13.6) | 46.1 ± 18.8 # 44.8 (32.2; 61.8) |
| Coronal Region | New Bone | Old Bone | Tot Bone | Debris | Graft | Soft Tissues | |
| Mb | Mean ± SD Median (25%; 75%) | 60.2 ± 10.3 60.6 (55.9; 64.1) | 6.0 ± 5.2 6.2 (1.9; 8.1) | 66.3 ± 12.7 63.3 (57.3; 78.0) | 2.2 ± 3.8 0.0 (0.0; 3.6) | 0.4 ± 1.3 0.0 (0.0; 0.0) | 31.0 ± 10.9 31.4 (22.0; 39.8) |
| Non-Mb | Mean ± SD Median (25%; 75%) | 58.4 ± 18.4 # 61.9 (43.3; 73.4) | 6.0 ± 6.8 3.6 (0.0; 10.9) | 64.4 ± 17.0 # 65.5 (56.2; 78.9) | 0.4 ± 1.0 0.0 (0.0; 0.0) | 0.0 ± 0.0 0.0 (0.0; 0.0) | 35.2 ± 16.9 # 34.5 (21.1; 42.6) |
| New Bone | Old Bone | Tot Bone | Debris | Graft | Soft Tissues | ||
| Mb | Mean ± SD Median (25%; 75%) | 33.2 ± 10.5 32.1 (25.9; 38.9) | 19.8 ± 9.0 19.6 (17.0; 26.6) | 53.1 ± 13.4 49.9 (44.1; 58.4) | 1.8 ± 3.5 0.0 (0.0; 1.4) | 12.7 ± 5.1 * 12.1 (9.5; 16.9) | 32.4 ± 13.8 36.2 (24.6; 44.5) |
| Non-Mb | Mean ± SD Median (25%; 75%) | 33.1 ± 9.6 35.4 (29.5; 39.9) | 14.2 ± 13.3 10.3 (4.0; 23.4) | 47.3 ± 6.2 49.4 (42.3; 52.1) | 3.8 ± 6.6 0.0 (0.0; 4.8) | 5.5 ± 3.0 * 5.0 (3.6; 6.2) | 43.4 ± 11.9 39.3 (37.7; 54.3) |
| Apical Region | New Bone | Old Bone | Tot Bone | Debris | Graft | Soft Tissues | |
| Mb | Mean ± SD Median (25%; 75%) | 33.6 ± 9.8 28.0 (26.0; 43.4) | 5.5 ± 7.6 # 0.0 (0.0; 13.3) | 39.1 ± 15.0 # 33.9 (26.2; 49.1) | 0.7 ± 1.4 0.0 (0.0; 0.5) | 23.2 ± 6.7 * # 22.2 (19.0; 29.1) | 37.0 ± 16.2 40.0 (32.6; 44.1) |
| Non-Mb | Mean ± SD Median (25%; 75%) | 30.9 ± 11.5 34.1 (24.6; 36.7) | 0.6 ± 1.7 0.0 (0.0; 0.0) | 31.5 ± 12.0 # 34.1 (24.6; 38.9) | 2.6 ± 6.0 0.0 (0.0; 1.0) | 11.6 ± 5.6 * # 12.8 (7.9; 14.4) | 54.3 ± 12.8 52.1 (45.6; 62.5) |
| Coronal Region | New Bone | Old Bone | Tot Bone | Debris | Graft | Soft Tissues | |
| Mb | Mean ± SD Median (25%; 75%) | 33.7 ± 13.3 31.3 (26.4; 39.6) | 32.7 ± 13.1 # 34.4 (27.8; 42.3) | 66.3 ± 14.6 # 62.8 (60.5; 72.1) | 2.8 ± 6.6 0.0 (0.0; 0.9) | 2.2 ± 3.3 # 0.3 (0.0; 3.4) | 28.7 ± 13.7 32.1 (17.5; 37.4) |
| Non-Mb | Mean ± SD Median (25%; 75%) | 32.9 ± 9.8 36.2 (31.0; 37.9) | 24.0 ± 23.4 20.3 (5.4; 40.7) | 57.0 ± 20.0 # 56.5 (46.1; 62.9) | 4.1 ± 9.2 0.0 (0.0; 2.0) | 0.2 ± 0.3 # 0.0 (0.0; 0.2) | 38.8 ± 22.3 43.5 (22.7; 53.3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morimoto, A.; Kobayashi, N.; Ferri, M.; Iezzi, G.; Piattelli, A.; Fortich Mesa, N.; Botticelli, D. Influence on Implant Bone Healing of a Collagen Membrane Placed Subjacent the Sinus Mucosa—A Randomized Clinical Trial on Sinus Floor Elevation. Dent. J. 2022, 10, 105. https://doi.org/10.3390/dj10060105
Morimoto A, Kobayashi N, Ferri M, Iezzi G, Piattelli A, Fortich Mesa N, Botticelli D. Influence on Implant Bone Healing of a Collagen Membrane Placed Subjacent the Sinus Mucosa—A Randomized Clinical Trial on Sinus Floor Elevation. Dentistry Journal. 2022; 10(6):105. https://doi.org/10.3390/dj10060105
Chicago/Turabian StyleMorimoto, Akihiro, Nobuhiro Kobayashi, Mauro Ferri, Giovanna Iezzi, Adriano Piattelli, Natalia Fortich Mesa, and Daniele Botticelli. 2022. "Influence on Implant Bone Healing of a Collagen Membrane Placed Subjacent the Sinus Mucosa—A Randomized Clinical Trial on Sinus Floor Elevation" Dentistry Journal 10, no. 6: 105. https://doi.org/10.3390/dj10060105
APA StyleMorimoto, A., Kobayashi, N., Ferri, M., Iezzi, G., Piattelli, A., Fortich Mesa, N., & Botticelli, D. (2022). Influence on Implant Bone Healing of a Collagen Membrane Placed Subjacent the Sinus Mucosa—A Randomized Clinical Trial on Sinus Floor Elevation. Dentistry Journal, 10(6), 105. https://doi.org/10.3390/dj10060105