Physiology-Enhanced Data Analytics to Evaluate the Effect of Altitude on Intraocular Pressure and Ocular Hemodynamics


 , ,
, ,  ,
,  and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. The Mont Blanc Study
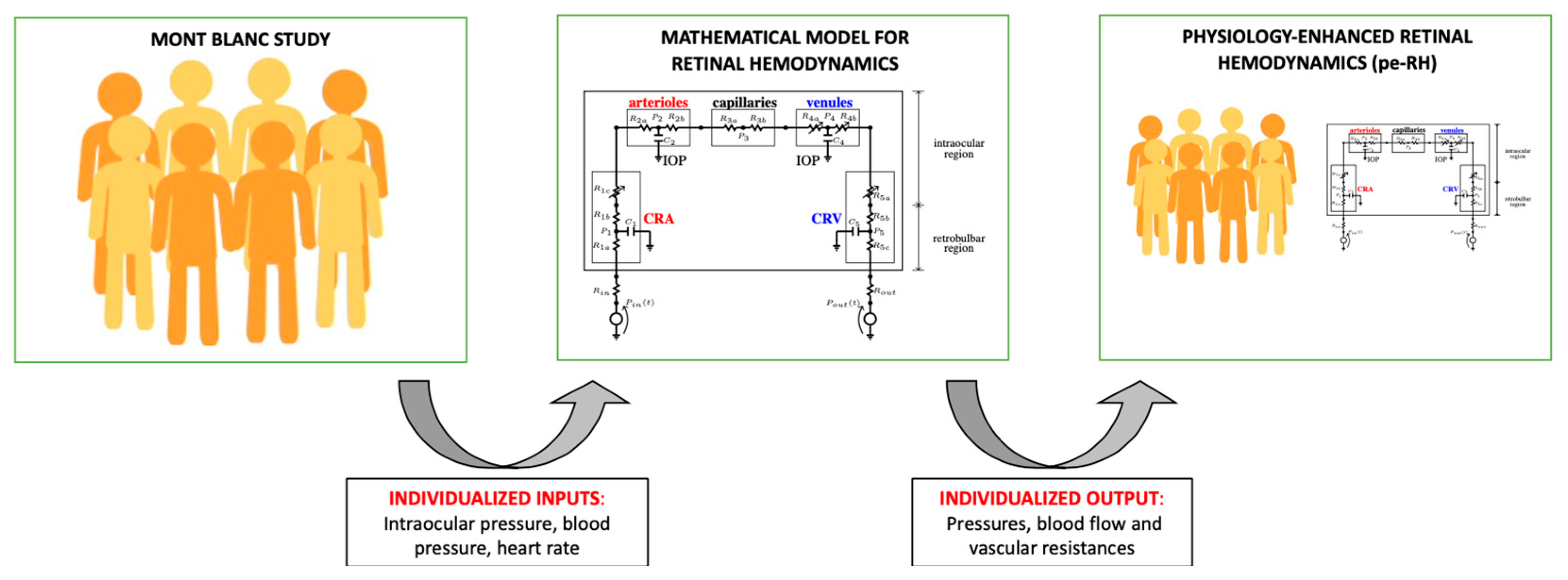
2.2. Mathematical Model of Retinal Hemodynamics
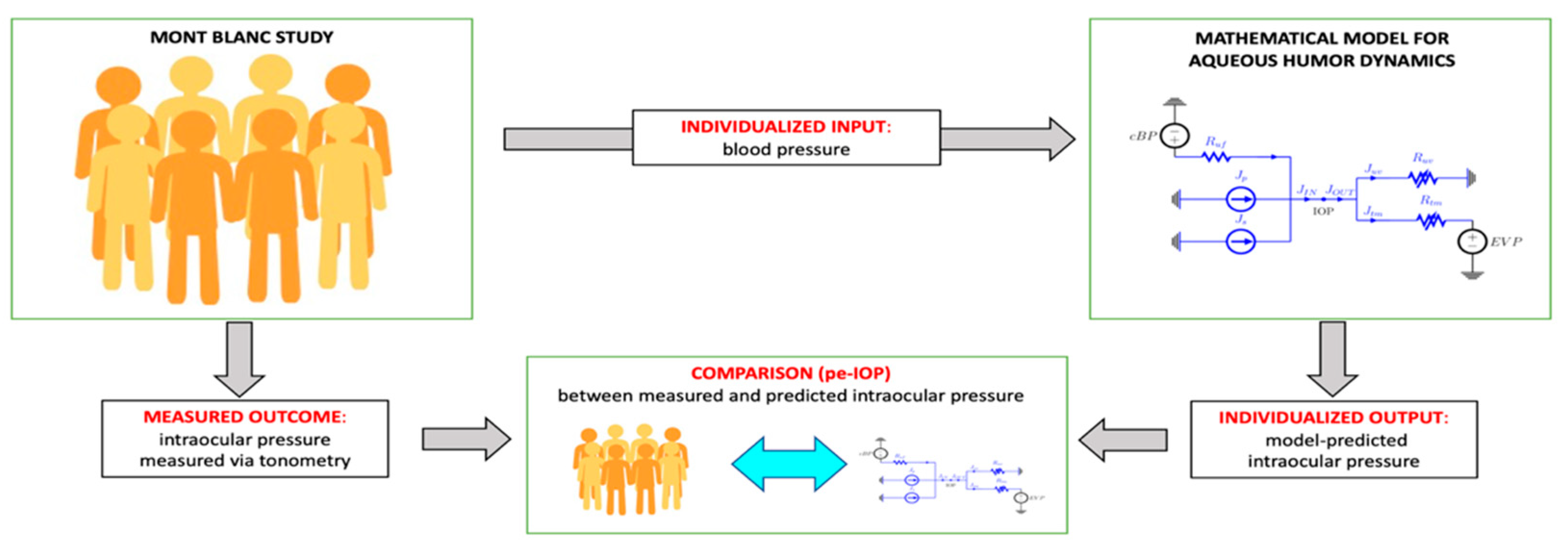
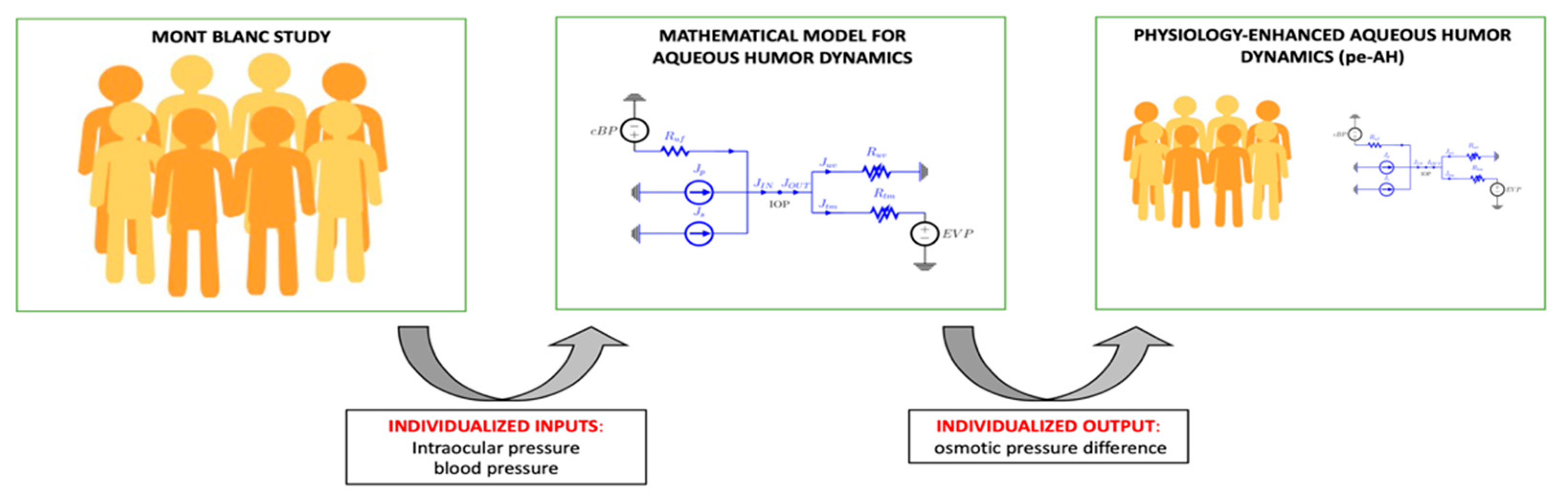
2.3. Mathematical Model of Aqueous Humor Dynamics
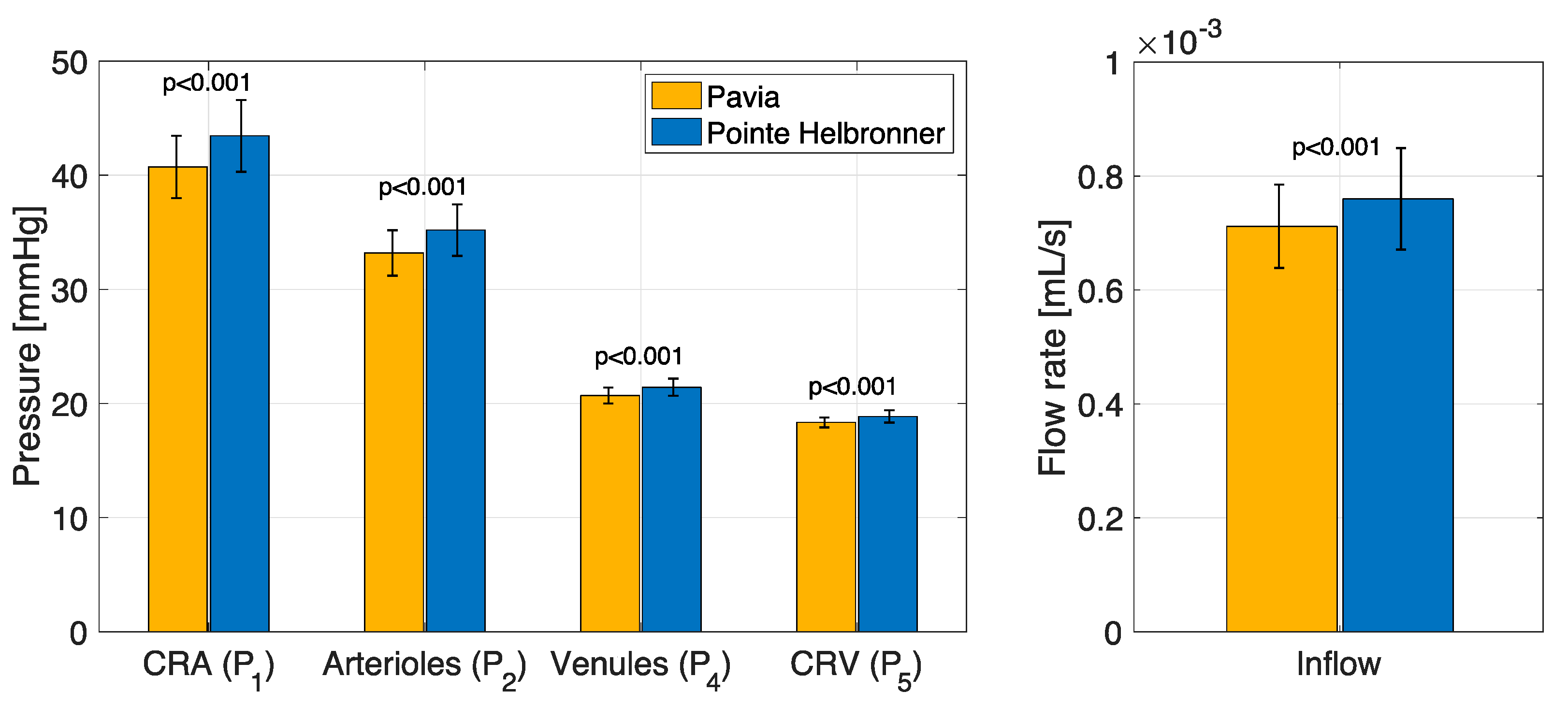
3. Results
3.1. Physiology-Enhanced Data Analytics: Retinal Hemodynamics
3.2. Physiology-Enhanced Data Analytics: Aqueous Humor Dynamics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tham, Y.C.; Li, X.; Wong, T.Y.; Quigley, H.A.; Aung, T.; Cheng, C.Y. Global prevalence of glaucoma and projections of glaucoma burden through 2040: A systematic review and meta-analysis. Ophthalmology 2014, 121, 2081–2090. [Google Scholar] [CrossRef] [PubMed]
- Kass, M.A.; Heuer, D.K.; Higginbotham, E.J.; Johnson, C.A.; Keltner, J.L.; Miller, J.P.; Parrish, R.K., 2nd; Wilson, M.R.; Gordon, M.O. The Ocular Hypertension Treatment Study: A randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma. Arch. Ophthalmol. 2002, 120, 701–713. [Google Scholar] [CrossRef] [PubMed]
- Costa, V.P.; Arcieri, E.S.; Harris, A. Blood pressure and glaucoma. Br. J. Ophthalmol. 2009, 93, 1276–1282. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Kook, M.S. Systemic and Ocular Hemodynamic Risk Factors in Glaucoma. Biomed. Res. Int. 2015, 2015, 141905. [Google Scholar] [CrossRef]
- Quaranta, L.; Katsanos, A.; Russo, A.; Riva, I. 24-hour intraocular pressure and ocular perfusion pressure in glaucoma. Surv. Ophthalmol. 2013, 58, 26–41. [Google Scholar] [CrossRef]
- Najmanova, E.; Pluhacek, F.; Botek, M.; Krejci, J.; Jarosova, J. Intraocular Pressure Response to Short-Term Extreme Normobaric Hypoxia Exposure. Front. Endocrinol. 2018, 9, 785. [Google Scholar] [CrossRef]
- Xie, Y.; Yang, Y.; Han, Y.; Yang, D.; Sun, Y.; Wang, X.; Nguyen, A.H.; Chen, Y.; Tian, J.; Zhang, Q.; et al. Association Between Arterial Blood Gas Variation and Intraocular Pressure in Healthy Subjects Exposed to Acute Short-Term Hypobaric Hypoxia. Transl. Vis. Sci. Technol. 2019, 8, 22. [Google Scholar] [CrossRef]
- Brinchmann-Hansen, O.; Myhre, K. Blood pressure, intraocular pressure, and retinal vessels after high altitude mountain exposure. Aviat. Space Environ. Med. 1989, 60, 970–976. [Google Scholar]
- Palatini, P.; Guzzardi, G.; Penzo, M.; Dorigatti, F.; Anaclerio, M.; Pessina, A.C. Effect of high and low altitude exposure on the blood pressure response to physical exercise. Cardiologia 1991, 36, 853–859. [Google Scholar]
- Bosch, M.M.; Merz, T.M.; Barthelmes, D.; Petrig, B.L.; Truffer, F.; Bloch, K.E.; Turk, A.; Maggiorini, M.; Hess, T.; Schoch, O.D.; et al. New insights into ocular blood flow at very high altitudes. J. Appl. Physiol. 2009, 106, 454–460. [Google Scholar] [CrossRef]
- Dyer, E.A.; Hopkins, S.R.; Perthen, J.E.; Buxton, R.B.; Dubowitz, D.J. Regional cerebral blood flow during acute hypoxia in individuals susceptible to acute mountain sickness. Respir. Physiol. Neurobiol. 2008, 160, 267–276. [Google Scholar] [CrossRef][Green Version]
- Karakucuk, S.; Mujdeci, M.; Baskol, G.; Arda, H.; Gumus, K.; Oner, A. Changes in central corneal thickness, intraocular pressure, and oxidation/antioxidation parameters at high altitude. Aviat. Space Environ. Med. 2012, 83, 1044–1048. [Google Scholar] [CrossRef] [PubMed]
- Somner, J.E.; Morris, D.S.; Scott, K.M.; MacCormick, I.J.; Aspinall, P.; Dhillon, B. What happens to intraocular pressure at high altitude? Investig. Ophthalmol. Vis. Sci. 2007, 48, 1622–1626. [Google Scholar] [CrossRef] [PubMed]
- Bosch, M.M.; Barthelmes, D.; Merz, T.M.; Truffer, F.; Knecht, P.B.; Petrig, B.; Bloch, K.E.; Hefti, U.; Schubiger, G.; Landau, K. Intraocular pressure during a very high altitude climb. Investig. Ophthalmol. Vis. Sci. 2010, 51, 1609–1613. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Qiong Da, C.R.; Liu, J.; Yan, X. Intraocular pressure and axial length changes during altitude acclimatization from Beijing to Lhasa. PLoS ONE 2020, 15, e0228267. [Google Scholar] [CrossRef]
- Ersanli, D.; Yildiz, S.; Sonmez, M.; Akin, A.; Sen, A.; Uzun, G. Intraocular pressure at a simulated altitude of 9000 m with and without 100% oxygen. Aviat. Space Environ. Med. 2006, 77, 704–706. [Google Scholar]
- Foulsham, W.; Tatham, A.J. High Altitude-associated Changes in Intraocular Pressure Abrogated by Trabeculectomy. J. Glaucoma 2017, 26, 957–960. [Google Scholar] [CrossRef]
- Noble, J.; Kanchanaranya, N.; Devenyi, R.G.; Lam, W.C. Evaluating the safety of air travel for patients with scleral buckles and small volumes of intraocular gas. Br. J. Ophthalmol. 2014, 98, 1226–1229. [Google Scholar] [CrossRef]
- Karadag, R.; Sen, A.; Golemez, H.; Basmak, H.; Yildirim, N.; Karadurmus, N.; Koseoglu, E.; Akin, A. The effect of short-term hypobaric hypoxic exposure on intraocular pressure. Curr. Eye Res. 2008, 33, 864–867. [Google Scholar] [CrossRef]
- Karadag, R.; Sen, A.; Yildirim, N.; Basmak, H.; Golemez, H.; Cakir, E.; Akin, A. The relation between intraocular pressure change and plasma natriuretic peptide under simulated hypobaric conditions. Indian J. Ophthalmol. 2010, 58, 195–198. [Google Scholar] [CrossRef]
- Baertschi, M.; Dayhaw-Barker, P.; Flammer, J. The effect of hypoxia on intra-ocular, mean arterial, retinal venous and ocular perfusion pressures. Clin. Hemorheol. Microcirc. 2016, 63, 293–303. [Google Scholar] [CrossRef] [PubMed]
- Amit, A.; Gaurav, K.; Vikas, A.; Ashok, K.; Harpreet, A.S.; Shivani, A. Evaluation of intraocular pressure and corneal thickness in individuals at high altitude area (10,000 ft above sea level). Rom. J. Ophthalmol. 2019, 63, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Nazari, H.; Nilforushan, N.; Sedaghat, A.; Soudi, R.; Irani, A.; Gordiz, A.; Hatamkhani, S. Intraocular pressure after exposure to moderate altitude. Graefes Arch. Clin. Exp. Ophthalmol. 2013, 251, 123–127. [Google Scholar] [CrossRef]
- Pavlidis, M.; Stupp, T.; Georgalas, I.; Georgiadou, E.; Moschos, M.; Thanos, S. Intraocular pressure changes during high-altitude acclimatization. Graefes Arch. Clin. Exp. Ophthalmol. 2006, 244, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Willmann, G.; Schommer, K.; Schultheiss, M.; Fischer, M.D.; Bartz-Schmidt, K.U.; Gekeler, F.; Schatz, A. Effect of High Altitude Exposure on Intraocular Pressure Using Goldmann Applanation Tonometry. High. Alt. Med. Biol. 2017, 18, 114–120. [Google Scholar] [CrossRef]
- Yang, Y.; Xie, Y.; Sun, Y.; Cao, K.; Li, S.; Fan, S.; Huang, L.; Wu, S.; Wang, N. Intraocular Pressure Changes of Healthy Lowlanders at Different Altitude Levels: A Systematic Review and Meta-Analysis. Front. Physiol. 2019, 10, 1366. [Google Scholar] [CrossRef]
- Xie, Y.; Sun, Y.X.; Han, Y.; Yang, D.Y.; Yang, Y.Q.; Cao, K.; Li, S.N.; Li, X.; Lu, X.X.; Wu, S.Z.; et al. Longitudinal observation of intraocular pressure variations with acute altitude changes. World J. Clin. Cases 2019, 7, 3226–3236. [Google Scholar] [CrossRef]
- Albis-Donado, O.; Rodriguez-Camacho, B.; Bhartiya, S.; Ramirez-Neria, P.; Lopez-Star, E.; Gonzalez-Daher, P.; Badillo-Fernandez, M.; Stalmans, I. Effects of Acute Atmospheric Pressure Changes on Dynamic Contour Tonometry and Goldmann Applanation Tonometry in Normal Individuals: A Pilot Study. J. Glaucoma 2020, 29, 756–760. [Google Scholar] [CrossRef]
- Cymerman, A.; Rock, P.B.; Muza, S.R.; Lyons, T.P.; Fulco, C.S.; Mazzeo, R.S.; Butterfield, G.; Moore, L.G. Intraocular pressure and acclimatization to 4300 M altitude. Aviat. Space Environ. Med. 2000, 71, 1045–1050. [Google Scholar]
- Bayer, A.; Mutlu, F.M.; Akay, F.; Bayraktar, M.Z. An assessment of intraocular pressure change in healthy subjects during air flight. Curr. Eye Res. 2008, 33, 345–349. [Google Scholar] [CrossRef]
- Bayer, A.; Yumusak, E.; Sahin, O.F.; Uysal, Y. Intraocular pressure measured at ground level and 10,000 feet. Aviat. Space Environ. Med. 2004, 75, 543–545. [Google Scholar] [PubMed]
- Bruttini, C.; Verticchio Vercellin, A.; Klersy, C.; De Silvestri, A.; Tinelli, C.; Riva, I.; Oddone, F.; Katsanos, A.; Quaranta, L. The Mont Blanc Study: The effect of altitude on intra ocular pressure and central corneal thickness. PLoS ONE 2020, 15, e0237343. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Yang, D.; Sun, Y.; Xie, Y.; Zhang, Z.; Li, S.; Wu, S.; Wang, N. Retinal vessel oxygen saturation and vessel diameter in healthy individuals during high-altitude exposure. Acta Ophthalmol. 2019, 97, 279–286. [Google Scholar] [CrossRef]
- Meehan, R.T.; Taylor, G.R.; Rock, P.; Mader, T.H.; Hunter, N.; Cymerman, A. An automated method of quantifying retinal vascular responses during exposure to novel environmental conditions. Ophthalmology 1990, 97, 875–881. [Google Scholar] [CrossRef]
- Barthelmes, D.; Bosch, M.M.; Merz, T.M.; Petrig, B.L.; Truffer, F.; Bloch, K.E.; Holmes, T.A.; Cattin, P.; Hefti, U.; Sellner, M.; et al. Delayed appearance of high altitude retinal hemorrhages. PLoS ONE 2011, 6, e11532. [Google Scholar] [CrossRef] [PubMed]
- Bhende, M.P.; Karpe, A.P.; Pal, B.P. High altitude retinopathy. Indian J. Ophthalmol. 2013, 61, 176–177. [Google Scholar] [CrossRef] [PubMed]
- Cushing, T.; Paterson, R.; Haukoos, J.; Harris, N.S. Intraocular pressure is not associated with acute mountain sickness. High. Alt. Med. Biol. 2013, 14, 342–345. [Google Scholar] [CrossRef]
- Harris, A.; Guidoboni, G.; Siesky, B.; Mathew, S.; Verticchio Vercellin, A.C.; Rowe, L.; Arciero, J. Ocular blood flow as a clinical observation: Value, limitations and data analysis. Prog. Retin. Eye Res. 2020, 100841. [Google Scholar] [CrossRef]
- Guidoboni, G.; Harris, A.; Cassani, S.; Arciero, J.; Siesky, B.; Amireskandari, A.; Tobe, L.; Egan, P.; Januleviciene, I.; Park, J. Intraocular pressure, blood pressure, and retinal blood flow autoregulation: A mathematical model to clarify their relationship and clinical relevance. Investig. Ophthalmol. Vis. Sci. 2014, 55, 4105–4118. [Google Scholar] [CrossRef]
- Szopos, M.; Cassani, S.; Guidoboni, G.; Prud’homme, C.S.; Ricardo; Siesky, B.; Harris, A. Mathematical modeling of aqueous humor flow and intraocular pressure under uncertainty: Towards individualized glaucoma management. J. Modeling Ophthalmol. 2016, 1, 29–39. [Google Scholar] [CrossRef]
- Sala, L. Mathematical Modelling and Simulation of Ocular Blood Flows and Their Interactions. Ph.D. Thesis, Université de Strasbourg, Strasbourg, France, 2019. [Google Scholar]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Verticchio Vercellin, A.; Harris, A.; Belamkar, A.; Zukerman, R.; Carichino, L.; Szopos, M.; Siesky, B.; Quaranta, L.; Bruttini, C.; Oddone, F.; et al. Physiology-Enhanced Data Analytics to Evaluate the Effect of Altitude on Intraocular Pressure and Ocular Hemodynamics. Photonics 2022, 9, 158. https://doi.org/10.3390/photonics9030158
Verticchio Vercellin A, Harris A, Belamkar A, Zukerman R, Carichino L, Szopos M, Siesky B, Quaranta L, Bruttini C, Oddone F, et al. Physiology-Enhanced Data Analytics to Evaluate the Effect of Altitude on Intraocular Pressure and Ocular Hemodynamics. Photonics. 2022; 9(3):158. https://doi.org/10.3390/photonics9030158
Chicago/Turabian StyleVerticchio Vercellin, Alice, Alon Harris, Aditya Belamkar, Ryan Zukerman, Lucia Carichino, Marcela Szopos, Brent Siesky, Luciano Quaranta, Carlo Bruttini, Francesco Oddone, and et al. 2022. "Physiology-Enhanced Data Analytics to Evaluate the Effect of Altitude on Intraocular Pressure and Ocular Hemodynamics" Photonics 9, no. 3: 158. https://doi.org/10.3390/photonics9030158
APA StyleVerticchio Vercellin, A., Harris, A., Belamkar, A., Zukerman, R., Carichino, L., Szopos, M., Siesky, B., Quaranta, L., Bruttini, C., Oddone, F., Riva, I., & Guidoboni, G. (2022). Physiology-Enhanced Data Analytics to Evaluate the Effect of Altitude on Intraocular Pressure and Ocular Hemodynamics. Photonics, 9(3), 158. https://doi.org/10.3390/photonics9030158