Intraoperative Control of Hemoglobin Oxygen Saturation in the Intestinal Wall during Anastomosis Surgery

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
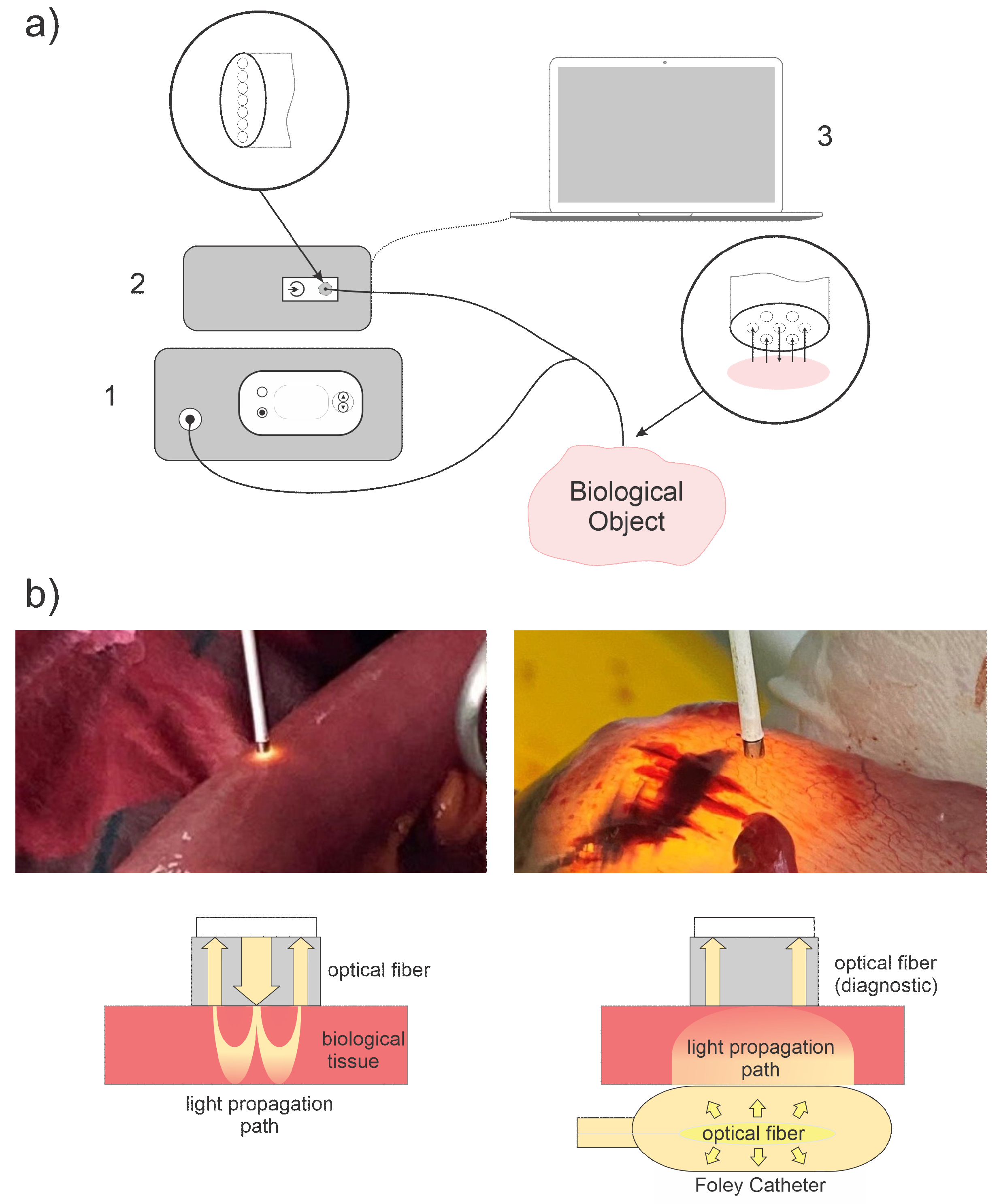
2.1. Spectroscopic Setup
2.2. Algorithm for Assessing the Hemoglobin Oxygen Saturation
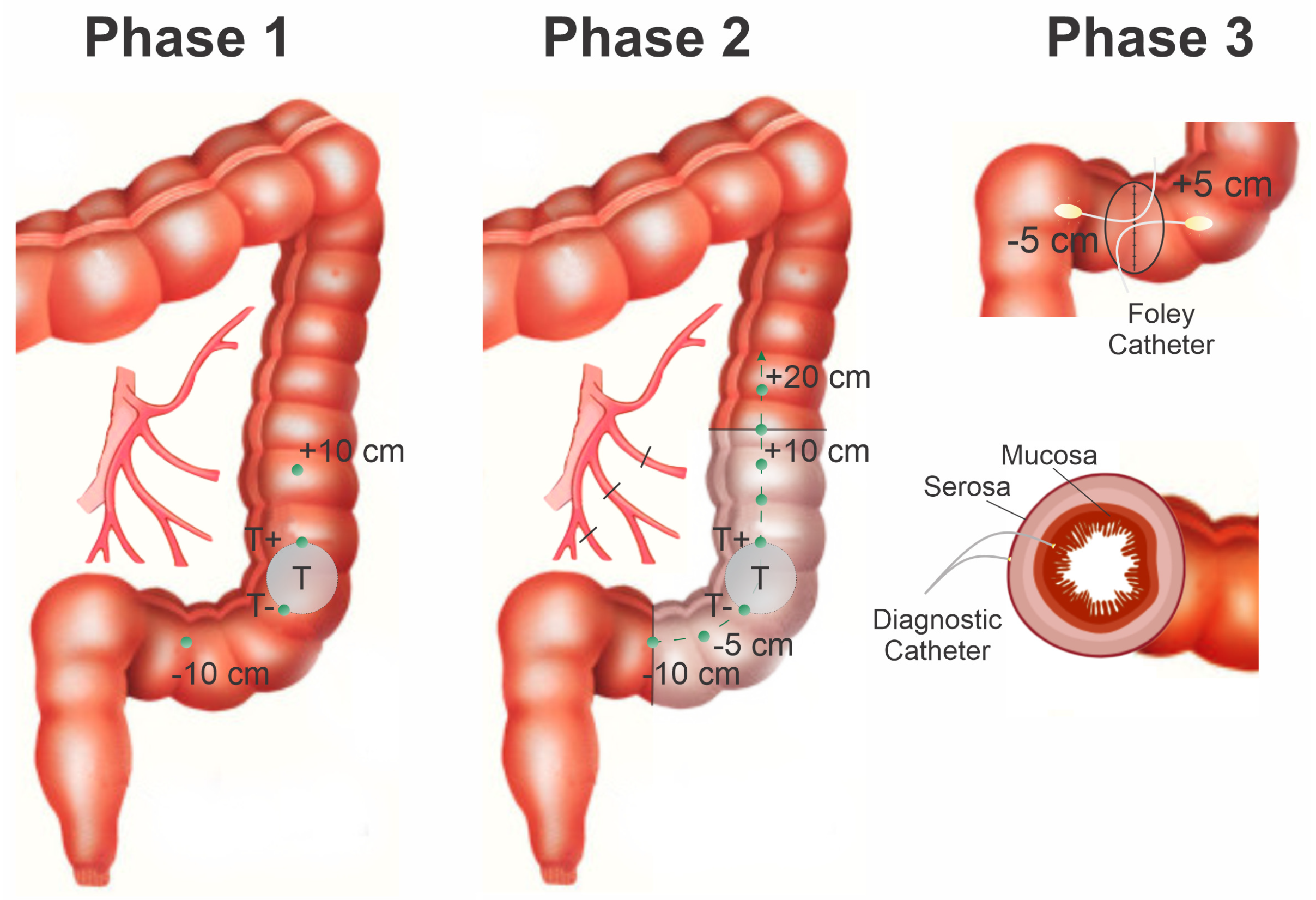
2.3. Biological Object of Research
3. Results and Discussion
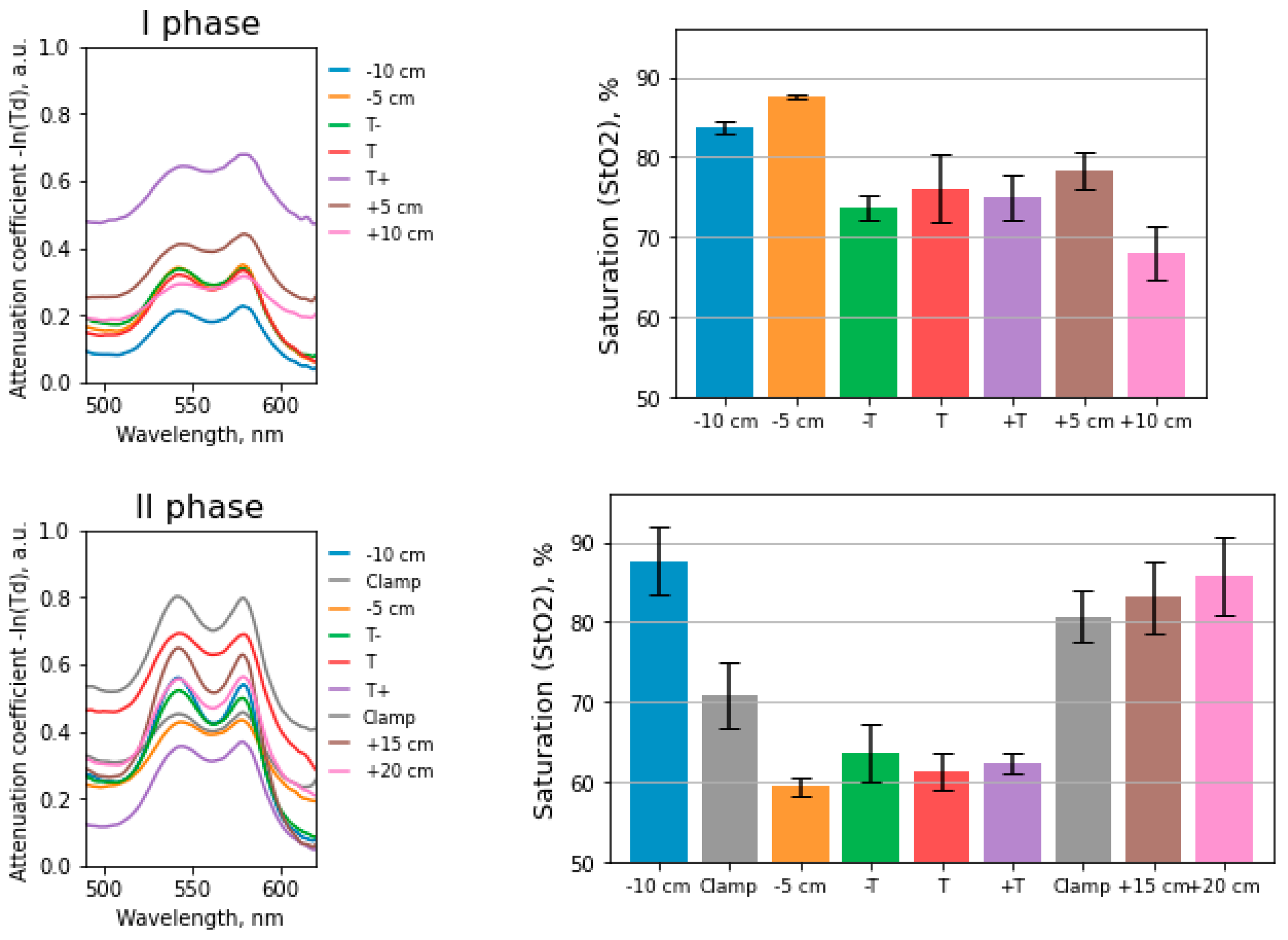
3.1. Mathematical Modeling of Diffuse Scattering and Transmission Spectra
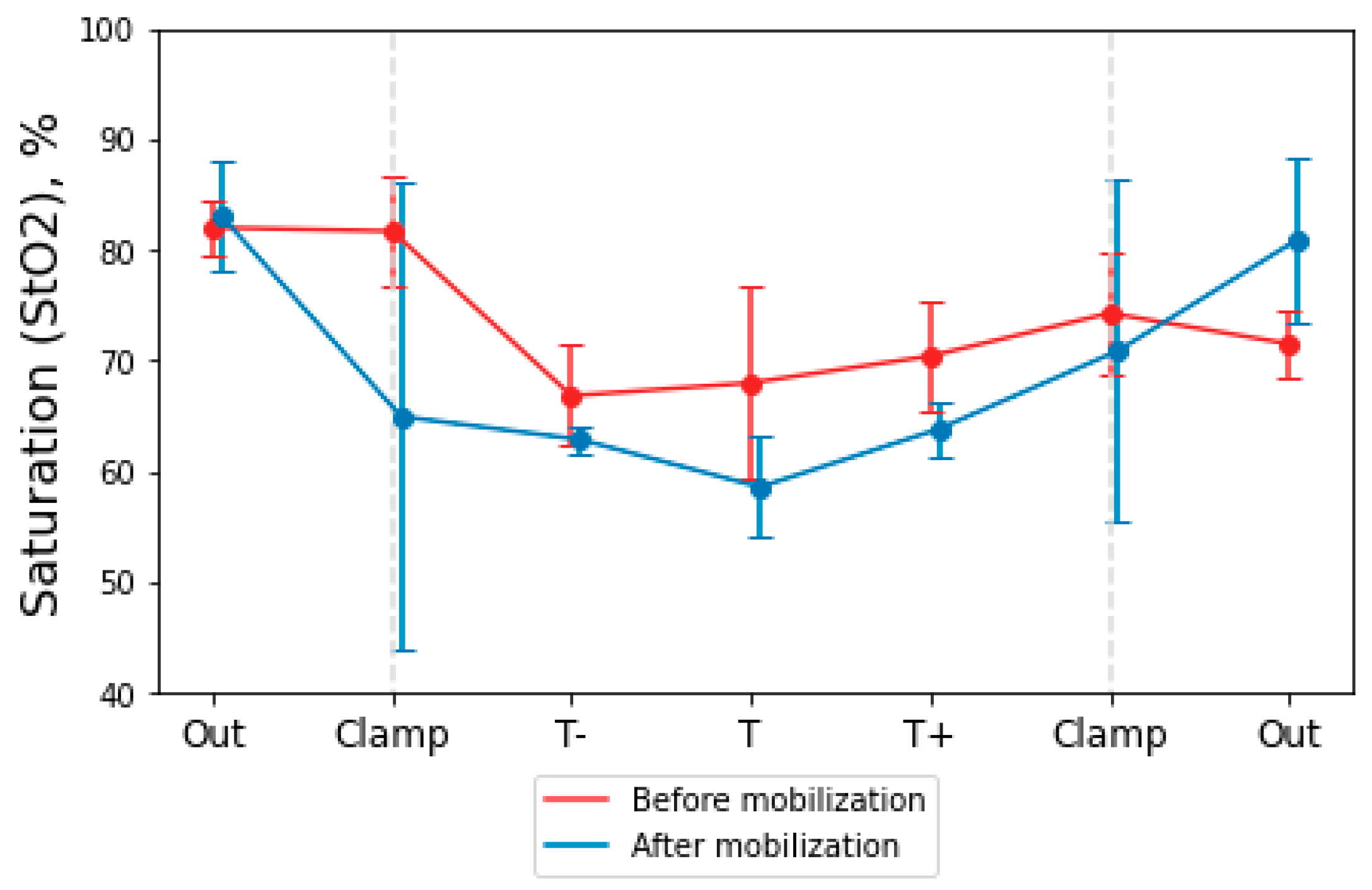
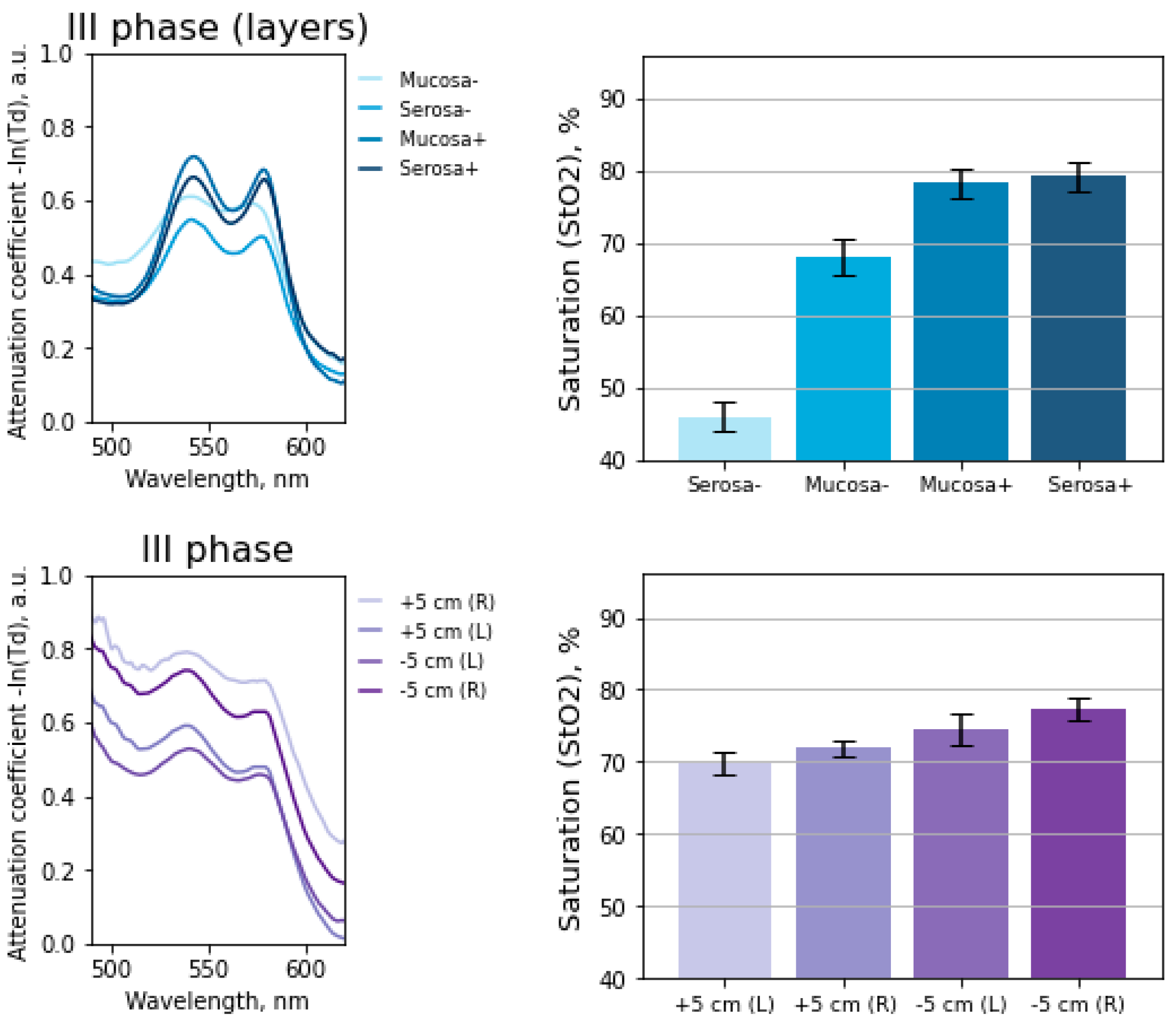
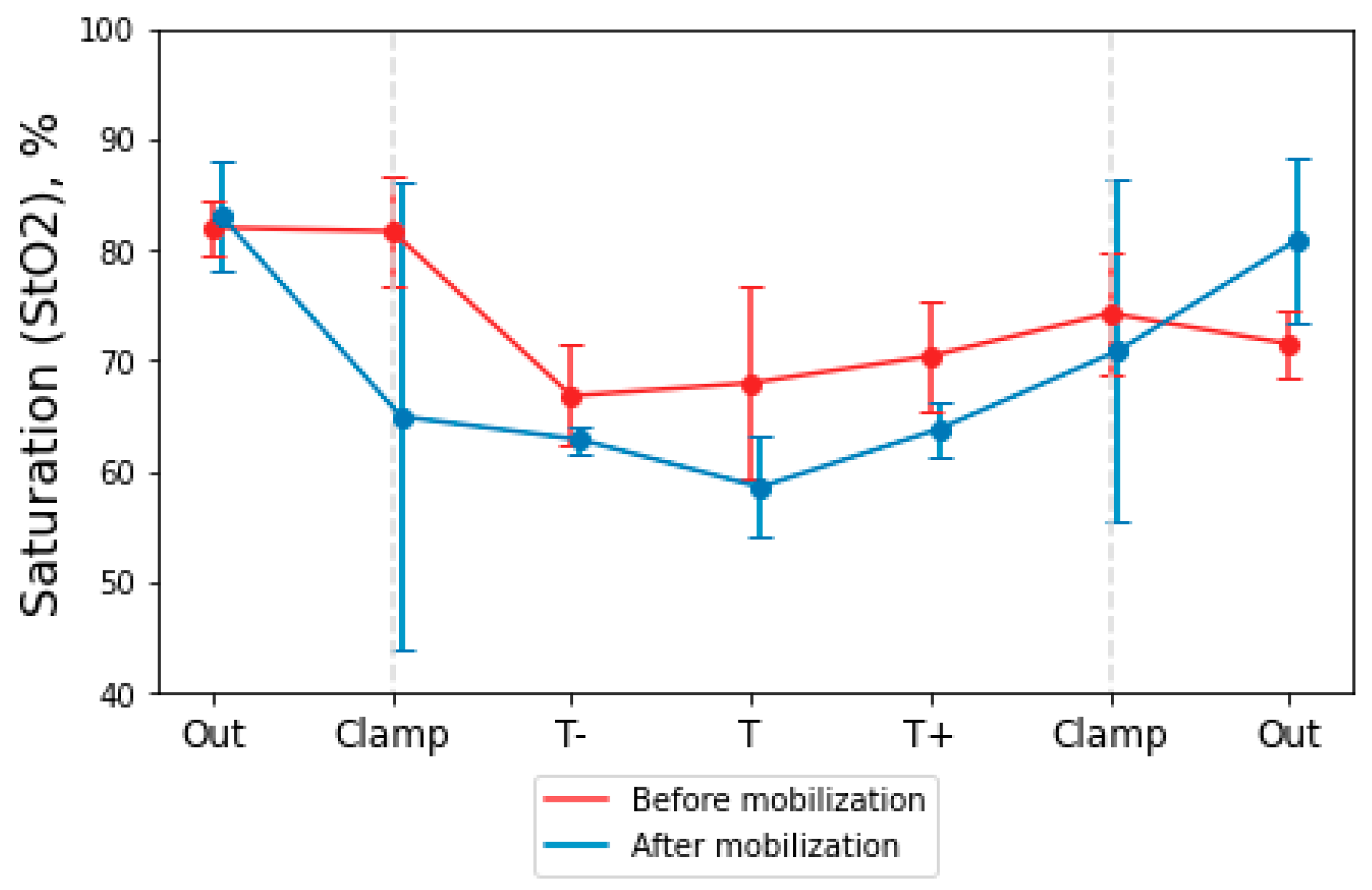
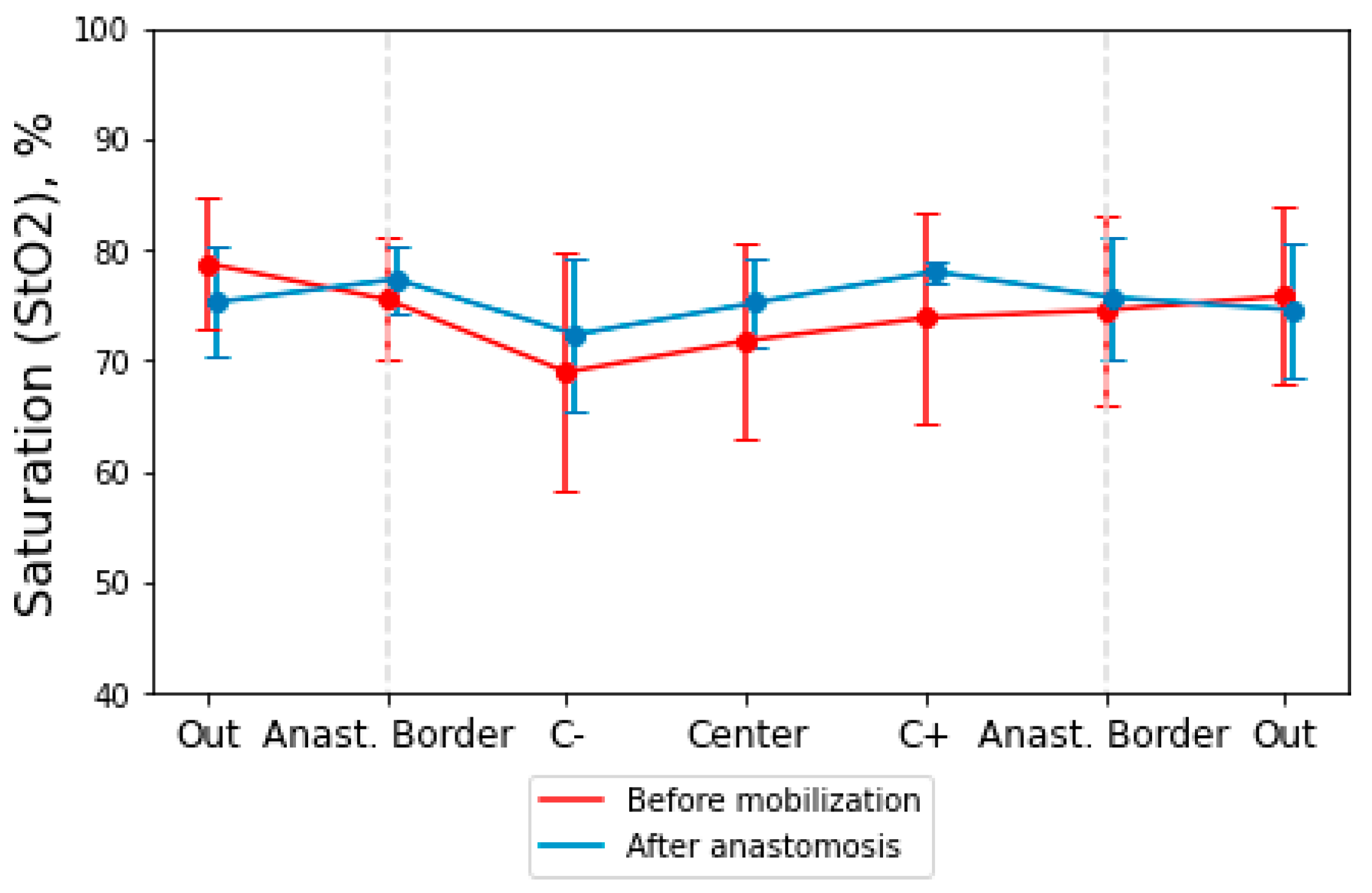
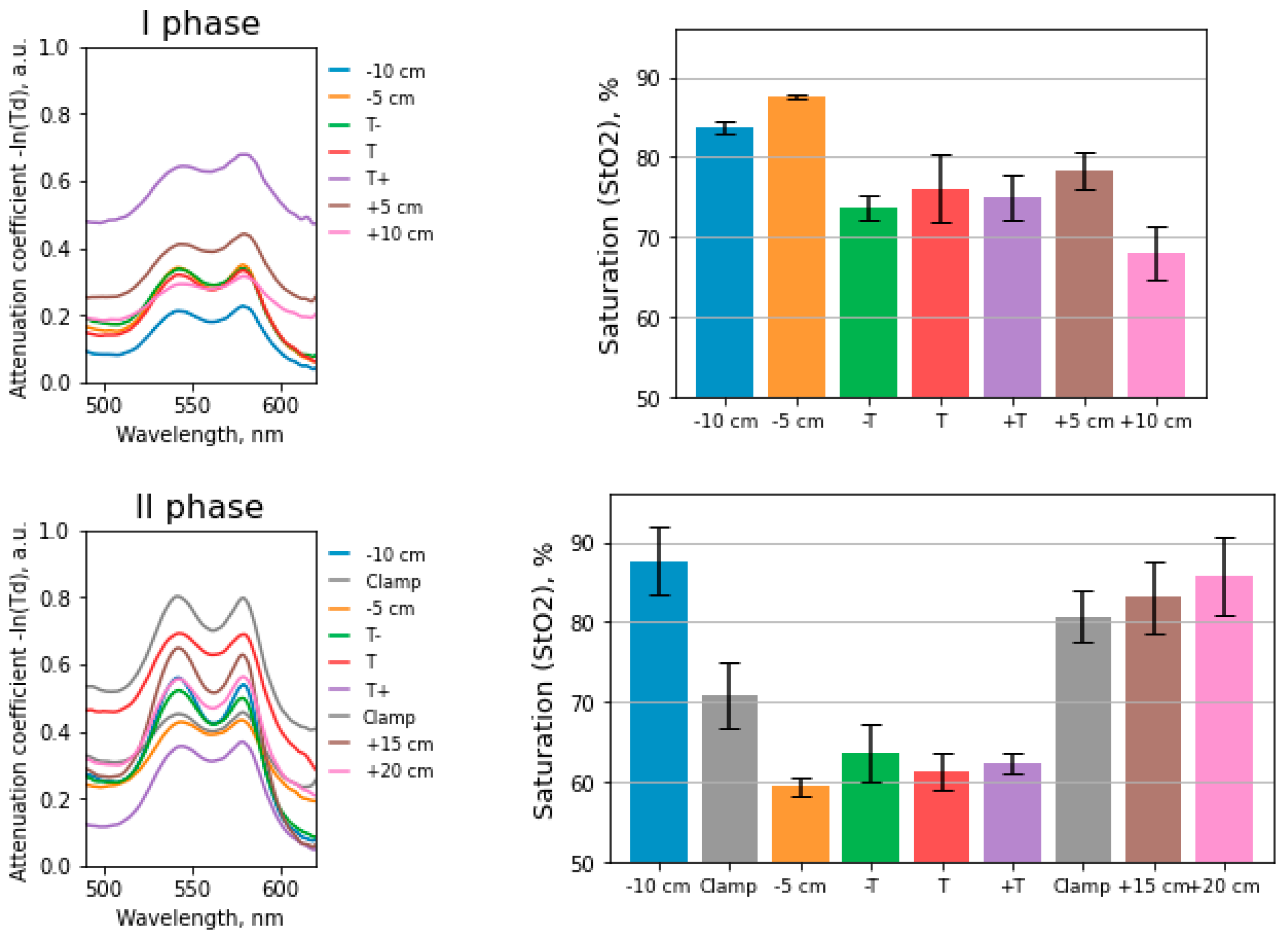
3.2. Study of the Level of Hemoglobin Oxygen Saturation in the Intestinal Wall
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gray, M.; Marland, J.R.; Murray, A.F.; Argyle, D.J.; Potter, M.A. Predictive and Diagnostic Biomarkers of Anastomotic Leakage: A Precision Medicine Approach for Colorectal Cancer Patients. J. Pers. Med. 2021, 11, 471. [Google Scholar] [CrossRef] [PubMed]
- Marinello, F.; Baguena, G.; Lucas, E.; Frasson, M.; Hervás, D.; Flor-Lorente, B.; Esclapez, P.; Espí, A.; García-Granero, E. Anastomotic leakage after colon cancer resection: Does the individual surgeon matter? Color. Dis. 2016, 18, 562–569. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, R.; Sparavigna, L.; Docimo, G.; Gubitosi, A.; Agresti, M.; Procaccini, E.; Docimo, L. Post-operative peritonitis due to anastomotic dehiscence after colonic resection. Ann. Ital. Chir. 2011, 82, 369–375. [Google Scholar] [PubMed]
- McDermott, F.; Heeney, A.; Kelly, M.; Steele, R.; Carlson, G.; Winter, D. Systematic review of preoperative, intraoperative and postoperative risk factors for colorectal anastomotic leaks. J. Br. Surg. 2015, 102, 462–479. [Google Scholar] [CrossRef] [PubMed]
- Kingham, T.P.; Pachter, H.L. Colonic anastomotic leak: Risk factors, diagnosis, and treatment. J. Am. Coll. Surg. 2009, 208, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Thornton, M.; Joshi, H.; Vimalachandran, C.; Heath, R.; Carter, P.; Gur, U.; Rooney, P. Management and outcome of colorectal anastomotic leaks. Int. J. Color. Dis. 2011, 26, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Boni, L.; David, G.; Dionigi, G.; Rausei, S.; Cassinotti, E.; Fingerhut, A. Indocyanine green-enhanced fluorescence to assess bowel perfusion during laparoscopic colorectal resection. Surg. Endosc. 2016, 30, 2736–2742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mangano, A.; Masrur, M.A.; Bustos, R.; Chen, L.L.; Fernandes, E.; Giulianotti, P.C. Near-Infrared Indocyanine Green-Enhanced Fluorescence and Minimally Invasive Colorectal Surgery: Review of the Literature. Surg. Technol. Int. 2018, 33, 77–83. [Google Scholar] [PubMed]
- Mirle, E.; Wogatzki, A.; Kunzmann, R.; Schoenfelder, A.M.; Litzke, L.F. Correlation between capillary oxygen saturation and small intestinal wall thickness in the equine colic patient. Vet. Rec. Open 2017, 4, e000197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salusjärvi, J.M.; Carpelan-Holmström, M.A.; Louhimo, J.M.; Kruuna, O.; Scheinin, T.M. Intraoperative colonic pulse oximetry in left-sided colorectal surgery: Can it predict anastomotic leak? Int. J. Color. Dis. 2018, 33, 333–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karliczek, A.; Benaron, D.; Baas, P.; Zeebregts, C.; Wiggers, T.; Van Dam, G. Intraoperative assessment of microperfusion with visible light spectroscopy for prediction of anastomotic leakage in colorectal anastomoses. Color. Dis. 2010, 12, 1018–1025. [Google Scholar] [CrossRef] [PubMed]
- Stratonnikov, A.A.; Loschenov, V.B. Evaluation of blood oxygen saturation in vivo from diffuse reflectance spectra. J. Biomed. Opt. 2001, 6, 457–467. [Google Scholar] [CrossRef] [PubMed]
- Jacques, S.L. Optical properties of biological tissues: A review. Phys. Med. Biol. 2013, 58, R37. [Google Scholar] [CrossRef] [PubMed]
- Tuchin, V.V. Tissue Optics; Society of Photo-Optical Instrumentation Engineers (SPIE): Bellingham, WA, USA, 2015. [Google Scholar]
- Wei, H.; Xing, D.; Wu, G.; Gu, H.; Lu, J.; Jin, Y.; Li, X.Y. Differences in optical properties between healthy and pathological human colon tissues using a Ti: Sapphire laser: An in vitro study using the Monte Carlo inversion technique. J. Biomed. Opt. 2005, 10, 044022. [Google Scholar] [CrossRef] [PubMed]
- Carneiro, I.; Carvalho, S.; Henrique, R.; Oliveira, L.; Tuchin, V.V. Kinetics of Optical Properties of Colorectal Muscle During Optical Clearing. IEEE J. Sel. Top. Quantum Electron. 2018, 25, 1–8. [Google Scholar] [CrossRef]
- Bashkatov, A.N.; Genina, E.A.; Kochubey, V.I.; Rubtsov, V.; Kolesnikova, E.A.; Tuchin, V.V. Optical properties of human colon tissues in the 350–2500 nm spectral range. Quantum Electron. 2014, 44, 779. [Google Scholar] [CrossRef] [Green Version]
- Wiesner, W.; Mortelé, K.J.; Ji, H.; Ros, P.R. Normal colonic wall thickness at CT and its relation to colonic distension. J. Comput. Assist. Tomogr. 2002, 26, 102–106. [Google Scholar] [CrossRef] [PubMed]
- Sanders, J.; Toor, I.S.; Yurik, T.M.; Keogh, B.E.; Mythen, M.; Montgomery, H.E. Tissue oxygen saturation and outcome after cardiac surgery. Am. J. Crit. Care 2011, 20, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Creteur, J.; Carollo, T.; Soldati, G.; Buchele, G.; De Backer, D.; Vincent, J.L. The prognostic value of muscle StO2 in septic patients. Intensive Care Med. 2007, 33, 1549–1556. [Google Scholar] [CrossRef] [PubMed]
- Lima, A.; van Bommel, J.; Jansen, T.C.; Ince, C.; Bakker, J. Low tissue oxygen saturation at the end of early goal-directed therapy is associated with worse outcome in critically ill patients. Crit. Care 2009, 13, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| One Side (OS) | Light Through (LT) | |
|---|---|---|
| linear | 0.0034 | 0.7449 |
| quadratic | 0.0039 | 0.7452 |
| cubic | 0.0054 | 0.1211 |
| a1 = 1.5 | 0.0033 | 0.1906 |
| a1 = 4 | 0.0029 | 0.0204 |
| func. superpos. for Mie scatters | 2.7220 | 0.0003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kustov, D.M.; Savelieva, T.A.; Mironov, T.A.; Kharnas, S.S.; Levkin, V.V.; Gorbunov, A.S.; Shiryaev, A.A.; Loschenov, V.B. Intraoperative Control of Hemoglobin Oxygen Saturation in the Intestinal Wall during Anastomosis Surgery. Photonics 2021, 8, 427. https://doi.org/10.3390/photonics8100427
Kustov DM, Savelieva TA, Mironov TA, Kharnas SS, Levkin VV, Gorbunov AS, Shiryaev AA, Loschenov VB. Intraoperative Control of Hemoglobin Oxygen Saturation in the Intestinal Wall during Anastomosis Surgery. Photonics. 2021; 8(10):427. https://doi.org/10.3390/photonics8100427
Chicago/Turabian StyleKustov, Daniil M., Tatiana A. Savelieva, Timofey A. Mironov, Sergey S. Kharnas, Vladimir V. Levkin, Andrey S. Gorbunov, Artem A. Shiryaev, and Victor B. Loschenov. 2021. "Intraoperative Control of Hemoglobin Oxygen Saturation in the Intestinal Wall during Anastomosis Surgery" Photonics 8, no. 10: 427. https://doi.org/10.3390/photonics8100427
APA StyleKustov, D. M., Savelieva, T. A., Mironov, T. A., Kharnas, S. S., Levkin, V. V., Gorbunov, A. S., Shiryaev, A. A., & Loschenov, V. B. (2021). Intraoperative Control of Hemoglobin Oxygen Saturation in the Intestinal Wall during Anastomosis Surgery. Photonics, 8(10), 427. https://doi.org/10.3390/photonics8100427