Standardizing Laser Speckle Orthogonal Contrast Imaging: Achieving Reproducible Measurements across Instruments


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
- Quantified Indices per Pixel: each pixel in the image should provide a quantified index of microcirculation activity, essential for informing and guiding treatment decisions.
- Stability in Repeated Acquisitions: when imaging the same area with the body at rest, the technology must produce consistently stable images and microcirculation activity values.
- Inter-Instrument Consistency: rResults must be comparable across different imaging systems.
- Dynamic and Accurate Imaging: the imaging system must exhibit sufficient dynamic range, stability, and accuracy to distinguish between different pathological states, despite challenges posed by in vivo conditions such as the cardiac cycle and unavoidable movements.
2. Materials and Methods
2.1. Experimental Setup
2.2. Contrast Variation Calibration Method (CVCM)
2.3. Equation for Normalized VMAI
3. Results
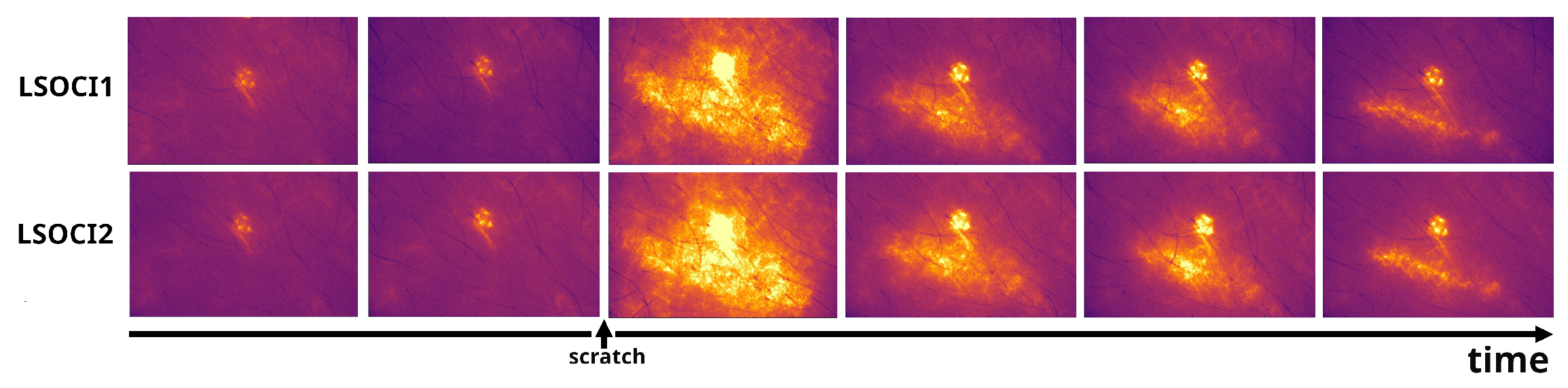
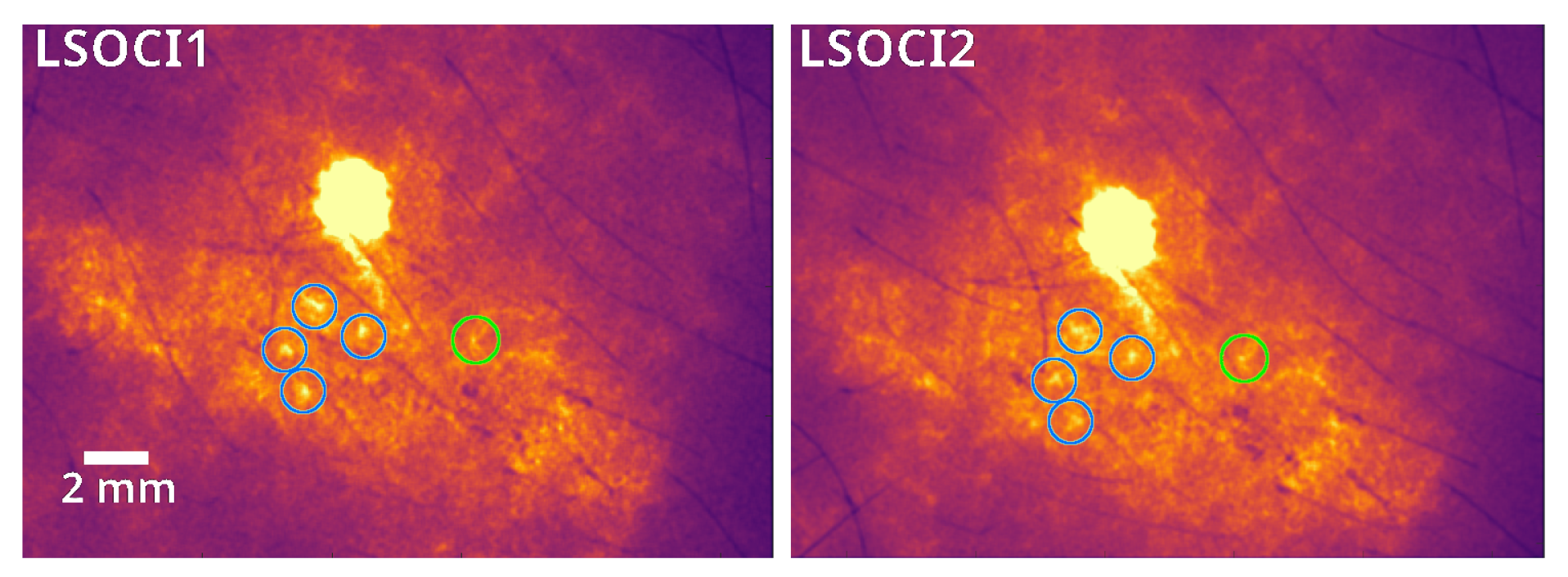
3.1. Qualitative Inter-Instrument Comparison for Temporal Speckle Contrast Images
3.2. Quantitative Inter-Instrument Comparison for Temporal Speckle Contrast Images
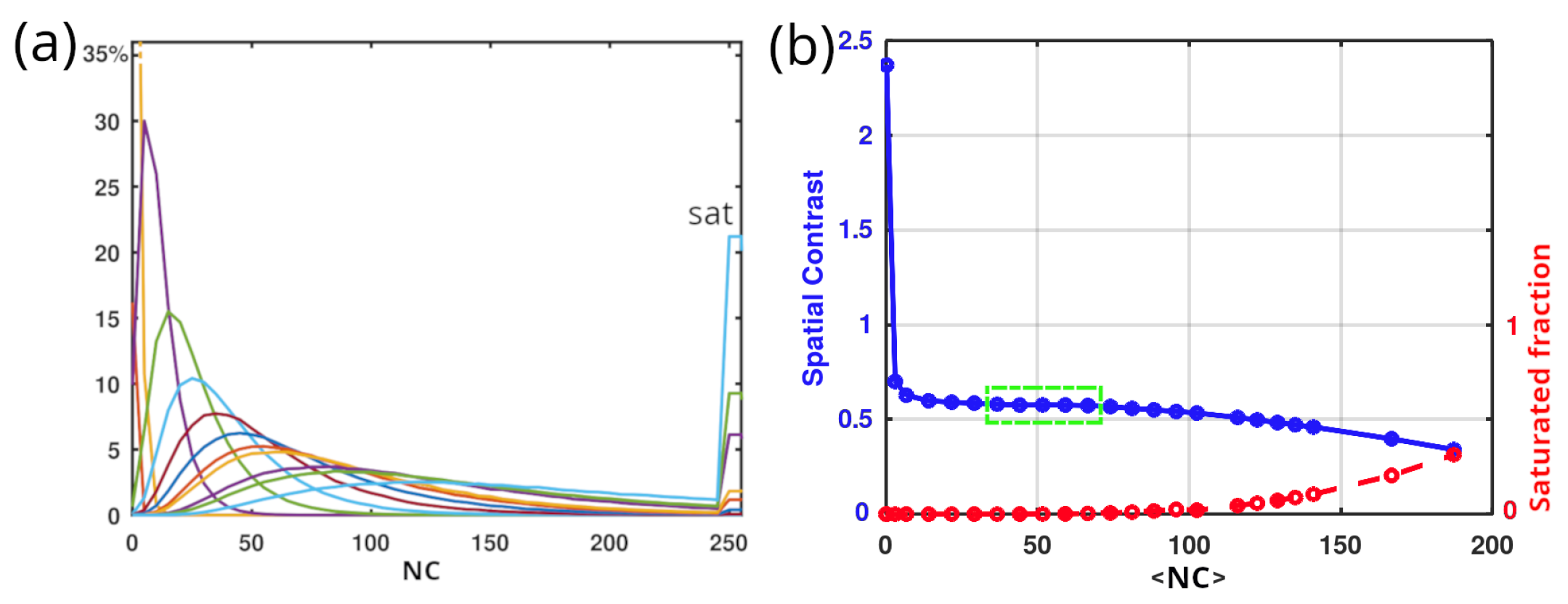
3.2.1. Contrast Linearity Domain
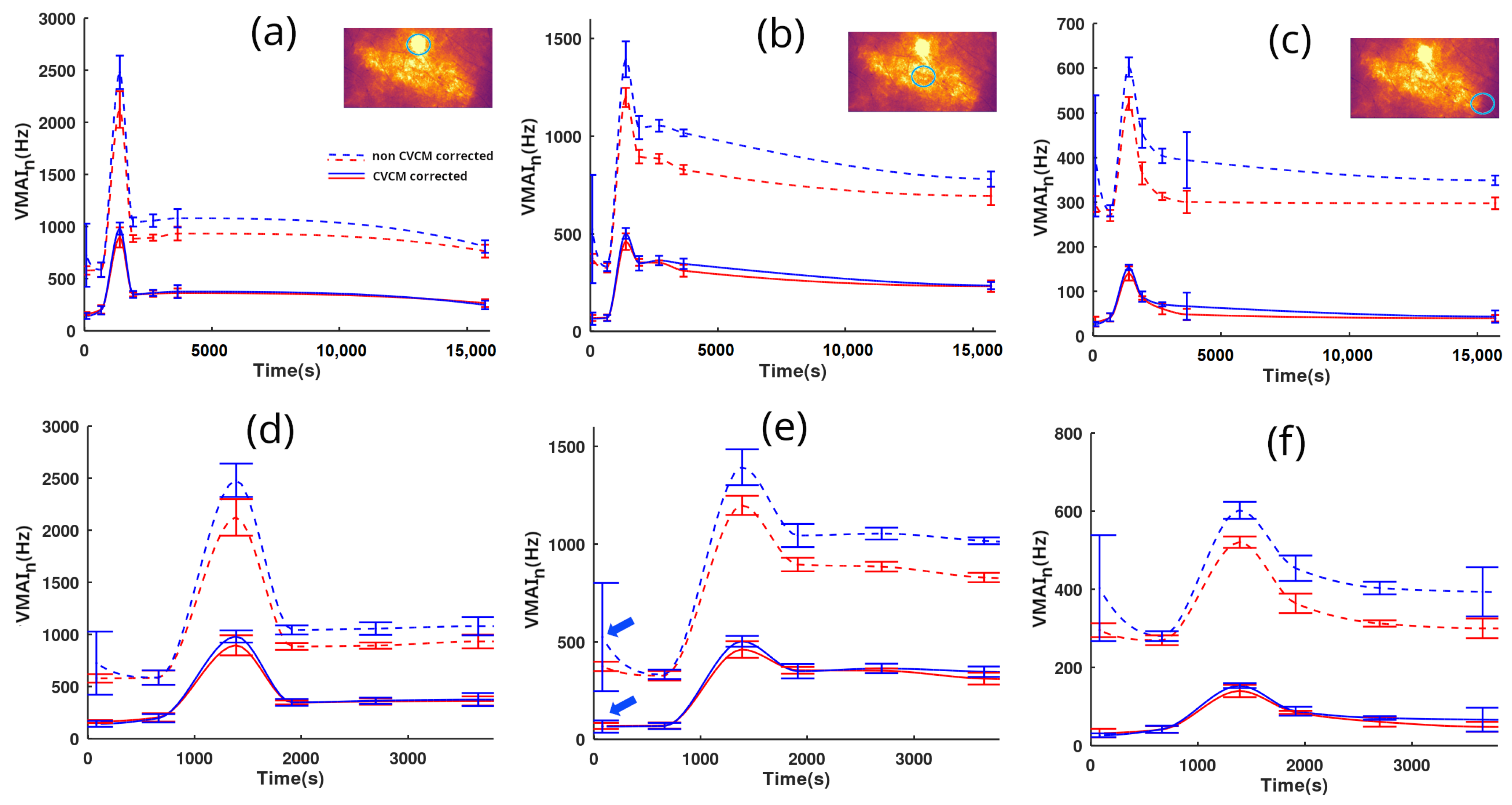
3.2.2. Measurements and Analysis between Two LSOCI Instruments
4. Discussion
5. Conclusions and Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stücker, M.; Horstmann, I.; Röchling, A.; Hoffmann, K.; Nüchel, C.; Altmeyer, P. Differential diagnosis of skin tumors using tumor microcirculation. In Skin Cancer and UV Radiation; Springer: Berlin/Heidelberg, Germany, 1997; pp. 999–1006. [Google Scholar]
- Li, J.; Cao, Y.; Liu, W.; Wang, Q.; Qian, Y.; Lu, P. Correlations among diabetic microvascular complications: A systematic review and meta-analysis. Sci. Rep. 2019, 9, 3137. [Google Scholar] [CrossRef]
- Strain, W.D.; Paldánius, P. Diabetes, cardiovascular disease and the microcirculation. Cardiovasc. Diabetol. 2018, 17, 57. [Google Scholar] [CrossRef]
- Lara Rezende, G.; da Silva, M.d.G.; Soares Takano, G.H.; Lopes Sampaio, A.L.; Oliveira Soares, R.; dos Santos Kückelhaus, C.; Souza Kückelhaus, S.A. Hypertension causes structural lesions in the microvasculature of the posterior nasal mucosa. Hypertens. Res. 2021, 44, 591–594. [Google Scholar] [CrossRef]
- De Backer, D.; Creteur, J.; Preiser, J.C.; Dubois, M.J.; Vincent, J.L. Microvascular blood flow is altered in patients with sepsis. Am. J. Respir. Crit. Care Med. 2002, 166, 98–104. [Google Scholar] [CrossRef]
- Damiani, E.; Carsetti, A.; Casarotta, E.; Scorcella, C.; Domizi, R.; Adrario, E.; Donati, A. Microvascular alterations in patients with SARS-CoV-2 severe pneumonia. Ann. Intensive Care 2020, 10, 60. [Google Scholar] [CrossRef]
- Narzulaeva, U. Pathogenetic Mechanisms of Microcirculation disorders. Int. Bull. Med. Sci. Clin. Res. 2023, 3, 60–65. [Google Scholar]
- Zharkikh, E.V.; Loktionova, Y.I.; Fedorovich, A.A.; Gorshkov, A.Y.; Dunaev, A.V. Assessment of blood microcirculation changes after COVID-19 using wearable laser Doppler flowmetry. Diagnostics 2023, 13, 920. [Google Scholar] [CrossRef]
- Sdobnov, A.; Piavchenko, G.; Bykov, A.; Meglinski, I. Advances in dynamic light scattering imaging of blood flow. Laser Photonics Rev. 2024, 18, 2300494. [Google Scholar] [CrossRef]
- Ruan, Z.; Li, R.; Dong, W.; Cui, Z.; Yang, H.; Ren, R. Laser speckle contrast imaging to monitor microcirculation: An effective method to predict outcome in patients with sepsis and septic shock. Front. Bioeng. Biotechnol. 2023, 10, 1067739. [Google Scholar] [CrossRef]
- Golubova, N.; Potapova, E.; Seryogina, E.; Dremin, V. Time–frequency analysis of laser speckle contrast for transcranial assessment of cerebral blood flow. Biomed. Signal Process. Control 2023, 85, 104969. [Google Scholar] [CrossRef]
- Briers, J.D.; Webster, S. Laser speckle contrast analysis (LASCA): A nonscanning, full-field technique for monitoring capillary blood flow. J. Biomed. Opt. 1996, 1, 174–179. [Google Scholar] [CrossRef]
- Colin, E.; Plyer, A.; Golzio, M.; Meyer, N.; Favre, G.; Orlik, X. Imaging of the skin microvascularization using spatially depolarized dynamic speckle. J. Biomed. Opt. 2022, 27, 046003. [Google Scholar] [CrossRef]
- Kirkpatrick, S.J.; Duncan, D.D.; Wells-Gray, E.M. Detrimental effects of speckle-pixel size matching in laser speckle contrast imaging. Opt. Lett. 2008, 33, 2886–2888. [Google Scholar] [CrossRef]
- Dupont, J.; Orlik, X.; Ghabbach, A.; Zerrad, M.; Soriano, G.; Amra, C. Polarization analysis of speckle field below its transverse correlation width: Application to surface and bulk scattering. Opt. Express 2014, 22, 24133–24141. [Google Scholar] [CrossRef]
- Wang, C.; Cao, Z.; Jin, X.; Lin, W.; Zheng, Y.; Zeng, B.; Xu, M. Robust quantitative single-exposure laser speckle imaging with true flow speckle contrast in the temporal and spatial domains. Biomed. Opt. Express 2019, 10, 4097–4114. [Google Scholar] [CrossRef]
- Liu, H.L.; Yuan, Y.; Han, L.; Bi, Y.; Yu, W.Y.; Yu, Y. Wide dynamic range measurement of blood flow in vivo using laser speckle contrast imaging. J. Biomed. Opt. 2024, 29, 016009. [Google Scholar] [CrossRef]
- Postnov, D.D.; Tang, J.; Erdener, S.E.; Kılıç, K.; Boas, D.A. Dynamic light scattering imaging. Sci. Adv. 2020, 6, eabc4628. [Google Scholar] [CrossRef]
- Fercher, A.; Briers, D. Flow visualization by means of single-exposure speckle photography. Opt. Commun. 1981, 37, 326–330. [Google Scholar] [CrossRef]
- Maret, G. Diffusing-wave spectroscopy. Curr. Opin. Colloid Interface Sci. 1997, 2, 251–257. [Google Scholar] [CrossRef]
- Goldfischer, L.I. Autocorrelation function and power spectral density of laser-produced speckle patterns. JOSA 1965, 55, 247–253. [Google Scholar] [CrossRef]
- Duncan, D.D.; Kirkpatrick, S.J. Can laser speckle flowmetry be made a quantitative tool? JOSA A 2008, 25, 2088–2094. [Google Scholar] [CrossRef]
- Ramirez-San-Juan, J.C.; Ramos-Garcia, R.; Guizar-Iturbide, I.; Martinez-Niconoff, G.; Choi, B. Impact of velocity distribution assumption on simplified laser speckle imaging equation. Opt. Express 2008, 16, 3197–3203. [Google Scholar] [CrossRef] [PubMed]
- Sunil, S.; Zilpelwar, S.; Boas, D.A.; Postnov, D.D. Guidelines for obtaining an absolute blood flow index with laser speckle contrast imaging. bioRxiv 2021. [Google Scholar] [CrossRef]
- Goodman, J.W. Statistical Optics; John Wiley & Sons: Hoboken, NJ, USA, 2015. [Google Scholar]
- Bergoënd, I.; Orlik, X.; Lacot, E. Study of a circular Gaussian transition in an optical speckle field. J. Eur. Opt. Soc.-Rapid Publ. 2008, 3. [Google Scholar] [CrossRef]
- Postnov, D.D.; Cheng, X.; Erdener, S.E.; Boas, D.A. Choosing a laser for laser speckle contrast imaging. Sci. Rep. 2019, 9, 2542. [Google Scholar] [CrossRef]
- Qureshi, M.M.; Allam, N.; Im, J.; Kwon, H.S.; Chung, E.; Vitkin, I.A. Advances in laser speckle imaging: From qualitative to quantitative hemodynamic assessment. J. Biophotonics 2024, 17, e202300126. [Google Scholar] [CrossRef]
- Parthasarathy, A.B.; Tom, W.J.; Gopal, A.; Zhang, X.; Dunn, A.K. Robust flow measurement with multi-exposure speckle imaging. Opt. Express 2008, 16, 1975–1989. [Google Scholar] [CrossRef]
- Chammas, M.; Pain, F. Synthetic exposure with a CMOS camera for multiple exposure speckle imaging of blood flow. Sci. Rep. 2022, 12, 4708. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orlik, X.; Colin, E.; Plyer, A. Standardizing Laser Speckle Orthogonal Contrast Imaging: Achieving Reproducible Measurements across Instruments. Photonics 2024, 11, 585. https://doi.org/10.3390/photonics11070585
Orlik X, Colin E, Plyer A. Standardizing Laser Speckle Orthogonal Contrast Imaging: Achieving Reproducible Measurements across Instruments. Photonics. 2024; 11(7):585. https://doi.org/10.3390/photonics11070585
Chicago/Turabian StyleOrlik, Xavier, Elise Colin, and Aurélien Plyer. 2024. "Standardizing Laser Speckle Orthogonal Contrast Imaging: Achieving Reproducible Measurements across Instruments" Photonics 11, no. 7: 585. https://doi.org/10.3390/photonics11070585
APA StyleOrlik, X., Colin, E., & Plyer, A. (2024). Standardizing Laser Speckle Orthogonal Contrast Imaging: Achieving Reproducible Measurements across Instruments. Photonics, 11(7), 585. https://doi.org/10.3390/photonics11070585