Numerical Analysis of the Effect of Decentered Refractive Segmented Extended Depth of Focus (EDoF) Intraocular Lenses on Predicted Visual Outcomes

 and
and
Abstract
1. Introduction
2. Materials and Methods
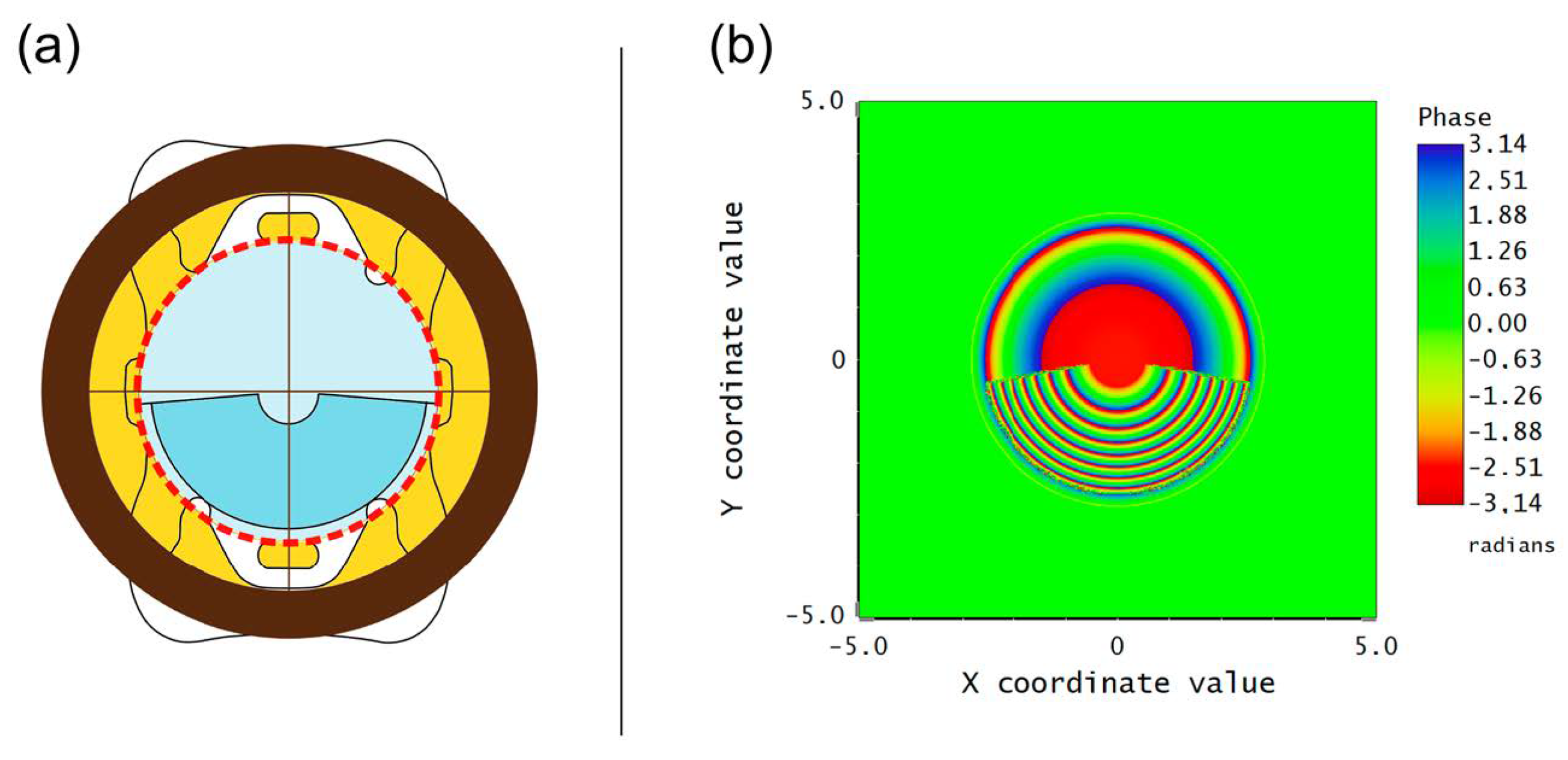
2.1. Multifocal Intraocular Lens
2.2. Numerical Evaluation
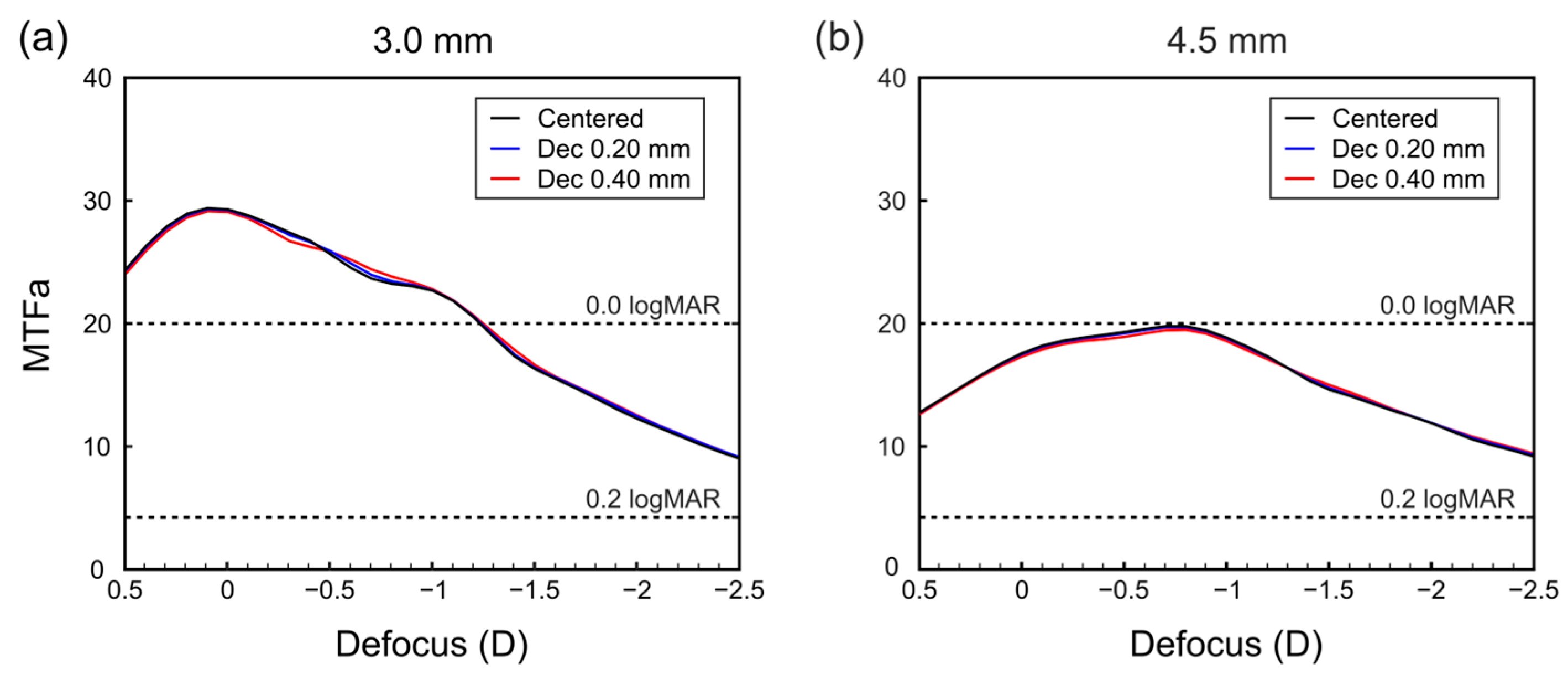
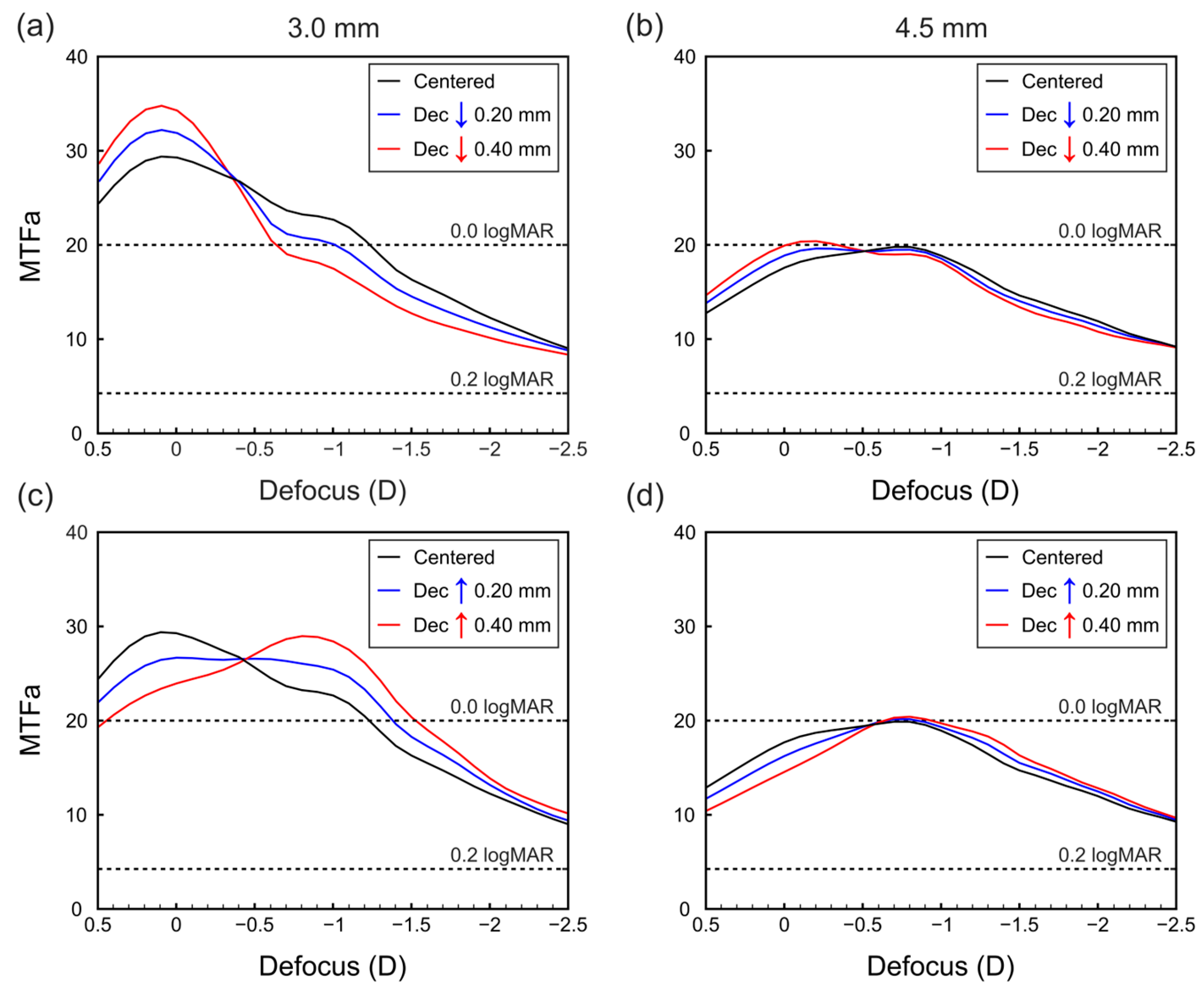
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Charman, W.N. Developments in the Correction of Presbyopia II: Surgical Approaches. Ophthalmic Physiol. Opt. 2014, 34, 397–426. [Google Scholar] [CrossRef] [PubMed]
- Gatinel, D.; Houbrechts, Y. Comparison of Bifocal and Trifocal Diffractive and Refractive Intraocular Lenses Using an Optical Bench. J. Cataract Refract. Surg. 2013, 39, 1093–1099. [Google Scholar] [CrossRef] [PubMed]
- Durrie, D.S.; Moshifar, M. Dysfunctional lens syndrome. In Proceedings of the Annual Meeting of ISRS. Pursuit of Perfection. Section II: Intraocular Refractive Surgery Topics, Chicago, IL, USA; 2016. [Google Scholar]
- Durrie, D.S. Dysfunctional Lens Syndrome, a New Way to Educate Patients—American Academy of Ophthalmology. Available online: https://www.aao.org/eyenet/academy-live/detail/dysfunctional-lens-syndrome-educate-patients (accessed on 9 March 2023).
- Rampat, R.; Gatinel, D. Multifocal and Extended Depth-of-Focus Intraocular Lenses in 2020. Ophthalmology 2021, 128, e164–e185. [Google Scholar] [CrossRef]
- Liu, J.; Dong, Y.; Wang, Y. Efficacy and Safety of Extended Depth of Focus Intraocular Lenses in Cataract Surgery: A Systematic Review and Meta-Analysis. BMC Ophthalmol. 2019, 19, 198. [Google Scholar] [CrossRef]
- MacRae, S.; Holladay, J.T.; Glasser, A.; Calogero, D.; Hilmantel, G.; Masket, S.; Stark, W.; Tarver, M.E.; Nguyen, T.; Eydelman, M. Special Report: American Academy of Ophthalmology Task Force Consensus Statement for Extended Depth of Focus Intraocular Lenses. Ophthalmology 2017, 124, 139–141. [Google Scholar] [CrossRef]
- Chen, X.-Y.; Wang, Y.-C.; Zhao, T.-Y.; Wang, Z.-Z.; Wang, W. Tilt and Decentration with Various Intraocular Lenses: A Narrative Review. World J. Clin. Cases 2022, 10, 3639–3646. [Google Scholar] [CrossRef]
- Pérez-Merino, P.; Marcos, S. Effect of Intraocular Lens Decentration on Image Quality Tested in a Custom Model Eye. J. Cataract Refract. Surg. 2018, 44, 889–896. [Google Scholar] [CrossRef] [PubMed]
- Gu, X.; Chen, X.; Yang, G.; Wang, W.; Xiao, W.; Jin, G.; Wang, L.; Dai, Y.; Ruan, X.; Liu, Z.; et al. Determinants of Intraocular Lens Tilt and Decentration after Cataract Surgery. Ann. Transl. Med. 2020, 8, 921. [Google Scholar] [CrossRef]
- Kimura, S.; Morizane, Y.; Shiode, Y.; Hirano, M.; Doi, S.; Toshima, S.; Fujiwara, A.; Shiraga, F. Assessment of Tilt and Decentration of Crystalline Lens and Intraocular Lens Relative to the Corneal Topographic Axis Using Anterior Segment Optical Coherence Tomography. PLoS ONE 2017, 12, e0184066. [Google Scholar] [CrossRef]
- Poyales, F.; Garzón, N.; Rozema, J.J.; Romero, C.; de Zárate, B.O. Stability of a Novel Intraocular Lens Design: Comparison of Two Trifocal Lenses. J. Refract. Surg. 2016, 32, 394–402. [Google Scholar] [CrossRef]
- Ashena, Z.; Maqsood, S.; Ahmed, S.N.; Nanavaty, M.A. Effect of Intraocular Lens Tilt and Decentration on Visual Acuity, Dysphotopsia and Wavefront Aberrations. Vision 2020, 4, 41. [Google Scholar] [CrossRef] [PubMed]
- Meng, J.; He, W.; Rong, X.; Miao, A.; Lu, Y.; Zhu, X. Decentration and Tilt of Plate-Haptic Multifocal Intraocular Lenses in Myopic Eyes. Eye Vis. 2020, 7, 17. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Xie, L.; Huang, Y. Effects of Decentration and Tilt at Different Orientations on the Optical Performance of a Rotationally Asymmetric Multifocal Intraocular Lens. J. Cataract Refract. Surg. 2019, 45, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Alió, J.L.; Plaza-Puche, A.B.; Javaloy, J.; Ayala, M.J.; Vega-Estrada, A. Clinical and Optical Intraocular Performance of Rotationally Asymmetric Multifocal IOL Plate-Haptic Design Versus C-Loop Haptic Design. J. Refract. Surg. 2013, 29, 252–259. [Google Scholar] [CrossRef]
- Darian-Smith, E.; Versace, P. Visual Performance and Positional Stability of a Capsulorhexis-Fixated Extended Depth-of-Focus Intraocular Lens. J. Cataract Refract. Surg. 2020, 46, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Shajari, M.; Sonntag, R.; Niermann, T.; Holland, D.; Kohnen, T.; Priglinger, S.; Mayer, W.J. Determining and Comparing the Effective Lens Position and Refractive Outcome of a Novel Rhexis-Fixated Lens to Established Lens Designs. Am. J. Ophthalmol. 2020, 213, 62–68. [Google Scholar] [CrossRef]
- Auffarth, G.U.; Friedmann, E.; Breyer, D.; Kaymak, H.; Holland, D.; Dick, B.; Petzold, A.; Shah, S.; Ladaria, L.S.; Garcia, S.A.; et al. Stability and Visual Outcomes of the Capsulotomy-Fixated FEMTIS-IOL After Automated Femtosecond Laser–Assisted Anterior Capsulotomy. Am. J. Ophthalmol. 2021, 225, 27–37. [Google Scholar] [CrossRef]
- García, S.; Salvá, L.; García-Delpech, S.; Martínez-Espert, A.; Ferrando, V.; Montagud-Martínez, D. Polychromatic Assessment of a Refractive Segmented EDOF Intraocular Lens. J. Clin. Med. 2022, 11, 1480. [Google Scholar] [CrossRef]
- Atchison, D.A. Optical Models for Human Myopic Eyes. Vis. Res. 2006, 46, 2236–2250. [Google Scholar] [CrossRef]
- Atchison, D.A.; Smith, G. Chromatic Dispersions of the Ocular Media of Human Eyes. J. Opt. Soc. Am. A 2005, 22, 29. [Google Scholar] [CrossRef]
- Remón, L.; Cabeza-gil, I. Influence of Material and Haptic Design on the Mechanical Stability of Intraocular Lenses by Means of Finite-Element Modeling. J. Biomed. Opt. 2018, 23, 1. [Google Scholar] [CrossRef] [PubMed]
- Guo, H.; Goncharov, A.; Dainty, C. Intraocular Lens Implantation Position Sensitivity as a Function of Refractive Error. Ophthalmic Physiol. Opt. 2012, 32, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Geniusz, M.; Kazimierska, M.; Zając, M. Impact of Glistenings on Optical Image Quality of Intraocular Lenses—A Preliminary Study. Photonics Lett. Pol. 2015, 7, 109–111. [Google Scholar] [CrossRef]
- Vega, F.; Millán, M.S.; Garzón, N.; Altemir, I.; Poyales, F.; Larrosa, J.M. Visual Acuity of Pseudophakic Patients Predicted from In-Vitro Measurements of Intraocular Lenses with Different Design. Biomed. Opt. Express 2018, 9, 4893. [Google Scholar] [CrossRef] [PubMed]
- Alarcon, A.; Canovas, C.; Rosen, R.; Weeber, H.; Tsai, L.; Hileman, K.; Piers, P. Preclinical Metrics to Predict Through-Focus Visual Acuity for Pseudophakic Patients. Biomed. Opt. Express 2016, 7, 1877. [Google Scholar] [CrossRef]
- Fernández, J.; Rodríguez-Vallejo, M.; Martínez, J.; Burguera, N.; Piñero, D.P. Prediction of Visual Acuity and Contrast Sensitivity From Optical Simulations with Multifocal Intraocular Lenses. J. Refract. Surg. 2019, 35, 789–795. [Google Scholar] [CrossRef]
- Atchison, D.A.; Thibos, L.N. Optical Models of the Human Eye. Clin. Exp. Optom. 2016, 99, 99–106. [Google Scholar] [CrossRef]
- Liou, H.-L.; Brennan, N.A. Anatomically Accurate, Finite Model Eye for Optical Modeling. J. Opt. Soc. Am. A 1997, 14, 1684. [Google Scholar] [CrossRef]
- Patel, S.; Marshall, J.; Fitzke, F.W. Model for Predicting the Optical Performance of the Eye in Refractive Surgery. Refract. Corneal Surg. 1993, 9, 366–375. [Google Scholar] [CrossRef]
- García, C.; Camps, V.J.; Caballero, M.T.; Piñero, D.P.; Tañá, P.; Tello, C.; Miret, J.J. Comparison of the Optical Quality Vision between Real Post-LASIK Myopic Laser Surgery and the Simulated Implantation of a Phakic IOL in Low Myopia. Sci. Rep. 2022, 12, 18942. [Google Scholar] [CrossRef]
- Radhakrishnan, A.; Dorronsoro, C.; Marcos, S. Differences in Visual Quality with Orientation of a Rotationally Asymmetric Bifocal Intraocular Lens Design. J. Cataract Refract. Surg. 2016, 42, 1276–1287. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Surface | Radius (mm) | Asphericity (Q) | Thickness (mm) | Refractive Index | Abbe Number |
|---|---|---|---|---|---|
| Cornea | 7.770 | −0.150 | 0.550 | 1.376 | 55.48 |
| Aqueous | 6.400 | −0.275 | 3.150 | 1.3374 | 50.37 |
| Pupil | - | - | - | 1.3374 | 50.37 |
| Anterior IOL | 21.400 | - | 0.700 | 1.460 | 58.00 |
| Posterior IOL | −8.700 | −1.275 | 18.900 | 1.336 | 51.30 |
| Retina X | −12.720 | 0.250 | - | - | - |
| Retina Y | −12.910 | 0.270 | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García, S.; Salvá, L.; García-Delpech, S.; Martínez-Espert, A.; Ferrando, V. Numerical Analysis of the Effect of Decentered Refractive Segmented Extended Depth of Focus (EDoF) Intraocular Lenses on Predicted Visual Outcomes. Photonics 2023, 10, 850. https://doi.org/10.3390/photonics10070850
García S, Salvá L, García-Delpech S, Martínez-Espert A, Ferrando V. Numerical Analysis of the Effect of Decentered Refractive Segmented Extended Depth of Focus (EDoF) Intraocular Lenses on Predicted Visual Outcomes. Photonics. 2023; 10(7):850. https://doi.org/10.3390/photonics10070850
Chicago/Turabian StyleGarcía, Scott, Luis Salvá, Salvador García-Delpech, Anabel Martínez-Espert, and Vicente Ferrando. 2023. "Numerical Analysis of the Effect of Decentered Refractive Segmented Extended Depth of Focus (EDoF) Intraocular Lenses on Predicted Visual Outcomes" Photonics 10, no. 7: 850. https://doi.org/10.3390/photonics10070850
APA StyleGarcía, S., Salvá, L., García-Delpech, S., Martínez-Espert, A., & Ferrando, V. (2023). Numerical Analysis of the Effect of Decentered Refractive Segmented Extended Depth of Focus (EDoF) Intraocular Lenses on Predicted Visual Outcomes. Photonics, 10(7), 850. https://doi.org/10.3390/photonics10070850