
Blisters and Milia around the Peritoneal Dialysis Catheter: A Case of Localized Bullous Pemphigoid



{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
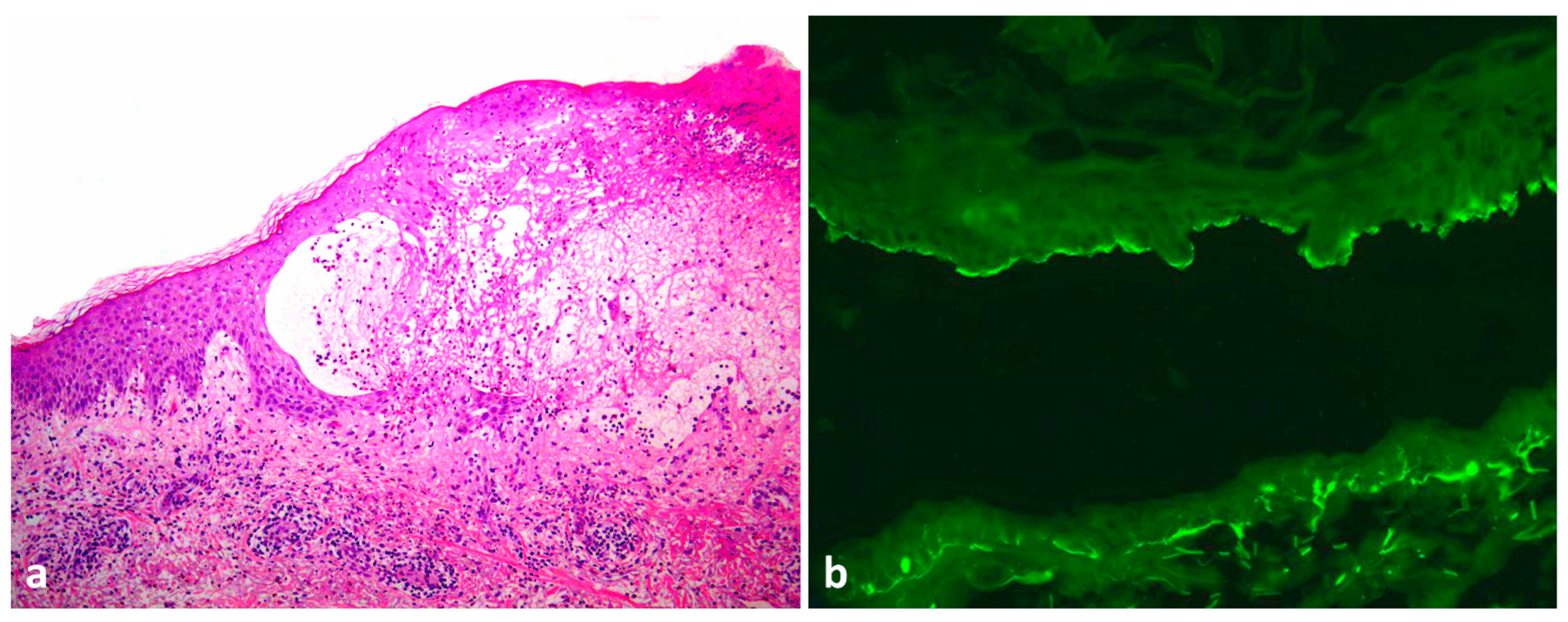
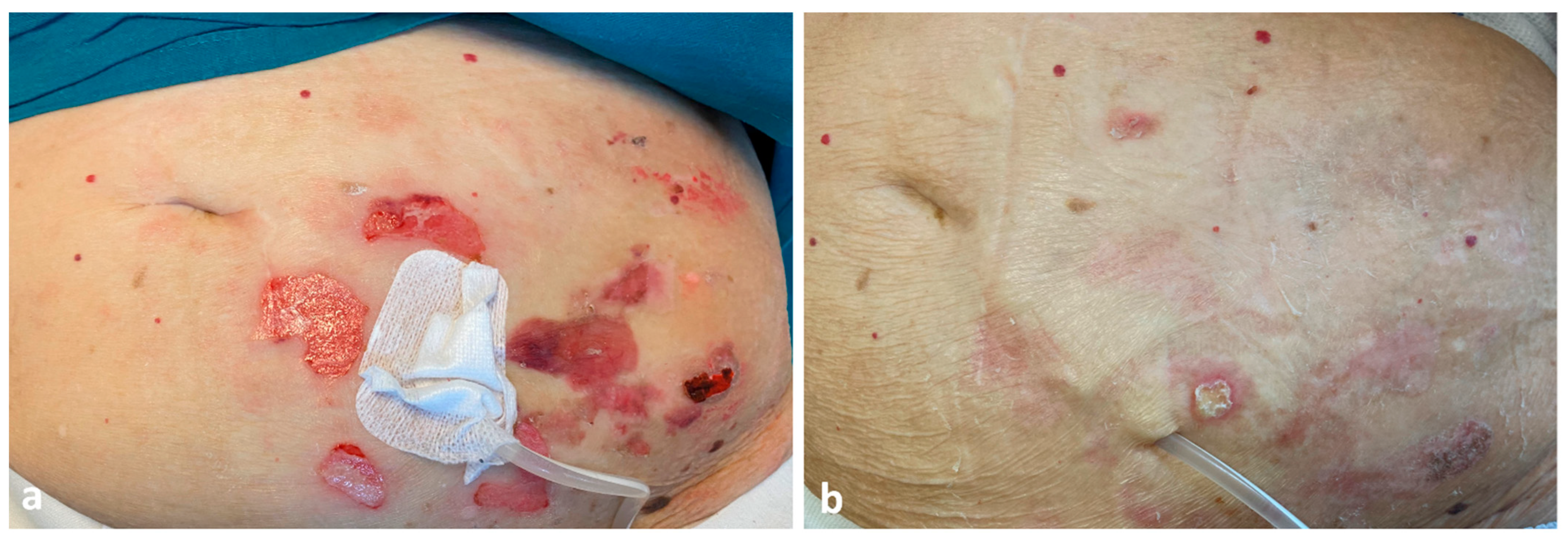
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ständer, S.; Kasperkiewicz, M.; Thaçi, D.; Schmidt, E.; Zillikens, D.; Vorobyev, A.; Ludwig, R.J. Prevalence and presumptive triggers of localized bullous pemphigoid. J. Dermatol. 2021, 48, 1257–1261. [Google Scholar] [CrossRef] [PubMed]
- Korman, N. Bullous pemphigoid. J. Am. Acad. Dermatol. 1987, 16, 907–924. [Google Scholar] [CrossRef]
- Nowsheen, S.; Wieland, C.N.; Camilleri, M.J.; Gibson, L.E.; Lehman, J.S. Peristomal pemphigoid: A single-center retrospective cohort study. J. Am. Acad. Dermatol. 2022, 86, 204–207. [Google Scholar] [CrossRef]
- Michelerio, A.; Croci, G.A.; Vassallo, C.; Brazzelli, V. Hemorrhagic vesiculobullous eruption on the palms and the soles as presentation of dyshidrosiform bullous pemphigoid. JAAD Case Rep. 2017, 4, 61–63. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Freeman, B.D.; Rubin, B.G. Bullous pemphigoid after prosthetic vascular graft placement. Surgery 1998, 124, 112–113. [Google Scholar] [CrossRef]
- Kamada, N.; Ino, N.; Hatamochi, A.; Shinkai, H. A case of bullous pemphigoid in a patient on hemodialysis. J. Dermatol. 1998, 25, 246–249. [Google Scholar] [CrossRef]
- Yesudian, P.D.; Dobson, C.M.; Ahmad, R.; Azurdia, R.M. Trauma-induced bullous pemphigoid around venous access site in a haemodialysis patient. Clin. Exp. Dermatol. 2002, 27, 70–72. [Google Scholar] [CrossRef]
- Pardo, J.; Rodríguez-Serna, M.; Mercader, P.; Fortea, J.M. Localized bullous pemphigoid overlying a fistula for hemodialysis. J. Am. Acad. Dermatol. 2004, 51, 131–132. [Google Scholar] [CrossRef] [PubMed]
- Peruzzo, J.; Dantas, L.D.P.; Zampese, M. Bullous pemphigoid associated with chronic renal allograft rejection. J. Am. Acad. Dermatol. 2013, 68, e192–e193. [Google Scholar] [CrossRef]
- Osipowicz, K.; Kalinska-Bienias, A.; Kowalewski, C.; Wozniak, K. Development of bullous pemphigoid during the haemodialysis of a young man: Case report and literature survey. Int. Wound J. 2017, 14, 288–292. [Google Scholar] [CrossRef]
- Giunzioni, D. Development of Bullous Pemphigoid after Tenckhoff Catheter Placement in a Peritoneal Dialysis Patient. Case Rep. Dermatol. 2020, 12, 42–46. [Google Scholar] [CrossRef]
- Anderson, C.; Mowad, C.; Goff, M.; Pelle, M. Bullous pemphigoid arising in surgical wounds. Br. J. Dermatol. 2001, 145, 670–672. [Google Scholar] [CrossRef]
- Biondo, M.; Fiorentino, C.; Persechino, S.; Tammaro, A.; Koverech, A.; Bartolazzi, A.; Raffa, S.; Canzoni, M.; Picchianti-Diamanti, A.; Di Rosa, R.; et al. May Bacterial Infections Trigger Bullous Pemphigoid? Case Report and Review of Literature. Microorganisms 2021, 9, 1235. [Google Scholar] [CrossRef] [PubMed]
- Bastuji-Garin, S.; Joly, P.; Picard-Dahan, C.; Bernard, P.; Vaillant, L.; Pauwels, C.; Salagnac, V.; Lok, C.; Roujeau, J.C. Drugs associated with bullous pemphigoid. A case-control study. Arch. Dermatol. 1996, 132, 272–276. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.G.; Lee, H.J.; Yoon, M.S.; Kim, D.H. Association of Dipeptidyl Peptidase 4 Inhibitor Use With Risk of Bullous Pemphigoid in Patients With Diabetes. JAMA Dermatol. 2019, 155, 172–177. [Google Scholar] [CrossRef]
- Liu, S.-D.; Chen, W.-T.; Chi, C.-C. Association Between Medication Use and Bullous Pemphigoid: A Systematic Review and Meta-analysis. JAMA Dermatol. 2020, 156, 891–900. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, R.; Haller, H.; Hiss, M. Quiz page september 2012: Erythematous rash around peritoneal dialysis catheter exit site. Am. J. Kidney Dis. 2012, 60, A29–A31. [Google Scholar] [CrossRef]
- McQuillan, R.F.; Chiu, E.; Nessim, S.; Lok, C.E.; Roscoe, J.M.; Tam, P.; Jassal, S.V. A randomized controlled trial comparing mupirocin and polysporin triple ointments in peritoneal dialysis patients: The MP3 Study. Clin. J. Am. Soc. Nephrol. 2012, 7, 297–303. [Google Scholar] [CrossRef]
- Yavascan, O.; Kara, O.D.; Sozen, G.; Aksu, N. Allergic dermatitis caused by povidone iodine: An uncommon complication of chronic peritoneal dialysis treatment. Adv. Perit. Dial. 2005, 21, 131–133. [Google Scholar]
- Piraino, B.; Bernardini, J.; Brown, E.; Figueiredo, A.E.; Johnson, D.; Lye, W.-C.; Price, V.; Ramalakshmi, S.; Szeto, C.C. ISPD position statement on reducing the risks of peritoneal dialysis–related infections. Perit. Dial. Int. 2011, 31, 614–630. [Google Scholar] [CrossRef]
- Patsatsi, A.; Uy, C.D.C.; Murrell, D.F. Multiple milia formation in blistering diseases. Int. J. Womens Dermatol. 2020, 6, 199–202. [Google Scholar] [CrossRef] [PubMed]
- Hisa, T.; Goto, Y.; Taniguchi, S.; Nakanishi, T.; Kakudo, K.; Takigawa, M. Post-bullous milia. Australas. J. Dermatol. 1996, 37, 153–154. [Google Scholar] [CrossRef] [PubMed]
- Uchida, S.; Oiso, N.; Koga, H.; Ishii, N.; Okahashi, K.; Matsuda, H.; Hashimoto, T.; Kawada, A. Refractory bullous pemphigoid leaving numerous milia during recovery. J. Dermatol. 2014, 41, 1003–1005. [Google Scholar] [CrossRef] [PubMed]
- Li, P.K.-T.; Chow, K.M.; Van de Luijtgaarden, M.W.; Johnson, D.W.; Jager, K.J.; Mehrotra, R.; Naicker, S.; Pecoits-Filho, R.; Yu, X.Q.; Lameire, N. Changes in the worldwide epidemiology of peritoneal dialysis. Nat. Rev. Nephrol. 2017, 13, 90–103. [Google Scholar] [CrossRef]
- Algoet, C.; Mostinckx, S.; Theate, I.; Vanhooteghem, O. Localized bullous pemphigoid: Four clinical cases and a literature review. Clin. Case Rep. 2020, 8, 516–519. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Michelerio, A.; Tomasini, C. Blisters and Milia around the Peritoneal Dialysis Catheter: A Case of Localized Bullous Pemphigoid. Dermatopathology 2022, 9, 282-286. https://doi.org/10.3390/dermatopathology9030033
Michelerio A, Tomasini C. Blisters and Milia around the Peritoneal Dialysis Catheter: A Case of Localized Bullous Pemphigoid. Dermatopathology. 2022; 9(3):282-286. https://doi.org/10.3390/dermatopathology9030033
Chicago/Turabian StyleMichelerio, Andrea, and Carlo Tomasini. 2022. "Blisters and Milia around the Peritoneal Dialysis Catheter: A Case of Localized Bullous Pemphigoid" Dermatopathology 9, no. 3: 282-286. https://doi.org/10.3390/dermatopathology9030033
APA StyleMichelerio, A., & Tomasini, C. (2022). Blisters and Milia around the Peritoneal Dialysis Catheter: A Case of Localized Bullous Pemphigoid. Dermatopathology, 9(3), 282-286. https://doi.org/10.3390/dermatopathology9030033