
A Case of IgG and IgA Anti-Laminin-332 Antibody-Positive Mucous Membrane Pemphigoid with IgG and IgA Anti-Envoplakin and Anti-Periplakin Antibodies

 , , , ,
, , , , {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
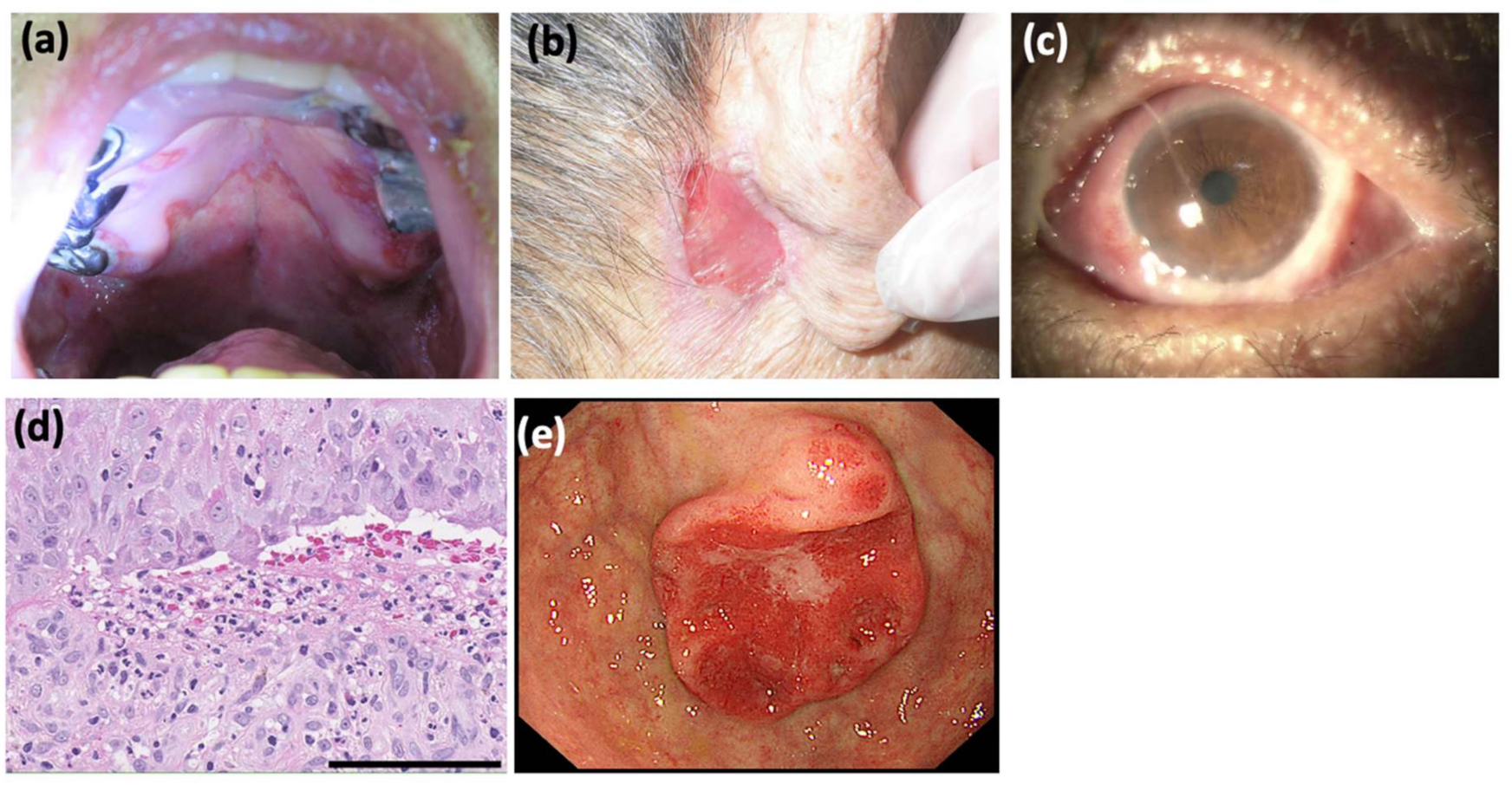
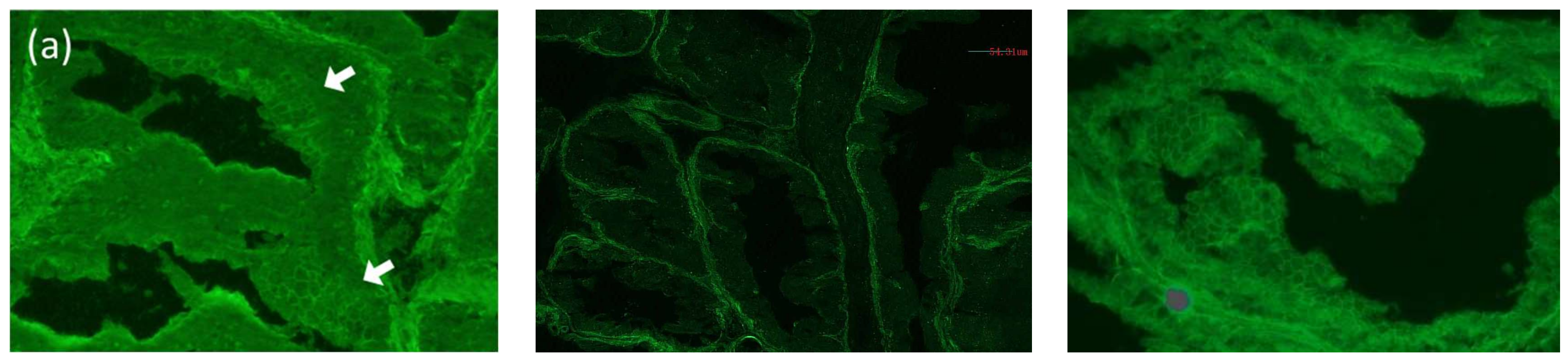
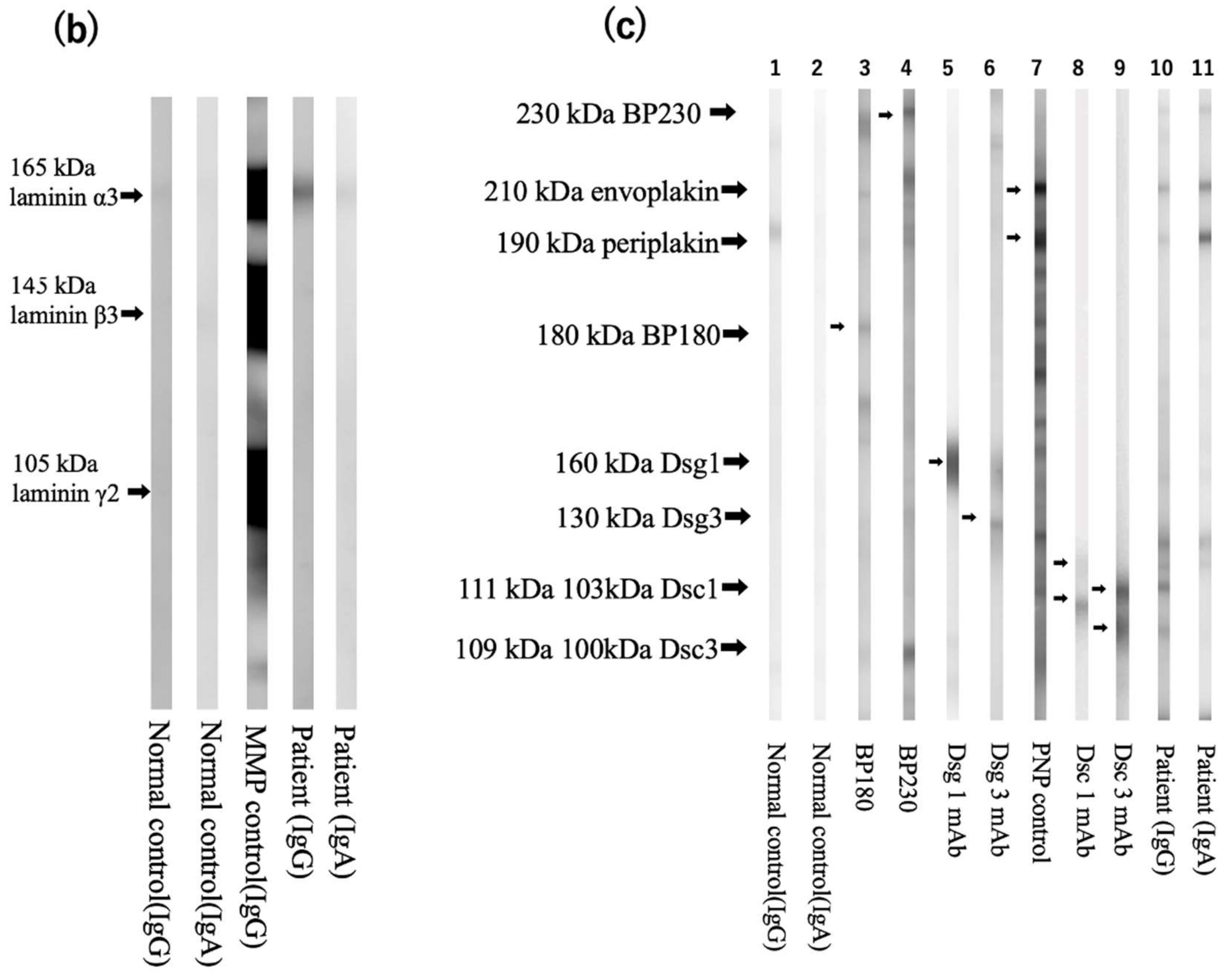
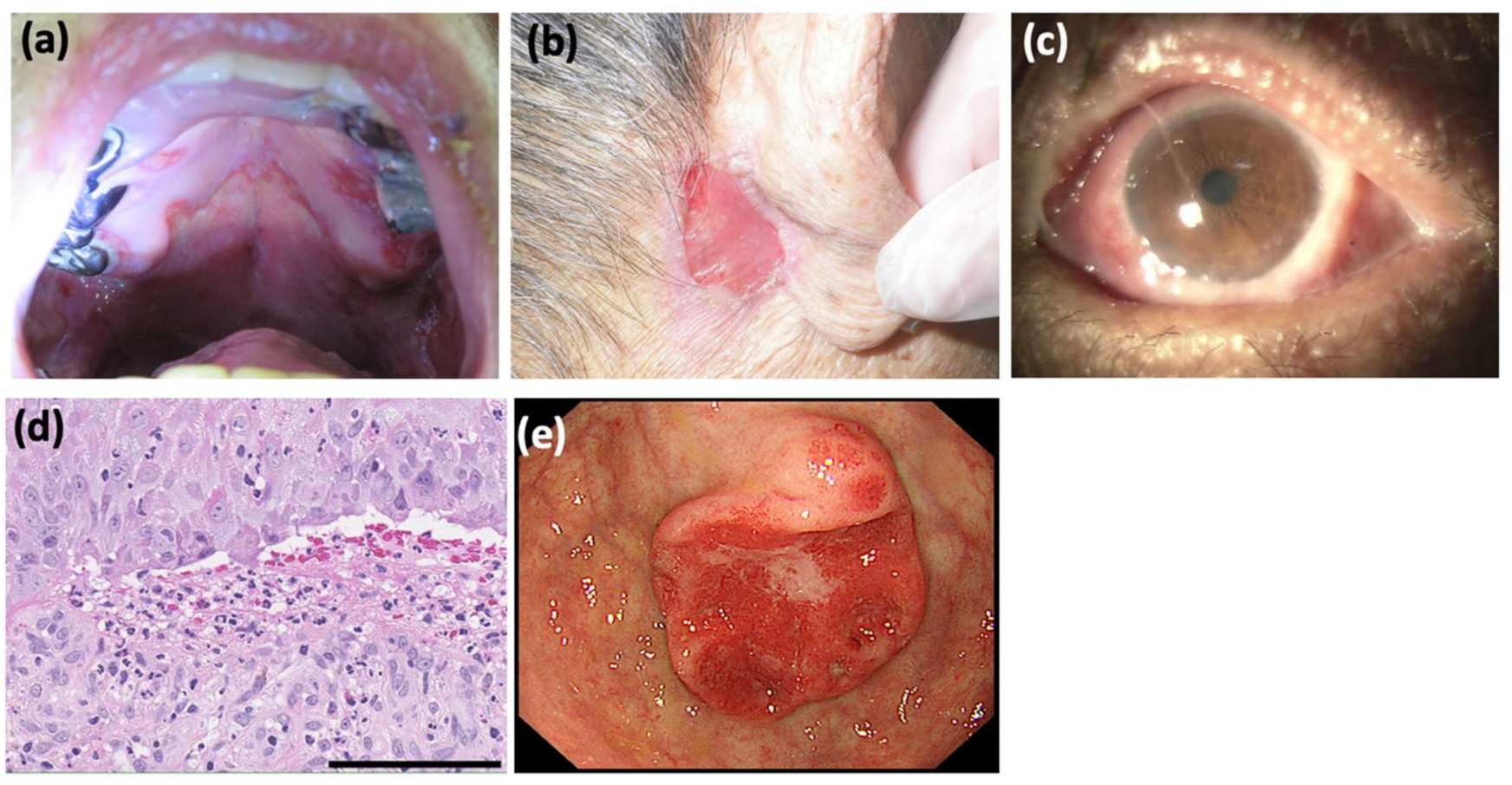
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Goletz, S.; Probst, C.; Komorowski, L.; Schlumberger, W.; Fechner, K.; van Beek, N.; Holtsche, M.M.; Recke, A.; Yancey, K.B.; Hashimoto, T.; et al. A sensitive and specific assay for the serological diagnosis of antilaminin 332 mucous membrane pemphigoid. Br. J. Dermatol. 2019, 180, 149–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayakawa, T.; Furumura, M.; Fukano, H.; Li, X.; Ishii, N.; Hamada, T.; Ohata, C.; Tsuruta, D.; Shimozato, K.; Hashimoto, T. Diagnosis of oral mucous membrane pemphigoid by means of combined serologic testing. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 117, 483–496. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Qian, H.; Natsuaki, Y.; Koga, H.; Kawakami, T.; Tateishi, C.; Tsuruta, D.; Ishii, N.; Hashimoto, T. Clinical and immunological findings in 55 patients with anti-laminin 332-type mucous membrane pemphigoid. Br. J. Dermatol. 2021, 185, 449–451. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, T.; Tsuruta, D.; Koga, H.; Fukuda, S.; Ohyama, B.; Komai, A.; Karashima, T.; Ohata, C.; Teye, K.; Ishii, N. Summary of results of serological tests and diagnoses for 4774 cases of various autoimmune bullous diseases consulted to Kurume University. Br. J. Dermatol. 2016, 175, 953–965. [Google Scholar] [CrossRef] [PubMed]
- Hisamatsu, Y.; Nishiyama, T.; Amano, S.; Matsui, C.; Ghohestani, R.; Hashimoto, T. Usefulness of immunoblotting using purified laminin 5 in the diagnosis of anti-laminin 5 cicatricial pemphigoid. J. Dermatol. Sci. 2003, 33, 113–119. [Google Scholar] [CrossRef]
- Ohzono, A.; Sogame, R.; Li, X.; Teye, K.; Tsuchisaka, A.; Numata, S.; Koga, H.; Kawakami, T.; Tsuruta, D.; Ishii, N.; et al. Clinical and immunological findings in 104 cases of paraneoplastic pemphigus. Br. J. Dermatol. 2015, 173, 1447–1452. [Google Scholar] [CrossRef] [PubMed]
- Allen, C.M.; Camisa, C. Paraneoplastic pemphigus: A review of the literature. Oral Dis. 2000, 6, 208–214. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsushima, Y.; Kitano, M.; Hayashi, D.; Goto, H.; Mine, M.; Yokoe, T.; Kondo, M.; Habe, K.; Toiyama, Y.; Hashimoto, T.; et al. A Case of IgG and IgA Anti-Laminin-332 Antibody-Positive Mucous Membrane Pemphigoid with IgG and IgA Anti-Envoplakin and Anti-Periplakin Antibodies. Dermatopathology 2022, 9, 287-291. https://doi.org/10.3390/dermatopathology9030034
Matsushima Y, Kitano M, Hayashi D, Goto H, Mine M, Yokoe T, Kondo M, Habe K, Toiyama Y, Hashimoto T, et al. A Case of IgG and IgA Anti-Laminin-332 Antibody-Positive Mucous Membrane Pemphigoid with IgG and IgA Anti-Envoplakin and Anti-Periplakin Antibodies. Dermatopathology. 2022; 9(3):287-291. https://doi.org/10.3390/dermatopathology9030034
Chicago/Turabian StyleMatsushima, Yoshiaki, Masako Kitano, Daisuke Hayashi, Hiroyuki Goto, Mako Mine, Takeshi Yokoe, Makoto Kondo, Koji Habe, Yuji Toiyama, Takashi Hashimoto, and et al. 2022. "A Case of IgG and IgA Anti-Laminin-332 Antibody-Positive Mucous Membrane Pemphigoid with IgG and IgA Anti-Envoplakin and Anti-Periplakin Antibodies" Dermatopathology 9, no. 3: 287-291. https://doi.org/10.3390/dermatopathology9030034
APA StyleMatsushima, Y., Kitano, M., Hayashi, D., Goto, H., Mine, M., Yokoe, T., Kondo, M., Habe, K., Toiyama, Y., Hashimoto, T., Tsuruta, D., Takeuchi, K., & Yamanaka, K. (2022). A Case of IgG and IgA Anti-Laminin-332 Antibody-Positive Mucous Membrane Pemphigoid with IgG and IgA Anti-Envoplakin and Anti-Periplakin Antibodies. Dermatopathology, 9(3), 287-291. https://doi.org/10.3390/dermatopathology9030034