
Dermatoscopic, Histological and Confocal Microscopic Analysis of a Kissing Nevus of the Penis


 , ,
, ,
Abstract
1. Introduction
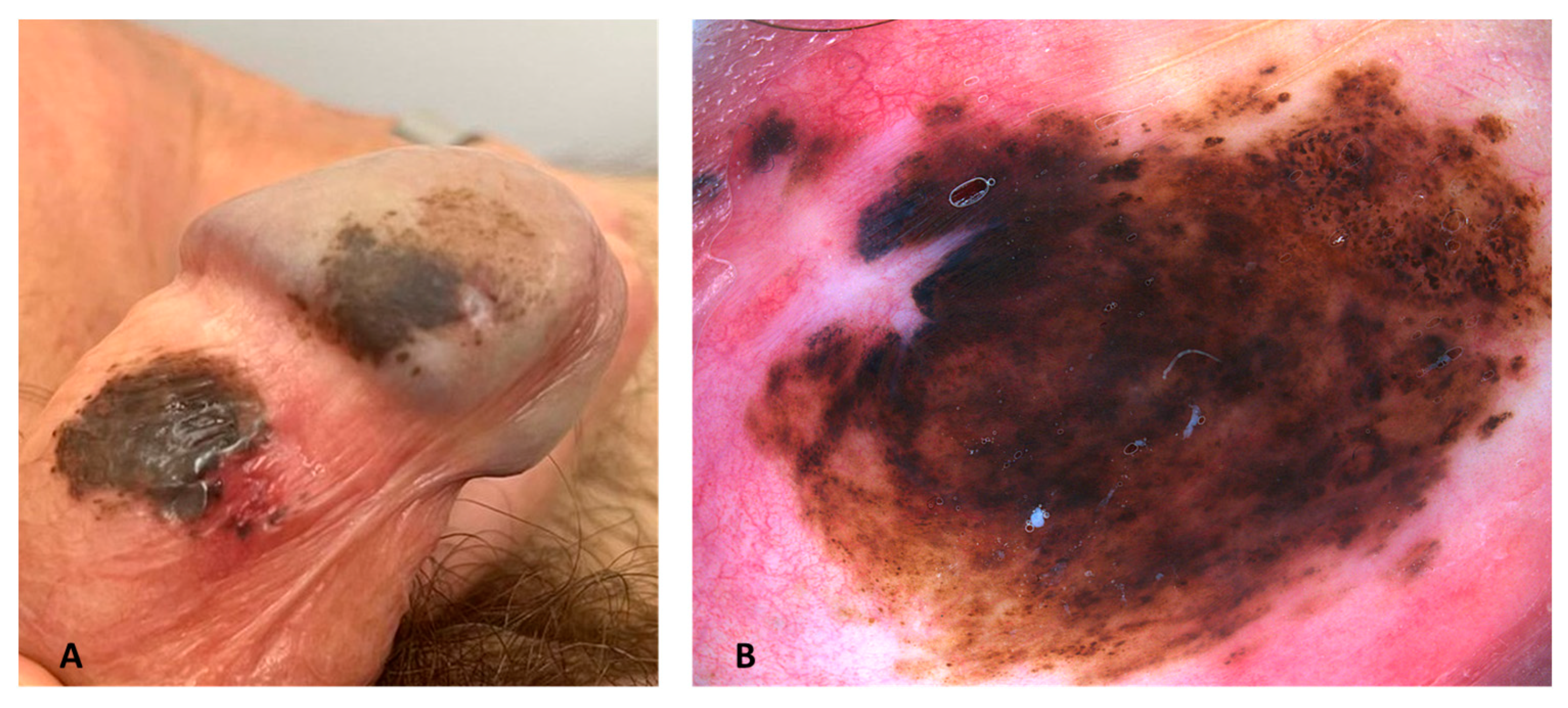
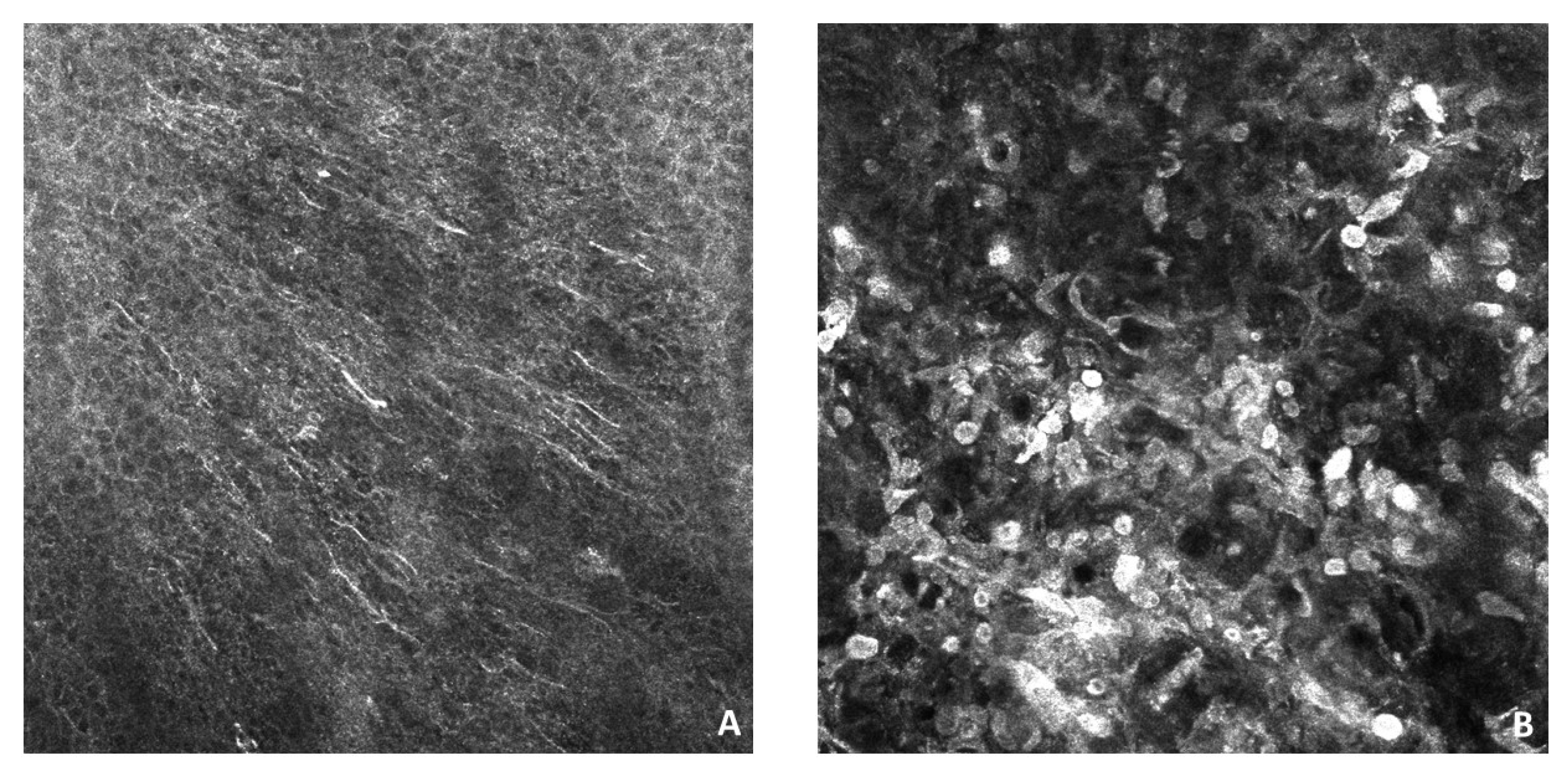
2. Case Report
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fuchs, A. Ueber geteilte naevi der augenlider. Klin. Mon. Augenheikd 1919, 63, 678–683. [Google Scholar]
- Sato, S.; Kato, H.; Hidano, A. Divided nevus spilus and divided form of spotted grouped pigmented nevus. J. Cutan. Pathol. 1979, 6, 507–512. [Google Scholar] [CrossRef]
- Niizawa, M.; Masahashi, T.; Maie, O.; Takahashi, S. A case of solitary mastocytoma suggesting a divided form of mast cell nevus. J. Dermatol. 1989, 16, 402–404. [Google Scholar] [CrossRef]
- Hayashi, N.; Soma, Y. A case of epidermal nevi showing a divided form on the fingers. J. Am. Acad. Dermatol. 1993, 29, 281–282. [Google Scholar]
- Phan, P.T.; Francis, N.; Madden, N.; Bunker, C.B. Kissing naevus of the penis. Clin. Exp. Dermatol. 2004, 29, 471–472. [Google Scholar] [CrossRef]
- Kono, T.; Nozaki, M.; Kikuchi, Y.; Erçöçe, A.R.; Hayashi, N.; Chan, H.H.L.; Ohkubo, R.; Fukaya, E. Divided naevus of the penis: A hypothesis on the embryological mechanism of its development. Acta Derm. Venereol. 2003, 83, 155–156. [Google Scholar] [CrossRef]
- Desruelles, F.; Lacour, J.P.; Mantoux, F.; Ortonne, J.P. Divided nevus of the penis: An unusual location. Arch. Dermatol. 1998, 134, 879–880. [Google Scholar] [CrossRef]
- Yun, S.J.; Wi, H.S.; Lee, J.B.; Kim, S.J.; Won, Y.H.; Lee, S.C. Kissing Nevus of the Penis. Ann. Dermatol. 2011, 23, 512–514. [Google Scholar] [CrossRef]
- Zhou, C.; Xu, H.; Zang, D.; Du, J.; Zhang, J. Divided nevus of the penis. Eur. J. Dermatol. 2010, 20, 527–528. [Google Scholar] [CrossRef]
- Higashida, Y.; Nagano, T.; Oka, M.; Nishigori, C. Divided naevus of the penis. Acta Derm. Venereol. 2010, 90, 319. [Google Scholar] [CrossRef]
- Palmer, B.; Hemphill, M.; Wootton, C.; Foshee, J.B.; Frimberger, D. Kissing nevus discovered at circumcision consult. J. Pediatr. Urol. 2010, 6, 318–319. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Zhou, M.; Qiao, J. Kissing nevus of the penis. Report of two cases and review of the literature. An. Bras. Dermatol. 2014, 89, 329. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.B.; Liu, T.; Zhang, Q.G.; Hu, J.T. Treatment of Divided Nevus of the Penis with Circumcision and Free Inner Prepuce Grafting. Plast. Reconstr. Surg. Glob. Open. 2015, 3, e389. [Google Scholar] [CrossRef]
- Hardin, C.A.; Tieu, K.D. Divided or kissing nevus of the penis. Derm. Online J. 2013, 19, 20027. [Google Scholar] [CrossRef]
- Choi, G.S.; Won, D.H.; Lee, S.J.; Lee, J.H.; Kim, Y.G. Divided naevus on the penis. Br. J. Dermatol. 2000, 143, 1126–1127. [Google Scholar] [CrossRef] [PubMed]
- Mendes, C.P.; Samorano, L.P.; Alessi, S.S.; Nico, M.M.S. Divided naevus of the penis: Two paediatric cases with dermoscopic findings. Clin. Exp. Dermatol. 2014, 39, 728–730. [Google Scholar] [CrossRef]
- Alves de Souza, N.G.; Nai, G.A.; Schaefer, A.L.F.; Schaefer, L.V. Kissing nevus of the penis: A case report and dermatoscopic findings. An. Bras. Dermatol. 2017, 92 (Suppl. S1), 95. [Google Scholar] [CrossRef]
- Egberts, F.; Egberts, J.H.; Schwarz, T.; Hauschild, A. Kissing melanoma or kissing nevus of the penis? Urology 2007, 69, e5–e384. [Google Scholar] [CrossRef]
- Savas, S.; Balı, Y.Y.; Erdemir, A.V.; Simsek, H. Divided nevus of the penis. Int. J. Dermatol. 2018, 57, 724–726. [Google Scholar] [CrossRef]
- Armengot-Carbó, M.; Rodrigo-Nicolás, B.; Botella-Estrada, R. Divided or kissing nevus of the penis: A new case with dermoscopic findings. Pediatr. Dermatol. 2018, 35, e321–e324. [Google Scholar] [CrossRef]
- Correia, B.; Duarte, A.F.; Haneke, E.; Correia, O. CO2 laser treatment of a kissing nevus of the penis: An alternative solution for a rare condition. J. Dermatolog Treat. 2021, 32, 120–123. [Google Scholar] [CrossRef] [PubMed]
- Guerra-Tapia, A.; Isarría, M.J. Periocular vitiligo with onset around a congenital divided nevus of the eyelid. Pediatr. Dermatol. 2005, 22, 427–429. [Google Scholar] [CrossRef]
- Spugnini, E.P.; Menicagli, F.; Giaconella, R.; Zanni, F.; Camponi, C.; De Luca, A.; Santoro, A.; Baldi, A. Filling the gap between histology and cytology: Description of an innovative technology (Cytomatrix) to increase the diagnostic effectiveness of fine needle aspirates data. J. Clin. Pathol. 2021, 74, 269–270. [Google Scholar] [CrossRef]
- Bonucci, M.; Minelli, S.; Castro, C.L.; Camponi, C.; Scimeca, M.; Scipioni, A.; Spugnini, E.P.; Baldi, A. Cytomatrix, a new procedure to enhance the diagnostic usefulness of fine needle aspirates. Ann. Res. Oncol. 2021, 1, 192–198. [Google Scholar] [CrossRef]
- Sood, N.; Mukherjee, M. Dermal Lymphatic Invasion: A Rare Feature in Benign Intradermal Nevus. Int. J. Appl. Basic. Med. Res. 2018, 8, 253–255. [Google Scholar] [CrossRef] [PubMed]
- Leblebici, C.; Kelten, C.; Gurel, M.S.; Hacıhasasanoglu, E. Intralymphatic nevus cells in benign nevi. Ann. Diagn. Pathol. 2016, 25, 1–6. [Google Scholar] [CrossRef]
- Bell, M.E.; Hill, D.P.; Bhargava, M.K. Lymphatic invasion in pigmented nevi. Am. J. Clin. Pathol. 1979, 72, 97–100. [Google Scholar] [CrossRef]
- Katsumata, M.; Matsunaga, T.; Maruyama, R.; Ezoe, K. Lymphatic invasion of nevus cells observed in intradermal nevus. J. Dermatol. 1990, 17, 264–265. [Google Scholar] [CrossRef]
- Howat, A.J.; Variend, S. Lymphatic invasion in Spitz nevi. Am. J. Surg. Pathol. 1985, 9, 125–128. [Google Scholar] [CrossRef]
- Demitsu, T.; Nagato, H.; Nishimaki, K.; Okada, O.; Kubota, T.; Yoneda, K.; Manabe, M. Melanoma in situ of the penis. J. Am. Acad. Dermatol. 2000, 42, 386–388. [Google Scholar] [CrossRef]
- Guiducci, L.; Kaleci, S.; Chester, J.; Longo, C.; Ciardo, S.; Farnetani, F.; Pellacani, G. Dendritic cells in reflectance confocal microscopy are a clue for early melanoma diagnosis in extrafacial flat pigmented melanocytic lesions. Exp. Dermatol. 2022, 31, 1048–1055. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Author | Age at the Diagnosis (y) | Dermoscopy | Histology |
|---|---|---|---|
| Mendes et al. [16] | 11 | Globular pattern: multiple pigment globules of different size | Compound melanocytic nevi |
| Alves de Souza et al. [17] | 9 | Compound pattern: fine pigmented network (periphery) and darkened globules of multiple size (center) | Compound melanocytic nevi |
| Savas et al. [19] | 3 | Globular pattern: scattered pigmented globules of varying size on a pigmented area with a pigmented center and dark periphery | Compound melanocytic nevi |
| Correia et al. [21] | 14 | Compound pattern: pigmented patch with dark dots and discrete annular-granular structures (prepuce) and a darker pigmented patch with greater density dark dots (glans) | Compound melanocytic nevi |
| Our case | 57 | Compound pattern: fine pigmented network (periphery) and darkened globules of multiple size (center) | Compound melanocytic nevi |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bianchi, A.; Baldi, A.; Farabini, A.; Nibid, L.; Roberti, V.; Pellacani, G.; Kazakov, D.V.; Donati, M. Dermatoscopic, Histological and Confocal Microscopic Analysis of a Kissing Nevus of the Penis. Dermatopathology 2023, 10, 147-152. https://doi.org/10.3390/dermatopathology10020022
Bianchi A, Baldi A, Farabini A, Nibid L, Roberti V, Pellacani G, Kazakov DV, Donati M. Dermatoscopic, Histological and Confocal Microscopic Analysis of a Kissing Nevus of the Penis. Dermatopathology. 2023; 10(2):147-152. https://doi.org/10.3390/dermatopathology10020022
Chicago/Turabian StyleBianchi, Alexander, Alfonso Baldi, Andrea Farabini, Lorenzo Nibid, Vincenzo Roberti, Giovanni Pellacani, Dmitry V. Kazakov, and Michele Donati. 2023. "Dermatoscopic, Histological and Confocal Microscopic Analysis of a Kissing Nevus of the Penis" Dermatopathology 10, no. 2: 147-152. https://doi.org/10.3390/dermatopathology10020022
APA StyleBianchi, A., Baldi, A., Farabini, A., Nibid, L., Roberti, V., Pellacani, G., Kazakov, D. V., & Donati, M. (2023). Dermatoscopic, Histological and Confocal Microscopic Analysis of a Kissing Nevus of the Penis. Dermatopathology, 10(2), 147-152. https://doi.org/10.3390/dermatopathology10020022