
Spiny Keratoderma in Association with Melanoma



{kind=link}
{kind=link}
Abstract
1. Introduction
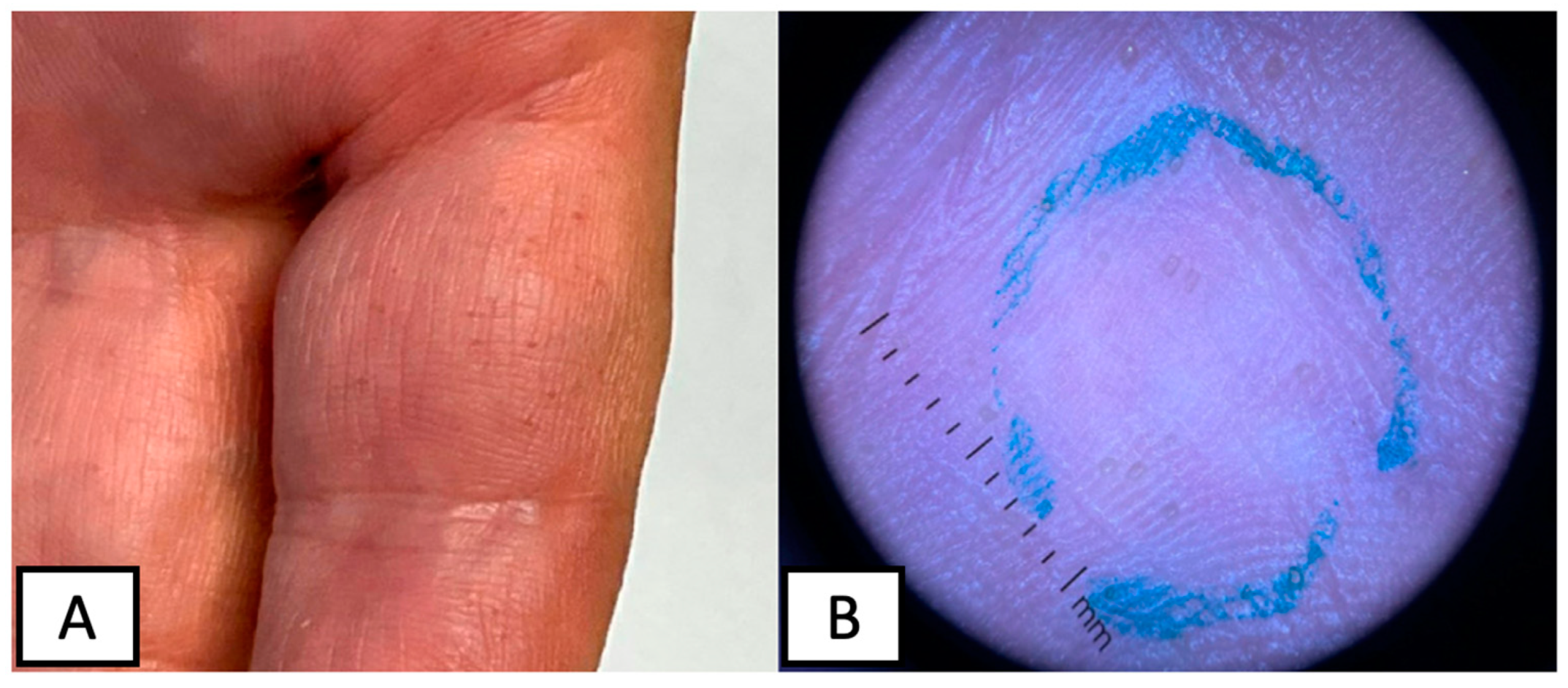
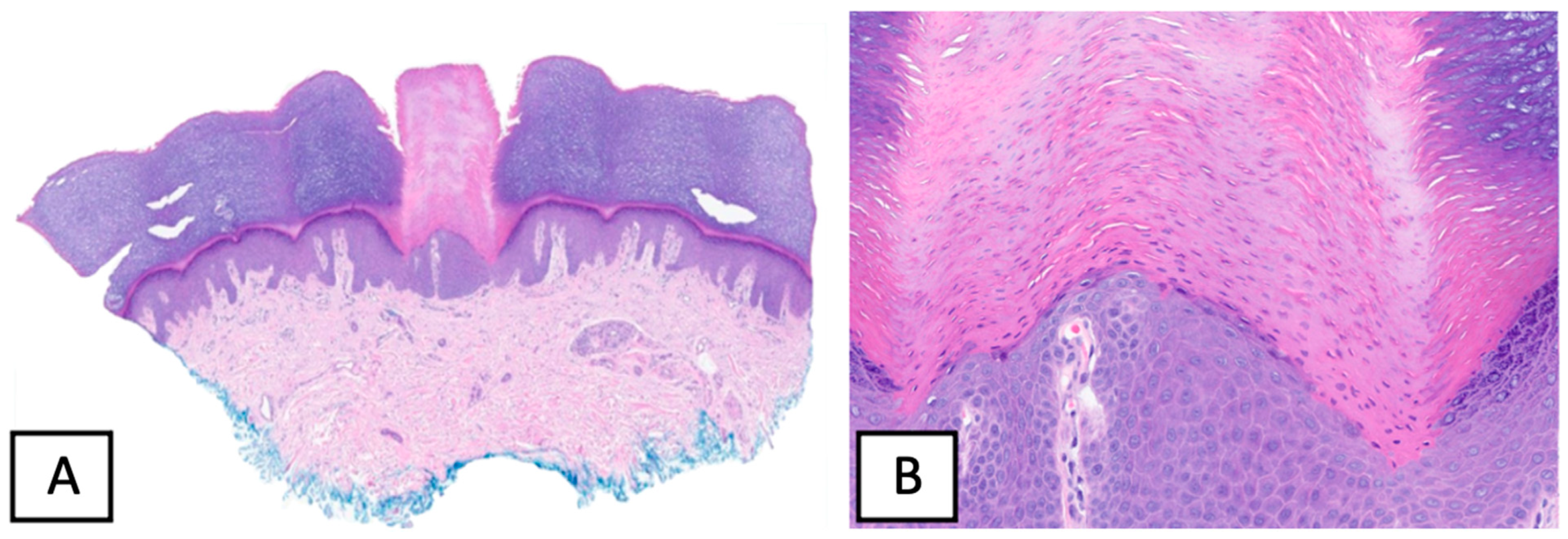
2. Case Presentation
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brown, F.C. Punctate keratoderma. Arch. Dermatol. 1971, 104, 682–683. [Google Scholar] [CrossRef] [PubMed]
- Osman, Y.; Daly, T.J.; Don, P.C. Spiny keratoderma of the palms and soles. J. Am. Acad. Dermatol. 1992, 26, 879–881. [Google Scholar] [CrossRef] [PubMed]
- Sakas, E.L.; Gentry, L.R.H. Porokeratosis punctata palmaris et plantaris (punctate porokeratosis): Case report and literature review. J. Am. Acad. Dermatol. 1985, 13, 908–912. [Google Scholar] [CrossRef] [PubMed]
- Roberts, L.C.; DeVillez, R.L. Congenital unilateral punctate porokeratosis. Am. J. Dermatopathol. 1984, 6, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Mehta, R.K.; Mallett, R.B.; Green, C.; Rytina, E. Palmar filiform hyperkeratosis (FH) associated with underlying pathology? Clin. Exp. Dermatol. 2002, 27, 216–219. [Google Scholar] [CrossRef] [PubMed]
- Poppe, H.; Kneitz, H.; Bröcker, E.-B.; Hamm, H. In situ melanoma and palmar spiny hyperkeratoses: Coincidence or paraneoplasia? Eur. J. Dermatol. 2012, 22, 281–282. [Google Scholar] [CrossRef]
- Kaddu, S.; Soyer, H.P.; Kerl, H. Palmar filiform hyperkeratosis: A new paraneoplastic syndrome? J. Am. Acad. Dermatol. 1995, 33, 337–340. [Google Scholar] [CrossRef]
- Caccetta, T.P.; Dessauvagie, B.; McCallum, D.; Kumarasinghe, S.P. Multiple minute digitate hyperkeratosis: A proposed algorithm for the digitate keratoses. J. Am. Acad. Dermatol. 2012, 67, e49–e55. [Google Scholar] [CrossRef]
- Nakamura, Y.; Muto, M. Spiny keratoderma of the palms in an insulin-treated diabetic patient. Int. J. Dermatol. 2013, 52, 1460–1461. [Google Scholar] [CrossRef]
- Handa, Y.; Sakakibara, A.; Araki, M.; Yamanaka, N. Spiny keratoderma of the palms and soles-report of two cases. Eur. J. Dermatol. 2000, 10, 542–545. [Google Scholar]
- Urbani, C.E.; Moneghini, L. Palmar spiny keratoderma associated with type IV hyperlipoproteinemia. J. Eur. Acad. Dermatol. Venereol. 1998, 10, 262–266. [Google Scholar] [CrossRef] [PubMed]
- Anderson, D.; Cohen, D.E.; Lee, H.S.; Thellman, C. Spiny keratoderma in association with autosomal dominant polycystic kidney disease with liver cysts. J. Am. Acad. Dermatol. 1996, 34, 935–936. [Google Scholar] [CrossRef] [PubMed]
- Salmon-Ehr, V.; Grosieux, C.; Derancourt, C.; Durlach, A.; Kalis, B.; Bernard, P. Palmoplantar filiform hyperkeratosis with Darier’s disease. Association or coincidence? Eur. J. Dermatol. 1998, 8, 519–520. [Google Scholar] [PubMed]
- Valverde, R.; Sánchez-Caminero, M.P.; Calzado, L.; de Frutos, F.J.O.; Rodríguez-Peralto, J.L.; Vanaclocha, F. Der-matomyositis and punctate porokeratotic keratoderma as paraneoplastic syndrome of ovarian carcinoma. Actas Dermosifiliogr. 2007, 98, 358–360. [Google Scholar] [CrossRef]
- Herman, P. Punctate Porokeratotic Keratoderma. Dermatology 1973, 147, 206–213. [Google Scholar] [CrossRef]
- Paul, C.; Fermand, J.-P.; Flageul, B.; Caux, F.; Duterque, M.; Dubertret, L.; Aractingi, S. Hyperkeratotic spicules and monoclonal gammopathy. J. Am. Acad. Dermatol. 1995, 33, 346–351. [Google Scholar] [CrossRef]
- Campbell, E.H.; Becknell, C. Spiny keratoderma exposes underlying renal cell carcinoma. JAAD Case Rep. 2018, 4, 382–383. [Google Scholar] [CrossRef]
- Hillion, B.; Le Bozec, P.; Moulonguet-Michau, I.; Blanchet-Bardon, C.; Petit, A.; Stephan, J.; Civatte, J. Filiform palmoplantar hyperkeratosis and cancer of the breast. Ann. Dermatol. Venereol. 1990, 117, 834–836. [Google Scholar]
- Beylot, C.; Taïeb, A.; Bioulac, P.; Doutre, M.S.; Foix, P. Filiform palmoplantar hyperkeratosis and visceral neoplasia. Ann. Dermatol. Venereol. 1982, 109, 747–748. [Google Scholar]
- Fegueux, S.; Bilet, S.; Crickx, B.; Perron, J.; Grossin, M.; Belaïch, S. Filiform palmar hyperkeratosis and rectosigmoid cancer. Ann. Dermatol. Venereol. 1988, 115, 1145–1146. [Google Scholar]
- Nazzaro, P.; Argentieri, R.; Balus, L.; Bassetti, F.; Fazio, M.; Giacalone, B.; Ponno, R. Paraneoplastic syndrome with papulo-keratosic lesions of the extremities and diffuse spinulose pilar ker-atosis. Ann. Dermatol. Syphiligr. 1974, 101, 411–413. [Google Scholar]
- Tomasini, C.; Michelerio, A.; Brazzelli, V. Eruptive ulcerative follicular spicules heralding progression of smoldering multiple myeloma. J. Cutan. Pathol. 2019, 46, 844–851. [Google Scholar] [CrossRef] [PubMed]
- Bork, K.; Böckers, M.; Pfeifle, J. Pathogenesis of Paraneoplastic Follicular Hyperkeratotic Spicules in Multiple Myeloma. Arch. Dermatol. 1990, 126, 509–513. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, L.; Orlandi, A.; Iraci, S.; Spagnoli, L.; Nini, G. Punctate porokeratotic keratoderma-its occurrence with internal neoplasia. Clin. Exp. Dermatol. 1994, 19, 139–141. [Google Scholar] [CrossRef] [PubMed]
- Kondo, S.; Shimoura, T.; Hozumi, Y.; Aso, K. Punctate porokeratotic keratoderma: Some pathogenetic analyses of hy-perproliferation and parakeratosis. Acta Derm. Venereol. 1990, 70, 478–482. [Google Scholar]
- Hashimoto, K.; Toi, Y.; Horton, S.; Sun, T.-T. Spiny keratoderma--a demonstration of hair keratin and hair type keratinization. J. Cutan. Pathol. 1999, 26, 25–30. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pukhalskaya, T.; Mully, T.W.; Wei, M.L. Spiny Keratoderma in Association with Melanoma. Dermatopathology 2023, 10, 142-146. https://doi.org/10.3390/dermatopathology10020021
Pukhalskaya T, Mully TW, Wei ML. Spiny Keratoderma in Association with Melanoma. Dermatopathology. 2023; 10(2):142-146. https://doi.org/10.3390/dermatopathology10020021
Chicago/Turabian StylePukhalskaya, Tatsiana, Thaddeus W. Mully, and Maria L. Wei. 2023. "Spiny Keratoderma in Association with Melanoma" Dermatopathology 10, no. 2: 142-146. https://doi.org/10.3390/dermatopathology10020021
APA StylePukhalskaya, T., Mully, T. W., & Wei, M. L. (2023). Spiny Keratoderma in Association with Melanoma. Dermatopathology, 10(2), 142-146. https://doi.org/10.3390/dermatopathology10020021