

Metabolic Adverse Effects of Psychotropic Drug Therapy: A Systematic Review

 and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Characteristics of the Studies
Selected Types of Studies
2.2. Participants
2.2.1. Types of Intervention
2.2.2. Types of Performance Measurement
2.3. Sources of Information
2.4. Search Strategy
2.5. Selection and Analysis
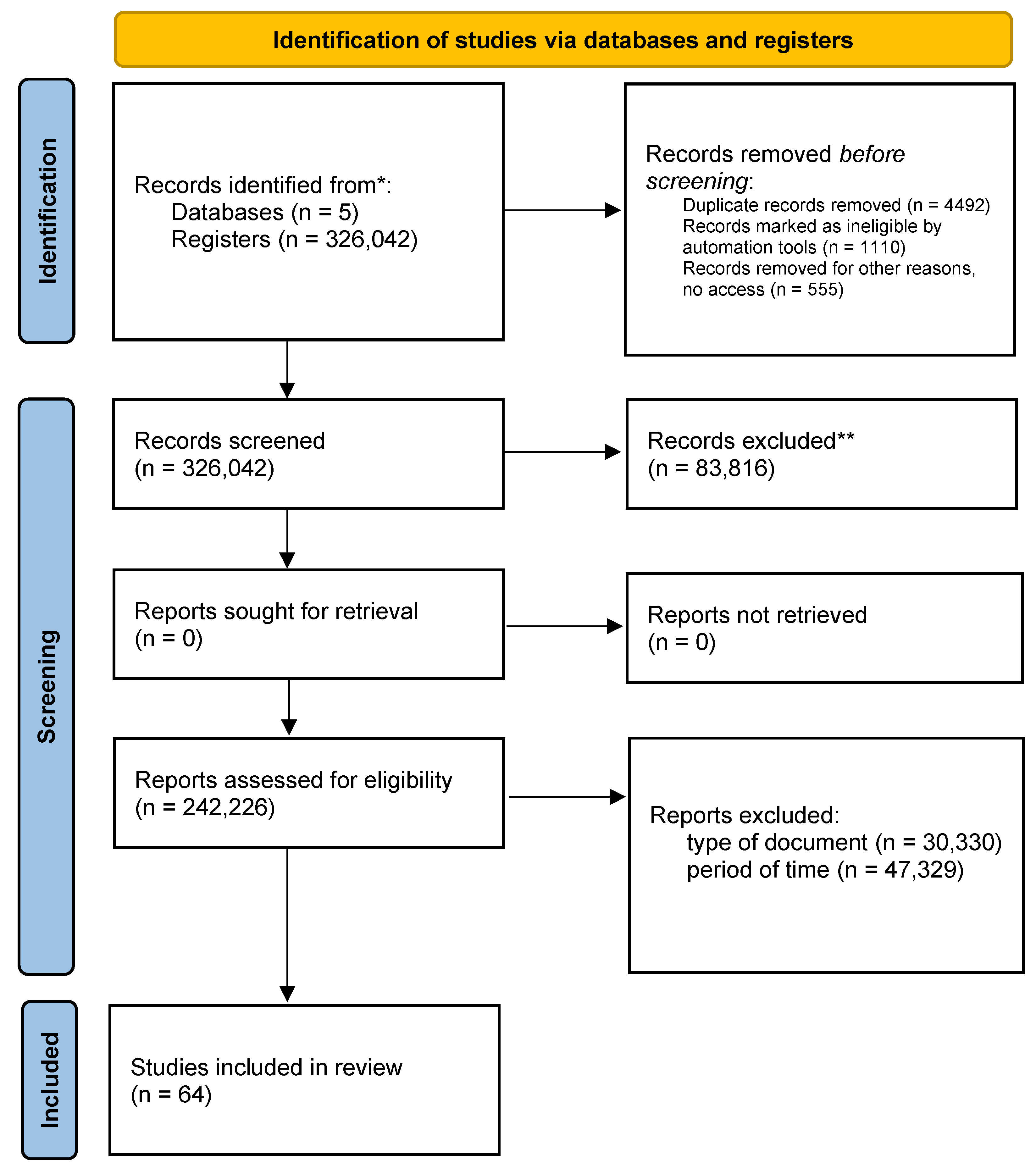
2.6. Inclusion Phase
3. Results

{kind=link}
| Ranking | Medication | Metabolic Change | Effect on the Patient |
|---|---|---|---|
| Antidepressants Tricyclics | Amitriptyline | Increased appetite by 19% [13]. Constipation 10% [14]. Weight gain of 10% [15]. Cardiovascular side effects 14% to 17% [14]. | 13.3% of patients with depression or anxiety who receive treatment with these psychotropic drugs for a period longer than 5 months’ notice significant changes in metabolism [13,15,16,17]. |
| Imipramine | Sedative effects [16]. Constipation 12%. Decreased blood pressure, dizziness 7% [14]. Metabolic risk 12% due to inappropriate drug metabolism [17]. | ||
| Clomipramine | Nausea, vomiting, intestinal flora alliteration and 12% to 17% body weight gain [18]. | ||
| Antidepressants (SSRIS) | Fluoxetine | Weight gain (6.8% Cardiac disturbance (12.5) [19]. Pulmonary hypertension in the fetus during gestation (1st to 20%) [20]. | 5.5% 21 to 25.5% of patients who are on selective serotonin reuptake inhibitors have a sedentary lifestyle and non-compliance with diets, which has as a consequence relevant change in their metabolism [20,21]. 38.4% (95% CI: 31.1–45.7) of patients on medication for more than six months report side effects [22]. Effects such as insomnia or hypersomnia due to citalopram consumption decrease in the second week, as long as the consumption of the drug is adequate to the medical order [21]. |
| Sertraline | Weight gain (7%), 0.8% constipation [22]. Gastrointestinal disorders 0.65% [23]. Metabolic disorders and nutritional alteration 0.45% [24]. | ||
| Citalopram | 4.6% Risk of postpartum hemorrhage [24]. | ||
| Escitalopram | 0.79% glycemic alteration in diabetics [24]. 1.7% risk of metabolic disturbance in patients with coronary heart disease [19]. 1 to 10% risk of metabolic disorders [25]. 16.9% to 22.9% risk of gastrointestinal disturbance [26]. | ||
| Paroxetine | 20–25% of digestive disorders [27]. 10–15% dry mouth and constipation [27,28]. |
| Ranking | Medication | Metabolic Change | Effect on the Patient |
|---|---|---|---|
| Anticonvulsant | Valproic acid | 12.89% Constipation [11,12]. 23.4% Weight gain [11,12]. Appetite and sleep changes [11]. | 100% of patients with diabetes, and hypertension, should not receive treatment with Fosphenytoin. |
| Fosphenytoin | 79% BMI alteration. 56% increase in abdominal obesity [11,28]. |
| Ranking | Medication | Metabolic Change | Effect on the Patient |
|---|---|---|---|
| Anti-psychotics | Clozapine | 13.8% weight gain [31]. 2.10% risk of diabetes [30]. 00.24% deterioration lipid profile [33,34]. 34% prevalence of metabolic side effects [33]. Withdrawal dyskinesias, increased prolactin levels, weight gain, and other metabolic abnormalities [32,33]. | 12.4% of patients reported significant weight gain, reporting an increase of 4.45 kg after 10 weeks of treatment. Patients under 16 years of age are at increased risk of metabolic derangement caused by clozapine use [32,33]. |
| Olanzapine | 13.8% weight gain. 2.10% risk of diabetes. 02.4% deterioration of lipid profile [35]. 12.9% Alteration of glucose metabolism. 0.97% Alteration of lipid metabolism. | 12.4% of patients reported significant changes in weight gain, reporting an increase of 4.45 kg after 10 weeks of treatment [35]. | |
| Risperidone | 12.9% alteration of glucose metabolism. 07% weight gain [35]. 25% diabetes [36]. 19.3% lipid alteration [37]. | 12.4% of patients reported significant changes in weight gain, reporting an increase of 4.45 kg after 10 weeks of treatment [35]. | |
| Zipracidone | Weight gain (7%). 34% prevalence of metabolic side effects [33]. 19.3% lipid alteration [37]. | 30% of the patients present changes in metabolism showing that the weight gain in the controls varies between 2.34 kg and 4.51 kg. | |
| Quetiapine | 16% weight gain [38]. 19% blood pressure [39]. 19.3% lipid alteration (varies according to drug dose) [39]. | 16% of the patients presented changes in metabolism showing that the weight gain in the controls varied between 2.34 kg and 4.51 kg after one year and six months of treatment [39,40]. | |
| Zipracidone | 7% weight gain [41]. 12% blood pressure [41]. 2.7% alteration of lipid and glycemic parameters [41]. Clinically significant metabolic alterations [41,42]. 23.2% hypercholesterolemia [41]. 1.7% hypertriglyceridemia [41]. | In 37.6% of patients treated with Zipracidone, the symptoms occur during the first year of treatment [41]. 19% of the patients at the 12th and 24th week of treatment report changes [41]. Tests and major alterations in metabolism [42]. 3 years after a psychotic episode, patients show an increase in BMI [37,42]. | |
| Perfenazine | 19.3% lipid alteration [37,42]. |
| Alterations in Mental Health | Metabolism |
|---|---|
| Depression Mood disorders | This is an alteration associated with metabolic syndrome, relating comorbidity with diabetes mellitus type 2 and cardiovascular disorders [43]. Direct relationship between physical and metabolic alterations, the stress regulatory system and the appetite activator, caused by the body’s energy deficiency in the major depressive disorder due to imbalance of the hypothalamus-pituitary-adrenal gland, the concentration of hormones, and appetite [33,55]. |
| Schizophrenia Psychotic disorders | Comorbidity of a psychotic disorder with metabolic alterations, hypertension, and cardiovascular risk; within the investigations, the need to follow up on the group of medications that the patient is taking arises [56]. |
| Autism | Decreased levels of oxytocin; this disorder is characterized by the presence of inborn errors in metabolism [12]. |
| Bipolar disorder | The patient presents an elevated glucose metabolism in the amygdala [57]. However, exposure to stressful situations and excessive consumption of sugars and fats produces a high risk of suffering alterations such as obesity, hypertension, and other disorders [58]. |
| Eating behavior disorder | Food is the basis for the development of energy. If the organism presents alterations in eating behavior, whether caused by disorders such as anorexia or bulimia, the processing of enzymes and micronutrients is not optimal [47,58,59]. |
| Sleep disturbances | Just as nutrition is important, rest is vital for the process of growth and protein generation, altering the sleep cycle generates the risk of metabolic alterations [34,60,61,62]. |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rojas, E.; Castro, A.; Manzano, A.; Suárez, M.K.; Lameda, V.; Carrasquero, R.; Nava, M.; Bermúdez, V. Diagnostic Criteria and Management of Metabolic Syndrome: Evolution Overtime. Gac. Medica Caracas 2021, 128, 480–504. [Google Scholar] [CrossRef]
- Moreira, F.P.; Jansen, K.; Cardoso, T.D.A.; Mondin, T.C.; Magalhães, P.V.; Kapczinski, F.; Souza, L.D.M.; da Silva, R.A.; Oses, J.P.; Wiener, C.D. Metabolic Syndrome and Psychiatric Disorders: A Population-Based Study. Rev. Bras. Psiquiatr. 2019, 41, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Tubbs, A.S.; Khader, W.; Fernandez, F.; Grandner, M.A. The Common Denominators of Sleep, Obesity, and Psychopathology. Curr. Opin. Psychol. 2020, 34, 84–88. [Google Scholar] [CrossRef]
- Sugai, T.; Suzuki, Y.; Yamazaki, M.; Shimoda, K.; Mori, T.; Ozeki, Y.; Matsuda, H.; Sugawara, N.; Yasui-Furukori, N.; Minami, Y.; et al. High Prevalence of Obesity, Hypertension, Hyperlipidemia, and Diabetes Mellitus in Japanese Outpatients with Schizophrenia: A Nationwide Survey. PLoS ONE 2016, 11, e0166429. [Google Scholar] [CrossRef]
- Zimmet, P.; Alberti, K.G.M.M.; Shaw, J. Global and Societal Implications of the Diabetes Epidemic. Nature 2001, 414, 782–787. [Google Scholar] [CrossRef] [PubMed]
- Domecq, J.P.; Prutsky, G.; Leppin, A.; Sonbol, M.B.; Altayar, O.; Undavalli, C.; Wang, Z.; Elraiyah, T.; Brito, J.P.; Mauck, K.F.; et al. Drugs Commonly Associated with Weight Change: A Systematic Review and Meta-Analysis. J. Clin. Endocrinol. Metab. 2015, 100, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.H.; Lee, D.K.; Liu, M.; Portincasa, P.; Wang, D.Q.H. Novel Insights into the Pathogenesis and Management of the Metabolic Syndrome. Pediatr. Gastroenterol. Hepatol. Nutr. 2015, 23, 189. [Google Scholar] [CrossRef] [PubMed]
- Núñez-Cortés, J.M.; Mantilla Morató, T.; Toro, R.; Millán Pérez, J.; Mangas Rojas, A.; Ascaso, J.; Civeira, F.; Mostaza, J.M.; Pintó, X.; Valdivielso, P. Metabolic Syndrome in Patients with Clinical Phenotype “Hypertriglyceridemic Waist”. Nutr. Hosp. 2015, 241, e172. [Google Scholar] [CrossRef]
- Abosi, O.; Lopes, S.; Schmitz, S.; Fiedorowicz, J.G. Cardiometabolic Effects of Psychotropic Medications. Horm. Mol. Biol. Clin. Investig. Gruyter 2018, 36. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Rakitin, A.; Eglit, T.; Kõks, S.; Lember, M.; Haldre, S. Comparison of the Metabolic Syndrome Risk in Valproate-Treated Patients with Epilepsy and the General Population in Estonia. PLoS ONE 2014, 9, e103856. [Google Scholar] [CrossRef]
- Delacrétaz, A.; Glatard, A.; Dubath, C.; Gholam, M.; Gamma, F.; von Gunten, A.; Conus, P.; Eap, C.B. Valproate Is Associated with Early Decrease of High-Density Lipoprotein Cholesterol Levels in the Psychiatric Population. Basic. Clin. Pharmacol. Toxicol. 2021, 129, 26–35. [Google Scholar] [CrossRef]
- Gomis, R. Presentation: The Threat of Metabolic Change. Span. J. Cardiol. 2008, 8 (Suppl. SC), 1. [Google Scholar] [CrossRef]
- Steffens, D.C.; Wei, J.; Krishnan, K.R.R.; Karoly, E.D.; Mitchell, M.W.; O’Connor, C.M.; Kaddurah-Daouk, R. Metabolomic Differences in Heart Failure Patients with and without Major Depression. J. Geriatr. Psychiatry Neurol. 2010, 23, 138–146. [Google Scholar] [CrossRef] [PubMed]
- Rajjo, T.; Mohammed, K.; Alsawas, M.; Ahmed, A.T.; Farah, W.; Asi, N.; Almasri, J.; Prokop, L.J.; Murad, M.H. Treatment of Pediatric Obesity: An Umbrella Systematic Review. J. Clin. Endocrinol. Metab. 2017, 102, 763–775. [Google Scholar] [CrossRef] [PubMed]
- de San, H.; de Bogotá, J.; Septiembre, D.C.; Jerónimo, C.; Sánchez, V.; Pablo, J.; Chacón, M.; Tovar Cortés, H.; De, H.; José, S.; et al. Prevalence of metabolic syndrome in patients attending the internal medicine outpatient clinic. Rev. Repert. Med. Y Cirugía 2011, 20, 93–102. [Google Scholar]
- Alalwan, A.A.; Friedman, J.; Alfayez, O.; Hartzema, A. Drug Absorption in Bariatric Surgery Patients: A Narrative Review. Health Sci. Rep. 2022, 5, e605. [Google Scholar] [CrossRef] [PubMed]
- Hinnouho, G.M.; Singh-Manoux, A.; Gueguen, A.; Matta, J.; Lemogne, C.; Goldberg, M.; Zins, M.; Czernichow, S. Metabolically Healthy Obesity and Depressive Symptoms: 16-Year Follow-up of the Gazel Cohort Study. PLoS ONE 2017, 12, e0174678. [Google Scholar] [CrossRef]
- Piña, I.L.; di Palo, K.E.; Ventura, H.O. Psychopharmacology and Cardiovascular Disease. J. Am. Coll. Cardiol. 2018, 71, 2346–2359. [Google Scholar] [CrossRef]
- Chen, J.; Yang, Y.; Yu, N.; Sun, W.; Yang, Y.; Zhao, M. Relationship between Gut Microbiome Characteristics and the Effect of Nutritional Therapy on Glycemic Control in Pregnant Women with Gestational Diabetes Mellitus. PLoS ONE 2022, 17, e0267045. [Google Scholar] [CrossRef] [PubMed]
- Laaboub, N.; Dubath, C.; Ranjbar, S.; Sibailly, G.; Grosu, C.; Piras, M.; Délessert, D.; Richard-Lepouriel, H.; Ansermot, N.; Crettol, S.; et al. Insomnia Disorders Are Associated with Increased Cardiometabolic Disturbances and Death Risks from Cardiovascular Diseases in Psychiatric Patients Treated with Weight-Gain-Inducing Psychotropic Drugs: Results from a Swiss Cohort. BMC Psychiatry 2022, 22, 342. [Google Scholar] [CrossRef]
- Wolff, J.; Reißner, P.; Hefner, G.; Normann, C.; Kaier, K.; Binder, H.; Hiemke, C.; Toto, S.; Domschke, K.; Marschollek, M.; et al. Pharmacotherapy, Drug-Drug Interactions and Potentially Inappropriate Medication in Depressive Disorders. PLoS ONE 2021, 16, e0255192. [Google Scholar] [CrossRef] [PubMed]
- Ulrich, S.; Ricken, R.; Adli, M. Tranylcypromine in Mind (Part I): Review of Pharmacology. Eur. Neuropsychopharmacol. 2017, 27, 697–713. [Google Scholar] [CrossRef] [PubMed]
- Párraga Martínez, I.; López-Torres Hidalgo, J.; Del Campo, J.M.; Villena Ferrer, A.; Morena Rayo, S.; Escobar Rabadán, F. Monitoring Adherence to Antidepressant Treatment in Patients Initiating Antidepressant Treatment. Aten. Primaria 2014, 46, 357–366. [Google Scholar] [CrossRef] [PubMed]
- Morriss, R.; Tyrer, F.; Zaccardi, F.; Khunti, K. Safety of Anti-depressants in a Primary Care Cohort of Adults with Obesity and Depression. PLoS ONE 2021, 16, e0245722. [Google Scholar] [CrossRef] [PubMed]
- Pagán-Busigó, J.E.; López-Carrasquillo, J.; Appleyard, C.B.; Torres-Reverón, A. Beyond Depression and Anxiety; a Systematic Review about the Role of Corticotropin-Releasing Hormone Antagonists in Diseases of the Pelvic and Abdominal Organs. PLoS ONE 2022, 17, e0264909. [Google Scholar] [CrossRef]
- Criado, K.K.; Sharp, W.G.; McCracken, C.E.; de Vinck-Baroody, O.; Dong, L.; Aman, M.G.; McDougle, C.J.; McCracken, J.T.; Eugene Arnold, L.; Weitzman, C.; et al. Overweight and Obese Status in Children with Autism Spectrum Disorder and Disruptive Behavior. Autism 2018, 22, 450–459. [Google Scholar] [CrossRef]
- Khuda, I.E.; Nazish, S.; Zeeshan, M.A.; Shariff, E.; Aljaafari, D.; Alabdali, M. It Is Illegal to Post This Copyrighted PDF on Any Website. Non-HDL Cholesterol, Obesity, and Metabolic Syndrome in Epileptic Patients. Prim. Care Companion J. Clin. Psychiatry 2022, 24, e1–e6. [Google Scholar] [CrossRef]
- Dalvi-Garcia, F.; Fonseca, L.L.; Vasoncelos, A.T.R.; Pereira, C.H.; Voit, E.O. A Model of Dopamine and Serotonin-Kynurenine Metabolism in Cortisolemia: Implications for Depression. PLoS Comput. Biol. 2021, 17, e1008956. [Google Scholar] [CrossRef]
- Correll, C.U.; Agid, O.; Crespo-Facorro, B.; de Bartolomeis, A.; Fagiolini, A.; Seppälä, N.; Howes, O.D. A Guideline and Checklist for Initiating and Managing Clozapine Treatment in Patients with Treatment-Resistant Schizophrenia. CNS Drugs 2022, 36, 659–679. [Google Scholar] [CrossRef]
- Suetani, R.J.; Siskind, D.; Reichhold, H.; Kisely, S. Genetic Variants Impacting Metabolic Outcomes among People on Clozapine: A Systematic Review and Meta-Analysis. Psychopharmacology 2017, 234, 2989–3008. [Google Scholar] [CrossRef]
- Simon, M.S.; Barton, B.B.; Glocker, C.; Musil, R. A Comprehensive Approach to Predicting Weight Gain and Therapy Response in Psychopharmacologically Treated Major Depressed Patients: A Cohort Study Protocol. PLoS ONE 2022, 17, e0271793. [Google Scholar] [CrossRef] [PubMed]
- Vasudev, K.; Choi, Y.H.; Norman, R.; Kim, R.B.; Schwarz, U.I. Genetic Determinants of Clozapine-Induced Metabolic Side Effects. Can. J. Psychiatry 2017, 62, 138–149. [Google Scholar] [CrossRef]
- Siskind, D.J.; Leung, J.; Russell, A.W.; Wysoczanski, D.; Kisely, S. Metformin for Clozapine Associated Obesity: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0156208. [Google Scholar] [CrossRef]
- Ciencia, C.; Médico, E. Weight Gain and Metabolic Change with Predictors of Symptom Improvement in Patients with First Episode Schizophrenia Spectrum Disorder Treated for 12 Months. Schizophr. Res. 2019, 206, 171–176. [Google Scholar] [CrossRef]
- Liu, Y.K.; Ling, S.; Lui, L.M.W.; Ceban, F.; Vinberg, M.; Kessing, L.V.; Ho, R.C.; Rhee, T.G.; Gill, H.; Cao, B.; et al. Prevalence of Type 2 Diabetes Mellitus, Impaired Fasting Glucose, General Obesity, and Abdominal Obesity in Patients with Bipolar Disorder: A Systematic Review and Meta-Analysis. J. Affect. Disord. 2022, 300, 449–461. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, E.; Govind, R.; Romero, A.; Dzahini, O.; Broadbent, M.; Stewart, R.; Smith, T.; Kim, C.H.; Werbeloff, N.; MacCabe, J.H.; et al. The Side Effect Profile of Clozapine in Real World Data of Three Large Mental Health Hospitals. PLoS ONE 2020, 15, e0243437. [Google Scholar] [CrossRef] [PubMed]
- Steuer, A.E.; Schmidhauser, C.; Tingelhoff, E.H.; Schmid, Y.; Rickli, A.; Kraemer, T.; Liechti, M.E. Impact of Cytochrome P450 2D6 Function on the Chiral Blood Plasma Pharmacokinetics of 3,4-Methylenedioxymethamphetamine (MDMA) and Its Phase I and II Metabolites in Humans. PLoS ONE 2016, 11, e0150955. [Google Scholar] [CrossRef]
- Vázquez-Bourgon, J.; Gómez-Revuelta, M.; Mayoral-van Son, J.; Labad, J.; Ortiz-García de la Foz, V.; Setién-Suero, E.; Ayesa-Arriola, R.; Tordesillas-Gutiérrez, D.; Juncal-Ruiz, M.; Crespo-Facorro, B. Pattern of Long-Term Weight and Metabolic Changes after a First Episode of Psychosis: Results from a 10-Year Prospective Follow-up of the PAFIP Program for Early Intervention in Psychosis Cohort. Eur. Psychiatry 2022, 65, E48. [Google Scholar] [CrossRef]
- Pinzón, J.B.; Serrano, N.C.; Díaz, L.A. Impact of the new definitions in the prevalence of the metabolic syndrome in an adult population at Bucaramanga, Colombia. Biomedica 2007, 27, 172–179. [Google Scholar] [CrossRef]
- Vázquez-Bourgon, J.; Ibáñez Alario, M.; Mayoral-van Son, J.; Gómez Revuelta, M.; Ayesa Arriola, R.; Juncal Ruiz, M.; Ortiz-García de la Foz, V.; Crespo Facorro, B. A 3-Year Prospective Study on the Metabolic Effect of Aripiprazole, Quetiapine and Ziprasidone: A Pragmatic Clinical Trial in First Episode Psychosis Patients. Eur. Neuropsychopharmacol. 2020, 39, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Revuelta, M.; Pelayo-Terán, J.M.; Juncal-Ruiz, M.; Ortiz-García de la Foz, V.; Vázquez-Bourgon, J.; González-Pinto, A.; Crespo-Facorro, B. Long-Term Antipsychotic Effectiveness in First Episode of Psychosis: A 3-Year Follow-up Randomized Clinical Trial Comparing Aripiprazole, Quetiapine, and Ziprasidone. Int. J. Neuropsychopharmacol. 2018, 21, 1090–1101. [Google Scholar] [CrossRef]
- Kahl, K.; Lampen-Inkamp, S.; Claassen, B.; Peschel, T.; Schik, G. E.05.02 Metabolic Alterations and Their Background in Patients with Affective Disorders. Eur. Neuropsychopharmacol. 2010, 20, S211. [Google Scholar] [CrossRef]
- Fernández-Aranda, F.; Sauchelli, S.; Pastor, A.; Gonzalez, M.L.; de La Torre, R.; Granero, R.; Jiménez-Murcia, S.; Baños, R.; Botella, C.; Fernández-Real, J.M.; et al. Moderate-Vigorous Physical Activity across Body Mass Index in Females: Moderating Effect of Endocannabinoids and Temperament. PLoS ONE 2014, 9, e104534. [Google Scholar] [CrossRef] [PubMed]
- Castillo Hernández, J.L.; Cuevas González, M.J.; Galiana, M.A.; Romero Hernández, E. Metabolic syndrome, a public health problem with different definitions and criteria. Rev. Médica Univ. Veracruzana 2017, 17, 7–14. [Google Scholar]
- Garmendia Lorena, F. Metabolic Syndrome, Artifice or Reality? Ann. Fac. Med. 2020, 81, 92–98. [Google Scholar] [CrossRef]
- Tabatabaei-Malazy, O.; Moghaddam, S.S.; Rezaei, N.; Sheidaei, A.; Hajipour, M.J.; Mahmoudi, N.; Mahmoudi, Z.; Dilmaghani-Marand, A.; Rezaee, K.; Sabooni, M.; et al. A Nationwide Study of Metabolic Syndrome Prevalence in Iran; A Comparative Analysis of Six Definitions. PLoS ONE 2021, 16, e0241926. [Google Scholar] [CrossRef]
- Asbjornsdottir, B.; Lauth, B.; Fasano, A.; Thorsdottir, I.; Karlsdottir, I.; Gudmundsson, L.S.; Gottfredsson, M.; Smarason, O.; Sigurdardottir, S.; Halldorsson, T.I.; et al. Meals, Microbiota and Mental Health in Children and Adolescents (MMM-Study): A Protocol for an Observational Longitudinal Case-Control Study. PLoS ONE 2022, 17, e0273855. [Google Scholar] [CrossRef]
- Voith, V.L. Recent Advances in Psychopharmacology. Tijdschr. Diergeneeskd. 1993, 118 (Suppl. S1), 59S–61S. [Google Scholar] [CrossRef]
- Maremmani, A.G.I.; Gazzarrini, D.; Fiorin, A.; Cingano, V.; Bellio, G.; Perugi, G.; Maremmani, I. Psychopathology of Addiction: Can the SCL90-Based Five-Dimensional Structure Differentiate Heroin Use Disorder from a Non-Substance-Related Addictive Disorder Such as Gambling Disorder? Ann. Gen. Psychiatry 2018, 17, 3. [Google Scholar] [CrossRef]
- Guerdjikova, A.I.; McElroy, S.L.; Kotwal, R.; Stanford, K.; Keck, P.E. Psychiatric and Metabolic Characteristics of Childhood versus Adult-Onset Obesity in Patients Seeking Weight Management. Eat. Behav. 2007, 8, 266–276. [Google Scholar] [CrossRef]
- Lee, K.; Abraham, S.; Cleaver, R. A Systematic Review of Licensed Weight-Loss Medications in Treating Antipsychotic-Induced Weight Gain and Obesity in Schizophrenia and Psychosis. Gen. Hosp. Psychiatry 2022, 78, 58–67. [Google Scholar] [CrossRef]
- Hod, R.; Mohd Nor, N.H.; Maniam, S. Systematic Review on E-Cigarette and Its Effects on Weight Gain and Adipocytes. PLoS ONE 2022, 17, e0270818. [Google Scholar] [CrossRef]
- Khalil, H.; Ellwood, L.; Lord, H.; Fernandez, R. Pharmacological Treatment for Obesity in Adults: An Umbrella Review. Ann. Pharmacother. 2020, 54, 691–705. [Google Scholar] [CrossRef]
- Orzelska-Górka, J.; Mikulska, J.; Wiszniewska, A.; Biała, G. New Atypical Antipsychotics in the Treatment of Schizophrenia and Depression. Int. J. Mol. Sci. 2022, 23, 10624. [Google Scholar] [CrossRef] [PubMed]
- Vogel Martinez, M.I.; León, F.; Torres, R.; Crossley, N.A. First and Second Generation Anti-psychotics in Schizophrenia: Efficacy, Effectiveness and Dose Effect. ARS MEDICA J. Med. Sci. 2017, 42. [Google Scholar] [CrossRef]
- Pañero Herranz, C.; Madrid, A.M. Psychological Aspects, Treatment and Prevention; Universidad Pontificia Comillas: Madrid, Spain, 2021. [Google Scholar]
- Pscheidt, S.L.; Zardeto, H.N.; de Sá Junior, A.R.; Schneider, I.J.C. Cardiovascular Diseases and Use of Antipsychotics in Schizophrenia: A Review. J. Bras. Psiquiatr. 2022, 71, 253–272. [Google Scholar] [CrossRef]
- Panizzutti, B.; Bortolasci, C.C.; Spolding, B.; Kidnapillai, S.; Connor, T.; Richardson, M.F.; Truong, T.T.T.; Liu, Z.S.J.; Gray, L.; Kim, J.H.; et al. Biological Mechanism(S) Underpinning the Association between Antipsychotic Drugs and Weight Gain. J. Clin. Med. 2021, 10, 4095. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.C.; Yang, S.Y.; Liao, Y.T.; Chen, C.C.; Kuo, C.J. Anti-psychotic Medications and Risk of Acute Coronary Syndrome in Schizophrenia: A Nested Case-Control Study. PLoS ONE 2016, 11, e0163533. [Google Scholar] [CrossRef]
- Kranzler, H.N.; Cohen, S.D. Psychopharmacologic Treatment of Psychosis in Children and Adolescents. Efficacy and Management. Child Adolesc. Psychiatr. Clin. N. Am. 2013, 22, 727–744. [Google Scholar] [CrossRef]
- Himmerich, H.; Bentley, J.; Lichtblau, N.; Brennan, C.; Au, K. Facets of Shared Decision-Making on Drug Treatment for Adults with an Eating Disorder. Int. Rev. Psychiatry 2019, 31, 332–346. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.; Stogios, N.; Smith, E.; Lee, J.; Maksyutynsk, K.; Au, E.; Wright, D.C.; De Palma, G.; Graff-Guerrero, A.; Gerretsen, P.; et al. Gut microbiome in schizophrenia and antipsychotic-induced metabolic alterations: A scoping review. Ther. Adv. Psychopharmacol. 2022, 20451253221096525. [Google Scholar]
- Allison, D.B.; Mentore, J.L.E.; Heo, M.; Chandler, L.P.; Cappelleri, J.C.; Infante, M.C.; Weiden, P.J. Antipsychotic-Induced Weight Gain: A Comprehensive Research Synthesis. Am. J. Psychiatry 1999, 156, 1686–1696. [Google Scholar] [CrossRef]
- Palacio-Ortiz, J.D.; Londoño-Herrera, J.P.; Nanclares-Márquez, A.; Robledo-Rengifo, P.; Quintero-Cadavid, C.P. Psychiatric Disorders in Children and Adolescents during the COVID-19 Pandemic. Rev. Colomb. Psiquiatr. 2020, 49, 279–288. [Google Scholar] [CrossRef] [PubMed]
- Stancil, S.L.; Abdel-Rahman, S.; Wagner, J. Developmental Considerations for the Use of Naltrexone in Children and Adolescents. J. Pediatr. Pharmacol. Ther. 2021, 26, 675–695. [Google Scholar] [CrossRef]
- van Mil, E.G.A.H.; Westerterp, K.R.; Kester, A.D.M.; Delemarre-van De Waal, H.A.; Gerver, W.J.M.; Saris, W.H.M. The Effect of Sibutramine on Energy Expenditure and Body Composition in Obese Adolescents. J. Clin. Endocrinol. Metab. 2007, 92, 1409–1414. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ford, T.C.; Nibbs, R.; Crewther, D.P. Glutamate/GABA+ Ratio Is Associated with the Psychosocial Domain of Autistic and Schizotypal Traits. PLoS ONE 2017, 12, e0181961. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.; Stubbs, B.; Hewitt, C.; Ajjan, R.A.; Alderson, S.L.; Gilbody, S.; Holt, R.I.G.; Hosali, P.; Hughes, T.; Kayalackakom, T.; et al. The Effectiveness of Pharmacological and Non-Pharmacological Interventions for Improving Glycaemic Control in Adults with Severe Mental Illness: A Systematic Review and Meta-Analysis. PLoS ONE 2017, 12, e0168549. [Google Scholar] [CrossRef] [PubMed]
- Frayne, J.; Watson, S.; Snellen, M.; Nguyen, T.; Galbally, M. The Association between Mental Illness, Psychotropic Medication Use and Hypertensive Disorders in Pregnancy: A Multicentre Study. Pregnancy Hypertens. 2021, 24, 22–26. [Google Scholar] [CrossRef]
- Ozdemir, A.C.; Wynn, G.M.; Vester, A.; Weitzmann, M.N.; Neigh, G.N.; Srinivasan, S.; Rudd, M.K. GNB3 Overexpression Causes Obesity and Metabolic Syndrome. PLoS ONE 2017, 12, e0188763. [Google Scholar] [CrossRef] [PubMed]
- Ahrens, K.R.; DuBois, D.L.; Richardson, L.P.; Fan, M.Y.; Lozano, P. Youth in Foster Care with Adult Mentors during Adolescence Have Improved Adult Outcomes. Pediatrics 2008, 121, e246–e252. [Google Scholar] [CrossRef] [PubMed]
- Planansky, K. Changes in Weight in Patients Receiving a “Tranquilizing” Drug. Psychiatr. Q. 1958, 32, 289–303. [Google Scholar] [CrossRef] [PubMed]
- Mejaddam, A.; Krantz, E.; Höskuldsdóttir, G.; Fändriks, L.; Mossberg, K.; Eliasson, B.; Trimpou, P.; Landin-Wilhelmsen, K. Comorbidity and Quality of Life in Obesity–a Comparative Study with the General Population in Gothenburg, Sweden. PLoS ONE 2022, 17, e0273553. [Google Scholar] [CrossRef] [PubMed]
- Oughli, H.; Lenze, E.J.; Locke, A.E.; Yingling, M.D.; Zhong, Y.; Miller, J.P.; Reynolds, C.F.; Mulsant, B.H.; Newcomer, J.W.; Peterson, T.R.; et al. Getting to Precision Psychopharmacology: Combining Clinical and Genetic Information to Predict Fat Gain from Aripiprazole. J. Psychiatr. Res. 2019, 114, 67–74. [Google Scholar] [CrossRef]
- Schulz, P. Opportunities and Challenges in Psychopharmacology. Dialogues Clin. Neurosci. 2019, 21, 119–130. [Google Scholar] [CrossRef] [PubMed]
- Goetz, R.L.; Miller, B.J. Meta-Analysis of Ghrelin Alterations in Schizophrenia: Effects of Olanzapine. Schizophr. Res. 2019, 206, 21–26. [Google Scholar] [CrossRef] [PubMed]

| Component | Descriptor | |
|---|---|---|
| P | Patient/Problem of interest | Patients |
| I | Intervention | Psychopharmacological treatment |
| C | Comparison | N/A |
| O | Outcome | Metabolic alterations and/or changes |
| MESH and DECS | ||
|---|---|---|
| Patient | Anticonvulsant, Antidepressants, Antiepileptics, Antipsychotic agent, Antipsychotic effect, Antipsychotics, Central nervous system depressants, Dopamine antagonist, GABA modulator, Hypnotic effect, Major Tranquilizers, Neuroleptics, Psychoactive agent, Psychoactive drug, Psychopharmacological treatment, Psychotropic drug, Second generation antidepressants, Sedative effect, Sedatives, Tranquilizers, Tranquilizing agents, Tricyclic antidepressants. | Abdominal Obesity, Abnormal metabolism, Blood pressure, LDL cholesterol, Metabolic, Metabolic disorders, Metabolic Syndrome, Metabolic Syndrome X, Morbid Obesity, Obesity, Pediatric Obesity, Reaven’s Syndrome, Severe Obesity, Triglycerides, Visceral Obesity. |
| Data Base | Search Algorithm |
|---|---|
| CLARIVATE PLOS ONE PUBMED SCIENCE DIRECT SCOPUS | (“Psychopharmaceuticals” OR “Agents Psychoactive” OR “Drugs Psychoactive” OR “Drugs Psychotropic” OR “Psychoactive Agents” OR “Psychoactive Drugs” OR “Psychopharmaceuticals” OR “Psychotropic Drugs” OR “Nootropic Agents” OR “Psychopharmacology”) AND (“Obesity” OR “Morbid Obesities” OR “Morbid Obesity” OR “Obesities Morbid” OR “Obesities Severe” OR “Obesity Severe” OR “Severe Obesities” OR “Severe Obesity”) |
| (“Psychopharmacology”) AND (“Metabolism”) | |
| (“Metabolic alteratios” OR ”Metabolic changes” OR ”Metabolic Sindrome”) AND (“Psychopharmacological treatment” OR “Psycofarmaceutical”) | |
| (“Psycoactive agent”) AND (“Metabolic Sindrome”) | |
| (“Metabolic alteration”AND “psychopharmacological treatment”) | |
| (“Psychopharmaceuticals” OR “Agents Psychoactive” OR “Drugs Psychoactive” OR “Drugs Psychotropic” OR “Psychoactive Agents” OR “Psychoactive Drugs” OR “Psychopharmaceuticals” OR “Psychotropic Drugs” OR “Nootropic Agents” OR “Psychopharmacology”) AND (“Patient Metabolic” OR “Adolescent Sindrome reaven” OR “Child Obesity” OR “Childhood Obesity” OR “Childhood Onset Obesity” OR “Childhood Overweight” OR “Infant Obesity” OR “Infant Overweight” OR “Infantile Obesity”) | |
| (“Psychopharmaceuticals” OR “Agents Psychoactive” OR “Drugs Psychoactive” OR “Drugs Psychotropic” OR “Psychoactive Agents” OR “Psychoactive Drugs” OR “Psychopharmaceuticals” OR “Psychotropic Drugs” OR “Nootropic Agents” OR “Psychopharmacology”) AND (“Obesity Infant” OR “Obesity” OR “Obesity Pediatric” OR “Overweight Adolescent” OR “Overweight Childhood” OR “Overweight Infant”) | |
| (“Metabolic change”) AND (“Psycofarmacological treatment”) | |
| (“Psychopharmaceuticals” OR “Agents Psychoactive” OR “Drugs Psychoactive” OR “Drugs Psychotropic” OR “Psychoactive Agents” OR “Psychoactive Drugs” OR “Psychopharmaceuticals” OR “Psychotropic Drugs” OR “Nootropic Agents” OR “Psychopharmacology”) AND (“Obesity in Adolescence” OR “Obesity in Childhood” OR “Obesity, Adolescent” OR “Obesity, Child” OR “Obesity, Childhood” OR “Obesity, Childhood Onset”) | |
| (“Psychopharmaceuticals” OR “Agents Psychoactive” OR “Drugs Psychoactive” OK “Drugs Psychotropic” OR “Psychoactive Agents” OR “Psychoactive Drugs” OR “Psychopharmaceuticals” OR “Psychotropic Drugs” OR “Nootropic Agents” OR “Psychopharmacology”) AND (“Adolescent Obesity” OR “Adolescent Overweight” OR “Child Obesity” OR “Childhood Obesity” OR “Childhood Onset Obesity” OR “Childhood Overweight” OR “Infant Obesity” OR “Infant Overweight” OR “Infantile Obesity”) | |
| (“Psicoactive agent” AND “metabolic challeng”) | |
| (“Antidepressants” OR “Antidepressant” OR “Tricyclic antidepressants” OR “Tricyclic antidepressant” OR “Second generation antidepressant” OR “Second generation antidepressant”) AND (“Metabolic changes”) OR (“Basal metabolism”) OR (“Metabolic syndrome”) OR (“Metabolic syndrome x”) OR (“Carbohydrate metabolism”) OR (“Abnormal metabolism”) OR (“Lipid metabolism”) OR (“Triglycerides”) OR (“Blood pressure”) OR (“Obesity”) OR (“Morbid Obesity”) OR (“Severe obesity”) OR (“Abdominal obesities”) | |
| (“Antipsychotic OR “Antipsychotic Agents” OR “Antipsychotic Agent” OR “Antipsychotic Effect” OR “Antipsychotic Effect” OR “ Antipsychotic Drugs” OR “Antipsychotic Drugs” OR “ Neuroleptics” OR “ Neuroleptic” OR “ Major Tranquilizers” OR “ Tranquilizer” OR “Dopamine antagonist”) OR (“Dopamine antagonist”) AND (“Metabolic changes”) OR (“Basal metabolism”) OR (“Metabolic syndrome”) OR (“Metabolic syndrome x”) OR (“Carbohydrate metabolism”) OR (“Abnormal metabolism”) OR (“Lipid metabolism”) OR (“Triglycerides”) OR (“Blood pressure”) OR (“Obesity”) OR (“Morbid Obesity”) OR (“Severe obesity”) OR (“Abdominal obesities”) | |
| (“Anticonvulsant” OR “Anticonvulsant” OR” Antiepileptic Drugs”) AND (“Metabolic changes”) OR (“Basal metabolism”) OR (“Metabolic syndrome”) OR (“Metabolic syndrome x”) OR (“Carbohydrate metabolism”) OR (“Abnormal metabolism”) OR (“Lipid metabolism”) OR (“Triglycerides”) OR (“Blood pressure”) OR (“Obesity”) OR (“Morbid Obesity”) OR (“Severe obesity”) OR (“Abdominal obesities”) | |
| (“Hypnotic Effect” OR “Hypnotic Effects” OR “Sedative Effect” OR “ Sedative Effects” OR “ Sedatives” OR “ Sedative” OR “ GABA Modulators” OR “ GABA modulator” OR “Tranquilizing Agents” OR “Central nervous system depressants”) AND (“Metabolic changes”) OR (“Basal metabolism”) OR (“Metabolic syndrome”) OR (“Metabolic syndrome x”) OR (“Carbohydrate metabolism”) OR (“Abnormal metabolism”) OR (“Lipid metabolism”) OR (“Triglycerides”) OR (“Blood pressure”) OR (“Obesity”) OR (“Morbid Obesity”) OR (“Severe obesity”) OR (“Abdominal obesities”) |
| Database | Total Found | Type of Document | Time Period | No Access | Revisions/Incomplete/Duplicated Texts | Non-Compliance with the Variable Criteria | Total Sample |
|---|---|---|---|---|---|---|---|
| PLOS ONE | 12,317 | 7921 | 2896 | 316 | 575 | 256 | 22 |
| SCOPUS | 3508 | 1561 | 956 | 126 | 249 | 63 | 12 |
| PUBMED | 287,491 | 13,650 | 27,330 | 10 | 2626 | 635 | 20 |
| SCIENCE DIRECT | 21,275 | 6729 | 16,069 | 94 | 1023 | 121 | 5 |
| CLARIVATE | 1451 | 469 | 78 | 9 | 19 | 35 | 5 |
| Total | 326,042 | 30,330 | 47,329 | 555 | 4492 | 1110 | 64 |
| Database | PLOS ONE | SCOPUS | PUB MED | SCIENCE DIRECT | CLARIVATE |
|---|---|---|---|---|---|
| Equation (1) | 7 | 4 | 5 | 0 | 2 |
| Equation (2) | 7 | 6 | 4 | 3 | 1 |
| Equation (3) | 3 | 1 | 2 | 2 | 1 |
| Equation (4) | 0 | 0 | 2 | 0 | 0 |
| Equation (5) | 0 | 1 | 2 | 0 | 1 |
| Equation (6) | 0 | 0 | 1 | 0 | 0 |
| Equation (12) | 2 | 0 | 1 | 0 | 0 |
| Equation (13) | 1 | 0 | 1 | 0 | 0 |
| Equation (14) | 1 | 0 | 1 | 0 | 0 |
| Equation (15) | 1 | 0 | 1 | 0 | 0 |
| Total | 22 | 12 | 20 | 5 | 5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sepúlveda-Lizcano, L.; Arenas-Villamizar, V.V.; Jaimes-Duarte, E.B.; García-Pacheco, H.; Paredes, C.S.; Bermúdez, V.; Rivera-Porras, D. Metabolic Adverse Effects of Psychotropic Drug Therapy: A Systematic Review. Eur. J. Investig. Health Psychol. Educ. 2023, 13, 1505-1520. https://doi.org/10.3390/ejihpe13080110
Sepúlveda-Lizcano L, Arenas-Villamizar VV, Jaimes-Duarte EB, García-Pacheco H, Paredes CS, Bermúdez V, Rivera-Porras D. Metabolic Adverse Effects of Psychotropic Drug Therapy: A Systematic Review. European Journal of Investigation in Health, Psychology and Education. 2023; 13(8):1505-1520. https://doi.org/10.3390/ejihpe13080110
Chicago/Turabian StyleSepúlveda-Lizcano, Lizeth, Vivian Vanessa Arenas-Villamizar, Enna Beatriz Jaimes-Duarte, Henry García-Pacheco, Carlos Silva Paredes, Valmore Bermúdez, and Diego Rivera-Porras. 2023. "Metabolic Adverse Effects of Psychotropic Drug Therapy: A Systematic Review" European Journal of Investigation in Health, Psychology and Education 13, no. 8: 1505-1520. https://doi.org/10.3390/ejihpe13080110
APA StyleSepúlveda-Lizcano, L., Arenas-Villamizar, V. V., Jaimes-Duarte, E. B., García-Pacheco, H., Paredes, C. S., Bermúdez, V., & Rivera-Porras, D. (2023). Metabolic Adverse Effects of Psychotropic Drug Therapy: A Systematic Review. European Journal of Investigation in Health, Psychology and Education, 13(8), 1505-1520. https://doi.org/10.3390/ejihpe13080110