
The Impact of Sociodemographic, Macroeconomic, and Health Status and Resources on Infant Mortality Rates in Oman: Evidence from 1980 to 2022




Abstract
1. Introduction
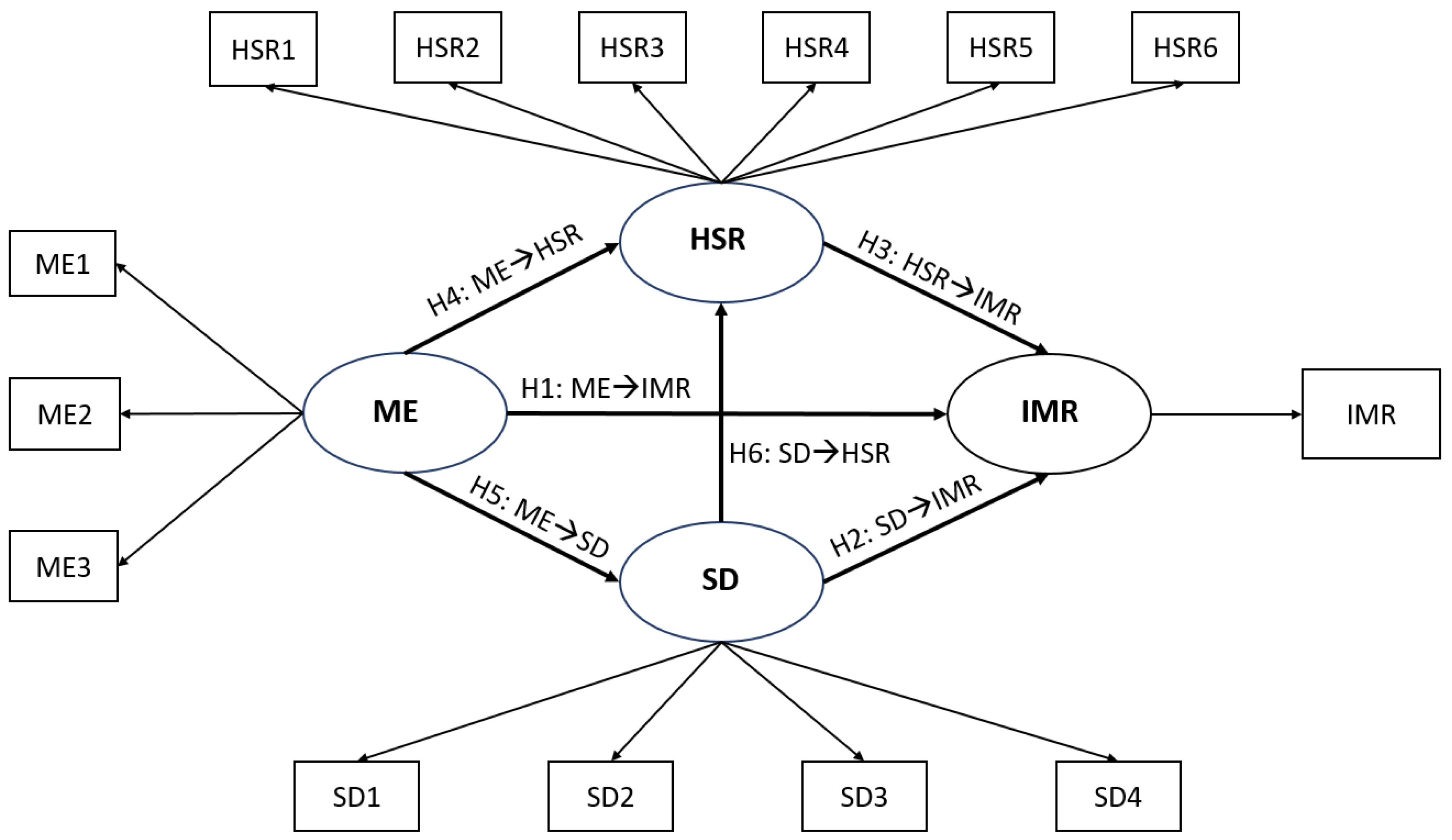
- To explore the effects of ME on IMR in Oman;
- To explore the effects of SD on IMR in Oman;
- To explore the effects of HSR on IMR in Oman;
- To explore the effects of ME on HSR in Oman;
- To explore the effects of ME on SD in Oman;
- To explore the effects of SD on HSR in Oman.
2. Materials and Methods
2.1. Study Design
2.2. Data Resources, Data Collection, and Sample Size
2.3. The Proposed Conceptual Model
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Variables in the Final Model
3.2. The Final Model Evaluation Indices
4. Discussion
4.1. The Effects of SD Determinants on IMR
4.2. The Effects of HSR Determinants on IMR
4.3. The Effects of ME Determinants on IMR
4.4. The Effects of ME Determinants on HSR
4.5. The Effects of ME Determinants on SD
4.6. Strengths and Limitations of This Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Infant Mortality Rate (between Birth and 11 Months per 1000 Live Births); World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Centers for Disease Control and Prevention. Principles of Epidemiology in Public Health Practice; U.S. Department of Health and Human Services: Washington, DC, USA, 2006. [Google Scholar]
- Gonzalez, R.M.; Gilleskie, D. Infant mortality rate as a measure of a country’s health: A robust method to improve reliability and comparability. Demography 2017, 54, 701–720. [Google Scholar] [CrossRef]
- World Health Organization. Millennium Development Goals, the Health Indicators: Scope, Definitions and Measurement Methods; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- United Nations. The 17 Goals|Sustainable Development. Available online: https://sdgs.un.org/goals (accessed on 1 April 2023).
- United Nations Inter-Agency Group for Child Mortality Estimation. Levels & Trends in Child Mortality, United Nations Inter-Agency Group for Child Mortality Estimation (UN IGME), Report 2021; UNICEF: Geneva, Switzerland, 2022. [Google Scholar]
- World Health Organization. Infant Mortality. Geneva, Switzerland. 2022. Available online: https://www.who.int/data/gho/data/themes/topics/indicator-groups/indicator-group-details/GHO/infant-mortality (accessed on 26 September 2022).
- Salam, A.A.; Al-Khraif, R.M. Child Mortality Transition in the Arabian Gulf: Wealth, Health System Reforms, and Development Goals. Front. Public Health 2020, 7, 402. [Google Scholar] [CrossRef]
- National Centre for Statistics and Information. Data Portal—Population—Infant Mortality Rate. Muscat, Sultanate of Oman. 2022. Available online: https://data.gov.om/OMPOP2016/population:: (accessed on 26 May 2022).
- Kim, D.; Saada, A. The social determinants of infant mortality and birth outcomes in Western developed nations: A cross-country systematic review. Int. J. Environ. Res. Public Health 2013, 10, 2296–2335. [Google Scholar] [CrossRef]
- Bugelli, A.; Borgès Da Silva, R.; Dowbor, L.; Sicotte, C. The determinants of infant mortality in Brazil, 2010–2020: A scoping review. Int. J. Environ. Res. Public Health 2021, 18, 6464. [Google Scholar] [CrossRef]
- Khadka, K.B.; Lieberman, L.S.; Giedraitis, V.; Bhatta, L.; Pandey, G. The socio-economic determinants of infant mortality in Nepal: Analysis of Nepal Demographic Health Survey, 2011. BMC Pediatr. 2015, 15, 152. [Google Scholar] [CrossRef]
- Kothari, C.L.; Corbit, K.; Presberry, J.; Bautista, T.; O’Rourke, B.; Lenz, D. Race, Multiraciality, Income, and Infant Mortality: Markers of Racial Equity. J. Child Fam. Stud. 2022, 31, 689–702. [Google Scholar] [CrossRef]
- Rezaei, S.; Jamshidi, K.; Moradi, K. Impact of socioeconomic and health system factors on infant mortality rate in Organization of the Petroleum Exporting Countries (OPEC): Evidence from 2004 to 2013. Int. J. Pediatr. 2015, 3, 493–499. [Google Scholar] [CrossRef]
- Tüzün, H. Factors Related to Infant Mortality Rate and Under-Five Mortality Rate in Turkey: An Ecological Study with Provincial Data. Çocuk Derg. 2021, 21, 221–230. [Google Scholar] [CrossRef]
- Valcin, J.; Jean-Charles, S.; Malfa, A.; Tucker, R.; Dorcélus, L.; Gautier, J.; Koster, M.P.; Lechner, B.E. Mortality, morbidity and clinical care in a referral neonatal intensive care unit in Haiti. PLoS ONE 2020, 15, e0240465. [Google Scholar] [CrossRef]
- Leal, M.D.C.; Bittencourt, S.D.D.A.; Torres, R.M.C.; Niquini, R.P.; Souza, P.R.B.D. Determinants of infant mortality in the Jequitinhonha Valley and in the North and Northeast regions of Brazil. Rev. De Saude Publica 2017, 51, 12. [Google Scholar] [CrossRef]
- World Health Organization. The Global Health Observatory. UHC Service Coverage Index (3.8.1). Geneva, Switzerland. 2022. Available online: https://www.who.int/data/gho/indicator-metadata-registry/imr-details/4834 (accessed on 4 January 2022).
- Lozano, R.; Fullman, N.; Mumford, J.E.; Knight, M.; Barthelemy, C.M.; Abbafati, C.; Abbastabar, H.; Abd-Allah, F.; Abdollahi, M.; Abedi, A. Measuring universal health coverage based on an index of effective coverage of health services in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1250–1284. [Google Scholar] [CrossRef]
- Tarekegn, W.; Tsegaye, S.; Berhane, Y. Skilled birth attendant utilization trends, determinant and inequality gaps in Ethiopia. BMC Women’s Health 2022, 22, 466. [Google Scholar] [CrossRef]
- Ayele, G.S.; Melku, A.T.; Belda, S.S. Utilization of skilled birth attendant at birth and associated factors among women who gave birth in the last 24 months preceding the survey in Gura Dhamole Woreda, Bale zone, southeast Ethiopia. BMC Public Health 2019, 19, 1501. [Google Scholar] [CrossRef]
- World Health Organization. Vaccines and Immunization. Geneva, Switzerland. 2022. Available online: https://www.who.int/health-topics/vaccines-and-immunization#tab=tab_1 (accessed on 1 April 2023).
- Testoni Costa-Nobre, D.; Kawakami, M.D.; Areco, K.C.N.; Sanudo, A.; Balda, R.C.X.; Marinonio, A.S.S.; Miyoshi, M.H.; Konstantyner, T.; Bandiera-Paiva, P.; Freitas, R.M.V. Clusters of cause specific neonatal mortality and its association with per capita gross domestic product: A structured spatial analytical approach. PLoS ONE 2021, 16, e0255882. [Google Scholar] [CrossRef]
- Shapira, G.; de Walque, D.; Friedman, J. How many infants may have died in low-income and middle-income countries in 2020 due to the economic contraction accompanying the COVID-19 pandemic? Mortality projections based on forecasted declines in economic growth. BMJ Open 2021, 11, e050551. [Google Scholar]
- Abdul Salam, A.; Elsegaey, I.; Khraif, R.; AlMutairi, A.; Aldosari, A. Components and public health impact of population growth in the Arab world. PLoS ONE 2015, 10, e0124944. [Google Scholar] [CrossRef]
- Bader, Y.; Ganguli, S. Analysis of the association between economic growth, environmental quality and health standards in the Gulf Cooperation Council during 1980-2012. Manag. Environ. Qual. 2019, 30, 1050–1071. Available online: https://www.emerald.com/insight/content/doi/10.1108/MEQ-03-2018-0061/full/html (accessed on 1 April 2023). [CrossRef]
- Al-Azri, M.; Al-Mamari, F.; Mondal, S. Healthcare expenditure and health outcome nexus: Exploring the evidences from Oman. J. Public Aff. 2020, 20, e2329. [Google Scholar] [CrossRef]
- Eltayib, R.A.A.; Al-Alawi, K.S.; Wirayuda, A.A.B.; Al-Azri, M.; Chan, M.F. The impact of sociodemographic, macroeconomic, and health status and resources determinants on infant mortality rates in the Gulf Cooperation Council (GCC) countries: A systematic review and meta-analysis. J. Neonatal Nurs. 2023, in press. [CrossRef]
- Abu-Heija, A.T.; Al-Bash, M.; Mathew, M. Gestational and Pregestational Diabetes Mellitus in Omani Women: Comparison of obstetric and perinatal outcomes. Sultan Qaboos Univ. Med. J. 2015, 15, e496–e500. [Google Scholar] [CrossRef]
- Patel, P.K. Profile of major congenital anomalies in the Dhahira region, Oman. Ann. Saudi Med. 2007, 27, 106–111. [Google Scholar] [CrossRef]
- Rahman, A.; Abdellatif, M.; Sharef, S.W.; Fazalullah, M.; Al-Senaidi, K.; Khan, A.A.; Ahmad, M.; Kripail, M.; Abuanza, M.; Bataclan, F. Changing Survival Rate of Infants Born Before 26 Gestational Weeks. Sultan Qaboos Univ. Med. J. 2015, 15, e351–e355. [Google Scholar] [CrossRef]
- Abdellatif, M.; Ahmed, M.; Bataclan, M.F.; Khan, A.A.; Al Battashi, A.; Al Maniri, A. The Patterns and Causes of Neonatal Mortality at a Tertiary Hospital in Oman. Oman Med. J. 2013, 28, 422–426. [Google Scholar] [CrossRef]
- Al-Haddabi, R.; Al-Bash, M.; Al-Mabaihsi, N.; Al-Maqbali, N.; Al-Dhughaishi, T.; Abu-Heija, A. Obstetric and perinatal outcomes of teenage pregnant women attending a tertiary teaching hospital in Oman. Oman Med. J. 2014, 29, 399–403. [Google Scholar] [CrossRef]
- Al Riyami, N.; Al-Rusheidi, A.; Al-Khabori, M. Perinatal Outcome of Monochorionic in Comparison to Dichorionic Twin Pregnancies. Oman Med. J. 2013, 28, 173–177. [Google Scholar] [CrossRef]
- Al-Shukri, M.; Khan, D.; Al-Hadrami, A.; Al-Riyami, N.; Gowri, V.; Haddabi, R.; Abdellatif, M.; Al-Dughaishi, T. Maternal and fetal outcomes of triplet gestation in a tertiary hospital in oman. Sultan Qaboos Univ. Med. J. 2014, 14, e204–e210. [Google Scholar]
- National Centre for Statistics and Information. Data Portal—Education/Health/Economy. Muscat, Sultanate of Oman. 2022. Available online: https://data.gov.om/ (accessed on 1 April 2023).
- The GCC Statistical Centre. Statistics. Available online: https://gccstat.org/en/statistic/statistics (accessed on 1 April 2023).
- The World Bank. Wolrd Bank Open Data. Available online: https://data.worldbank.org/ (accessed on 1 April 2023).
- Statistical, Economic and Social Research and Training Centre for Islamic Countries. OIC Statistics Database. Available online: https://www.sesric.org/oicstat.php (accessed on 1 April 2023).
- Institute for Health Metrics and Evaluation. The Global Health Data Exchange (GHDx) Data Catalog. Available online: https://ghdx.healthdata.org/ (accessed on 1 April 2023).
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: New York, NY, USA, 2013. [Google Scholar]
- Hair, J.F. Multivariate Data Analysis, 8th ed.; Cengage Learning EMEA: London, UK, 2018. [Google Scholar]
- Chan, M.F. Factors affecting infant mortality rates: Evidence from 1969–2008 data in Singapore. J. Public Health Z. Für Gesund. 2011, 19, 15–22. [Google Scholar] [CrossRef]
- Wirayuda, A.A.B.; Jaju, S.; Alsaidi, Y.; Chan, M.F. A structural equation model to explore sociodemographic, macroeconomic, and health factors affecting life expectancy in Oman. Pan Afr. Med. J. 2022, 41, 75. [Google Scholar]
- Wirayuda, A.A.B.; Al-Mahrezi, A.; Chan, M.F. Factors Impacting Life Expectancy in Bahrain: Evidence from 1971 to 2020 Data. Int. J. Soc. Determ. Health Health Serv. 2023, 53, 74–84. [Google Scholar] [CrossRef]
- Chan, M.F.; Devi, M.K. Factors affecting life expectancy: Evidence from 1980-2009 data in Singapore, Malaysia, and Thailand. Asia-Pac. J. Public Health 2015, 27, 136–146. [Google Scholar] [CrossRef]
- Ibrahim, A.; Salama, H.; Al-Obiedly, S.; Al-Rifai, H.; Al-Qubaisi, M. Socioeconomic Risk Factors for Hospital-based Neonatal Death: A Population-based Study. Asploro J. Pediatr. Child Health 2021, 2020, 72. [Google Scholar]
- Amir, A.-H.; Mahdi, S.; Samira, V.; Reza Omani, S. The Correlation of Human Development Index on Fertility and Mortality Rate: A Global Ecological Study. Int. J. Pediatr. 2016, 4, 4071–4080. [Google Scholar] [CrossRef]
- Al Awaidy, S.; Bawikar, S.; Prakash, K.P.; Al Rawahi, B.; Mohammed, A.J. Surveillance of adverse events following immunization: 10 years’ experience in Oman. East. Mediterr. Health J. 2010, 16, 474–480. [Google Scholar] [CrossRef]
- Abuqamar, M.; Coomans, D.; Louckx, F. Correlation between socioeconomic differences and infant mortality in the Arab World (1990-2009). Int. J. Sociol. Anthropol. 2011, 3, 15. [Google Scholar]
- Rahman, S.; Nimeri, N.; El Ansari, W.; Bener, A. Chapter 4: Socio-demographic, Obstetric and Fetal Determinants of Neonatal Mortality. In Neonatal and Perinatal Mortality: Global Challenges, Risk Factors and Interventions; Nova Biomedical: New York, NY, USA, 2017; pp. 43–80. [Google Scholar]
- Hair, J.F., Jr.; Hult, G.T.M.; Ringle, C.M.; Sarstedt, M.; Danks, N.P.; Ray, S. Partial Least Squares Structural Equation Modeling (PLS-SEM) Using R: A Workbook; Springer: Cham, Switzerland, 2021. [Google Scholar]
- Hair, J.F.; Hult, G.T.M.; Ringle, C.M.; Sarstedt, M.; Thiele, K.O. Mirror, mirror on the wall: A comparative evaluation of composite-based structural equation modeling methods. J. Acad. Mark. Sci. 2017, 45, 616–632. [Google Scholar] [CrossRef]
- Chin, W.; Cheah, J.-H.; Liu, Y.; Ting, H.; Lim, X.-J.; Cham, T.H. Demystifying the role of causal-predictive modeling using partial least squares structural equation modeling in information systems research. Ind. Manag. Data Syst. 2020, 120, 2161–2209. [Google Scholar] [CrossRef]
- Jöreskog, K.G.; Sörbom, D. PRELIS 2 User’s Reference Guide: A Program for Multivariate Data Screening and Data Summarization: A Preprocessor for LISREL; Scientific Software International: Chicago, IL, USA, 1996. [Google Scholar]
- Henseler, J. On the convergence of the partial least squares path modeling algorithm. Comput. Stat. 2010, 25, 107–120. [Google Scholar] [CrossRef]
- Hair, J.F.; Ringle, C.M.; Sarstedt, M. PLS-SEM: Indeed a silver bullet. J. Mark. Theory Pract. 2011, 19, 139–152. [Google Scholar] [CrossRef]
- Henseler, J.; Ringle, C.M.; Sarstedt, M. A new criterion for assessing discriminant validity in variance-based structural equation modeling. J. Acad. Mark. Sci. 2015, 43, 115–135. [Google Scholar] [CrossRef]
- Franke, G.; Sarstedt, M. Heuristics versus statistics in discriminant validity testing: A comparison of four procedures. Internet Res. 2019, 29, 430–447. [Google Scholar] [CrossRef]
- Chin, W.W. How to write up and report PLS analyses. In Handbook of Partial Least Squares; Springer: Berlin/Heidelberg, Germany, 2010; pp. 655–690. [Google Scholar]
- Roemer, E.; Schuberth, F.; Henseler, J. HTMT2–an improved criterion for assessing discriminant validity in structural equation modeling. Ind. Manag. Data Syst. 2021, 121, 2637–2650. [Google Scholar] [CrossRef]
- Hair, J.F.; Hult, G.T.M.; Ringle, C.M.; Sarstedt, M. A Primer on Partial Least Squares Structural Equation Modeling (PLS-SEM), 2nd ed.; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2017. [Google Scholar]
- Aguirre-Urreta, M.I.; Rönkkö, M. Statistical inference with PLSc using bootstrap confidence intervals. MIS Q. 2018, 42, 1001–1020. [Google Scholar] [CrossRef]
- Streukens, S.; Leroi-Werelds, S. Bootstrapping and PLS-SEM: A step-by-step guide to get more out of your bootstrap results. Eur. Manag. J. 2016, 34, 618–632. [Google Scholar] [CrossRef]
- Shmueli, G.; Ray, S.; Estrada, J.M.V.; Chatla, S.B. The elephant in the room: Predictive performance of PLS models. J. Bus. Res. 2016, 69, 4552–4564. [Google Scholar] [CrossRef]
- Hair, J.F.; Risher, J.J.; Sarstedt, M.; Ringle, C.M. When to use and how to report the results of PLS-SEM. Eur. Bus. Rev. 2019, 31, 2–24. [Google Scholar] [CrossRef]
- Hair, J.F.; Sarstedt, M.; Pieper, T.M.; Ringle, C.M. The use of partial least squares structural equation modeling in strategic management research: A review of past practices and recommendations for future applications. Long Range Plan. 2012, 45, 320–340. [Google Scholar] [CrossRef]
- Subramaniam, T.; Loganathan, N.; Yerushalmi, E.; Devadason, E.S.; Majid, M. Determinants of infant mortality in older ASEAN economies. Soc. Indic. Res. 2018, 136, 397–415. [Google Scholar] [CrossRef]
- Neiger, R. Long-term effects of pregnancy complications on maternal health: A review. J. Clin. Med. 2017, 6, 76. [Google Scholar] [CrossRef]
- Hauspurg, A.; Ying, W.; Hubel, C.A.; Michos, E.D.; Ouyang, P. Adverse pregnancy outcomes and future maternal cardiovascular disease. Clin. Cardiol. 2018, 41, 239–246. [Google Scholar] [CrossRef]
- Yang, W.; Han, F.; Gao, X.; Chen, Y.; Ji, L.; Cai, X. Relationship between gestational weight gain and pregnancy complications or delivery outcome. Sci. Rep. 2017, 7, 12531. [Google Scholar] [CrossRef]
- Vilanova, C.S.; Hirakata, V.N.; de Souza Buriol, V.C.; Nunes, M.; Goldani, M.Z.; da Silva, C.H. The relationship between the different low birth weight strata of newborns with infant mortality and the influence of the main health determinants in the extreme south of Brazil. Popul. Health Metr. 2019, 17, 15. [Google Scholar] [CrossRef]
- Anele, C.R.; Hirakata, V.N.; Goldani, M.Z.; da Silva, C.H. The influence of the municipal human development index and maternal education on infant mortality: An investigation in a retrospective cohort study in the extreme south of Brazil. BMC Public Health 2021, 21, 194. [Google Scholar] [CrossRef]
- Munoz, F.M. Current challenges and achievements in maternal immunization research. Front. Immunol. 2018, 9, 436. [Google Scholar] [CrossRef]
- David, J. Infant mortality and public health expenditure in Nigeria: Empirical explanation of the nexus. Timis. J. Econ. Bus. (TJEB) 2018, 11, 149–164. [Google Scholar] [CrossRef]
- Department of Surveillance & Disease Control. Manual on Expanded Program on Immunization, 3rd ed.; Directorate General of Health Affairs: 2002. Available online: https://pdf4pro.com/amp/view/manual-on-expanded-program-on-immunization-5aa1e9.html (accessed on 1 April 2023).
- Al-Abri, S.S.; Al-Rawahi, B.; Abdelhady, D.; Al-Abaidani, I. Effective vaccine management and Oman’s healthcare system’s challenge to maintain high global standards. J. Infect. Public Health 2018, 11, 742–744. [Google Scholar] [CrossRef]
- Abbuy, K.E. Macroeconomic Determinants of Infant Mortality in WAEMU Countries: Evidence from Panel Data Analysis. Appl. Econ. Financ. 2018, 5, 6. [Google Scholar] [CrossRef]
- Genowska, A.; Strukcinskiene, B.; Villerusa, A.; Konstantynowicz, J. Converging or diverging trajectories of mortality under one year of age in the Baltic States: A comparison with the European Union. Arch. Public Health 2021, 79, 76. [Google Scholar] [CrossRef]
- Ortigoza, A.F.; Granados, J.A.T.; Miranda, J.J.; Alazraqui, M.; Higuera, D.; Villamonte, G.; de Lima Friche, A.A.; Gutierrez, T.B.; Roux, A.V.D. Characterising variability and predictors of infant mortality in urban settings: Findings from 286 Latin American cities. J. Epidemiol. Community Health 2021, 75, 264–270. [Google Scholar] [CrossRef]
- Jagrič, T.; Mun, J.C.; Brown, C.E.; Fister, D. Economic Impact of the Health Sector on the Regional Level-Case of a Small, Open Economy. Lex Localis 2021, 19, 621–657. [Google Scholar] [CrossRef]
- Naik, Y.; Baker, P.; Ismail, S.A.; Tillmann, T.; Bash, K.; Quantz, D.; Hillier-Brown, F.; Jayatunga, W.; Kelly, G.; Black, M. Going upstream—An umbrella review of the macroeconomic determinants of health and health inequalities. BMC Public Health 2019, 19, 1678. [Google Scholar] [CrossRef]
- Rezapour, A.; Teimourizad, A.; Movahed, M.S.; Khazaei, T.; Khalilabad, T.H. Factors affecting healthcare sector inflation rate in Iran’s provinces for 2004–2015. Int. Trans. J. Eng. Manag. Appl. Sci. Technol. 2020, 11, 11A02Q. Available online: https://tuengr.com/V11/11A02QM.pdf (accessed on 1 April 2023). [CrossRef]
- Finlay, J.E.; Mejia-Guevara, I.; Akachi, Y. Inequality in total fertility rates and the proximate determinants of fertility in 21 sub-Saharan African countries. PLoS ONE 2018, 13, e0203344. [Google Scholar] [CrossRef]
- Pezzulo, C.; Nilsen, K.; Carioli, A.; Tejedor-Garavito, N.; Hanspal, S.E.; Hilber, T.; James, W.H.; Ruktanonchai, C.W.; Alegana, V.; Sorichetta, A. Geographical distribution of fertility rates in 70 low-income, lower-middle-income, and upper-middle-income countries, 2010–2016: A subnational analysis of cross-sectional surveys. Lancet Glob. Health 2021, 9, e802–e812. [Google Scholar] [CrossRef]
- Furstenberg, F.F. Family change in global perspective: How and why family systems change. Fam. Relat. 2019, 68, 326–341. [Google Scholar] [CrossRef]
- Islam, M.M. Demographic transition in Sultanate of Oman: Emerging demographic dividend and challenges. Middle East Fertil. Soc. J. 2020, 25, 7. [Google Scholar] [CrossRef]
- Schrecker, T.; Bambra, C. How Politics Makes Us Sick: Neoliberal Epidemics. 2015. Springer Link. Available online: https://link.springer.com/book/10.1057/9781137463074 (accessed on 1 April 2023).



{kind=link}
{kind=link}
| Label | Variable | Definition | Source |
|---|---|---|---|
| IMR | Infant Mortality Rate | The infant mortality rate is the number of infants dying before one year per 1000 live births yearly. | World Bank |
| SD variables | |||
| SD1 | Birth rate (crude) | Crude birth rate indicates the number of live births per 1000 midyear population. | World Bank |
| SD2 | Adolescent fertility rate | Adolescent fertility rate is the number of births per 1000 women aged 15–19. | World Bank |
| SD3 | Fertility rate (total, births per woman) | Total fertility rate represents the number of children that would be born to a woman if she were to live to the end of her childbearing years and bear children in accordance with age-specific fertility rates of the specified year | World Bank |
| SD4 | Percentages (%) of women married | Proportion of married or in-union women of reproductive-age (ages 15–49) in total population of women in the same age group, expressed in terms of percentage. | SESRIC |
| HSR variables | |||
| HSR1 | Newborns protected against tetanus (%) | Percentage of births by women of child-bearing age who are immunized against tetanus, i.e., newborns who achieved protection at birth from their mothers who received tetanus toxoid doses during the pregnancy. | World Bank |
| HSR2 | One-year-olds immunized with BCG (%) | One-year-olds who have received one dose of Bacille Calmette-Guérin (BCG) vaccine in a given year, expressed in terms of percentage. | SESRIC |
| HSR3 | One-year-olds immunized with MCV1 (%) | One-year-olds who have received at least one dose of measles-containing vaccine (MCV1) in a given year, expressed in terms of percentage. | SESRIC |
| HSR4 | One-year-olds immunized with Pol3 (%) | One-year-olds who have received three doses of polio vaccine (Pol3) in a given year, expressed in terms of percentage | SESRIC |
| HSR5 | Births attended by skilled health personnel (%) | Birth attended by Skilled Health worker in a given period (as % of total birth) | IHME-GHDx |
| HSR6 | UHC service coverage index (0 to 100) | Coverage of essential health services | IHME-GHDx |
| ME variables | |||
| ME1 | GDP per capita (current US$) | GDP per capita is gross domestic product divided by midyear population | World Bank |
| ME2 | Employment to population ratio (15+, males) in % | Proportion of a country’s female population (with ages 15+) that is employed, expressed in terms of percentage. | World Bank |
| ME3 | Employment to population ratio (15+, females) in % | Proportion of a country’s male population (with ages 15+) that is employed, expressed in terms of percentage. | World Bank |
| Label | N | Min | Max | Mean | SD | Skewness | Kurtosis |
|---|---|---|---|---|---|---|---|
| IMR | 43 | 9.50 | 78.90 | 24.09 | 19.53 | 1.44 | 1.08 |
| SD3 | 43 | 2.57 | 8.13 | 4.64 | 2.013 | 0.64 | −1.24 |
| SD4 | 43 | 55.21 | 69.47 | 61.884 | 5.89 | 0.28 | −1.76 |
| HSR1 | 43 | 29.00 | 99.00 | 83.77 | 21.22 | −1.84 | 1.94 |
| HSR2 | 43 | 51.00 | 99.00 | 94.07 | 10.74 | −3.14 | 9.69 |
| HSR3 | 43 | 10.00 | 99.00 | 88.26 | 23.30 | −2.41 | 4.66 |
| HSR4 | 43 | 18.00 | 99.00 | 88.51 | 23.62 | −2.31 | 3.92 |
| ME1 | 43 | 5073.85 | 24,722.64 | 11,899.81 | 6770.15 | 0.66 | −1.20 |
| ME2 | 43 | 43.88 | 87.80 | 73.93 | 11.06 | −1.19 | 1.34 |
| ME3 | 43 | 16.07 | 27.59 | 22.16 | 3.18 | −0.07 | −1.17 |
| LV | MV | FL | CA | Rho-A | CR | R2 | Q2 | AVE | HTMT (95% CI) | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IMR | ME | SD | HSR | |||||||||
| IMR | IMR | 1.000 | 1.000 | 1.000 | 1.000 | 0.959 | 0.942 | 1.000 | - | - | - | 0.934 (0.854–0.970) |
| ME | ME1 | 0.893 | 0.938 | 0.963 | 0.960 | - | - | 0.889 | 0.851 (0.763–0.910) | - | - | 0.728 (0.606–0.818) |
| ME2 | 0.946 | |||||||||||
| ME3 | 0.987 | |||||||||||
| SD | SD3 | 0.990 | 0.978 | 0.981 | 0.989 | 0.839 | 0.816 | 0.978 | 0.878 (0.833–0.928) | 0.954 (0.913–0.983) | - | 0.698 (0.595–0.815) |
| SD4 | 0.988 | |||||||||||
| HSR | HSR1 | 0.944 | 0.978 | 0.979 | 0.984 | 0.521 | 0.474 | 0.940 | - | - | - | - |
| HSR2 | 0.953 | |||||||||||
| HSR3 | 0.992 | |||||||||||
| HSR4 | 0.988 | |||||||||||
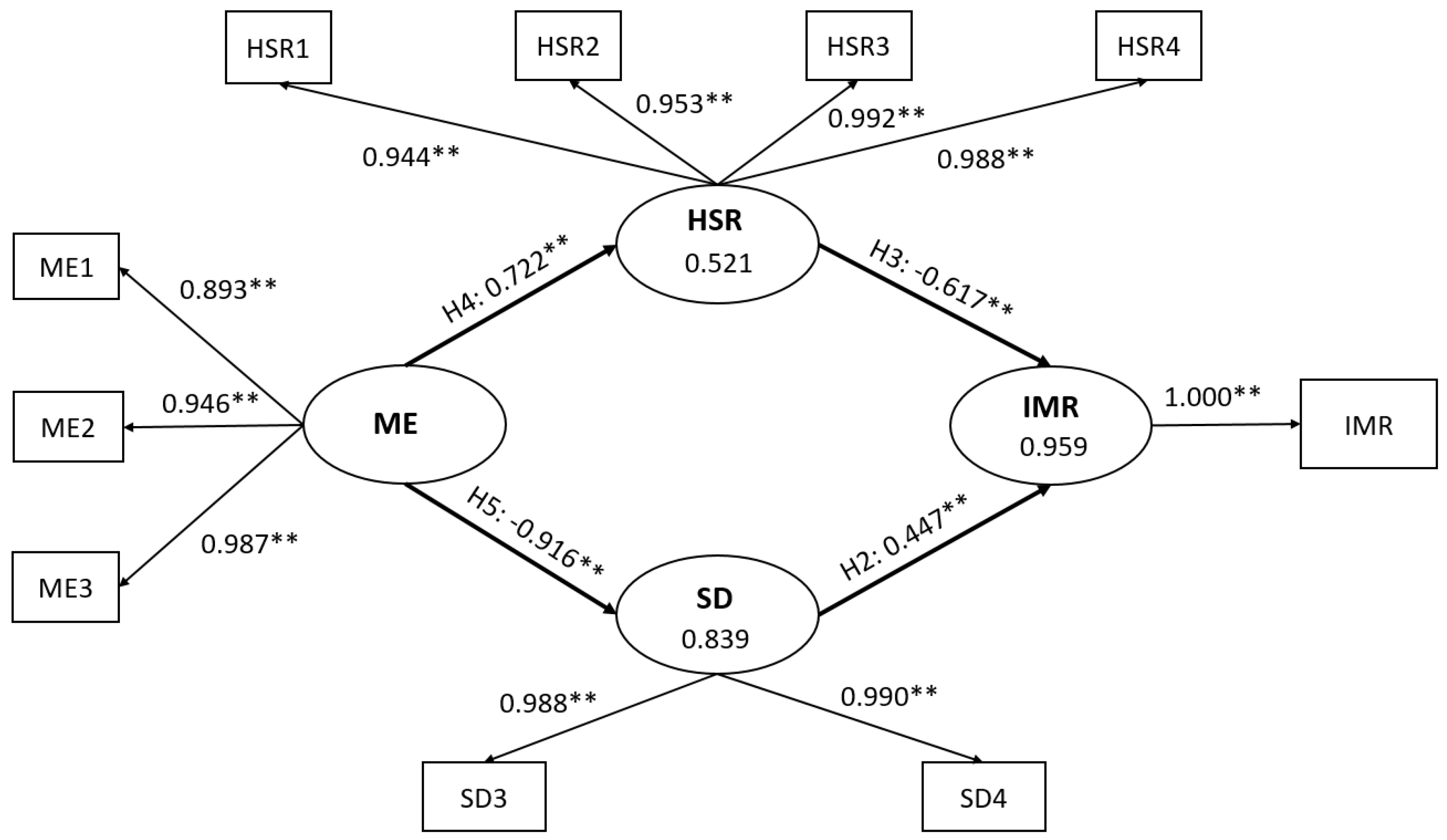
| Hypothesis | Pathway | Direct Effect (95% CI) | Indirect Effect (95% CI) | Total Effect (95% CI) | ƒ2 |
|---|---|---|---|---|---|
| H1 | ME→IMR | - | −0.854 (−0.898 to −0.790) | −0.854 (−0.898 to −0.790) | - |
| H2 | SD→IMR | 0.447 (0.327 to 0.601) | - | 0.447 (0.327 to 0.601) | 2.560 |
| H3 | HSR→IMR | −0.617 (−0.712 to −0.458) | - | −0.617 (−0.712 to −0.458) | 4.891 |
| H4 | ME→HSR | 0.722 (0.605 to 0.806) | - | 0.722 (0.605 to 0.806) | 1.087 |
| H5 | ME→SD | −0.916 (−0.945 to −0.880) | - | −0.916 (−0.945 to −0.880) | 5.193 |
| H6 | SD→HSR | - | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eltayib, R.A.A.; Al-Azri, M.; Chan, M.F. The Impact of Sociodemographic, Macroeconomic, and Health Status and Resources on Infant Mortality Rates in Oman: Evidence from 1980 to 2022. Eur. J. Investig. Health Psychol. Educ. 2023, 13, 986-999. https://doi.org/10.3390/ejihpe13060075
Eltayib RAA, Al-Azri M, Chan MF. The Impact of Sociodemographic, Macroeconomic, and Health Status and Resources on Infant Mortality Rates in Oman: Evidence from 1980 to 2022. European Journal of Investigation in Health, Psychology and Education. 2023; 13(6):986-999. https://doi.org/10.3390/ejihpe13060075
Chicago/Turabian StyleEltayib, Rawaa Abubakr Abuelgassim, Mohammed Al-Azri, and Moon Fai Chan. 2023. "The Impact of Sociodemographic, Macroeconomic, and Health Status and Resources on Infant Mortality Rates in Oman: Evidence from 1980 to 2022" European Journal of Investigation in Health, Psychology and Education 13, no. 6: 986-999. https://doi.org/10.3390/ejihpe13060075
APA StyleEltayib, R. A. A., Al-Azri, M., & Chan, M. F. (2023). The Impact of Sociodemographic, Macroeconomic, and Health Status and Resources on Infant Mortality Rates in Oman: Evidence from 1980 to 2022. European Journal of Investigation in Health, Psychology and Education, 13(6), 986-999. https://doi.org/10.3390/ejihpe13060075