
Virtual Approach to the Comparative Analysis of Biomaterials Used in Endodontic Treatment

 ,
,  ,
,  ,
,  and
and 
Abstract
1. The Importance of Endodontics in the General Concept of Sustainable Dentistry Development
2. General Characteristics of Materials and Clinical Procedures in Endodontic Treatment
- A self-etching primer comprising a sulfonic acid-terminated functional monomer, HEMA 2-hydroxyelylmethacrylate, water, and a polymerization initiator;
- A dual-curing resin sealant containing approximately 70% calcium hydroxide, bismuth oxychloride, barium glass, and silica filler;
- A core made of synthetic thermoplastic filling material based on polyester materials, including approximately 65% of fillers with bismuth oxychloride, bioactive glass, and barium sulphate.
3. General Concept and Scope of the Work Performed
- Root canal filling material during endodontic treatment, assuming that the process can be carried out both cold and warm;
- The methodology of root canal preparation with the use of available methods and various tools to ensure three-dimensional hermetization of the root canal with replacement material;
- Root canal obturation technology during cold and hot endodontic treatment;
- The most advantageous visualization methods for assessing the effectiveness of endodontic treatment, including the use of methodological experiences used in materials science and engineering for the study of micro- and nanostructured objects.
- Performing a literature review and preliminary analyses to determine the scope of materials, techniques for the development and obturation of root canals, and the selection of methods for assessing the effectiveness of the filling, which will be subjected to detailed tests, with the results presented in subsequent publications in this series [286];
- Performing a theoretical analysis using the methods of procedural benchmarking and comparative analysis, with the use of contextual matrices to optimize the selection of materials virtually, techniques for the development and obturation of root canals, methods for assessing the effectiveness of fillings, which methods are usually used among others in management science and especially in foresight research as part of knowledge management; the results of the analyses are the subject of this paper;
- Performing a series of in vitro tests on the removed human incisors of the maxilla, canines, and single-canal premolars of the maxilla and mandible for empirical confirmation of the correctness of the methodology selected in the virtual analysis mode presented in this paper, and substantive studies of the regularities presented in the series of subsequent publications [286];
- Development of teeth for testing with the use of rotary nickel–titanium conical drills, and comparatively, nickel–titanium hand-held drills;
- Obturation with filling material selected in the virtual analysis mode, with the use of contextual matrices and comparative material based on polymeric polyester materials: Resilon, of the trade name RealSeal, with the use of cold and hot techniques;
- Demineralization of parts of the prepared and filled teeth with the use of various analysed methods to prepare them for microscopic examinations;
- Making longitudinal fractures in the parts of the prepared and filled tooth roots, after cutting the notches along the axis of the teeth, cooling them in liquid nitrogen, and making longitudinal fractures in these conditions initiated by the incisions made;
- Performing materialographic examinations on the transverse and longitudinal sections of the prepared and filled tooth roots;
- Performing microscopic examinations of exams, fractures, and demineralized teeth with the use of a stereoscopic light microscope, scanning electron microscope, and confocal laser microscope to verify experimentally the developed methodology of material selection, techniques for the development and obturation of root canals, methods for assessing the effectiveness of fillings, and substantive tests of regularities presented in a series of subsequent publications [286];
- Development of methodological procedures for the selection of materials, development and obturation techniques of root canals, assessing methods of the filling effectiveness, and the substantive results of the examination of the regularities, together with the examinations of statistical results, presented in a series of subsequent publications [286].
- Selecting the conditions for the preparation and obstruction of the root canals to ensure that the filling remains in the oral cavity of the endodontically treated teeth for the longest possible time;
- Selecting the optimal methods for the preparation and obturation of root canals, ensuring the best tightness of the filling;
- Development of the most appropriate and useful research methods to assess the effectiveness of endodontic treatment due to the appropriate quality of root canal fillings and the required high tightness, possibly with the minimum number of the smallest gaps on the border of the root canal wall and the filling material;
- Explanation of the reasons for the differences in the tightness of the filling between the root canal wall and the filling material in connection with the considered methods of root canal preparation and obturation;
- In line with the previously presented assumptions, this paper covers the first three of the presented research tasks, while the fourth task is the main content of subsequent papers from the announced series [286].
4. Description of the Methodological Concept of Materials Selection, Techniques for the Development and Obturation of Root Canals, and the Assessment of the Effectiveness of Fillings
5. Description of Authors’ Contextual Matrices Concerning Materials for Filling Root Canals
6. Description of Authors’ Contextual Matrices Relating to Techniques for the Development of Root Canals
7. Description of the Authors’ Contextual Matrices Concerning the Techniques of Obturation of Root Canals
8. Description of the Authors’ Contextual Matrices Concerning the Methods of Assessing the Effectiveness of Fillings
- The number of leaks along the entire length of the root canal;
- A representative value characterizing the mean dimensions of such leakage.
- Mean value;
- Standard deviation;
- Confidence interval with the assumed significance level of 0.95;
- Mean difference significance test.
9. Experimental Verification and Examples of the Application of the Selected Methods to Evaluate the Effectiveness of Root Canal Filling
10. Summary and Final Comments
- Materials selection in the coordinate system generalized index of material quality for root canal filling (x) and generalized index of material strength in the root canal (y);
- Root canal development technique selection in the coordinate system of a generalized organizational index of techniques for the development of root canals (x) and generalized index of the quality of filling with selected techniques (y);
- Techniques of obturation selection in the coordinate system generalized index of material strength applied in root canal obturation techniques (x) and generalized index of the effectiveness of root canal obturation techniques (y);
- Assessing the tightness of root canal fillings selection in the coordinate system of the generalized index of organizational conditions (x) and generalized index of investigations effectiveness (y).
Author Contributions
Funding
Notice
Conflicts of Interest
References
- Dobrzański, L.A.; Dobrzański, L.B.; Dobrzańska-Danikiewicz, A.D.; Dobrzańska, J. The Concept of Sustainable Development of Modern Dentistry. Processes 2020, 8, 1605. [Google Scholar] [CrossRef]
- Watt, R.G.; Daly, B.; Allison, P.; Macpherson, L.M.D.; Venturelli, R.; Listl, S.; Weyant, R.J.; Mathur, M.R.; Guarnizo-Herreño, C.C.; Celeste, R.K.; et al. Ending the neglect of global oral health: Time for radical action. Lancet 2019, 394, 261–272. [Google Scholar] [CrossRef]
- Peres, M.A.; Macpherson, L.M.D.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreño, C.C.; Kearns, C.; et al. Oral diseases: A global public health challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef]
- Fejerskov, O. Concepts of dental caries and their consequences for understanding the disease. Community Dent. Oral Epidemiol. 1997, 25, 5–12. [Google Scholar] [CrossRef]
- Reisine, S.; Litt, M. Social and psychological theories and their use for dental practice. Int. Dent. J. 1993, 43 (Suppl. 1), 279–287. [Google Scholar]
- Selwitz, R.H.; Ismail, A.I.; Pitts, N.B. Dental caries. Lancet 2007, 369, 51–59. [Google Scholar] [CrossRef]
- GBD Compare. Viz Hub. Available online: https://vizhub.healthdata.org/gbd-compare/ (accessed on 6 April 2021).
- Li, X.; Tornstad, L.; Olsen, I. Brain abscesses caused by oral infection. Dent. Traumatol. 1999, 15, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Scannapieco, F.A.; Bush, R.B.; Paju, S. Associations between periodontal disease and risk for nosocomial bacterial pneumonia and chronic obstructive pulmonary disease. A systemic review. Ann. Periodontol. 2003, 8, 54–69. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzański, L.B. Dentistry 4.0 Concept in the Design and Manufacturing of Prosthetic Dental Restorations. Processes 2020, 8, 525. [Google Scholar] [CrossRef]
- Aleksander, M.; Krishnan, B.; Shenoy, N. Diabetes mellitus and odontogenic infections-an exaggerated risk? Oral Maxillofac. Surg. 2008, 12, 129–130. [Google Scholar] [CrossRef]
- Scannapieco, F.A. Role of oral bacteria in respiratory infection. J. Periodontol. 1999, 70, 793–802. [Google Scholar] [CrossRef] [PubMed]
- Mueller, A.A.; Saldami, B.; Stübinger, S.; Walter, C.; Flückiger, U.; Merlo, A.; Schwenzer-Zimmerer, K.; Zeilhofer, H.F.; Zimmerer, S. Oral bacterial cultures in nontraumatic brain abscesses: Results of a first line study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 107, 469–476. [Google Scholar] [CrossRef]
- Buset, S.L.; Walter, C.; Friedmann, A.; Weiger, R.; Borgnakke, W.S.; Zitzmann, N.U. Are periodontal diseases really silent? A systematic review of their effect on quality of life. J. Clin. Periodontol. 2016, 43, 333–344. [Google Scholar] [CrossRef] [PubMed]
- Sierpinska, T.; Golebiewska, M.; Dlugosz, J.W.; Kemona, A.; Laszewicz, W. Connection between masticatory efficiency and pathomorphologic changes in gastric mucosa. Quintessence Int. 2007, 38, 31–37. [Google Scholar]
- Al-Nawas, B.; Maeurer, M. Severe versus local odontogenic bacterial infections: Comparison of microbial isolates. Eur. Surg. Res. 2008, 40, 220–224. [Google Scholar] [CrossRef] [PubMed]
- Pallasch, T.J.; Wahl, M.J. Focal infection: New age or ancient history? Endodon. Top. 2003, 4, 32–45. [Google Scholar] [CrossRef]
- De Pablo, P.; Dietrich, T.; McAlindon, T.E. Association of periodontal disease and tooth loss with rheumatoid arthritis in the US population. J. Rheumatol. 2008, 35, 70–76. [Google Scholar] [PubMed]
- Felton, D.A. Edentualism and comorbid factors. J. Prosthodont. 2009, 18, 88–96. [Google Scholar] [CrossRef]
- Volzke, H.; Schwahn, C.; Hummel, A.; Wolff, B.; Kleine, V.; Robinson, D.M.; Dahm, J.B.; Felix, S.B.; John, U.; Kocher, T. Tooth loss is independently associated with the risk of acquired aortic valve sclerosis. Am. Heart J. 2005, 150, 1198–1203. [Google Scholar] [CrossRef] [PubMed]
- Bagchi, S.; Tripathi, A.; Tripathi, S.; Kar, S.; Tiwari, S.C.; Singh, J. Obstructive sleep apnea and neurocognitive dysfunction in edentulous patients. J. Prosthodont. 2019, 28, e837–e842. [Google Scholar] [CrossRef]
- Nagpal, R.; Yamashiro, Y.; Izumi, Y. The two-way association of periodontal infection with systemic disorders: An overview. Mediat. Inflamm. 2015, 2015, 793898. [Google Scholar] [CrossRef] [PubMed]
- Abnet, C.C.; Qiao, Y.L.; Dawsey, S.M.; Dong, Z.W.; Taylor, P.R.; Mark, S.D. Tooth loss is associated with increased risk of total death and death from upper gastrointestinal cancer, heart disease, and stroke in a Chinese population-based cohort. Int. J. Epidemiol. 2005, 34, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Burzyńska, B.; Mierzwińska-Nastalska, E. Rehabilitacja protetyczna pacjentów bezzębnych. Nowa Stomatol. 2011, 4, 167–199. [Google Scholar]
- Bui, F.Q.; Almeida-da-Silva, C.L.C.; Huynh, B.; Trinh, A.; Liu, J.; Woodward, J.; Asadi, H.; Ojcius, D.M. Association between periodontal pathogens and systemic disease. Biomed. J. 2019, 42, 27–35. [Google Scholar] [CrossRef]
- Holmlund, A.; Holm, G.; Lind, L. Number of teeth as a predictor of cardiovascular mortality in a cohort of 7674 subjects followed for 12 years. J. Periodontol. 2010, 81, 870–876. [Google Scholar] [CrossRef] [PubMed]
- Takata, Y.; Ansai, T.; Matsumura, K.; Awano, S.; Hamasaki, T.; Sonoki, K.; Kusaba, A.; Akifusa, S.; Takehara, T. Relationship between tooth loss and electrocardiographic abnormalities in octogenarians. J. Dent. Res. 2001, 80, 1648–1652. [Google Scholar] [CrossRef] [PubMed]
- Felton, D.A. Complete edentulism and comorbid diseases: An update. J. Prosthodont. 2016, 25, 5–20. [Google Scholar] [CrossRef]
- Chen, H.; Iinuma, M.; Onozuka, M.; Kubo, K.-Y. Chewing maintains hippocampus-dependent cognitive. Int. J. Med. Sci. 2015, 12, 502–509. [Google Scholar] [CrossRef]
- Stein, P.S.; Desrosiers, M.; Donegan, S.J.; Yepes, J.F.; Kryscio, R.J. Tooth loss, dementia and neuropathology in the Nun study. J. Am. Dent. Assoc. 2007, 138, 1314–1322. [Google Scholar] [CrossRef]
- Henke, K. A model for memory systems based on processing modes rather than consciousness. Nat. Rev. Neurosci. 2010, 11, 523–532. [Google Scholar] [CrossRef]
- Lexomboon, D.; Trulsson, M.; Wårdh, I.; Parker, W.G. Chewing ability and tooth loss: Association with cognitive impairment in an elderly population study. J. Am. Geriatr. Soc. 2012, 60, 1951–1956. [Google Scholar] [CrossRef]
- Hirano, Y.; Obata, T.; Takahashi, H.; Tachibana, A.; Kuroiwa, D.; Takahashi, T.; Ikehira, H.; Onozuka, M. Effects of chewing on cognitive processing speed. Brain Cognit. 2013, 81, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Onishi, M.; Iinuma, M.; Tamura, Y.; Kubo, K.Y. Learning deficits and suppression of the cell proliferation in the hippocampal dentate gyrus of offspring are attenuated by maternal chewing during prenatal stress. Neurosci. Lett. 2014, 560, 77–80. [Google Scholar] [CrossRef]
- Kawahata, M.; Ono, Y.; Ohno, A.; Kawamoto, S.; Kimoto, K.; Onozuka, M. Loss of molars early in life develops behavioral lateralization and impairs hippocampus-dependent recognition memory. BMC Neurosci. 2014, 15, 4. [Google Scholar] [CrossRef] [PubMed]
- Clarkson, B.H.; Exterkate, R.A.M. Noninvasive dentistry: A dream or reality? Caries Res. 2015, 49 (Suppl. 1), 11–17. [Google Scholar] [CrossRef]
- Pitts, N.B.; Zero, D.T. White Paper on Dental Caries Prevention and Management. FDI World Dental Federation. Available online: http://www.fdiworlddental.org/sites/default/files/media/documents/2016-fdi_cpp-white_paper.pdf (accessed on 6 April 2021).
- Wierichs, R.J.; Meyer-Lueckel, H. Systematic review on noninvasive treatment of root caries lesions. J. Dent. Res. 2015, 94, 261–271. [Google Scholar] [CrossRef] [PubMed]
- Marsh, P.D.; Head, D.A.; Devine, D.A. Prospects of oral disease control in the future—an opinion. J. Oral. Microbiol. 2014, 6, 261–276. [Google Scholar] [CrossRef] [PubMed]
- Marthaler, T.M. A standardized system of recording dental conditions. Helv. Odontol. Acta 1966, 10, 1–18. [Google Scholar]
- Dirks, O.B.; van Amerongen, J.; Winkler, K.C. A reproducible method for caries evaluation. J. Dent. Res. 1951, 30, 346–359. [Google Scholar] [CrossRef] [PubMed]
- Black, G.V. A Work on Operative Dentistry: The Technical Procedures in Filling Teeth; Medico-Dental Publishing: Chicago, IL, USA, 1917; p. 5. [Google Scholar]
- Pitts, N. “ICDAS”-an international system for caries detection and assessment being developed to facilitate caries epidemiology, research and appropriate clinical management. Community Dent. Health 2004, 21, 193–198. [Google Scholar]
- ICDAS Website. Available online: https://www.icdas.org/ (accessed on 6 April 2021).
- Featherstone, J.D. The continuum of dental caries—evidence for a dynamic disease process. J. Dent. Res. 2004, 83, C39–C42. [Google Scholar] [CrossRef] [PubMed]
- Ismail, A.I.; Sohn, W.; Tellez, M.; Amaya, A.; Sen, A.; Hasson, H.; Pitts, N.B. The International Caries Detection and Assessment System (ICDAS): An integrated system for measuring dental caries. Community Dent. Oral Epidemiol. 2007, 35, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Ismail, A.; Tellez, M.; Pitts, N.B.; Ekstrand, K.R.; Ricketts, D.; Longbottom, C.; Eggertsson, H.; Deery, C.; Fisher, J.; Young, D.A.; et al. Caries management pathways preserve dental tissues and promote oral health. Community Dent. Oral Epidemiol. 2013, 41, e12–e40. [Google Scholar] [CrossRef] [PubMed]
- Pitts, N.B.; Ekstrand, K.R. International Caries Detection and Assessment System (ICDAS) and its International Caries Classification and Management System (ICCMS)—methods for staging of the caries process and enabling dentists to manage caries. Community Dent. Oral Epidemiol. 2013, 41, e41–e52. [Google Scholar] [CrossRef]
- Ormond, C.; Douglas, G.; Pitts, N. The use of the International Caries Detection and Assessment System (ICDAS) in a National Health Service general dental practice as part of an oral health assessment. Prim. Dent. Care 2010, 17, 153–159. [Google Scholar] [CrossRef]
- Ismail, A.; Pitts, N.B.; Tellez, M. The international caries classification and management system (ICCMSTM) an example of a caries management pathway. BMC Oral Health 2015, 15, S9. [Google Scholar] [CrossRef]
- Sunay, H.; Tanalp, J.; Dikbas, I.; Bayirli, G. Cross-sectional evaluation of the periapical status and quality of root canal treatment in a selected population of urban Turkish adults. Int. Endodon. J. 2007, 40, 139–145. [Google Scholar] [CrossRef]
- Tsuneishi, M.; Yamamoto, T.; Yamanaka, R.; Tamaki, N.; Sakamoto, T.; Tsuji, K.; Watanabe, T. Radiographic evaluation of periapical status and prevalence of endodontic treatment in an adult Japanese population. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2005, 100, 631–635. [Google Scholar] [CrossRef]
- Lazarski, M.P.; Walker, W.A.; Flores, C.M.; Schindler, W.G.; Hargreaves, K.M. Epidemiological evaluation of the outcomes of nonsurgical root canal treatment in a large cohort of insured dental patients. J. Endodon. 2001, 27, 791–796. [Google Scholar] [CrossRef]
- Chen, S.C.; Chuech, L.H.; Hsiao, C.K.; Tsai, M.Y.; Ho, S.C.; Chiang, C.P. An epidemiologic study of tooth retention after nonsurgical endodontic treatment in a large population in Taiwan. J. Endodon. 2007, 33, 226–229. [Google Scholar] [CrossRef]
- Meuwissen, R.; Eschen, S. Twenty years of endodontic treatment. J. Endodon. 1983, 9, 390–393. [Google Scholar] [CrossRef]
- Kirkevang, L.L.; Horsted-Bindslev, P.; Orstavik, D.; Wenzel, A. Frequency and distribution of endodontically treated teeth and apical periodontitis in an urban Danish population. Int. Endodon. J. 2001, 34, 198–205. [Google Scholar] [CrossRef]
- Salehrabi, R.; Rotstein, I. Endodontic treatment outcomes in a large patient population in the USA: An epidemiological study. J. Endodon. 2004, 30, 846–850. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, M.; Haapasalo, M.; Imazato, S.; Il Lee, J.; Momoi, Y.; Murakami, S.; Whelton, H.; Wilson, N. Dentistry in the 21st century: Challenges of a globalising world. Int. Dent. J. 2014, 64, 333–342. [Google Scholar] [CrossRef] [PubMed]
- Dobrzański, L.B.; Dobrzański, L.A.; Dobrzańska, J.; Rudziarczyk, K.; Achtelik-Franczak, A. Akcesorium do ochrony osobistej personelu dentystycznego przed koronawirusem SARS-CoV-2 i innymi drobnoustrojami chorobotwórczymi. Zgłoszenie Pat. 2020, 434391. [Google Scholar]
- Galicia, J.C.; Mungia, R.; Taverna, M.V.; Mendoza, M.J.; Estrela, C.; Gaudin, A.; Zhang, C.; Vaughn, B.A.; Khan, A.A. Response by Endodontists to the SARS-CoV-2 (COVID−19) Pandemic: An International Survey. Front. Dent. Med. 2021, 1, 1–24. [Google Scholar] [CrossRef]
- Ates, A.A.; Alomari, T.; Bhardwaj, A.; Tabnjh, A.; Gambarini, G. Differences in endodontic emergency management by endodontists and general dental practitioners in COVID-19 times. Braz. Oral Res. 2020, 34, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Dobrzański, L.A.; Dobrzański, L.B. Approach to the Design and Manufacturing of Prosthetic Dental Restorations According to the Rules of Industry 4.0. Mater. Perform. Charact. 2020, 9, 394–476. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzańska-Danikiewicz, A.D.; Dobrzański, L.B. Effect of Biomedical Materials in the Implementation of a Long and Healthy Life Policy. Processes 2021, 9, 865. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzański, L.B.; Dobrzańska-Danikiewicz, A.D. Overview of conventional technologies using the powders of metals, their alloys and ceramics in Industry 4.0 stage. JAMME 2020, 98, 56–85. [Google Scholar] [CrossRef]
- Dobrzański, L.A. Role of materials design in maintenance engineering in the context of industry 4.0 idea. JAMME 2019, 96, 12–49. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzański, L.B.; Achtelik-Franczak, A.; Dobrzańska, J. Application Solid Laser-Sintered or Machined Ti6Al4V Alloy in Manufacturing of Dental Implants and Dental Prosthetic Restorations According to Dentistry 4.0 Concept. Processes 2020, 8, 664. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzańska-Danikiewicz, A.D. Applications of Laser Processing of Materials in Surface Engineering in the Industry 4.0 Stage of the Industrial Revolution. Mater. Perform. Charact. 2019, 8, 1091–1129. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzańska-Danikiewicz, A.D. Why Are Carbon-Based Materials Important in Civilization Progress and Especially in the Industry 4.0 Stage of the Industrial Revolution. Mater. Perform. Charact. 2019, 8, 337–370. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzański, L.B.; Dobrzańska-Danikiewicz, A.D.; Kraszewska, M. Manufacturing powders of metals, their alloys and ceramics and the importance of conventional and additive technologies for products manufacturing in Industry 4.0 stage. AMSE 2020, 102, 13–41. [Google Scholar] [CrossRef]
- Hermann, M.; Pentek, T.; Otto, B. Design Principles for Industrie 4.0 Scenarios: A Literature Review; Technische Universität Dortmund: Dortmund, Germany, 2015. [Google Scholar]
- Kagermann, H.; Wahlster, W.; Helbig, J. Recommendations for Implementing the Strategic Initiative INDUSTRIE 4.0: Final Report of the Industrie 4.0 Working Group; Federal Ministry of Education and Research: Bonn, Germany, 2013. [Google Scholar]
- Rüßmann, M.; Lorenz, M.; Gerbert, P.; Waldner, M.; Justus, J.; Engel, P.; Harnisch, M. Industry 4.0: The Future of Productivity and Growth in Manufacturing Industries; Boston Consulting Group: Boston, MA, USA, 2015. [Google Scholar]
- Kagermann, H. Chancen von Industrie 4.0 Nutzen. In Industrie 4.0 in Produktion, Automatisierung und Logistik; Springer Fachmedien Wiesbaden: Wiesbaden, Germany, 2014; pp. 603–614. [Google Scholar]
- Lee, J.; Kao, H.-A.; Yang, S. Service Innovation and Smart Analytics for Industry 4.0 and Big Data Environment. Proc. CIRP 2014, 16, 3–8. [Google Scholar] [CrossRef]
- Jose, R.; Ramakrishna, S. Materials 4.0: Materials Big Data Enabled Materials Discovery. Appl. Mat. Today. 2018, 10, 127–132. [Google Scholar] [CrossRef]
- Buer, S.-V.; Strandhagen, J.O.; Chan, F.T.S. The Link between Industry 4.0 and Lean Manufacturing: Mapping Current Research and Establishing a Research Agenda. Int. J. Produc. Res. 2018, 56, 2924–2940. [Google Scholar] [CrossRef]
- Brettel, M.; Friederichsen, N.; Keller, M.; Rosenberg, M. How Virtualization, Decentralization, and Network-Building Change the Manufacturing Landscape: An Industry 4.0 Perspective. Int. J. Mech. Aerospac. Indust. Mechatron. Manuf. Eng. 2014, 8, 37–44. [Google Scholar]
- Tay, S.I.; Lee, T.C.; Hamid, N.A.A.; Ahmad, A.N.A. An Overview of Industry 4.0: Definition, Components, and Government Initiatives. J. Adv. Res. Dynamic Control Syst. 2018, 10, 1379–1387. [Google Scholar]
- Xu, X. Machine Tool 4.0 for the New Era of Manufacturing. Int. J. Adv. Manuf. Techn. 2017, 92, 1893–1900. [Google Scholar] [CrossRef]
- Sipsas, K.; Alexopoulos, K.; Xanthakis, V.; Chryssolouris, G. Collaborative Maintenance in Flow-Line Manufacturing Environments: An Industry 4.0 Approach. Proc. CIRP 2016, 55, 236–241. [Google Scholar] [CrossRef]
- Posada, J.; Toro, C.; Barandiaran, I.; Oyarzun, D.; Stricker, D.; de Amicis, R.; Pinto, E.B.; Eisert, P.; Döllner, J.; Vallarino, I. Visual Computing as a Key Enabling Technology for Industrie 4.0 and Industrial Internet. IEEE Comp. Graph Appl. 2015, 35, 26–40. [Google Scholar] [CrossRef] [PubMed]
- Hozdic, E. Smart Factory for Industry 4.0: A Review. Int. J. Modern Manuf. Tech. 2015, 7, 28–35. [Google Scholar]
- Zhong, R.Y.; Xu, X.; Klotz, E.; Newman, S.T. Intelligent Manufacturing in the Context of Industry 4.0: A Review. J. Eng. 2017, 3, 616–630. [Google Scholar] [CrossRef]
- Łobaziewicz, M. Zarządzanie Inteligentnym Przedsiębiorstwem w Dobie Przemysłu 4.0; Towarzystwo Naukowe Organizacji i Kierownictwa: Toruń, Poland, 2019. [Google Scholar]
- Bahrin, M.A.K.; Othman, M.F.; Azli, N.H.N.; Talib, M.F. Industry 4.0: A Review on Industrial Automation and Robotic. J. Tekno 2016, 78, 137–143. [Google Scholar] [CrossRef]
- Vaidya, S.; Ambad, P.; Bhosle, S. Industry 4.0–A Glimpse. Proc. Manuf. 2018, 20, 233–238. [Google Scholar] [CrossRef]
- Lee, J.; Bagheri, B.; Kao, H.-A. A Cyber-Physical Systems Architecture for Industry 4.0-Based Manufacturing Systems. Manuf. Lett. 2015, 3, 18–23. [Google Scholar] [CrossRef]
- Stock, T.; Seliger, G. Opportunities of Sustainable Manufacturing in Industry 4.0. Proc. CIRP 2016, 40, 536–541. [Google Scholar] [CrossRef]
- Schumacher, A.; Erol, S.; Sihn, W. A Maturity Model for Assessing Industry 4.0 Readiness and Maturity of Manufacturing Enterprises. Proc. CIRP 2016, 52, 161–166. [Google Scholar] [CrossRef]
- Kumar, K.; Zindani, D.; Davim, J.P. Industry 4.0: Developments towards the Fourth Industrial Revolution; Springer Nature: Singapore, 2019. [Google Scholar]
- Pfeiffer, S. Robots, Industry 4.0 and Humans, or Why Assembly Work Is More than Routine Work. Societies 2016, 6, 16. [Google Scholar] [CrossRef]
- Wang, S.; Wan, J.; Zhang, D.; Li, D.; Zhang, C. Towards Smart Factory for Industry 4.0: A Self-Organized Multi-Agent System with Big Data Based Feedback and Coordination. Comp. Network 2016, 101, 158–168. [Google Scholar] [CrossRef]
- Ardito, L.; Petruzzelli, A.M.; Panniello, U.; Garavelli, A.C. Towards Industry 4.0: Mapping Digital Technologies for Supply Chain Management-Marketing Integration. Business Proc. Manag. J. 2019, 25, 323–346. [Google Scholar] [CrossRef]
- Mosterman, P.J.; Zander, J. Industry 4.0 as a Cyber-Physical System Study. Software Syst. Model 2016, 15, 17–29. [Google Scholar] [CrossRef]
- Almada-Lobo, F. The Industry 4.0 Revolution and the Future of Manufacturing Execution Systems (MES). J. Innov. Manag. 2015, 3, 16–21. [Google Scholar] [CrossRef]
- Lu, Y. Industry 4.0: A Survey on Technologies, Applications and Open Research Issues. J. Indust. Infor. Integrat. 2017, 6, 1–10. [Google Scholar] [CrossRef]
- Qin, J.; Liu, Y.; Grosvenor, R. A Categorical Framework of Manufacturing for Industry 4.0 and Beyond. Proc. CIRP 2016, 52, 173–178. [Google Scholar] [CrossRef]
- Thoben, K.-D.; Wiesner, S.; Wuest, T. ‘Industrie 4.0’ and Smart Manufacturing–A Review of Research Issues and Application Examples. Int. J. Automat. Techn. 2017, 11, 4–16. [Google Scholar] [CrossRef]
- Peroz, I.; Blankenstein, F.; Lange, K.-P.; Naumann, M. Restoring endodontically treated teeth with post and cores–A review. Quintessence Int. 2005, 36, 737–746. [Google Scholar]
- Shutzky-Goldberg, I.; Shutzky, H.; Gorfil, C.; Smidt, A. Restoration of endodontically treated teeth review and treatment recommendations. Int. J. Dent. 2009, 2009, 150251. [Google Scholar] [CrossRef]
- Schwartz, R.S.; Robbins, J.W. Post placement and restoration of endodontically treated teeth: A literature review. J. Endodon. 2004, 5, 289–301. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, B.P.; Câmara, A.C.; Aguiar, C.M. Prevalence of endodontic diseases: An epidemiological evaluation in a Brazilian subpopulation. Braz. J. Oral Sci. 2016, 15, 119–123. [Google Scholar] [CrossRef][Green Version]
- Alwadani, M.; Mashyakhy, M.H.; Jali, A.; Hakami, A.O.; Areshi, A.; Daghriri, A.A.; Shaabi, F.I.; Al Moaleem, M.M. Dentists and Dental Intern’s Preferences of Root Canal Treatment with Restoration Versus Extraction then Implant-Supported Crown Treatment Plan. Open Dent. J. 2019, 13, 93–100. [Google Scholar] [CrossRef]
- Estrela, C.; Holland, R.; Estrela, C.R.; Alencar, A.H.; Sousa-Neto, M.D.; Pécora, J.D. Characterization of successful root canal treatment. Braz. Dent. J. 2014, 25, 3–11. [Google Scholar] [CrossRef]
- Aggarwal, A.; Pandey, V.; Bansal, N. Regenerative Endodontics- Potential Approaches in Revitalizing the Tooth Pulp-A Review Article. J. Adv. Med. Dent. Sci. Res. 2019, 7, 27–32. [Google Scholar] [CrossRef]
- Sreedev, C.P.; Karthick, K.; Mathew, S.; Raju, I. Regenerative endodontics: An overview. J. Indian Acad. Dent. Spec. Res. 2017, 4, 18–22. [Google Scholar] [CrossRef]
- Nair, P.N.R. On the cause of persistent apical periodontitis: A review. Int. Endod. J. 2006, 34, 249–281. [Google Scholar] [CrossRef]
- Malarvizhi, D.; Shuruthi, J.; Anuradha, B.; Subbiya, A. Etiology And Management Of Separation Of Instruments In Endodontics – An Overview. Eur. J. Mol. Clin. Med. 2020, 7, 1229–1234. [Google Scholar]
- Drabarczyk-Nasińska, M.; Kacprzak, M. Nowoczesne leczenie endodontyczne–materiały i metody wypełniania kanału korzeniowego. Borgis Nowa Stomatol. 2001, 3, 11–14. [Google Scholar]
- Siqueira, J.F.; Rocas, I.N.; Lopes, H.P. de Uzeda, M. Coronal leakage of two root canal sealers containing calcium hydroxide after exposure to human saliva. J. Endod. 1999, 25, 14–16. [Google Scholar] [CrossRef]
- Hirsch, J.M.; Ahlstrom, U.; Henrikson, P.A.; Peterson, L.E. Periapical surgery. Int. J. Oral Surg. 1979, 8, 173–185. [Google Scholar] [CrossRef]
- Sundqvist, G.; Figdor, D.; Persson, S.; Sjörgren, U. Microbiological analysis of teeth with failed endodontic treatment and the outcome of conservative re-treatment. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1998, 85, 86–93. [Google Scholar] [CrossRef]
- Carrotte, P. Endodontics: Part 1. The modern concept of root canal treatment. Br. Dent. J. 2004, 197, 181–183. [Google Scholar] [CrossRef] [PubMed]
- Karamifar, K.; Tondari, A.; Saghiri, M.A. Endodontic Periapical Lesion: An Overview on the Etiology, Diagnosis and Current Treatment Modalities. Eur. Endod. J. 2020, 2, 54–67. [Google Scholar] [CrossRef]
- Grossman, L. Endodontic Practice, 11th ed.; Lea & Fibiger: Phildelphia, PA, USA, 1988; p. 242. [Google Scholar]
- Muliyar, S.; Shameem, K.A.; Thankachan, R.P.; Francis, P.G.; Jayapalan, C.S.; Hafiz, K.A. Microleakage in endodontics. J. Int. Oral Health. 2014, 6, 99–104. [Google Scholar]
- Krastl, G.; Allgayer, N.; Lenherr, P.; Filippi, A.; Taneja, P.; Weiger, R. Tooth discoloration induced by endodontic materials: A literature review. Dent. Traumatol. 2013, 29, 2–7. [Google Scholar] [CrossRef]
- Teixeira, F.B.; Teixeira, E.C.; Thompson, J.Y.; Trope, M. Fracture resistance of roots endodontically treated with a new resin filling material. J. Am. Dent. Assoc. 2004, 135, 646–652. [Google Scholar] [CrossRef]
- Ahmad, P.; Dummer, P.M.H.; Noorani, T.Y.; Asif, J.A. The top 50 most-cited articles published in the International Endodontic Journal. Int. Endod. J. 2019, 52, 803–818. [Google Scholar] [CrossRef]
- Raghavendra, S.S.; Jadhav, G.R.; Gathani, K.M.; Kotadia, P. Bioceramics in Endodontics–a review. J. Istanbul Univ. Fac. Dent. 2017, 51, S128–S137. [Google Scholar] [CrossRef]
- Parirokh, M.; Torabinejad, M.; Dummer, P.M.H. Mineral trioxide aggregate and other bioactive endodontic cements: An updated overview - part I: Vital pulp therapy. Int. Endod. J. 2018, 51, 177–205. [Google Scholar] [CrossRef]
- Torabinejad, M.; Parirokh, M.; Dummer, P.M.H. Mineral trioxide aggregate and other bioactive endodontic cements: An updated overview-part II: Other clinical applications and complications. Int. Endod. J. 2018, 51, 284–317. [Google Scholar] [CrossRef] [PubMed]
- Malkondu, Ö.; Karapinar-Kazandağ, M.; Kazazoğlu, E. A review on biodentine, a contemporary dentine replacement and repair material. Biomed. Res. Int. 2014, 2014, 160951. [Google Scholar] [CrossRef]
- Debelian, G.; Trope, M. The use of premixed bioceramic materials in endodontics. G. Italia. Endod. 2016, 30, 70–80. [Google Scholar] [CrossRef]
- Ekambaram, M.; Yiu, C.K.Y.; Matinlinna, J.P. Bonding of adhesive resin to intraradicular dentine: A review of the literature. Int. J. Adhes. Adhes. 2015, 60, 92–103. [Google Scholar] [CrossRef]
- Dental Endodontics Market (Product-Instruments (Endodontic Scalers & Lasers, Motors, Apex Locators, and Machine Assisted Obturation Systems) and Consumables (Obturation, Shaping and Cleaning, and Access Cavity Preparation); End User: Dental Hospitals, Dental Clinics, and Dental Academic & Research Institutes)-Global Industry Analysis, Size, Share, Growth, Trends, and Forecast 2017–2025. Dental Endodontics Market Size, Share & Trend|Industry Analysis Report, 2025. Available online: transparencymarketresearch.com (accessed on 6 April 2021).
- Endodontic Devices Market Size, Share & Trends Analysis Report By Type (Instruments, Consumables), By End Use (Hospitals, Clinics, Dental Academic & Research Institutes), And Segment Forecasts, 2019–2026. Endodontic Devices Market Size & Share|Industry Report, 2019–2026. Available online: grandviewresearch.com (accessed on 6 April 2021).
- Dental Consumables Market by Product [Dental Implants (Root Form Dental Implants and Plate Form Dental Implants), Dental Prosthetics (Crowns, Bridges, Dentures, Abutments, Veneers, and Inlays & Onlays), Endodontics (Endodontic Files, Obturators, and Permanent Endodontic Sealers), Orthodontics (Brackets, Archwires, Anchorage Appliances, and Ligatures), Periodontics (Dental Sutures and Dental Hemostats), Retail Dental Care Essentials (Specialized Dental Pastes, Dental Brushes, Dental Wash Solutions, Whitening Agents, and Dental Floss), and Other Dental Consumables (Dental Splints, Dental Sealants, Dental Burs, Dental Impression Materials, Dental Disposables, Bonding Agents, Patient Bibs, and Aspirator Tubes & Saliva Ejectors)]-Global Opportunity Analysis and Industry Forecast, 2017–2023. Dental Consumables Market Size, Share and Growth opportunities 2023. Available online: alliedmarketresearch.com (accessed on 6 April 2021).
- Endodontics Market by Instruments (Scalers, Apex Locator, Motors, Handpiece, Laser), Consumables (Access Cavity Preparation, Endodontic Files, Burs, Drill, Lubricant, Obturation), End User (Clinic, Hospital)-Global Forecast to 2022. Endodontics Market by Consumables & End User | Global Forecast 2022. Available online: marketsandmarkets.com (accessed on 6 April 2021).
- Ferreira, C.M.; Silva, J.B.A., Jr.; Monteiro de Paula, R.C.; Andrade Feitosa, J.P.; Negreiros Cortez, D.G.; Zaia, A.A.; de Souza-Filho, F.J. Brazilian gutta-percha points. Part I: Chemical composition and X-ray diffraction analysis. Braz. Oral Res. 2005, 19, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Dobrzańska, J.; Gołombek, K.; Dobrzański, L.B. Polymer materials used in endodontic treatment–in vitro testing. AMSE 2012, 58, 110–115. [Google Scholar]
- Dobrzańska, J. Analiza Szczelności Wypełnień Kanałów Korzeniowych. Ph.D. Thesis, Śląski Uniwersytet Medyczny w Katowicach, Zabrze, Poland, 2011. [Google Scholar]
- Schilder, H.; Goodman, A.; Winthrop, A. The termomechanical properties of gutta-percha. Determination of phase transition temperatures for gutta-percha, Oral Surg. Oral Med. Oral Pathol. 1974, 38, 109–114. [Google Scholar] [CrossRef]
- Ferreira, C.M.; Gurgel-Filho, E.D.; Silva, J.B.A., Jr.; Monteiro de Paula, R.C.; Pessoa Andrade Feitosa, J.; Figueiredo de Almeida Gomes, B.P.; de Souza-Filho, F.J. Brazilian gutta-percha points. Part II: Thermal properties. Braz. Oral Res. 2007, 21, 29–34. [Google Scholar] [CrossRef]
- Combe, E.C.; Cohen, B.D.; Cumming, K. Alpha- and beta-forms of gutta-percha in products for root canal filling. Int. Endodon. J. 2001, 34, 447–451. [Google Scholar] [CrossRef]
- Tully, J. A Victorian Ecological Disaster: Imperialism, the Telegraph, and Gutta-Percha. J. World Hist. 2009, 20, 559–579. [Google Scholar] [CrossRef]
- Schilder, H. Filling root canals in three dimensions. Dent. Clin. North Am. 1967, 32, 723–744. [Google Scholar] [CrossRef]
- Buchanan, L.S. The continuous wave of condensation technique: A convergence of conceptual and procedural advances in obturation. Dent. Today 1994, 13, 84–85. [Google Scholar]
- Hand, R.E.; Huget, E.F.; Tsakinis, P.J. Effects of a warm gutta-percha technique on the lateral periodontium. Oral Surg. Oral Med. Oral Pathol. 1976, 42, 395–401. [Google Scholar] [CrossRef]
- Nahmias, Y.; Mab, T.; Dovgan, J.S. The Thermo Hydraulic Condensation Technique. Oral Health 2001, 91, 11–15. [Google Scholar]
- Nahmias, Y.; Serota, K.S.; Watson Jr, W.R. Predictable Endodontic Success: Part II -Microstructural Replication. Available online: http://www.ecoweek.ca/issues/PrinterFriendly.asp?aid=1000156065&RType=&PC=&issue=12012003 (accessed on 6 April 2021).
- Barattolo, R.; Santarcangelo, F. Otturazione del sistema dei canali radicolari con guttaperca termoplasticizzata: Principi, materiali e tecniche. G. Italia. Endod. 2011, 25, 112–124. [Google Scholar] [CrossRef][Green Version]
- Nahmias, Y.; Mab, T.; Dovgan, J.S. La tecnica di condensazione termoidraulica. L’infor. Endod. 2002, 5, 28–33. [Google Scholar]
- Nahmias, Y.; Bery, P. Due radici palatine nei primi molari superiori. L’infor. Endod. 2007, 10, 48–51. [Google Scholar]
- Carvalho-Sousa, B.; Almeida-Gomes, F.; Carvalho, P.R.; Maníglia-Ferreira, C.; Gurgel-Filho, E.D.; Albuquerque, D.S. Filling lateral canals: Evaluation of different filling techniques. Eur. J. Dent. 2010, 4, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, J.F.; Roças, I.N.; Favieri, A.; Abad, E.C.; Castro, A.J.; Gahyva, S.M. Bacterial leakage in coronally unsealed root canals obturated with 3 different techniques. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2000, 90, 647–650. [Google Scholar] [CrossRef]
- Limkangwalmongkol, S.; Burtscher, P.; Abbot, P.; Sandler, A.; Bishop, B. A comparative study of the apical leakage of four root canals sealers and laterally condensed gutta percha. J. Endod. 1991, 17, 495–499. [Google Scholar] [CrossRef]
- Swanson, K.; Madison, S. An evaluation of coronal microleakage in endodontically treated teeth. Part 1. Time periods. J. Endod. 1987, 13, 56–59. [Google Scholar] [CrossRef]
- Friedman, S.; Torneck, C.; Komorowsji, R.; Ouzounian, Z.; Syrtash, P.; Kaufman, A. In vivo model for assessing the functional efficacy of endodontic materials and techniques. J. Endod. 1997, 23, 557–561. [Google Scholar] [CrossRef]
- Torabinejad, M.; Ung, B.; Kettering, J. In vitro bacterial penetration of coronally unsealed endodontically treated teeth. J. Endod. 1990, 16, 566–569. [Google Scholar] [CrossRef]
- Shipper, G.; Trope, M. In vitro microbial leakage of endodontically treated teeth using new and standard obturation techniques. J Endod 2004, 30, 154–158. [Google Scholar] [CrossRef] [PubMed]
- Magura, M.E.; Kafrawy, A.H.; Brown, C.E.; Newton, C.W. Human saliva coronal microleakeage in obturated root canals: An in vitro study. J. Endod. 1991, 17, 324–331. [Google Scholar] [CrossRef]
- Oliver, C.; Abbott, P. An in vitro study of apical and coronal micro leakage of laterally condensed gutta-percha with Ketac-Endo and AH-26. Aust. Dent. J. 1998, 43, 262–268. [Google Scholar] [CrossRef] [PubMed]
- Madison, S.; Wilcox, L. An evaluation of coronal microleakge in endodontically treated teeth. Part III. In vivo study. J. Endod. 1988, 14, 455–458. [Google Scholar] [CrossRef]
- Khayat, A.; Lee, S.J.; Torabinejad, M. Human saliva penetration of coronally unsealed obturated root canals. J. Endod. 1993, 19, 458–461. [Google Scholar] [CrossRef]
- Jafari, F.; Jafari, S. Importance and methodologies of endodontic microleakage studies: A systematic review. J. Clin. Exp. Dent. 2017, 9, e812–e819. [Google Scholar] [CrossRef][Green Version]
- Møller, L.; Wenzel, A.; Wegge-Larsen, A.M.; Ding, M.; Væth, M.; Hirsch, E.; Kirkevang, L.-L. Comparison of images from digital intraoral receptors and cone beam computed tomography scanning for detection of voids in root canal fillings: An in vitro study using micro-computed tomography as validation. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 115, 810–818. [Google Scholar] [CrossRef]
- Imura, N.; Kato, A.S.; Hata, G.I.; Uemura, M.; Toda, T.; Weine, F. A comparison of the relative efficacies of four hand and rotary instrumentation techniques during endodontic retreatment. Int. Endod. J. 2000, 33, 361–366. [Google Scholar] [CrossRef]
- Ferreira, J.J.; Rhodes, J.S.; Pitt Ford, T.R. The efficacy of gutta-percha removal using ProFiles. Int. Endod. J. 2001, 34, 267–274. [Google Scholar] [CrossRef]
- Li, G.H.; Niu, L.N.; Selem, L.C.; Eid, A.A.; Bergeron, B.E.; Chen, J.H.; Pashley, D.H.; Tay, F.R. Quality of obturation achieved by an endodontic core-carrier system with crosslinked gutta-percha carrier in single-rooted canals. J. Dent. 2014, 42, 1124–1134. [Google Scholar] [CrossRef] [PubMed]
- Donnermeyer, D.; Bürklein, S.; Dammaschke, T.; Schäfer, E. Endodontic sealers based on calcium silicates: A systematic review. Odontol. 2019, 107, 421–436. [Google Scholar] [CrossRef]
- Gandolfi, M.G.; Siboni, F.; Prati, C. Properties of a novel polysiloxane-guttapercha calcium silicate-bioglass-containing root canal sealer. Dent. Mater. 2016, 32, e113–e126. [Google Scholar] [CrossRef] [PubMed]
- Zoufan, K.; Jiang, J.; Komabayashi, T.; Wang, Y.-H.; Safavi, K.E.; Zhu, Q. Cytotoxicity evaluation of Gutta Flow and Endo Sequence BC sealers. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2011, 112, 657–661. [Google Scholar] [CrossRef] [PubMed]
- Zmener, O. Tissue response to a new methacrylate-based root canal sealer: Preliminary observations in the subcutaneous connective tis- sues of rats. J. Endod. 2004, 30, 348–351. [Google Scholar] [CrossRef]
- Friedman, S.; Löst, C.; Zarrabian, M.; Trope, M. Evaluation of success and failure after endodontic therapy using a glass ionomer cement sealer. J. Endod. 1995, 21, 384–390. [Google Scholar] [CrossRef]
- Lee, K.W.; Williams, M.C.; Camps, J.J.; Pashley, D.H. Adhesion of endodontic sealers to dentin and gutta-percha. J. Endod. 2002, 28, 684–688. [Google Scholar] [CrossRef]
- Gatwood, R.S. Endodontic materials. Dent. Clin. North Am. 2007, 15, 695–712. [Google Scholar] [CrossRef]
- Shipper, G.; Ørstavik, D.; Teixeira, F.B.; Trope, M. An evaluation of microbial leakage in roots filled with a thermoplastic synthetic polymer-based root canal filling material (Resilon). J. Endod. 2004, 30, 342–347. [Google Scholar] [CrossRef] [PubMed]
- Resilon™ Obturation Material-The New Standard of Care? Available online: https://www.endoexperience.com/filecabinet/Clinical%20Endodontics/Obturation/Resilon/Resilon.Fact.Sheet.pdf (accessed on 1 April 2021).
- Lipski, M.; Woźniak, K.; Buczkowska-Radlińska, J.; Łagocka, R.; Bochińska, J.; Nowicka, A. Resilon i Epiphany nowy materiał do wypełniania kanałów korzeniowych zębów: Badania wstępne w SEM. Mag. Stomat. 2005, 9, 108–112. [Google Scholar]
- Lotfi, M.; Ghasemi, N.; Rahimi, S.; Vosoughhosseini, S.; Saghiri, M.A.; Shahidi, A. Resilon: A comprehensive literature review. J. Dent. Res. Dent. Clin. Dent. Prospects 2013, 7, 119–130. [Google Scholar] [CrossRef] [PubMed]
- Pawińska, M.; Kierklo, A.; Marczuk-Kolada, G. New technology in endodontics—the Resilon-Epiphany system for obturation of root canals. Adv. Med. Sci. 2006, 51 (Suppl. 1), 154–157. [Google Scholar]
- Pocket Dentistry. Gutta-percha Substitute: Resilon. Available online: https://pocketdentistry.com/33-gutta-percha-substitute-resilon/ (accessed on 1 April 2021).
- Mohammadi, Z.; Jafarzadeh, H.; Shalavi, S.; Bhandi, S.; Kinoshita, J. Resilon: Review of a New Material for Obturation of the Canal. J. Contemp. Dent. Pract. 2015, 16, 407–414. [Google Scholar] [CrossRef]
- Barnett, F.; Trope, M. Resilon™: A novel material to replace gutta-percha. Contemp. Endod. 2004, 1, 16–19. [Google Scholar]
- Hammad, M.; Qualtrough, A.; Silikas, N. Effect of a new obturating material on vertical root fracture resistance of endodontically treated teeth. J. Endod. 2007, 33, 732–736. [Google Scholar] [CrossRef]
- Teixeira, F.B.; Teixeira, E.C.N.; Thompson, J.Y.; Leinfelder, K.F.; Trope, M. Dentinal bonding reaches the root canal system. J. Esthet. Restor. Dent. 2004, 16, 348–354. [Google Scholar] [CrossRef]
- Shipper, G.; Teixeira, F.B.; Arnold, R.R.; Trope, M. Periapical inflammation after coronal microbial inoculation of dog roots filled with gutta-percha or resilon. J. Endod. 2005, 31, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, D.; Wei, X.; Wu, W.-C.; Ling, J.-Q. Resilon: A methacrylate resin-based obturation system. J. Dent. Sci. 2010, 5, 47–52. [Google Scholar] [CrossRef][Green Version]
- Resende, L.M.; Rached-Junior, F.J.; Versiani, M.A.; Souza-Gabriel, A.E.; Miranda, C.E.; Silva-Sousa, Y.T.; Sousa Neto, M.D. A comparative study of physicochemical properties of AH Plus, Epiphany, and Epiphany SE root canal sealers. Int. Endod. J. 2009, 42, 785–793. [Google Scholar] [CrossRef]
- Rocha, A.W.; de Andrade, C.D.; Leitune, V.C.; Collares, F.M.; Samuel, S.M.; Grecca, F.S.; de Figueiredo, J.A.; dos Santos, R.B. Influence of endodontic irrigants on resin sealer bond strength to radicular dentin. Bull. Tokyo Dent. Coll. 2012, 53, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Strange, K.A.; Tawil, P.Z.; Phillips, C.; Walia, H.D.; Fouad, A.F. Long-term Outcomes of Endodontic Treatment Performed with Resilon/Epiphany. J. Endod. 2019, 45, 507–512. [Google Scholar] [CrossRef]
- Pawińska, M.; Kierklo, A.; Tokajuk, G.; Sidun, J. New endodontic obturation systems and their interfacial bond strength with intraradicular dentine-ex vivo studies. Adv. Med. Sci. 2011, 56, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Kqiku, L.; Miletic, I.; Gruber, H.J.; Anic, I.; Städtler, P. Dichtigkeit von Wurzelkanalfüllungen mit GuttaFlow und Resilon im Vergleich zur lateralen Kondensation. Wien Med. Wochenschr. 2010, 160, 230–234. [Google Scholar] [CrossRef]
- Shokouhinejad, N.; Sabeti, M.A.; Hasheminasab, M.; Shafiei, F.; Shamshiri, A.R. Push-out bond strength of Resilon/Epiphany self-etch to intraradicular dentin after retreatment: A preliminary study. J. Endod. 2010, 36, 493–496. [Google Scholar] [CrossRef]
- De-Deus, G.; Namen, F.; Galan Jr, J.; Zehnder, M. Soft chelating irrigation protocol optimizes bonding quality of Resilon/Epiphany root fillings. J. Endod. 2008, 34, 703–705. [Google Scholar] [CrossRef] [PubMed]
- Üreyen Kaya, B.; Keçeci, A.D.; Orhan, H.; Belli, S. Micropush-out bond strengths of gutta-percha versus thermoplastic synthetic polymer-based systems—an ex vivo study. Int. Endod. J. 2008, 41, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Fisher, M.A.; Berzins, D.W.; Bahcall, J.K. An in vitro comparison of bond strength of various obturation materials to root canal dentin using a push-out test design. J. Endod. 2007, 33, 856–858. [Google Scholar] [CrossRef]
- Sly, M.M.; Moore, B.K.; Platt, J.A.; Brown, C.E. Push-out bond strength of a new endodontic obturation system (Resilon/Epiphany). J. Endod. 2007, 33, 160–162. [Google Scholar] [CrossRef]
- Dumani, A.; Yoldas, O.; Isci, A.S.; Köksal, F.; Kayar, B.; Polat, E. Disinfection of artificially contaminated Resilon cones with chlorhexidine and sodium hypochlorite at different time exposures. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 103, e82–e85. [Google Scholar] [CrossRef]
- Shokouhinejad, N.; Sharifian, M.R.; Jafari, M.; Sabeti, M.A. Push-out bond strength of Resilon/Epiphany self-etch and gutta-percha/AH26 after different irrigation protocols. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 110, e88–e92. [Google Scholar] [CrossRef] [PubMed]
- Kumar, N.; Aggarwal, V.; Singla, M.; Gupta, R. Effect of various endodontic solutions on punch out strength of Resilon under cyclic loading. J. Conserv. Dent. 2011, 14, 366–369. [Google Scholar] [CrossRef] [PubMed]
- Tay, F.R.; Loushine, R.J.; Weller, R.N.; Kimbrough, W.F.; Pashley, D.H.; Mak, Y.F.; Lai, C.N.; Raina, R.; Williams, M.C. Ultrastructural evaluation of the apical seal in roots filled with a polycaprolactone-based root canal filling material. J. Endod. 2005, 31, 514–519. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.J.; Jee, S.W.; Song, J.S.; Jung, I.Y.; Cha, J.H.; Kim, E. Comparison of regrowth of Enterococcus faecalis in dentinal tubules after sealing with gutta-percha or Resilon. J. Endod. 2008, 34, 445–448. [Google Scholar] [CrossRef] [PubMed]
- Jack, R.M.; Goodell, G.G. In vitro comparison of coronal microleakage between Resilon alone and gutta-percha with a glass ionomer intraorifice barrier using a fluid filtration model. J. Endod. 2008, 34, 718–720. [Google Scholar] [CrossRef]
- Santos, J.; Tjäderhane, L.; Ferraz, C.; Zaia, A.; Alves, M.; De Goes, M.; Carrilho, M. Long-term sealing ability of resin-based root canal fillings. Int. Endod. J. 2010, 43, 455–460. [Google Scholar] [CrossRef]
- Shemesh, H.; Wu, M.K.; Wesselink, P.R. Leakage along the apical root fillings with and without smear layer using two different leakage models: A two month longitudinal ex vivo study. Int. Endod. J. 2006, 39, 968–976. [Google Scholar] [CrossRef]
- De Bruyne, M.A.; De Moor, R.J. Long-term sealing ability of Resilon apical root-end fillings. Int. Endod. J. 2009, 42, 884–892. [Google Scholar] [CrossRef]
- Deus, G.A.D.; Fábio, M.; Rocha, L.A.C.M.; Gurgel-Filho, E.D.; Maniglia, C.F.; Coutinho-Filho, T. Analysis of the film thickness of a root canal sealer following three obturation techniques. Pesqui Odontol. Bras. 2003, 17, 119–125. [Google Scholar] [CrossRef][Green Version]
- Paqué, F.; Sirtes, G. Apical sealing ability of Resilon/Epiphany versus gutta-percha/AH Plus: Immediate and 16 month leakage. Int. Endod. J. 2007, 40, 722–729. [Google Scholar] [CrossRef] [PubMed]
- Pasqualini, D.; Scotti, N.; Mollo, L.; Berutti, E.; Angelini, E.; Migliaretti, G.; Cuffini, A.; Adlerstein, D. Microbial leakage of Gutta-Percha and Resilon root canal filling material: A comparative study using a new homogeneous assay for sequence detection. J. Biomater. Appl. 2008, 22, 337–352. [Google Scholar] [CrossRef] [PubMed]
- Shemesh, H.; Souza, E.M.; Wu, M.K.; Wesselink, P.R. Glucose reactivity with filling materials as a limitation for using the glucose leakage model. Int. Endod. J. 2008, 41, 869–872. [Google Scholar] [CrossRef]
- Kokorikos, I.; Kolokouris, I.; Economides, N.; Gogos, C.; Helvatjoglu-Antoniades, M. Long-term evaluation of the sealing ability of two root canal sealers in combination with self-etching bonding agents. J. Adhes. Dent. 2009, 11, 239–246. [Google Scholar] [PubMed]
- Onay, E.O.; Ungor, M.; Orucoglu, H. An in vitro evaluation of the apical sealing ability of a new resin based root canal obturation system. J. Endod. 2006, 32, 976–978. [Google Scholar] [CrossRef] [PubMed]
- Hirai, V.H.; da Silva Neto, U.X.; Westphalen, V.P.D.; Perin, C.P.; Carneiro, E.; Fariniuk, L.F. Comparative analysis of leakage in root canal filling performed with gutta-percha and Resilon cones with AH Plus and Epiphany sealers. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 109, 131–135. [Google Scholar] [CrossRef]
- Saleh, I.M.; Ruyter, I.E.; Haapasalo, M.; Ørstavik, D. Bacterial penetration along different root canal filling materials in the presence or absence of smear layer. Int. Endod. J. 2008, 41, 32–40. [Google Scholar] [CrossRef]
- De-Deus, G.; Namen, F.; Galan, J. Reduced long-term sealing ability of adhesive root fillings after water-storage stress. J. Endod. 2008, 34, 322–325. [Google Scholar] [CrossRef]
- Pandey, P.; Aggarwal, H.; Tikku, A.P.; Singh, A.; Bains, R.; Mishra, S. Comparative evaluation of sealing ability of gutta percha and resilon as root canal filling materials- a systematic review. J Oral Biol Craniofac Res 2020, 10, 220–226. [Google Scholar] [CrossRef]
- Barborka, B.J.; Woodmansey, K.F.; Glickman, G.N.; Schneiderman, E.; He, J. Long-term Clinical Outcome of Teeth Obturated with Resilon. J. Endod. 2017, 43, 556–560. [Google Scholar] [CrossRef]
- Lyons, W.W.; Hartwell, G.R.; Stewart, J.T.; Reavley, B.; Appelstein, C.; Lafkowitz, S. Comparison of coronal bacterial leakage between immediate versus delayed post-space preparations in root canals filled with Resilon/Epiphany. Int. Endod. J. 2009, 42, 203–207. [Google Scholar] [CrossRef] [PubMed]
- Silveira, F.F.; Soares, J.A.; Nunes, E.; Mordente, V.L. Negative influence of continuous wave technique on apical sealing of the root canal system with Resilon. J. Oral Sci. 2007, 49, 121–128. [Google Scholar] [CrossRef] [PubMed][Green Version]
- De-Deus, G.; Audi, C.; Murad, C.; Fidel, S.; Fidel, R.A. Sealing ability of oval-shaped canals filled using the System B heat source with either gutta-percha or Resilon: An ex vivo study using a polymicrobial leakage model. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 104, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, G.; Zehnder, M.; Paqué, F. Enterococcus faecalis type strain leakage through root canals filled with Gutta-Percha/AH plus or Resilon/Epiphany. J. Endod. 2007, 33, 45–47. [Google Scholar] [CrossRef] [PubMed]
- Hollanda, A.C.B.; Estrela, C.R.; Decurcio, D.A.; Silva, J.A.; Estrela, C. Sealing ability of three commercial resin-based endodontic sealers. Gen. Dent. 2009, 57, 368–373. [Google Scholar]
- Kocak, M.M.; Er, O.; Saglam, B.C.; Yaman, S. Apical leakage of epiphany root canal sealer combined with different master cones. Eur. J. Dent. 2008, 2, 91–95. [Google Scholar] [CrossRef]
- Bodrumlu, E.; Tunga, U. The apical sealing ability of a new root canal filling material. Am. J. Dent. 2007, 20, 295–298. [Google Scholar]
- Raina, R.; Loushine, R.J.; Weller, R.N.; Tay, F.R.; Pashley, D.H. Evaluation of the quality of the apical seal in Resilon/ Epiphany and gutta-percha/AH Plus-filled root canals by using a fluid filtration approach. J. Endod. 2007, 33, 944–947. [Google Scholar] [CrossRef]
- Pitout, E.; Oberholzer, T.G.; Blignaut, E.; Molepo, J. Coronal leakage of teeth root-filled with gutta-percha or Resilon root canal filling material. J. Endod. 2006, 32, 610–615. [Google Scholar] [CrossRef]
- Fransen, J.N.; He, J.; Glickman, G.N.; Rios, A.; Shulman, J.D.; Honeyman, A. Comparative assessment of ActiV GP/glass ionomer sealer, Resilon/Epiphany, and gutta-percha/AH plus obturation: A bacterial leakage study. J. Endod. 2008, 34, 725–727. [Google Scholar] [CrossRef]
- Shokouhinejad, N.; Sharifian, M.R.; Aligholi, M.; Assadian, H.; Tabor, R.K.; Nekoofar, M.H. The sealing ability of Resilon and gutta-percha following different smear layer removal methods: An ex vivo study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 110, 45–49. [Google Scholar] [CrossRef]
- Kangarlou, A.; Dianat, O.; Esfahrood, Z.R.; Asharaf, H.; Zandi, B.; Eslami, G. Bacterial leakage of GuttaFlow-filled root canals compared with Resilon/Epiphany and Gutta-percha/AH26-filled root canals. Aust. Endod. J. 2012, 38, 10–13. [Google Scholar] [CrossRef]
- Biggs, S.C.; Knowles, K.I.; Ibarrola, J.L.; Pashley, D.H. An in vitro assessment of the sealing ability of Resilon/Epiphany using a fluid filtration. J. Endod. 2006, 32, 759–761. [Google Scholar] [CrossRef]
- Karapınar-Kazandağ, M.; Tanalp, J.; Bayrak, Ö.F.; Sunay, H.; Bayirh, G. Microleakage of various root filling systems by glucose filtration analysis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 109, e96–e102. [Google Scholar] [CrossRef]
- Oddoni, P.G.; Mello, I.; Coil, J.M.; Antoniazzi, J.H. Coronal and apical leakage analysis of two different root canal obturation systems. Braz. Oral Res. 2008, 22, 211–215. [Google Scholar] [CrossRef]
- De Almeida-Gomes, F.; Maniglia-Ferreira, C.; de Morais Vitoriano, M.; Carvalho-Sousa, B.; Guimaraes, N.L.; dos Santos, R.A.; Gurgel-Filho, E.D.; Rocha, M.M. Ex vivo evaluation of coronal and apical microbial leakage of root canal--filled with gutta-percha or Resilon/Epiphany root canal filling material. Indian J. Dent. Res. 2010, 21, 98–103. [Google Scholar] [CrossRef]
- Üreyen Kaya, B.; Keçeci, A.D.; Belli, S. Evaluation of the sealing ability of gutta-percha and thermoplastic synthetic polymer-based systems along the root canals through the glucose penetration model. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 104, E66–E73. [Google Scholar] [CrossRef]
- Dultra, F.; Barroso, J.M.; Carrasco, L.D.; Capelli, A.; Guerisoli, D.M.; Pécora, J.D. Evaluation of apical microleakage of teeth sealed with four different canal sealers. J. Appl. Oral Sci. 2006, 14, 341–345. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, H.R.; Saravia-Lemus, G.A.; Florián, W.E.; Lainfiesta, J.F. Microbial leakage of Enterococcus faecalis after post space preparation in teeth filled in vivo with RealSeal versus gutta-percha. J. Endod. 2007, 33, 674–675. [Google Scholar] [CrossRef] [PubMed]
- Tanomaru-Filho, M.; Sant’anna-Junior, A.; Bosso, R.; Guerreiro-Tanomaru, J.M. Effectiveness of gutta-percha and Resilon in filling lateral root canals using the Obtura II system. Braz. Oral Res. 2011, 25, 205–209. [Google Scholar] [CrossRef] [PubMed]
- Bodrumlu, E.; Tunga, U. Coronal sealing ability of a new root canal filling material. J. Can. Dent. Assoc. 2007, 73, 623. [Google Scholar] [PubMed]
- Sharifian, M.R.; Shokouhinejad, N.; Aligholi, M.; Jafari, Z. Effect of chlorhexidine on coronal microleakage from root canals obturated with Resilon/Epiphany Self-Etch. J. Oral Sci. 2010, 52, 83–87. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Bodrumlu, E.; Tunga, U. Apical leakage of Resilon obturation material. J. Contemp. Dent. Pract. 2006, 7, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Verissimo, D.M.; do Vale, M.S.; Monteiro, A.J. Comparison of apical leakage between canals filled with gutta-percha/AH-plus and Resilon/Epiphany System, when submitted to two filling techniques. J. Endod. 2007, 33, 291–294. [Google Scholar] [CrossRef]
- Moura-Netto, C.; Pinto, T.; Davidowicz, H.; de Moura, A.A.M. Apical leakage of three resin-based endodontic sealers after 810-nm-diode laser irradiation. Photomed. Laser Surg. 2009, 27, 891–894. [Google Scholar] [CrossRef]
- Wedding, J.R.; Brown, C.E.; Legan, J.J.; Moore, B.K.; Vail, M.M. An in vitro comparison of micro leakage between Resilon and gutta-percha with a fluid filtration model. J. Endod. 2007, 33, 1447–1449. [Google Scholar] [CrossRef]
- Ishimura, H.; Yoshioka, T.; Suda, H. Sealing ability of new adhesive root canal filling materials measured by new dye penetration method. Dent. Mater. J. 2007, 26, 290–295. [Google Scholar] [CrossRef]
- Nawal, R.R.; Parande, M.; Sehgal, R.; Rao, N.R.; Naik, A. A comparative evaluation of 3 root canal filling systems. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2011, 111, 387–393. [Google Scholar] [CrossRef]
- Punia, S.K.; Nadig, P.; Punia, V. An in vitro assessment of apical microleakage in root canals obturated with guttaflow, Resilon, thermafil and lateral condensation: A stereomicroscopic study. J. Conserv. Dent. 2011, 14, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Tunga, U.; Bodrumlu, E. Assessment of the sealing ability of a new root canal obturation material. J. Endod. 2006, 32, 876–878. [Google Scholar] [CrossRef] [PubMed]
- Shashidhar, C.; Shivanna, V.; Shivamurthy, G.; Shashidhar, J. The comparison of microbial leakage in roots filled with resilon and gutta-percha: An in vitro study. J. Conserv. Dent. 2011, 14, 21–27. [Google Scholar] [CrossRef]
- Sagsen, B.; Er, O.; Kahraman, Y.; Orucoglu, H. Evaluation of micro leakage of roots filled with different techniques with a computerized fluid filtration technique. J. Endod. 2006, 32, 1168–1170. [Google Scholar] [CrossRef] [PubMed]
- Kqiku, L.; Städtler, P.; Gruber, H.J.; Baraba, A.; Anic, I.; Miletic, I. Active versus passive microleakage of Resilon/Epiphany and gutta-percha/AH Plus. Aust. Endod. J. 2011, 37, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Aptekar, A.; Ginnan, K. Comparative analysis of microleakage and seal for two obturation materials: Resilon/Epiphany and gutta-percha. J. Can. Dent. Assoc. 2006, 72, 245. [Google Scholar] [PubMed]
- Stratton, R.K.; Apicella, M.J.; Mines, P. A fluid filtration comparison of gutta-percha versus Resilon, a new soft resin endodontic obturation system. J. Endod. 2006, 32, 642–645. [Google Scholar] [CrossRef]
- Kurtzman, G.M. Resilon Update. Inside Dent. 2007, 3, 1–5. [Google Scholar]
- Mohammadi, Z.; Khademi, A. An evaluation of the sealing ability of MTA and Resilon: A bacterial leakage study. Iran Endod. J. 2007, 2, 43–46. [Google Scholar] [PubMed]
- Maltezos, C.; Glickman, G.N.; Ezzo, P.; He, J. Comparison of the sealing of Resilon, Pro Root MTA, and Super-EBA as root-end filling materials: A bacterial leakage study. J. Endod. 2006, 32, 324–327. [Google Scholar] [CrossRef] [PubMed]
- Nagas, E.; Cehreli, Z.C.; Durmaz, V.; Vallittu, P.K.; Lassila, L.V. Regional push-out bond strength and coronal microleakage of Resilon after different light-curing methods. J. Endod. 2007, 33, 1464–1468. [Google Scholar] [CrossRef] [PubMed]
- Williamson, A.E.; Marker, K.L.; Drake, D.R.; Dawson, D.V.; Walton, R.E. Resin-based versus gutta-percha-based root canal obturation: Influence on bacterial leakage in an in vitro model system. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 108, 292–296. [Google Scholar] [CrossRef]
- Hanada, T.; Quevedo, C.G.; Okitsu, M.; Yoshioka, T.; Iwasaki, N.; Takahashi, H.; Suda, H. Effects of new adhesive resin root canal filling materials on vertical root fractures. Aust. Endod. J. 2010, 36, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Ulusoy, Ö.İ.A.; Nayır, Y.; Darendeliler-Yaman, S. Effect of different root canal sealers on fracture strength of simulated immature roots. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2011, 112, 544–547. [Google Scholar] [CrossRef] [PubMed]
- Shashidhar, J.; Shashidhar, C. Gutta percha verses resilon: An in vitro comparison of fracture resistance in endodontically treated teeth. J Indian Soc Pedod Prev Dent 2014, 32, 53–57. [Google Scholar] [CrossRef]
- Baba, S.M.; Grover, S.I.; Tyagi, V. Fracture resistance of teeth obturated with gutta percha and Resilon: An in vitro study. J. Conserv. Dent. 2010, 13, 61–64. [Google Scholar] [CrossRef] [PubMed]
- De Temiño Morante, P.R. ¿Es el Resilon el nuevo Material de Obturación Endodóntica? Available online: https://gacetadental.com/2011/10/es-el-resilon-el-nuevo-material-de-obturacin-endodntica-25262/ (accessed on 1 April 2021).
- Hemalatha, H.; Sandeep, M.; Kulkarni, S.; Yakub, S.S. Evaluation of fracture resistance in simulated immature teeth using Resilon and Ribbond as root reinforcements—an in vitro study. Dent. Traumatol. 2009, 25, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Sagsen, B.; Er, O.; Kahraman, Y.; Akdogan, G. Resistance to fracture of roots filled with three different techniques. Int. Endod. J. 2007, 40, 31–35. [Google Scholar] [CrossRef]
- Grande, N.M.; Plotino, G.; Lavorgna, L.; Ioppolo, P.; Bedini, R.; Pameijer, C.H.; Somma, F. Influence of different root canal-filling materials on the mechanical properties of root canal dentin. J. Endod. 2007, 33, 859–863. [Google Scholar] [CrossRef]
- Ribeiro, F.C.; Souza-Gabriel, A.E.; Marchesan, M.A.; Alfredo, E.; Silva-Sousa, Y.T.; Sousa-Neto, M.D. Influence of different endodontic filling materials on root fracture susceptibility. J. Dent. 2008, 36, 69–73. [Google Scholar] [CrossRef]
- Economides, N.; Koulaouzidou, E.A.; Gogos, C.; Kolokouris, I.; Beltes, P.; Antoniades, D. Comparative study of the cytotoxic effect of Resilon against two cell lines. Braz. Dent. J. 2008, 19, 291–295. [Google Scholar] [CrossRef][Green Version]
- Donadio, M.; Jiang, J.; He, J.; Wang, Y.H.; Safavi, K.E.; Zhu, Q. Cytotoxicity evaluation of Activ GP and Resilon sealers in vitro. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 107, e74–e78. [Google Scholar] [CrossRef]
- Susini, G.; About, I.; Tran-Hung, L.; Camps, J. Cytotoxicity of Epiphany and Resilon with a root model. Int. Endod. J. 2006, 39, 940–944. [Google Scholar] [CrossRef]
- Leonardo, M.R.; Barnett, F.; Debelian, G.J.; de Pontes Lima, R.K.; da Silva, L.A.B. Root canal adhesive filling in dogs’ teeth with or without coronal restoration: A histopathological evaluation. J. Endod. 2007, 33, 1299–1303. [Google Scholar] [CrossRef]
- Bodrumlu, E.; Muglali, M.; Sumer, M.; Guvenc, T. The response of subcutaneous connective tissue to a new endodontic filling material. J. Biomed. Mater. Res. B Appl. Biomater. 2008, 84, 463–467. [Google Scholar] [CrossRef] [PubMed]
- Merdad, K.; Pascon, A.E.; Kulkarni, G.; Santerre, P.; Friedman, S. Short-term cytotoxicity assessment of components of the epiphany resin-percha obturating system by indirect and direct contact millipore filter assays. J. Endod. 2007, 33, 24–27. [Google Scholar] [CrossRef]
- Onay, E.O.; Ungor, M.; Ozdemir, B.H. In vivo evaluation of the biocompatibility of a new resin-based obturation system. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 104, e60–e66. [Google Scholar] [CrossRef]
- Bodrumlu, E.; Alaçamm, T. The antimicrobial and antifungal activity of a root canal core material. J. Am. Dent. Assoc. 2007, 138, 1228–1232. [Google Scholar] [CrossRef] [PubMed]
- Gomes, B.P.; Berber, V.B.; Montagner, F.; Sena, N.T.; Zaia, A.A.; Ferraz, C.C.; Souza-Filho, F.J. Residual effects and surface alterations in disinfected gutta-percha and Resilon cones. J. Endod. 2007, 33, 948–951. [Google Scholar] [CrossRef] [PubMed]
- Cunha, R.S.; De Martin, A.S.; Barros, P.P.; da Silva, F.M.; de Castilho Jacinto, R.; da Silveira Bueno, C.E. In vitro evaluation of the cleansing working time and analysis of the amount of gutta-percha or Resilon remnants in the root canal walls after instrumentation for endodontic retreatment. J. Endod. 2007, 33, 1426–1428. [Google Scholar] [CrossRef]
- Fenoul, G.; Meless, G.D.; Pérez, F. The efficacy of R-Endo rotary NiTi and stainless steel hand instruments to remove gutta-percha and Resilon. Int. Endod. J. 2010, 43, 135–141. [Google Scholar] [CrossRef]
- Schirrmeister, J.F.; Meyer, K.M.; Hermanns, P.; Altenburger, M.J.; Wrbas, K.T. Effectiveness of hand and rotary instrumentation for removing a new synthetic polymer-based root canal obturation material (Epiphany) during retreatment. Int. Endod. J. 2006, 39, 150–156. [Google Scholar] [CrossRef]
- Marfisi, K.; Mercade, M.; Plotino, G.; Duran-Sindreu, F.; Bueno, R.; Roig, M. Efficacy of three different rotary files to remove gutta-percha and resilon from root canals. Int. Endod. J. 2010, 43, 1022–1028. [Google Scholar] [CrossRef]
- Zarei, M.; Shahrami, F.; Vatanpour, M. Comparison between gutta-percha and Resilon retreatment. J. Oral Sci. 2009, 51, 181–185. [Google Scholar] [CrossRef]
- Somma, F.; Cammarota, G.; Plotino, G.; Grande, N.M.; Pameijer, C.H. The effectiveness of manual and mechanical instrumentation for the retreatment of three different root canal filling materials. J. Endod. 2008, 34, 466–469. [Google Scholar] [CrossRef]
- Taşdemir, T.; Yildirim, T.; Celik, D. Comparative study of removal of current endodontic fillings. J. Endod. 2008, 34, 326–329. [Google Scholar] [CrossRef]
- Iizuka, N.; Takenaka, S.; Shigetani, Y.; Okiji, T. Removal of resin-based root canal filling materials with K3 rotary instruments: Relative efficacy for different combinations of filling materials. Dent. Mater. J. 2008, 27, 75–80. [Google Scholar] [CrossRef]
- Hassanloo, A.; Watson, P.; Finer, Y.; Friedman, S. Retreatment efficacy of the Epiphany soft resin obturation system. Int. Endod. J. 2007, 40, 633–643. [Google Scholar] [CrossRef]
- Tanomaru-Filho, M.; Orlando, T.A.; Bortoluzzi, E.A.; Silva, G.F.; Tanomaru, J.M. Solvent capacity of different substances on gutta-percha and Resilon. Braz. Dent. J. 2010, 21, 46–49. [Google Scholar] [CrossRef]
- Faria-Júnior, N.B.; Loiola, L.E.; Guerreiro-Tanomaru, J.M.; Berbert, F.L.; Tanomaru-Filho, M. Effectiveness of three solvents and two associations of solvents on gutta-percha and Resilon. Braz. Dent. J. 2011, 22, 41–44. [Google Scholar] [CrossRef] [PubMed]
- Bodrumlu, E.; Uzun, O.; Topuz, O.; Semiz, M. Efficacy of three techniques in removing root canal filling material. J. Can. Dent. Assoc. 2008, 74, 721. [Google Scholar] [PubMed]
- Ezzie, E.; Fleury, A.; Solomon, E.; Spears, R.; He, J. Efficacy of retreatment techniques for a resin based root canal obturation material. J. Endod. 2006, 32, 341–344. [Google Scholar] [CrossRef]
- Ring, J.; Murray, P.E.; Namerow, K.N.; Moldauer, B.I.; Garcia-Godoy, F. Removing root canal obturation materials: A comparison of rotary file systems and re-treatment agents. J. Am. Dent. Assoc. 2009, 140, 680–688. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, D.P.; Barbizam, J.V.; Trope, M.; Teixeira, F.B. Comparison between gutta-percha and Resilon removal using two different techniques in endodontic retreatment. J. Endod. 2006, 32, 362–364. [Google Scholar] [CrossRef]
- Azar, M.; Khojastehpour, L.; Iranpour, N. A comparison of the effectiveness of chloroform in dissolving Resilon and gutta-percha. J. Dent. (Tehran) 2011, 8, 19–24. [Google Scholar]
- Shanahan, D.J.; Duncan, H.F. Root canal filling using Resilon: A review. Br. Dent. J. 2011, 211, 81–88. [Google Scholar] [CrossRef]
- Steinke, H. Der Hippokratische Eid: Ein schwieriges Erbe. Horiz. Med. Schweiz. Ärztezeitung Bull. Médecins Suisses Boll. Med. Svizz. 2016, 97, 1699–1701. [Google Scholar]
- Dobrzańska, J.; Dobrzański, L.B.; Gołombek, K.; Dobrzański, L.A.; Dobrzańska-Danikiewicz, A.D. Results of in vitro experimental research assessing the tightness of filling materials with the pulp of extracted human teeth depending on the obturation techniques during endodontic treatment. Processes. (prepared for printing).
- Dobrzański, L.A.; Dobrzański, L.B.; Dobrzańska-Danikiewicz, A.D. Manufacturing technologies thick-layer coatings on various substrates and manufacturing gradient materials using powders of metals, their alloys and ceramics. JAMME 2020, 99, 14–41. [Google Scholar] [CrossRef]
- Dobrzańska-Danikiewicz, A.D.; Dobrzański, L.A.; Szindler, M.; Achtelik-Franczak, A.; Dobrzański, L.B. Obróbka powierzchni materiałów mikroporowatych wytworzonych metodą selektywnego spiekania laserowego w celu uefektywnienia proliferacji żywych komórek. In Metalowe Materiały Mikroporowate i Lite do Zastosowań Medycznych i Stomatologicznych; Dobrzański, L.A., Dobrzańska-Danikiewicz, A.D., Eds.; Open Access Library VII(1); International OCSCO World Press: Gliwice, Poland, 2017; pp. 289–375. [Google Scholar]
- Dobrzańska-Danikiewicz, A. The methodological fundaments of development state analysis of surface engineering technologies. JAMME 2010, 40, 203–210. [Google Scholar]
- Dobrzańska-Danikiewicz, A.D.; Hajduczek, E.; Polok-Rubiniec, M.; Przybył, M.; Adamaszek, K. Evaluation of selected steel thermochemical treatment technologies using foresight methods. JAMME 2011, 46, 115–146. [Google Scholar]
- Dobrzańska-Danikiewicz, A.D. The development perspectives of Physical Vapour Deposition technologies. JAMME 2012, 54, 103–109. [Google Scholar]
- Dobrzańska-Danikiewicz, A.D. Metodologia Komputerowo Zintegrowanego Prognozowania Rozwoju Inżynierii Powierzchni Materiałów; Dobrzański, L.A., Ed.; In Open Access Library 1(7); International OCSCO World Press: Gliwice, Poland, 2012; pp. 1–289. [Google Scholar]
- Dobrzańska-Danikiewicz, A.D. Księga Technologii Krytycznych Kształtowania Struktury i Własności Powierzchni Materiałów Inżynierskich; Dobrzański, L.A., Ed.; In Open Access Library 8(26); International OCSCO World Press: Gliwice, Poland, 2013; pp. 1–823. [Google Scholar]
- Dobrzańska-Danikiewicz, A.D. (Ed.) Materials Surface Engineering Development Trends; Open Access Library 6; International OCSCO World Press: Gliwice, Poland, 2011; pp. 1–594. [Google Scholar]
- Dobrzańska-Danikiewicz, A.D.; Dobrzański, L.A.; Sękala, A. Results of Technology Foresight in the Surface Engineering Area. AMM 2014, 657, 916–920. [Google Scholar] [CrossRef]
- Dobrzańska-Danikiewicz, A.D.; Dobrzański, L.A.; Mazurkiewicz, J.; Tomiczek, B.; Reimann, Ł. E-transfer of materials surface engineering e-foresight results. AMSE 2011, 52, 87–100. [Google Scholar]
- Dobrzańska-Danikiewicz, A.D.; Tański, T.; Malara, S.; Domagała-Dubiel, J. Technology Foresight Results Concerning Laser Surface Treatment of Casting Magnesium Alloys. In New Features on Magnesium Alloys; Monteiro, W.A., Ed.; IntechOpen: Rijeka, Croatia, 2012; pp. 1–30. [Google Scholar] [CrossRef]
- Dobrzańska-Danikiewicz, A.D. Foresight of Material Surface Engineering as a Tool Building a Knowledge-Based Economy. MSF 2012, 706–709, 2511–2516. [Google Scholar] [CrossRef]
- Dobrzański, L.A. (Ed.) 1st Workshop on Foresight of Surface Properties Formation Leading Technologies of Engineering Materials and Biomaterials; International OCSCO World Press: Gliwice, Poland, 2009; pp. 1–272. [Google Scholar]
- Dobrzański, L.A. (Ed.) 2nd Workshop on Foresight of Surface Properties Formation Leading Technologies of Engineering Materials and Biomaterials; International OCSCO World Press: Gliwice, Poland, 2009; pp. 1–324. [Google Scholar]
- Dobrzański, L.A.; Dobrzańska-Danikiewicz, A.D. (Eds.) 3rd Workshop on Foresight of Surface Properties Formation Leading Technologies of Engineering Materials and Biomaterials; Raport z realizacji zadania 2. “Analiza Istniejącej Sytuacji w Zakresie Rozwoju Technologii oraz Uwarunkowań Społeczno-Gospodarczych w Odniesieniu do Przedmioty Foresightu pt. FORSURF-Foresight Wiodących Technologii Kształtowania Własności Powierzchni Materiałów Inżynierskich i Biomedycznych”; International OCSCO World Press: Gliwice, Poland, 2010; pp. 1–184. [Google Scholar]
- Dobrzański, L.A.; Achtelik-Franczak, A. Struktura i własności tytanowych szkieletowych materiałów mikroporowatych wytworzonych metodą selektywnego spiekania laserowego do zastosowań w implantologii oraz medycynie regeneracyjnej. In Metalowe Materiały Mikroporowate i Lite do Zastosowań Medycznych i Stomatologicznych; Dobrzański, L.A., Dobrzańska-Danikiewicz, A.D., Eds.; Open Access Library VII(1); International OCSCO World Press: Gliwice, Poland, 2017; pp. 186–244. [Google Scholar]
- Dobrzański, L.A. Effect of heat and surface treatment on the structure and properties of the Mg-Al-Zn-Mn casting alloys. In Magnesium and Its Alloys; Dobrzański, L.A., Totten, G.E., Bamberger, M., Eds.; CRC Press: Boca Raton, FL, USA, 2019; pp. 91–202. [Google Scholar]
- Dobrzański, L.A.; Dobrzańska-Danikiewicz, A.D. Perspektywy i trendy rozwojowe inżynierii powierzchni materiałów. In Inżynieria Powierzchni Materiałów: Kompendium Wiedzy i Podręcznik Akademicki; Dobrzański, L.A., Ed.; Open Access Library VIII(1); International OCSCO World Press: Gliwice, Poland, 2018; pp. 89–157. [Google Scholar]
- Dobrzański, L.A.; Nieradka-Buczek, B. Transparent conductive nanocomposite layers with polymer matrix and silver nanowires reinforcement. AMSE 2018, 93, 59–84. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzańska-Danikiewicz, A.D.; Czuba, Z.P.; Dobrzański, L.B.; Achtelik-Franczak, A.; Malara, P.; Szindler, M.; Kroll, L. Metallic skeletons as reinforcement of new composite materials applied in orthopaedics and dentistry. AMSE 2018, 92, 53–85. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzański, L.B.; Dobrzańska-Danikiewicz, A.D.; Dobrzańska, J.; Rudziarczyk, K.; Achtelik-Franczak, A. Non-Antagonistic Contradictoriness of the Progress of Advanced Digitized Production with SARS-CoV-2 Virus Transmission in the Area of Dental Engineering. Processes 2020, 8, 1097. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzańska-Danikiewicz, A.; Achtelik-Franczak, A. The structure and properties of aluminium alloys matrix composite materials with reinforcement made of titanium skeletons. AMSE 2016, 80, 16–30. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Prokopiuk vel Prokopowicz, M. The influence of reduced graphene oxide on the structure of the electrodes and the properties of dye-sensitized solar cells. AMSE 2016, 77, 12–30. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Hudecki, A.; Chladek, G.; Król, W.; Mertas, A. Biodegradable and antimicrobial polycaprolactone nanofibers with and without silver precipitates. AMSE 2015, 76, 5–26. [Google Scholar]
- Dobrzański, L.A.; Hudecki, A. Structure, geometrical characteristics and properties of biodegradable micro- and polycaprolactone nanofibers. AMSE 2014, 70, 5–13. [Google Scholar]
- Dobrzański, L.A.; Pawlyta, M.; Hudecki, A. Conceptual study on a new generation of the high-innovative advanced porous and composite nanostructural functional materials with nanofibers. JAMME 2011, 49, 550–565. [Google Scholar]
- Dobrzańska-Danikiewicz, A.D.; Żmudzki, J. Development trends of mucous-borne dentures in the aspect of elastomers applications. AMSE 2012, 55, 5–13. [Google Scholar]
- Dobrzański, L.B. Struktura i Własności Materiałów Inżynierskich na Uzupełnienia Protetyczne Układu Stomatognatycznego Wytwarzane Metodami Przyrostowymi i Ubytkowymi. Ph.D. Thesis, Akademia Górniczo-Hutnicza im. Stanisława Staszica w Krakowie, Kraków, Poland, 2017. [Google Scholar]
- Rudziarczyk, K. Modelowanie Stanu Naprężeń w Wybranych Rodzajach Implantów Stomatologicznych Oraz w Otaczającej je Tkance Kostnej. Master’s Thesis, Politechnika Śląska, Gliwice, Poland, 2020. (manuscript not punlished). [Google Scholar]
- Berliński, M.; Suprvisory guidance Dobrzański, L.A. Modelowanie Zależności między Warunkami Wytapiania w Wielkim Piecu i Składem Chemicznym Surówki z Wykorzystaniem Sieci Neuronowych. Ph.D. Thesis, Politechnika Śląska, Gliwice, Poland, 2018. [Google Scholar]
- Nieradka-Buczek, B.; Suprvisory Guidance Dobrzański, L.A. Zastosowanie Nanodrutów Srebra jako Wzmocnienia Transparentnych Warstw Nanokompozytowych. Ph.D. Thesis, Politechnika Śląska, Gliwice, Poland, 2018. [Google Scholar]
- Kędzierski, K.; Suprvisory guidance Dobrzański, L.A. Charakterystyka Ekologicznych Ośrodków Polimerowych do Chłodzenia Nawęglonych Stali Niskowęglowych. Ph.D. Thesis, Politechnika Śląska, Gliwice, Poland, 2017. [Google Scholar]
- Szindler, M.; Suprvisory Guidance Dobrzański, L.A. Polimerowe Warstwy Półprzewodnikowe zol-żel do Zastosowań Fotowoltaicznych. Ph.D. Thesis, Politechnika Śląska, Gliwice, Poland, 2017. [Google Scholar]
- Achtelik-Franczak, A.; suprvisory guidance Dobrzański, L.A. Inżynierskie Materiały Kompozytowe O Wzmocnieniu Z Mikroporowatego Tytanu Selektywnie Spiekanego Laserowo. Ph.D. Thesis, Politechnika Śląska, Gliwice, Poland, 2016. [Google Scholar]
- Macek, M.; Suprvisory Guidance Dobrzański, l.a. Struktura i Własności Aluminiowych Materiałów Nanokompozytowych Wzmacnianych Nanorurkami Węglowymi. Ph.D. Thesis, Politechnika Śląska, Gliwice, Poland, 2016. [Google Scholar]
- Prokopiuk vel Prokopowicz, M.; Suprvisory Guidance Dobrzański, L.A. Wpływ zredukowanego Tlenku Grafenu na Strukturę Elektrod i Własności Barwnikowych Ogniw Fotowoltaicznych. Ph.D. Thesis, Politechnika Śląska, Gliwice, Poland, 2016. [Google Scholar]
- Czaja, I.; Suprvisory Guidance Dobrzański, L.A. Wpływ Nanodrutów i Nanoproszków Miedzi na Strukturę i Własności Nanokompozytowych Materiałów Polimerowych. Ph.D. Thesis, Politechnika Śląska, Gliwice, Poland, 2015. [Google Scholar]
- Hudecki, A.; Suprvisory Guidance Dobrzański, L.A. Nanowłókna kompozytowe o bioaktywnym rdzeniu i antybakteryjnej powłoce na rusztowania tkankowe. Ph.D. Thesis, Politechnika Śląska, Gliwice, Poland, 2015. [Google Scholar]
- Mucha, A.; Suprvisory Guidance Dobrzański, L.A. Wpływ nanorurek węglowych na własności barwnikowych ogniw fotowoltaicznych. Ph.D. Thesis, Politechnika Śląska, Gliwice, Poland, 2015. [Google Scholar]
- Górniak, M.; Suprvisory Guidance Dobrzański, L.A. Wpływ Organofilizacji Powierzchni Nanorurek Haloizytowych i Nanopłytek Montmorylonitowych na Własności Kompozytów Polimerowych. Ph.D. Thesis, Politechnika Śląska, Gliwice, Poland, 2014. [Google Scholar]
- Szindler, M.; Suprvisory Guidance Dobrzański, L.A. Struktura i Własności Nanostrukturalnych Warstw Antyrefleksyjnych Otrzymanych Metodą ALD Oraz zol-żel na Krzemowych Ogniwach Fotowoltaicznych. Ph.D. Thesis, Politechnika Śląska, Gliwice, Poland, 2014. [Google Scholar]
- Reimann, Ł.; Suprvisory Guidance Dobrzański, L.A. System Komputerowego Wspomagania Doboru Materiałów Na Wieloczłonowe Częściowe Stałe Protezy Stomatologiczne. Ph.D. Thesis, Politechnika Śląska, Gliwice, Poland, 2013. [Google Scholar]
- Henderson, B. The Product Portfolio. Available online: https://www.bcg.com/publications/1970/strategy-the-product-portfolio (accessed on 8 April 2021).
- Suresh Chandra, B.; Gopikrishna, V. (Eds.) Grossman’s Endodontic Practice, 13th ed.; Wolters Kluwer: New Delhi, India, 2014; pp. 1–576. [Google Scholar]
- Durey, I. Deming’s Management Method and Total Quality Management. Available online: https://www.gembadesk.com/2014/10/demings-management-method-and-total-quality-management/#:~:text=Created%20in%201951%2C%20The%20Deming%20Prize%20was%20awarded,American%20Society%20for%20Quality%E2%80%99s%20Deming%20Medal%20in%20 (accessed on 17 April 2021).
- Lina, L.R.; Ullah, H. The concept and implementation of Kaizen in organization. Int. J. Bus. Adm. Manag. Res. 2019, 19, 1–9. [Google Scholar]
- Rokke, C.; Yadav, O.P. Challenges and Barriers to Total Quality Management: An Overview. Int. J. Performability Eng. 2012, 8, 653–665. [Google Scholar]



















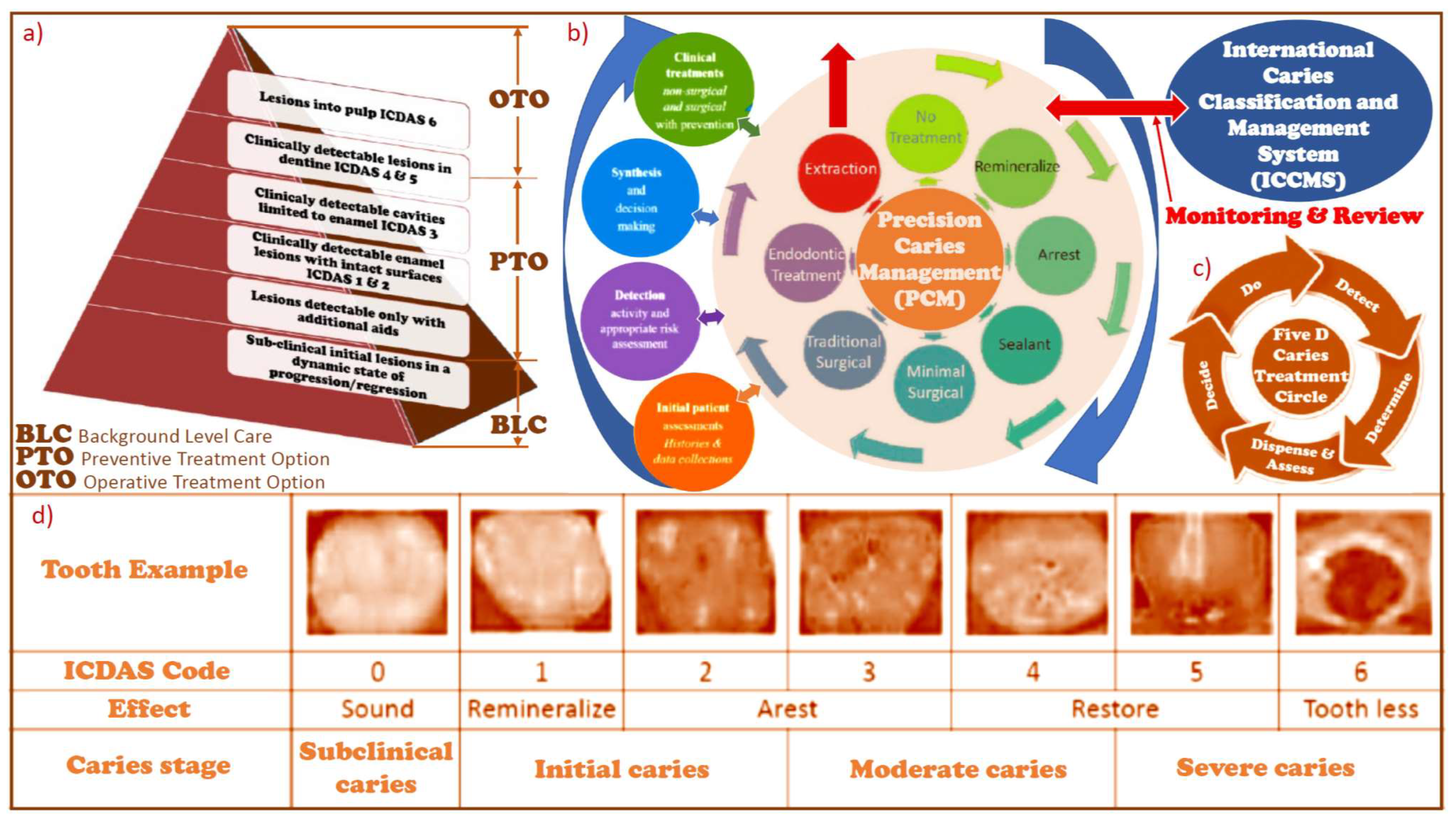{kind=link}
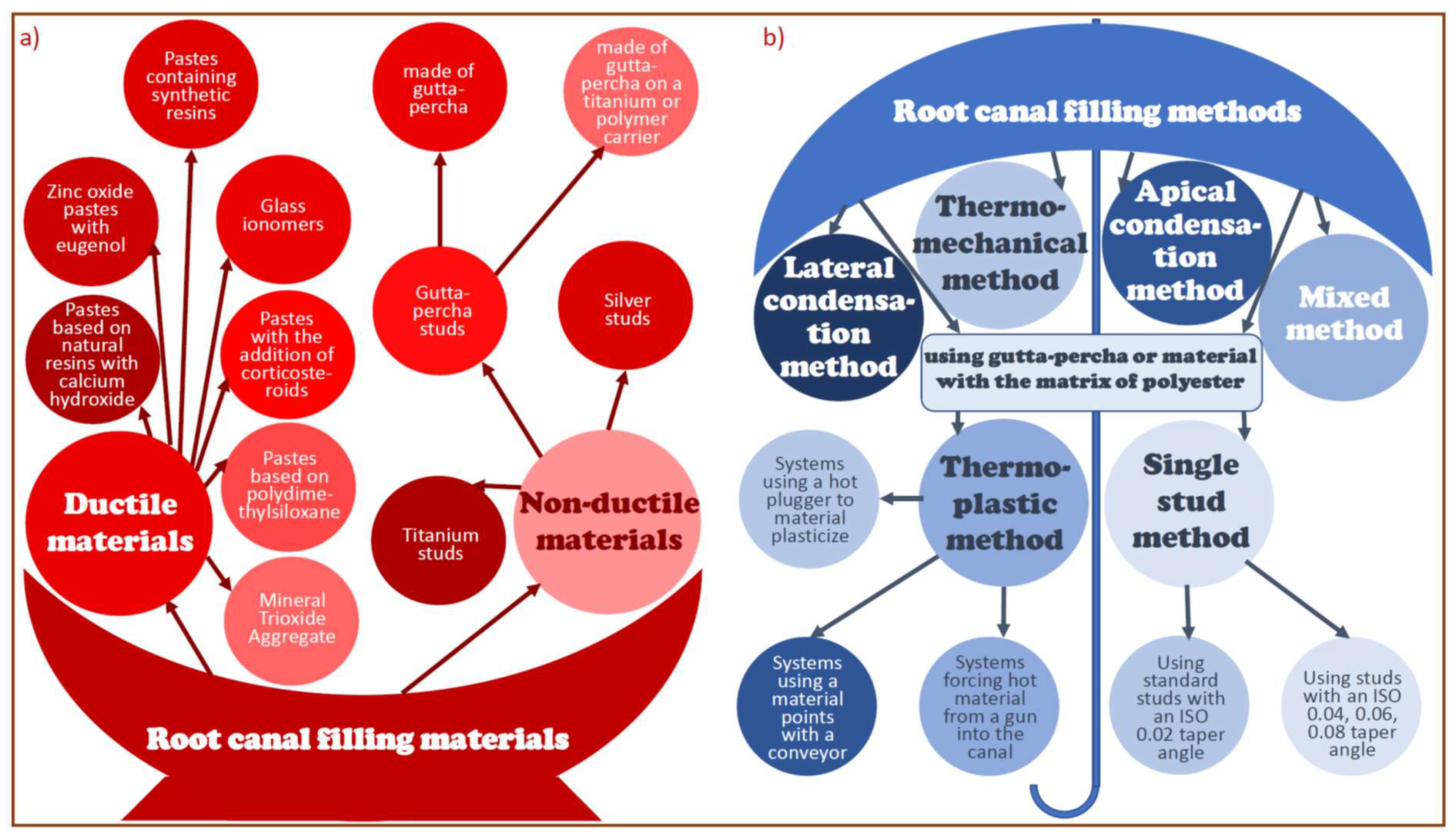{kind=link}
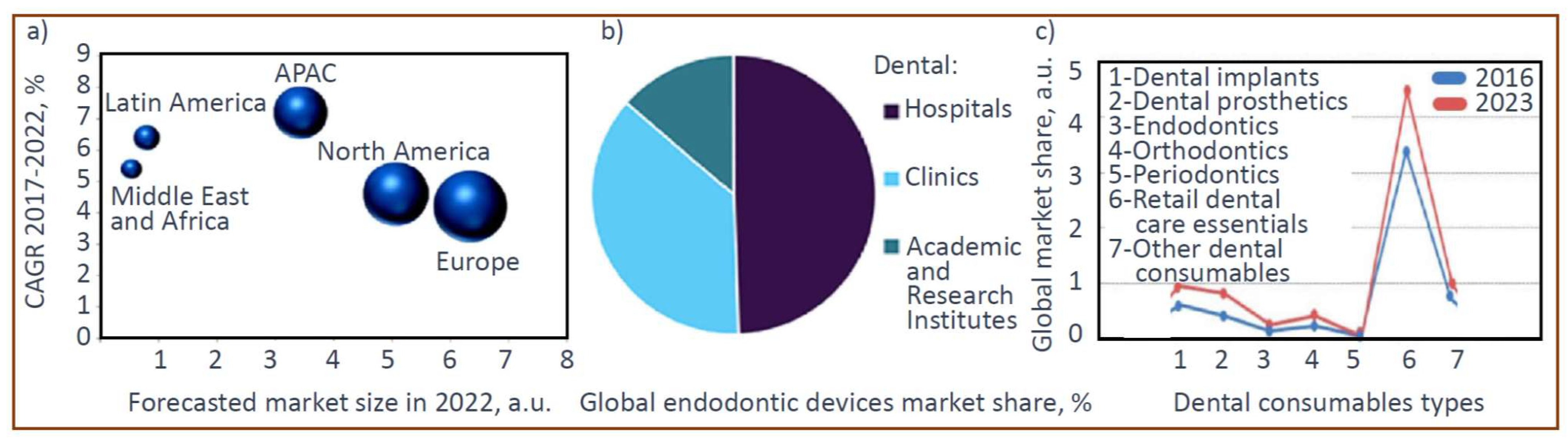{kind=link}
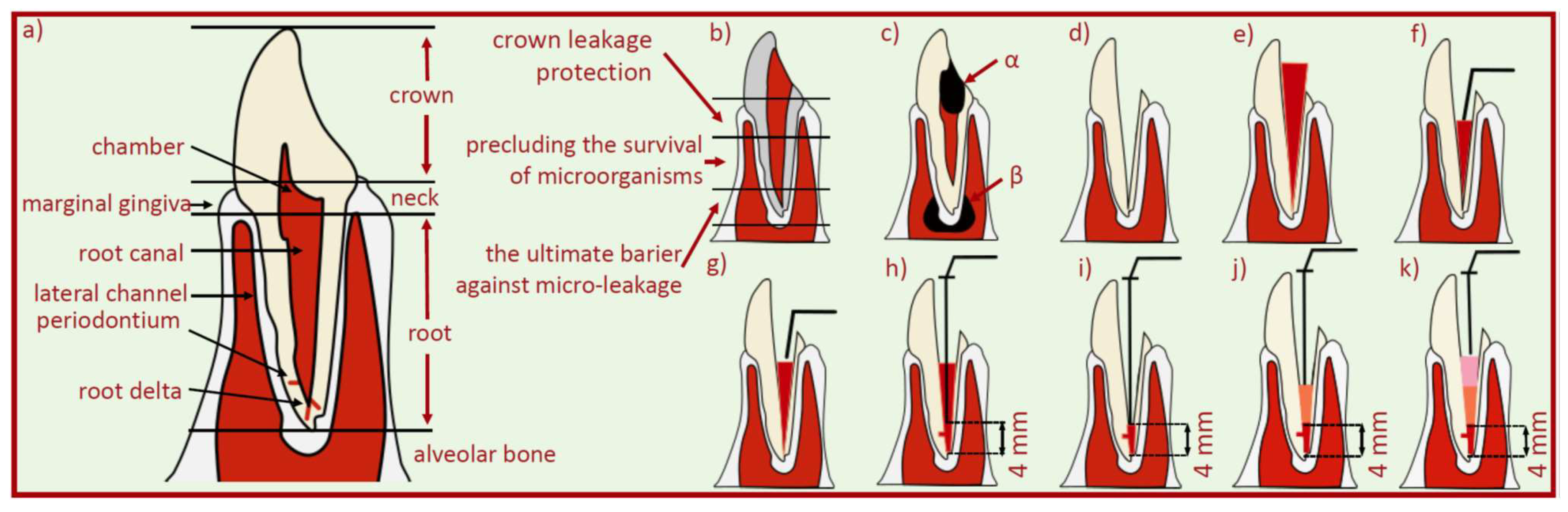{kind=link}
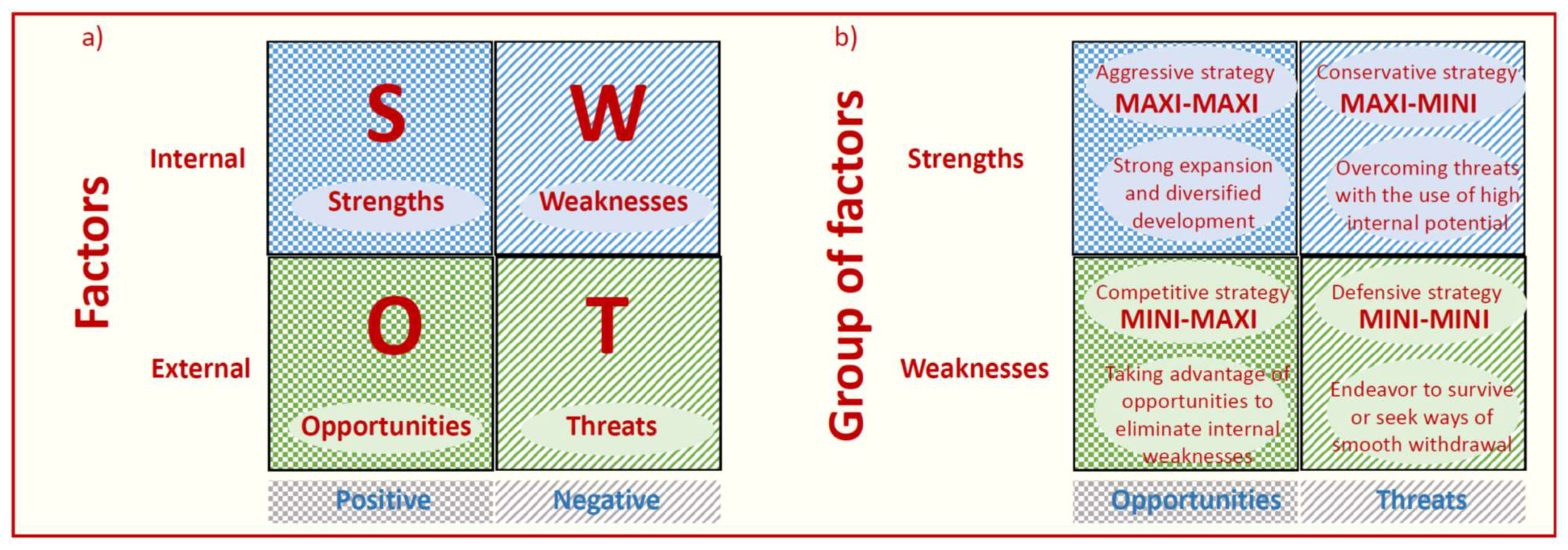{kind=link}
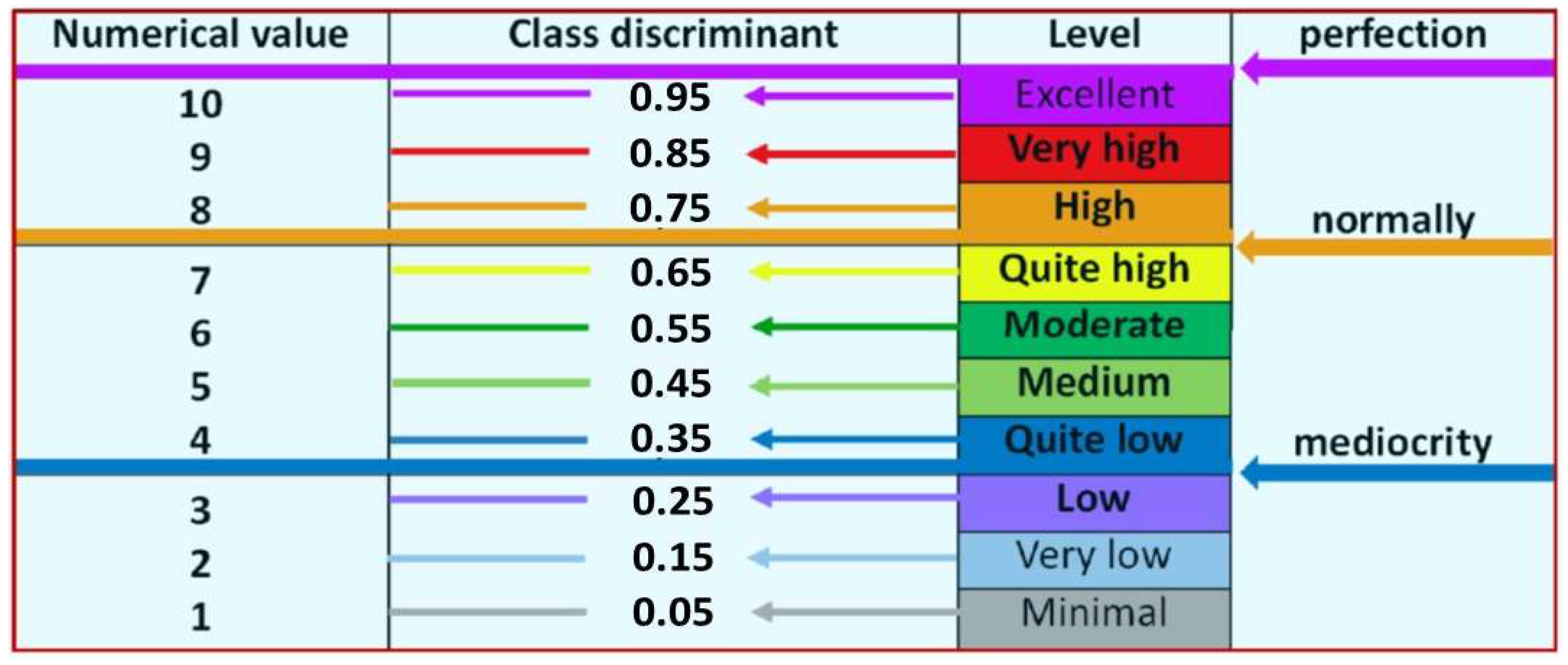{kind=link}
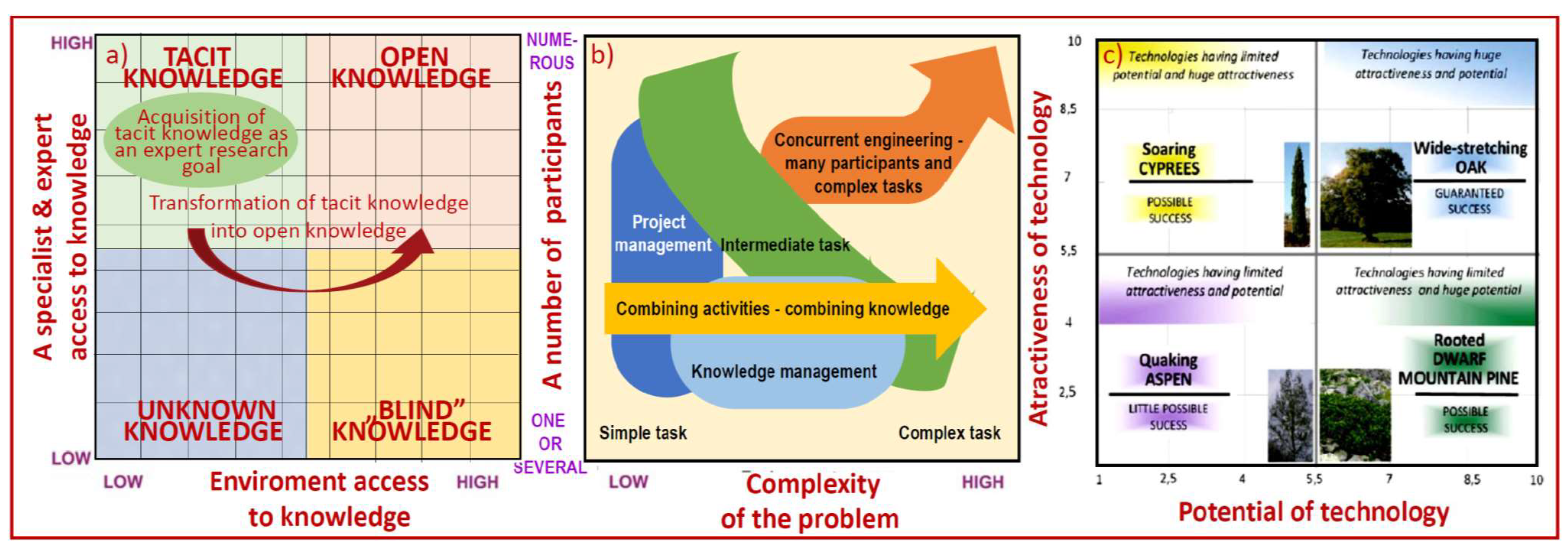{kind=link}
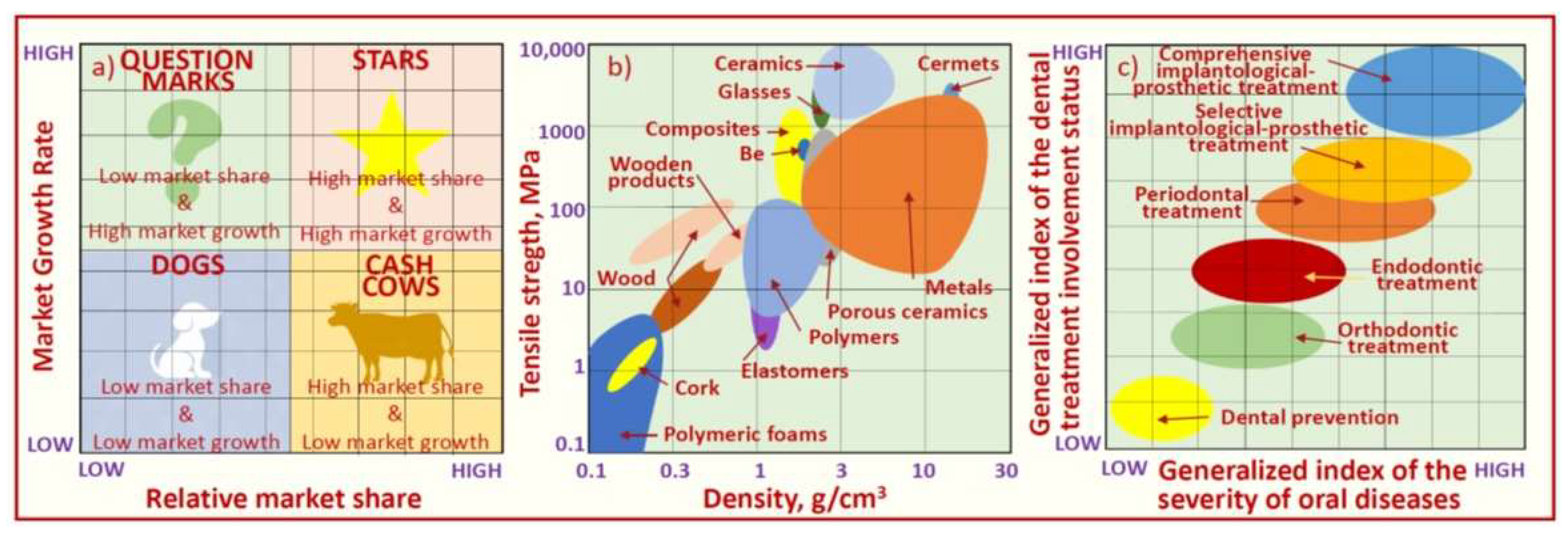{kind=link}
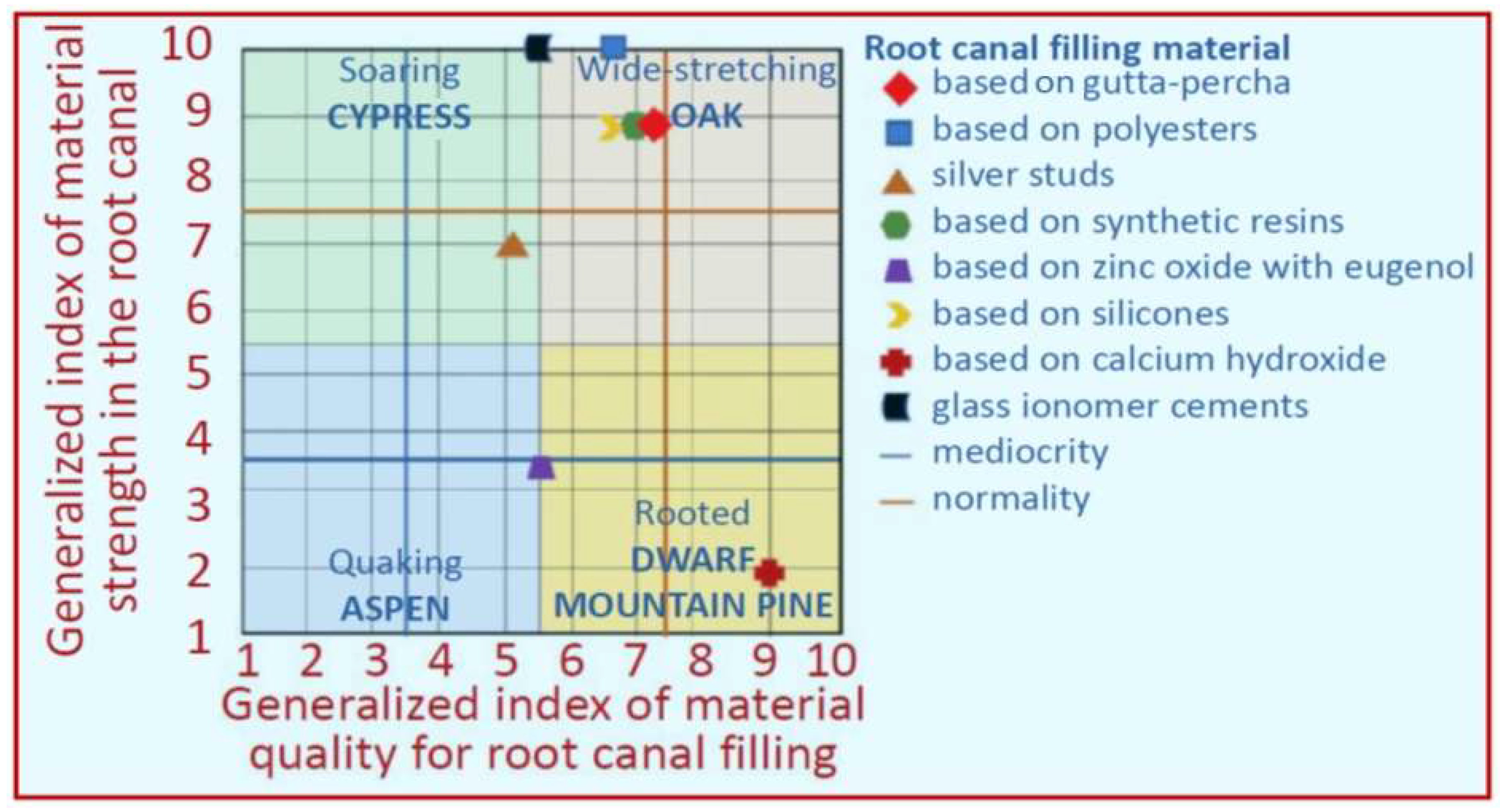{kind=link}
{kind=link}
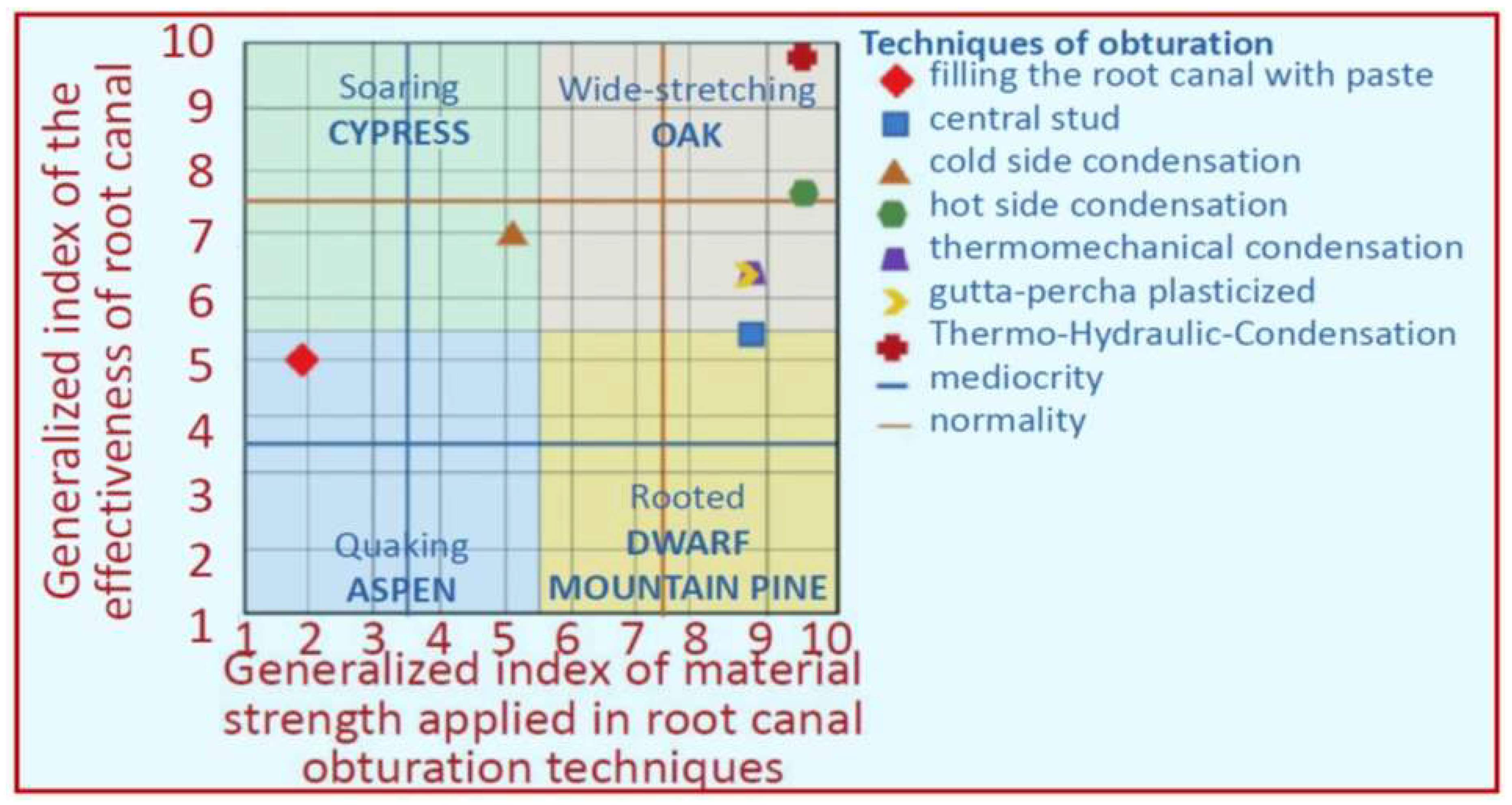{kind=link}
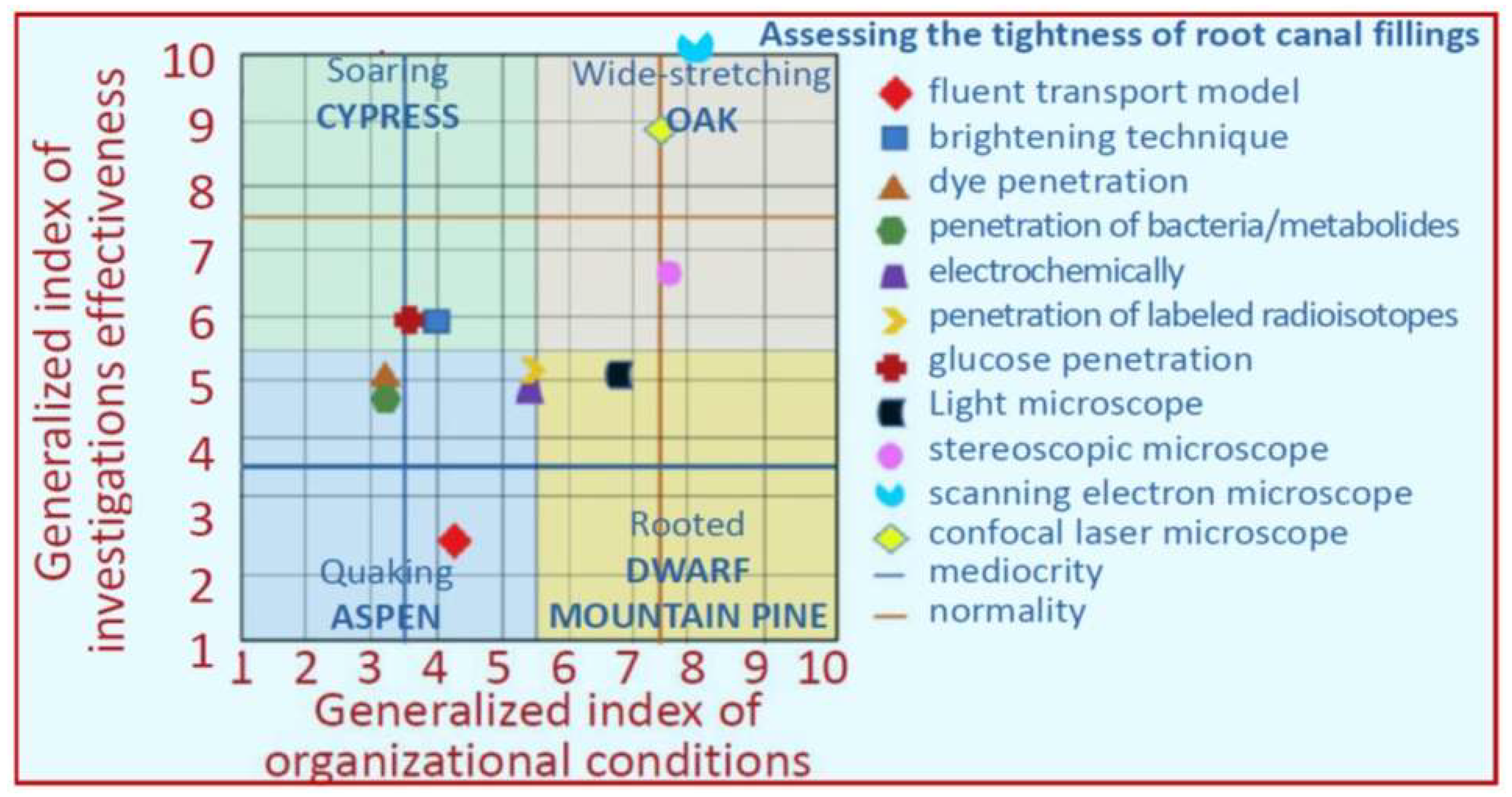{kind=link}
{kind=link}
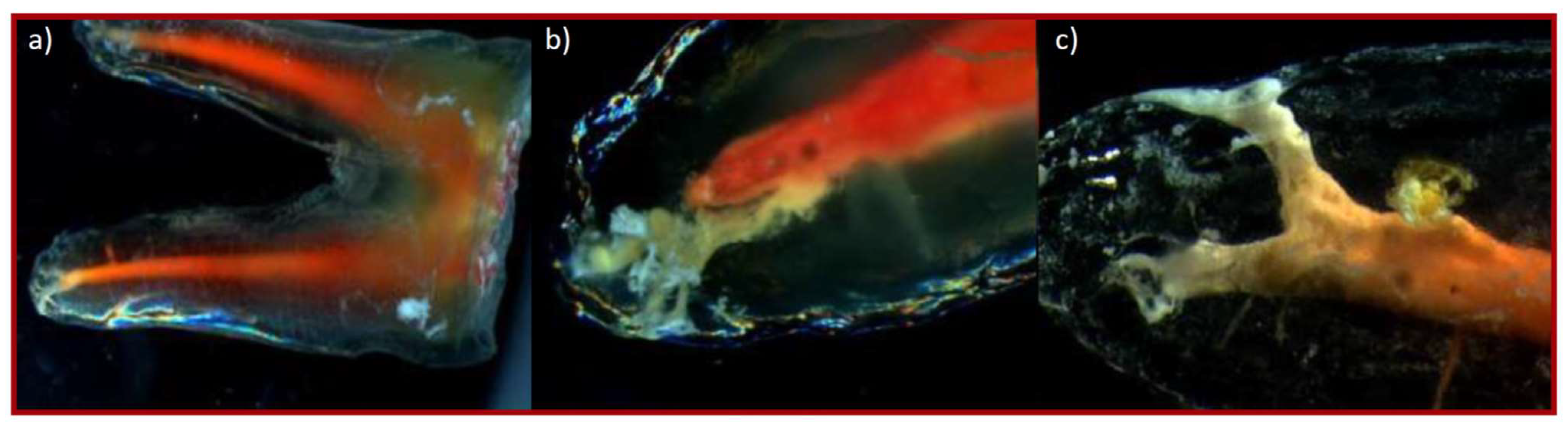{kind=link}
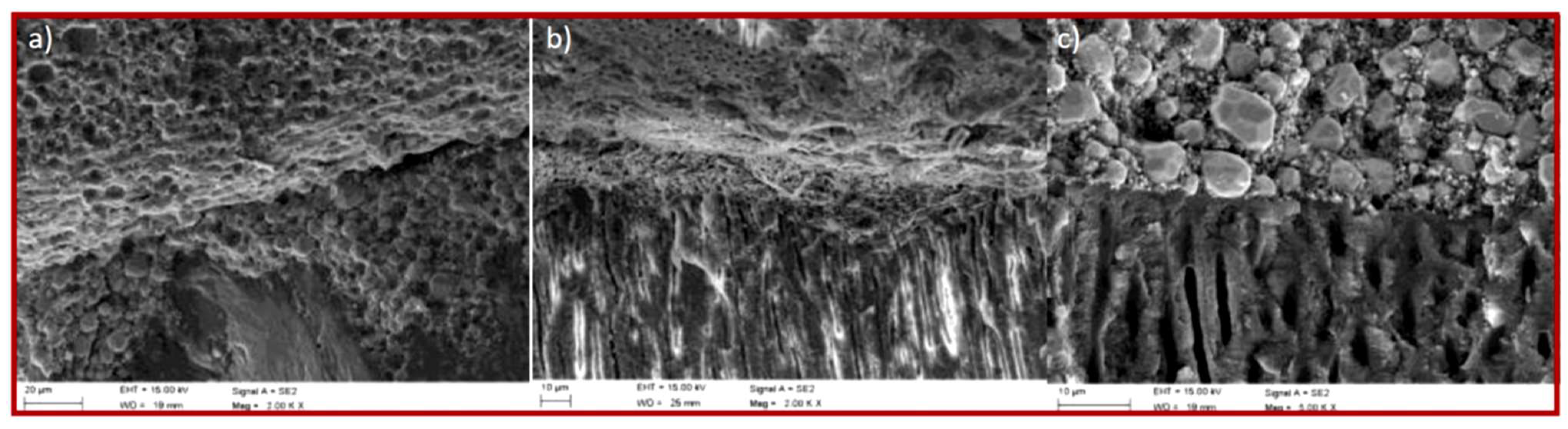{kind=link}
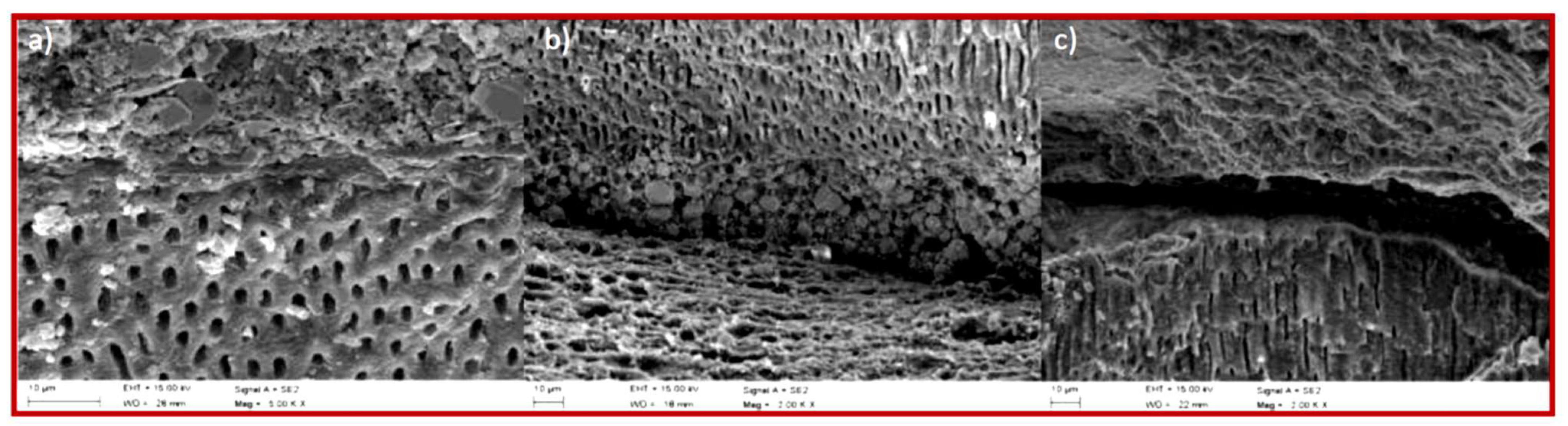{kind=link}
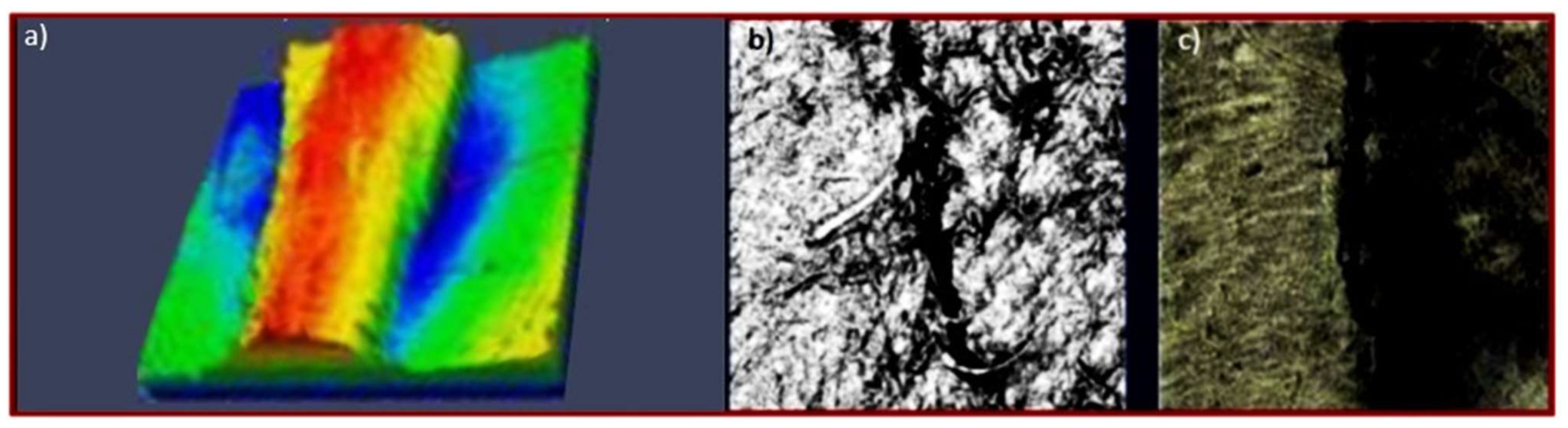{kind=link}
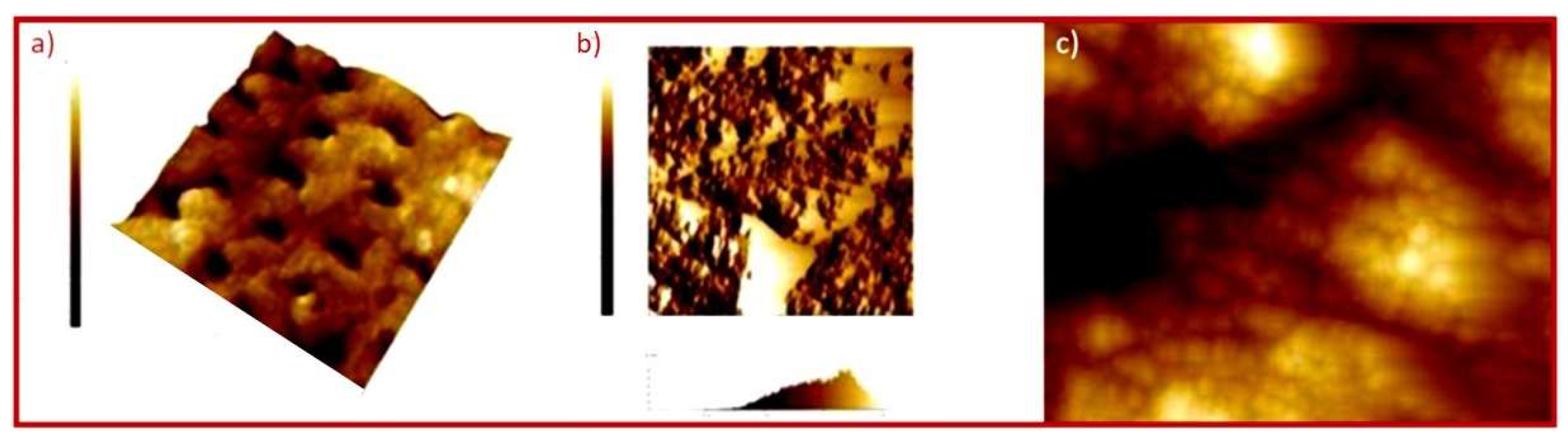{kind=link}
| No. | Table | Figure | Analysed Dependence on the Context Matrix | Quantity on the Horizontal Axis (Generalized Potential) | Quantity on the Vertical Axis (Generalized Attractiveness) |
|---|---|---|---|---|---|
| 1. | Table 2 | Figure 4 | Materials selection | Generalized index of material quality for root canal filling | Generalized index of material strength in the root canal |
| 2. | Table 3 | Figure 5 | Root canal development technique selection | Generalized organizational index of techniques for the development of root canals | Generalized index of the quality of filling with selected techniques |
| 3. | Table 4 | Figure 7 | Techniques of obturation selection | Generalized index of material strength applied in root canal obturation techniques | Generalized index of the effectiveness of root canal obturation techniques |
| 4. | Table 5 | Figure 8 | Assessing the tightness of root canal filling selection | Generalized index of organizational conditions | Generalized index of investigations effectiveness |
| General Descriptors | Criteria for Determining the Generalized Quality Index of the Root Canal Filling Material | Criteria for Determining the Generalized Strength Index of the Root Canal Filling Material | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Material | Application Form/Consistency | Method of Application to the Root Canal | |||||||
| Based on gutta-percha | Studs | Cold techniques | The possibility of sterilization | Ease of removal from the root canal in the event of revision | Toxicity | Bactericide | X-ray transmittance | No resorption over time | Mechanical resistance of the root to fracture after using the material |
| Based on polyesters | Hot techniques | ||||||||
| silver studs | Applied with a sealant | ||||||||
| Based on synthetic resins | Pellets | ||||||||
| Based on zinc oxide with eugenol | Independently | ||||||||
| Based on silicones | On the Lentulo needle | ||||||||
| Based on calcium hydroxide | Paste | As a sealant for studs | |||||||
| glass ionomer cements | As a gutta-percha sealant | ||||||||
| Weight | 0.1 | 0.25 | 0.4 | 0.2 | 0.05 | 0.4 | 0.6 | ||
| General Descriptors–Techniques for the Development of Root Canals | Criteria for Determining the Generalized Quality Index of the Root Canal Filling with Selected Techniques | Criteria for Determining the Generalized Organizational Index of Techniques for the Development of Root Canals | ||||||
|---|---|---|---|---|---|---|---|---|
| Laser | No risk of thermal damage to periodontal tissues | No risk of tool breakage | No risk of losing the natural course of the root canal and creating niches | Root canal disinfection | No risk of pushing the cut dentine beyond the periapical foramen | Conical root canal preparation | Minimization of the unit cost of the procedure | Ease of mastering the technique |
| Ultrasonic | ||||||||
| Mechanical–steel tools | ||||||||
| Mechanical—nickel–titanium tools | ||||||||
| Weight | 0.3 | 0.2 | 0.1 | 0.1 | 0.2 | 0.1 | 0.5 | 0.5 |
| General Descriptors | Criteria For Determining the Generalized Quality Index of the Root Canal Obturation Technique Effectiveness | Criteria for Determining the Generalized Index of Material Strength Applied in Root Canal Obturation Techniques | ||||||
|---|---|---|---|---|---|---|---|---|
| Techniques of Root Canal Obstruction | Type of Material Used | Additional Devices | ||||||
| Filling the root canal with paste | Sealant | Lentulo needle | The amount of sealant used | Speed of proceeding using a given technique | No risk of pushing the material beyond the tip | Possibility of filling additional channels | No resorption occurs over time | Mechanical resistance of the root to fracture after using the material |
| Central stud | Gutta-percha + sealant | |||||||
| Cold side condensation | Gutta-percha or material based on polyester polymeric materials + sealant | Cold plugger | ||||||
| Hot side condensation | Hot plugger + cold plugger | |||||||
| Thermo-mechanical condensation | Gutta-percha on a compactor; e.g., Quickfill + sealant | Caecum | ||||||
| Gutta-percha plasticized | Gutta-percha on plastic; e.g., Thermafil + sealant | Heating furnace; e.g., TermaPrep | ||||||
| Thermo-hydraulic-condensation | Gutta-percha or material based on polyester polymeric materials + sealant | Hot plugger, cold plugger, hot gutta-percha feeding device; e.g., System B + Obtura III | ||||||
| Weight | 0.15 | 0.05 | 0.3 | 0.5 | 0.4 | 0.6 | ||
| General Descriptors | Criteria for Determining the Generalized Index of Organizational Conditions of Assessed Investigations Methods | Criteria for Determining the Generalized Index Investigations Effectiveness | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Investigation Method | ||||||||||
| Fluent transport model | Difficulty preparing the specimen | Complicating the procedure of preparing the test system | Destructive/non-destructive method | Possibility of multiple test realization | Maximum possible duration of a research experiment | Cost of materials necessary to realize the investigation | The investment cost and the purposefulness of the expenses incurred | Cost of investigation equipment | Sensitivity/resolution | Relevance of the determination |
| Brightening technique | ||||||||||
| Dye penetration | ||||||||||
| Penetration of bacteria/metabolites | ||||||||||
| Electrochemical | ||||||||||
| penetration of labelled radioisotopes | ||||||||||
| Glucose penetration | ||||||||||
| Light microscope | ||||||||||
| Stereoscopic microscope | ||||||||||
| Scanning electron microscope | ||||||||||
| Confocal laser microscope | ||||||||||
| Weight | 0.05 | 0.15 | 0.1 | 0.1 | 0.1 | 0.2 | 0.2 | 0.1 | 0.5 | 0.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dobrzańska, J.; Dobrzański, L.B.; Gołombek, K.; Dobrzański, L.A.; Dobrzańska-Danikiewicz, A.D. Virtual Approach to the Comparative Analysis of Biomaterials Used in Endodontic Treatment. Processes 2021, 9, 926. https://doi.org/10.3390/pr9060926
Dobrzańska J, Dobrzański LB, Gołombek K, Dobrzański LA, Dobrzańska-Danikiewicz AD. Virtual Approach to the Comparative Analysis of Biomaterials Used in Endodontic Treatment. Processes. 2021; 9(6):926. https://doi.org/10.3390/pr9060926
Chicago/Turabian StyleDobrzańska, Joanna, Lech B. Dobrzański, Klaudiusz Gołombek, Leszek A. Dobrzański, and Anna D. Dobrzańska-Danikiewicz. 2021. "Virtual Approach to the Comparative Analysis of Biomaterials Used in Endodontic Treatment" Processes 9, no. 6: 926. https://doi.org/10.3390/pr9060926
APA StyleDobrzańska, J., Dobrzański, L. B., Gołombek, K., Dobrzański, L. A., & Dobrzańska-Danikiewicz, A. D. (2021). Virtual Approach to the Comparative Analysis of Biomaterials Used in Endodontic Treatment. Processes, 9(6), 926. https://doi.org/10.3390/pr9060926