The Concept of Sustainable Development of Modern Dentistry

 ,
,  ,
,  and
and 
Abstract
1. Introduction
“Balance appears as the basic nature of all things, no matter what level we pay attention to. It applies to the same degree to elementary particles, the functioning of the organism, social phenomena, or the movement of galaxies. Opposites strive towards each other, they try to complement and complete each other because in themselves they do not actually exist. This process is constantly accompanied by movement, which is a tool of balance. It is because of him that everything that exists is constantly changing and tends to the perfect point that can never be achieved. Because balance is not so much a point, an ideal, but a constant balancing around that point. Balancing unity is the ever-pulsating dance of everything, it is the beating heart of the Cosmos, it is the very breath of God.” [1].
2. Analysis of the Contemporary State of Oral Cavity Diseases in the World
3. Dentistry 4.0 as an Avant-Garde Stage of Dental Treatment
- The frequent and/or long-term consumption of sugars, when they are a large part of the diet;
- insufficient saliva flow rate;
- poor oral hygiene;
- suboptimal exposure to fluoride;
- tooth deformities caused by poor nutrition due to socio-economic degradation;
- a lack or low level of dental care.
- Detect lesions;
- Determine lesions’ activity;
- Dispense and assess the scale of lesions and their activity;
- Decide on the patient’s personalized care plan;
- Conduct the right intervention at the right time.
4. Development Strategy for the Prevention of Oral Cavity Diseases and Coordinated and Related Systemic and Political Actions
5. Safety of Dentists and Dental Staff as a Development Determinant of Dentistry
6. Ethical Context of the Treatment of Oral Diseases
- physical (health and fitness, endurance, disease resistance and regenerative abilities);
- emotional (the ability to realistically perceive the world, coping with stress, flexibility and a compromise attitude to conflict);
- social (family and environmental relationships, social skills and cultural sensitivity);
- intellectual (personal development, perceptual, analytical, decision-making and rational skills);
- spiritual (religiosity and/or value system, relations to the living world, empathy and an active attitude towards society and other people);
- professional (career, finances, quality of life, professional and non-professional interactions);
- environmental (relations with the natural environment and with the material and metaphysical surroundings in general).
7. Final Remarks
Author Contributions
Funding
Conflicts of Interest
Notice
References
- Kulik, R. Czym jest równowaga? Dzikie Życie 2008, 3, 165. Available online: https://dzikiezycie.pl/archiwum/2008/marzec-2008/czym-jest-rownowaga (accessed on 6 September 2020).
- Von Carlowitz, H.C. Sylvicultura Oeconomica Oder Haußwirthliche Nachricht und Naturmäßige Anweisung zur Wilden Baum-Zucht (Deutsch); Hamberger, J., Ed.; Oekom Verlag: München, Germany, 2013. [Google Scholar]
- Brundtland, G.H. (Ed.) Report of the World Commission on Environment and Development (WCED): Our Common Future (also known as the Brundtland Report); United Nations: New York, NY, USA, 1987; Available online: https://sustainabledevelopment.un.org/content/documents/5987our-common-future.pdf (accessed on 6 September 2020).
- Meadows, D.H.; Meadows, D.L.; Randers, J.; Behrens, W.W., III. The Limits to Growth: A Report for the Club of Rome’s Project on the Predicament of Mankind; A Potomac Associates Book: New York, NY, USA, 1972; Available online: https://collections.dartmouth.edu/teitexts/meadows/diplomatic/meadows_ltg-diplomatic.html (accessed on 6 September 2020).
- Holcombe, R.G. A theory of the theory of public goods. Rev. Austrian Econ. 1997, 10, 1–22. [Google Scholar] [CrossRef]
- Peres, M.A.; Macpherson, L.M.D.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreño, C.C.; Kearns, C.; et al. Oral diseases: A global public health challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef]
- Watt, R.G.; Daly, B.; Allison, P.; Macpherson, L.M.D.; Venturelli, R.; Listl, S.; Weyant, R.J.; Mathur, M.R.; Guarnizo-Herreño, C.C.; Celeste, R.K.; et al. Ending the neglect of global oral health: Time for radical action. Lancet 2019, 394, 261–272. [Google Scholar] [CrossRef]
- Clarkson, J.E.; Young, L.; Ramsay, C.R.; Bonner, B.C.; Bonetti, D. How to influence patient oral hygiene behavior effectively. J. Dent. Res. 2009, 88, 933–937. [Google Scholar] [CrossRef] [PubMed]
- Edwards Deming, W. Out of the Crisis; Massachusetts Institute of Technology, Center for Advanced Engineering Study: Cambridge, MA, USA, 1986. [Google Scholar]
- Pitts, N.B.; Zero, D.T. White Paper on Dental Caries Prevention and Management. FDI World Dental Federation. Available online: http://www.fdiworlddental.org/sites/default/files/media/documents/2016-fdi_cpp-white_paper.pdf (accessed on 8 November 2020).
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.; Marcenes, W. Global burden of untreated caries: A systematic review and metaregression. J. Dent. Res. 2015, 94, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Pitts, N.B.; Zero, D.T.; Marsh, P.D.; Ekstrand, K.; Weintraub, J.A.; Ramos-Gomez, F.; Tagami, J.; Twetman, S.; Tsakos, G.; Ismail, A. Dental caries. Nat. Rev. Dis. Primers 2017, 3, 17030. [Google Scholar] [CrossRef]
- Mejàre, I.; Axelsson, S.; Dahlén, G.; Espelid, I.; Norlund, A.; Tranæus, S.; Twetman, S. Caries risk assessment. A systematic review. Acta Odontol. Scand. 2014, 72, 81–91. [Google Scholar] [CrossRef] [PubMed]
- Twetman, S.; Banerjee, A. Caries risk assessment. In Risk Assessment in Oral Health; Chapple, I., Papapanou, P., Eds.; Springer: Cham, Switzerland, 2020. [Google Scholar] [CrossRef]
- Yadav, K.; Prakash, S. Dental caries: A microbiological approach. J. Clin. Infect. Dis. Pr. 2017, 2, 1000118. [Google Scholar] [CrossRef]
- Selwitz, R.H.; Ismail, A.I.; Pitts, N.B. Dental caries. Lancet 2007, 369, 51–59. [Google Scholar] [CrossRef]
- Van Houte, J. Role of micro-organisms in caries etiology. J. Dent. Res. 1994, 73, 672–681. [Google Scholar] [CrossRef] [PubMed]
- Bolin, A.K.; Bolin, A.; Jansson, L.; Calltorp, J. Children’s dental health in Europe. Swed. Dent. J. 1997, 21, 25–40. [Google Scholar] [PubMed]
- Fejerskov, O. Concepts of dental caries and their consequences for understanding the disease. Community Dent. Oral. Epidemiol. 1997, 25, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Fejerskov, O. Changing paradigms in concepts on dental caries: Consequences for oral health care. Caries Res. 2004, 38, 182–191. [Google Scholar] [CrossRef] [PubMed]
- Pitts, N. “ICDAS”—An international system for caries detection and assessment being developed to facilitate caries epidemiology, research and appropriate clinical management. Community Dent. Health 2004, 21, 193–198. [Google Scholar] [PubMed]
- Zero, D.T.; Zandona, A.F.; Vail, M.M.; Spolnik, K.J. Dental caries and pulpal disease. Dent. Clin. North Am. 2011, 55, 29–46. [Google Scholar] [CrossRef]
- Zero, D.T. Dental caries process. Dent. Clin. North Am. 1999, 43, 635–664. [Google Scholar]
- Thomson, W.M. Epidemiology of oral health conditions in older people. Gerodontology 2014, 31 (Suppl. 1), 9–16. [Google Scholar] [CrossRef]
- Psoter, W.J.; Reid, B.C.; Katz, R.V. Malnutrition and dental caries: A review of the literature. Caries Res. 2005, 39, 441–447. [Google Scholar] [CrossRef]
- López, N.J.; Smith, P.C.; Gutierrez, J. Periodontal therapy reduce the risk of preterm low birth weight in women with periodontal disease: A randomized controlled trial. J. Periodontol. 2002, 73, 911–924. [Google Scholar] [CrossRef]
- Al-Nawas, B.; Maeurer, M. Severe versus local odontogenic bacterial infections: Comparison of microbial isolates. Eur. Surg. Res. 2008, 40, 220–224. [Google Scholar] [CrossRef] [PubMed]
- Biguzzi, E.; Dougall, A.; Romero-Lux, O. Non-gynaecological issues in women with bleeding disorders. J. Haemophil. Pr. 2019, 6, 39–43. [Google Scholar] [CrossRef]
- Chapple, I.L.C.; Genco, R.; Working Group 2 of the Joint EFP/AAP Workshop. Diabetes and periodontal diseases: Consensus report of the Joint EFP/AAP Workshop on periodontitis and systemic diseases. J. Periodontol. 2013, 84, S106–S112. [Google Scholar] [CrossRef] [PubMed]
- Fuller, E.; Steele, J.; Watt, R.; Nuttal, N. 1: Oral Health and Function—A Report from the Adult Dental Health Survey 2009; NHS Health and Social Care Information Centre, 2011. Available online: https://files.digital.nhs.uk/publicationimport/pub01xxx/pub01086/adul-dent-heal-surv-summ-them-the1-2009-rep3.pdf (accessed on 28 August 2020).
- Albandar, J.M.; Rams, T.E. Global epidemiology of periodontal diseases: An overview. Periodontol. 2000 2002, 29, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Sheiham, A.; Netuveli, G.S. Periodontal diseases in Europe. Periodontol. 2000 2002, 29, 104–121. [Google Scholar] [CrossRef]
- Papapanou, P.N. Commentary: Advances in periodontal disease epidemiology: A retrospective commentary. J. Periodontol. 2014, 85, 877–879. [Google Scholar] [CrossRef]
- Albandar, J.M.; Tinoco, E.M. Global epidemiology of periodontal diseases in children and young persons. Periodontol. 2000 2002, 29, 153–176. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzański, L.B.; Dobrzańska-Danikiewicz, A.D.; Dobrzańska, J.; Rudziarczyk, K.; Achtelik-Franczak, A. Non-antagonistic contradictoriness of the progress of advanced digitized production with SARS-CoV-2 virus transmission in the area of dental engineering. Processes 2020, 8, 1097. [Google Scholar] [CrossRef]
- Scannapieco, F.A. Role of oral bacteria in respiratory infection. J. Periodontol. 1999, 70, 793–802. [Google Scholar] [CrossRef]
- Scannapieco, F.A.; Bush, R.B.; Paju, S. Associations between periodontal disease and risk for nosocomial bacterial pneumonia and chronic obstructive pulmonary disease. A systemic review. Ann. Periodontol. 2003, 8, 54–69. [Google Scholar] [CrossRef]
- Mueller, A.A.; Saldami, B.; Stübinger, S.; Walter, C.; Flückiger, U.; Merlo, A.; Schwenzer-Zimmerer, K.; Zeilhofer, H.F.; Zimmerer, S. Oral bacterial cultures in nontraumatic brain abscesses: Results of a first line study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 107, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Tornstad, L.; Olsen, I. Brain abscesses caused by oral infection. Dent. Traumatol. 1999, 15, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Aleksander, M.; Krishnan, B.; Shenoy, N. Diabetes mellitus and odontogenic infections-an exaggerated risk? Oral Maxillofac. Surg. 2008, 12, 129–130. [Google Scholar] [CrossRef] [PubMed]
- Isola, G.; Matarese, G.; Ramaglia, L.; Pedullà, E.; Rapisarda, E.; Iorio-Siciliano, V. Association between periodontitis and glycosylated haemoglobin before diabetes onset: A cross-sectional study. Clin. Oral Investig. 2020, 24, 2799–2808. [Google Scholar] [CrossRef]
- Gocke, C.; Holtfreter, B.; Meisel, P.; Grotevendt, A.; Jablonowski, L.; Jablonowski, L.; Markus, M.R.; Kocher, T. Abdominal obesity modifies long-term associations between periodontitis and markers of systemic inflammation. Atherosclerosis 2014, 235, 351–357. [Google Scholar] [CrossRef]
- Isola, G.; Polizzi, A.; Santonocito, S.; Alibrandi, A.; Ferlito, S. Expression of salivary and serum malondialdehyde and lipid profile of patients with periodontitis and coronary heart disease. Int. J. Mol. Sci. 2019, 20, 6061. [Google Scholar] [CrossRef]
- Friedewald, V.E.; Kornman, K.S.; Beck, J.D.; Genco, R.; Goldfine, A.; Libby, P.; Offenbacher, S.; Ridker, P.M.; Van Dyke, T.E.; Roberts, W.C. The American journal of cardiology and journal of periodontology editors’ consensus: Periodontitis and atherosclerotic cardiovascular disease. J. Periodontol. 2009, 80, 1021–1032. [Google Scholar] [CrossRef]
- Isola, G.; Alibrandi, A.; Currò, M.; Matarese, M.; Ricca, S.; Matarese, G.; Ientile, R.; Kocher, T. Evaluation of salivary and serum ADMA levels in patients with periodontal and cardiovascular disease as subclinical marker of cardiovascular risk. J. Periodontol. 2020, 91, 1076–1084. [Google Scholar] [CrossRef]
- Vidal, F.; Figueredo, C.M.; Cordovil, I.; Fischer, R.G. Periodontal therapy reduces plasma levels of interleukin-6, C-reactive protein, and fib-rinogen in patients with severe periodontitis and refractory arterial hypertension. J. Periodontol. 2009, 80, 786–791. [Google Scholar] [CrossRef]
- Isola, G.; Polizzi, A.; Muraglie, S.; Leonardi, R.M.; Lo Giudice, A. Assessment of vitamin C and antioxidants profiles In Saliva and serum in patients with periodontitis and ischemic heart disease. Nutrients 2019, 11, 2956. [Google Scholar] [CrossRef]
- Zhou, X.; Cao, F.; Lin, Z. Updated evidence of association between periodontal disease and incident erectile dysfunction. J. Sex. Med. 2019, 16, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Shamloul, R.; Ghanem, H. Erectile dysfunction. Lancet 2013, 381, 153–165. [Google Scholar] [CrossRef]
- Tsao, C.W.; Liu, C.Y.; Cha, T.L.; Wu, S.T.; Chen, S.C.; Hsu, C.Y. Exploration of the association between chronic periodontal disease and erectile dysfunction from a population-based view point. Andrologia 2015, 47, 513–518. [Google Scholar] [CrossRef] [PubMed]
- Rosen, R.C.; Cappelleri, J.C.; Gendrano, N., III. The international index of erectile function (IIEF): A state-of-the-science review. Int. J. Impot. Res. 2002, 14, 226–244. [Google Scholar] [CrossRef]
- Rosen, R.C.; Cappelleri, J.C.; Smith, M.D.; Lipsky, J.; Peña, B.M. Development and evaluation of an abridged, 5-item version of the international index of erectile function (IIEF-5) as a diagnostic tool for erectile dysfunction. Int. J. Impot. Res. 1999, 11, 319–326. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Pradeep, A.R.; Raju, P.A. Association between chronic periodontitis and vasculogenic erectile dysfunction. J. Periodontol. 2011, 82, 1665–1669. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, S.; Matsuda, M.; Takekawa, M.; Okada, M.; Hashizume, K.; Wada, N.; Hori, J.; Tamaki, G.; Kita, M.; Iwata, T.; et al. Association of ED with chronic periodontal disease. Int. J. Impot. Res. 2014, 26, 13–15. [Google Scholar] [CrossRef][Green Version]
- Eltas, A.; Oguz, F.; Uslu, M.O.; Akdemir, E. The effect of periodontal treatment in improving erectile dysfunction: A randomized controlled trial. J. Clin. Periodontol. 2013, 40, 148–154. [Google Scholar] [CrossRef]
- Lee, J.H.; Choi, J.K.; Kim, S.H.; Cho, K.H.; Kim, Y.T.; Choi, S.H.; Jung, U.W. Association between periodontal flap surgery for periodontitis and vasculogenic erectile dysfunction in Koreans. J. Periodontal. Implant. Sci. 2017, 47, 96–105. [Google Scholar] [CrossRef]
- Martín, A.; Bravo, M.; Arrabal, M.; Magán-Fernández, A.; Mesa, F. Chronic periodontitis is associated with erectile dysfunction. A case-control study in european population. J. Clin. Periodontol. 2018, 45, 791–798. [Google Scholar] [CrossRef]
- Oguz, F.; Eltas, A.; Beytur, A.; Akdemir, E.; Uslu, M.O.; Gunes, A. Is there a relationship between chronic periodontitis and erectile dysfunction? J. Sex. Med. 2013, 10, 838–843. [Google Scholar] [CrossRef] [PubMed]
- Keller, J.J.; Chung, S.D.; Lin, H.C. A nationwide population-based study on the association between chronic periodontitis and erectile dysfunction. J. Clin. Periodontol. 2012, 39, 507–512. [Google Scholar] [CrossRef] [PubMed]
- Zadik, Y.; Bechor, R.; Galor, S.; Justo, D.; Heruti, R.J. Erectile dysfunction might be associated with chronic periodontal disease: Two ends of the cardiovascular spectrum. J. Sex. Med. 2009, 6, 1111–1116. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.H.; Li, E.M.; Zhong, S.L.; Li, Y.Q.; Yang, Z.Y.; Kang, R.; Zhao, S.K.; Li, F.T.; Wan, S.P.; Zhao, Z.G. Chronic periodontitis and the risk of erectile dysfunction: A systematic review and meta-analysis. Int. J. Impot. Res. 2017, 29, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Kang, J.; Cai, X.; Wu, Y.; Zhao, L. The association between chronic periodontitis and vasculogenic erectile dysfunction: A systematic review and meta-analysis. J. Clin. Periodontol. 2016, 43, 206–215. [Google Scholar] [CrossRef] [PubMed]
- Singh, V.P.; Nettemu, S.K.; Nettem, S.; Hosadurga, R.; Nayak, S.U. Oral health and erectile dysfunction. J. Hum. Reprod. Sci. 2017, 10, 162–166. [Google Scholar] [CrossRef]
- Gandaglia, G.; Briganti, A.; Jackson, G.; Kloner, R.A.; Montorsi, F.; Montorsi, P.; Vlachopoulos, C. A systematic review of the association between erectile dysfunction and cardiovascular disease. Eur. Urol. 2014, 65, 968–978. [Google Scholar] [CrossRef] [PubMed]
- Eastham, J.; Seymour, R. Is oral health a risk factor for sexual health? Dent. Update 2015, 42, 160–162. [Google Scholar] [CrossRef]
- Peng, S.; Zhang, D.X. Chronic periodontal disease may be a sign for erectile dysfunction in men. Med. Hypotheses 2009, 73, 859–860. [Google Scholar] [CrossRef]
- Gurav, A.N. The implication of periodontitis in vascular endothelial dysfunction. Eur. J. Clin. Invest. 2014, 44, 1000–1009. [Google Scholar] [CrossRef]
- Brito, L.C.; DalBó, S.; Striechen, T.M.; Farias, J.M.; Olchanheski, L.R., Jr.; Mendes, R.T.; Vellosa, J.C.; Fávero, G.M.; Sordi, R.; Assreuy, J.; et al. Experimental periodontitis promotes transient vascular inflammation and endothelial dysfunction. Arch. Oral Biol. 2013, 58, 1187–1198. [Google Scholar] [CrossRef] [PubMed]
- Zuo, Z.; Jiang, J.; Jiang, R.; Chen, F.; Liu, J.; Yang, H.; Cheng, Y. Effect of periodontitis on erectile function and its possible mechanism. J. Sex. Med. 2011, 8, 2598–2605. [Google Scholar] [CrossRef] [PubMed]
- Kellesarian, S.V.; Malmstrom, H.; Abduljabbar, T.; Vohra, F.; Kellesarian, T.V.; Javed, F.; Romanos, G.E. Low testosterone levels in body fluids are associated with chronic periodontitis. Am. J. Mens. Health 2017, 11, 443–453. [Google Scholar] [CrossRef] [PubMed]
- Steffens, J.P.; Wang, X.; Starr, J.R.; Spolidorio, L.C.; Van Dyke, T.E.; Kantarci, A. Associations between sex hormone levels and periodontitis in men: Results from NHANES III. J. Periodontol. 2015, 86, 1116–1125. [Google Scholar] [CrossRef]
- Singh, B.P.; Makker, A.; Tripathi, A.; Singh, M.M.; Gupta, V. Association of testosterone and bone mineral density with tooth loss in men with chronic periodontitis. J. Oral Sci. 2011, 53, 333–339. [Google Scholar] [CrossRef]
- Daltaban, O.; Saygun, I.; Bolu, E. Periodontal status in men with hypergonadotropic hypogonadism: Effects of testosterone deficiency. J. Periodontol. 2006, 77, 1179–1183. [Google Scholar] [CrossRef]
- Bobjer, J.; Katrinaki, M.; Tsatsanis, C.; Lundberg Giwercman, Y.; Giwercman, A. Negative association between testosterone concentration and inflammatory markers in young men: A nested cross-sectional study. PLoS ONE 2013, 8, e61466. [Google Scholar] [CrossRef]
- Machado, V.; Lopes, J.; Patrão, M.; Botelho, J.; Proença, L.; Mendes, J.J. Validity of the association between periodontitis and female infertility conditions: A concise review. Reproduction 2020, 160, R41–R54. [Google Scholar] [CrossRef]
- Gajendra, S.; Kumar, J.V. Oral health and pregnancy: A review. NY State Dent. J. 2004, 70, 40–44. [Google Scholar]
- Pallasch, T.J.; Wahl, M.J. Focal infection: New age or ancient history? Endodon. Top. 2003, 4, 32–45. [Google Scholar] [CrossRef]
- Burzyńska, B.; Mierzwińska-Nastalska, E. Rehabilitacja protetyczna pacjentów bezzębnych. Nowa Stomatol. 2011, 4, 167–199. [Google Scholar]
- Felton, D.A. Edentualism and comorbid factors. J. Prosthodont. 2009, 18, 88–96. [Google Scholar] [CrossRef] [PubMed]
- Felton, D.A. Complete edentulism and comorbid diseases: An update. J. Prosthodont. 2016, 25, 5–20. [Google Scholar] [CrossRef] [PubMed]
- Holmlund, A.; Holm, G.; Lind, L. Number of teeth as a predictor of cardiovascular mortality in a cohort of 7674 subjects followed for 12 years. J. Periodontol. 2010, 81, 870–876. [Google Scholar] [CrossRef]
- Volzke, H.; Schwahn, C.; Hummel, A.; Wolff, B.; Kleine, V.; Robinson, D.M.; Dahm, J.B.; Felix, S.B.; John, U.; Kocher, T. Tooth loss is independently associated with the risk of acquired aortic valve sclerosis. Am. Heart J. 2005, 150, 1198–1203. [Google Scholar] [CrossRef] [PubMed]
- Takata, Y.; Ansai, T.; Matsumura, K.; Awano, S.; Hamasaki, T.; Sonoki, K.; Kusaba, A.; Akifusa, S.; Takehara, T. Relationship between tooth loss and electrocardiographic abnormalities in octogenarians. J. Dent. Res. 2001, 80, 1648–1652. [Google Scholar] [CrossRef] [PubMed]
- De Pablo, P.; Dietrich, T.; McAlindon, T.E. Association of periodontal disease and tooth loss with rheumatoid arthritis in the US population. J. Rheumatol. 2008, 35, 70–76. [Google Scholar]
- Sierpinska, T.; Golebiewska, M.; Dlugosz, J.W.; Kemona, A.; Laszewicz, W. Connection between masticatory efficiency and pathomorphologic changes in gastric mucosa. Quintessence Int. 2007, 38, 31–37. [Google Scholar]
- Abnet, C.C.; Qiao, Y.L.; Dawsey, S.M.; Dong, Z.W.; Taylor, P.R.; Mark, S.D. Tooth loss is associated with increased risk of total death and death from upper gastrointestinal cancer, heart disease, and stroke in a Chinese population-based cohort. Int. J. Epidemiol. 2005, 34, 467–474. [Google Scholar] [CrossRef]
- Bagchi, S.; Tripathi, A.; Tripathi, S.; Kar, S.; Tiwari, S.C.; Singh, J. Obstructive sleep apnea and neurocognitive dysfunction in edentulous patients. J. Prosthodont. 2019, 28, e837–e842. [Google Scholar] [CrossRef]
- Buset, S.L.; Walter, C.; Friedmann, A.; Weiger, R.; Borgnakke, W.S.; Zitzmann, N.U. Are periodontal diseases really silent? A systematic review of their effect on quality of life. J. Clin. Periodontol. 2016, 43, 333–344. [Google Scholar] [CrossRef] [PubMed]
- Bui, F.Q.; Almeida-da-Silva, C.L.C.; Huynh, B.; Trinh, A.; Liu, J.; Woodward, J.; Asadi, H.; Ojcius, D.M. Association between periodontal pathogens and systemic disease. Biomed. J. 2019, 42, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Nagpal, R.; Yamashiro, Y.; Izumi, Y. The two-way association of periodontal infection with systemic disorders: An overview. Mediat. Inflamm. 2015, 2015, 793898. [Google Scholar] [CrossRef] [PubMed]
- Henke, K. A model for memory systems based on processing modes rather than consciousness. Nat. Rev. Neurosci. 2010, 11, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Kawahata, M.; Ono, Y.; Ohno, A.; Kawamoto, S.; Kimoto, K.; Onozuka, M. Loss of molars early in life develops behavioral lateralization and impairs hippocampus-dependent recognition memory. BMC Neurosci. 2014, 15, 4. [Google Scholar] [CrossRef] [PubMed]
- Hirano, Y.; Obata, T.; Takahashi, H.; Tachibana, A.; Kuroiwa, D.; Takahashi, T.; Ikehira, H.; Onozuka, M. Effects of chewing on cognitive processing speed. Brain Cogn. 2013, 81, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Iinuma, M.; Onozuka, M.; Kubo, K.-Y. Chewing maintains hippocampus-dependent cognitive. Int. J. Med. Sci. 2015, 12, 502–509. [Google Scholar] [CrossRef]
- Lexomboon, D.; Trulsson, M.; Wårdh, I.; Parker, W.G. Chewing ability and tooth loss: Association with cognitive impairment in an elderly population study. J. Am. Geriatr. Soc. 2012, 60, 1951–1956. [Google Scholar] [CrossRef]
- Stein, P.S.; Desrosiers, M.; Donegan, S.J.; Yepes, J.F.; Kryscio, R.J. Tooth loss, dementia and neuropathology in the nun study. J. Am. Dent. Assoc. 2007, 138, 1314–1322. [Google Scholar] [CrossRef]
- Onishi, M.; Iinuma, M.; Tamura, Y.; Kubo, K.Y. Learning deficits and suppression of the cell proliferation in the hippocampal dentate gyrus of offspring are attenuated by maternal chewing during prenatal stress. Neurosci. Lett. 2014, 560, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Durán, D. Ignoring the life course: GES oral health for adults of 60 years. J. Oral Res. 2019, 8, 272–274. [Google Scholar] [CrossRef]
- Murray, C.J.L.; Lopez, A.D. The Global Burden of Disease: A Comprehensive Assessment of Mortality and Disability from Diseases, Injuries, and Risk Factors in 1990 and Projected to 2020; University Press on behalf of the World Health Organization and The World Bank: Boston, MA, USA; Harvard: Cambridge, MA, USA, 1996; Available online: https://apps.who.int/iris/handle/10665/41864 (accessed on 30 September 2020).
- Available online: https://vizhub.healthdata.org/gbd-compare/ (accessed on 28 August 2020).
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.L.; Marcenes, W. Global burden of severe tooth loss: A systematic review and meta-analysis. J. Dent. Res. 2014, 93 (Suppl. 7), 20S–28S. [Google Scholar] [CrossRef]
- Tan, H.; Peres, K.G.; Peres, M.A. Retention of teeth and oral health-related quality of life. J. Dent. Res. 2016, 95, 1350–1357. [Google Scholar] [CrossRef] [PubMed]
- Ricci, S.; Capecchi, G.; Boschin, F.; Arrighi, S.; Ronchitelli, A.; Condemi, S. Toothpick use among epigravettian humans from Grotta Paglicci (Italy). Int. J. Osteoarchaeo. 2016, 26, 281–289. [Google Scholar] [CrossRef]
- Lozano, M.; Subirà, M.; Aparicio, J.; Lorenzo, C.; Gomez-Merino, G. Toothpicking and periodontal disease in a neanderthal specimen from Cova Foradà Site (Valencia, Spain). PLoS ONE 2013, 8, e76852. [Google Scholar] [CrossRef] [PubMed]
- Coppa, A.; Bondioli, L.; Cucina, A.; Frayer, D.W.; Jarrige, C.; Jarrige, J.-F.; Quivron, G.; Rossi, M.; Vidale, M.; Macchiarelli, R. Early neolithic tradition of dentistry. Nature 2006, 440, 755–756. [Google Scholar] [CrossRef] [PubMed]
- Estalrrich, A.; Alarcon, J.A.; Rosas, A. Evidence of toothpick groove formation in neandertal anterior and posterior teeth. Am. J. Physic. Anthr. 2017, 162, 747–756. [Google Scholar] [CrossRef] [PubMed]
- Mantini, S.; Marini, M.; del Monte, S.; Mazza, D.; Primicerio, P.; Brea, M.B.; Salvadei, L. Early dentistry practice in Italian neolithic site of Gaione (Parma). Origini 2007, 29, 221–225. [Google Scholar]
- Dobrzański, L.A.; Dobrzański, L.B. Approach to the design and manufacturing of prosthetic dental restorations according to the rules of industry 4.0. Mater. Perform. Charact. 2020, 9, 394–476. [Google Scholar] [CrossRef]
- Oxilia, G.; Peresani, M.; Romandini, M.; Matteucci, C.; Debono Spiteri, C.; Henry, A.G.; Schulz, D.; Archer, W.; Crezzini, J.; Boschin, F.; et al. Earliest evidence of dental caries manipulation in the Late Upper Palaeolithic. Sci. Rep. 2015, 5, 1–10. [Google Scholar] [CrossRef]
- Allen, J.P. The Art of Medicine in Ancient Egypt; The Metropolitan Museum of Art: New York, NY, USA, 2005. [Google Scholar]
- Frayer, D.W.; Gatti, J.; Monge, J.; Radovčic, D. Prehistoric dentistry? P4 rotation, partial M3 impaction, toothpick grooves and other signs of manipulation in krapina dental person 20. Bull. Int. Assoc. Paleodont. 2017, 11, 1–10. [Google Scholar]
- Bernardini, F.; Tuniz, C.; Coppa, A.; Mancini, L.; Dreossi, D.; Eichert, D.; Turco, G.; Biasotto, M.; Terrasi, F.; De Cesare, N.; et al. Beeswax as dental filling on a neolithic human tooth. PLoS ONE 2012, 7, e44904. [Google Scholar] [CrossRef] [PubMed]
- Leek, F.F. The practice of dentistry in Ancient Egypt. J. Egypt. Archeol. 1967, 53, 51–58. [Google Scholar] [CrossRef]
- Wilwerding, T. History of Dentistry. The Free Information Society 2001. Available online: http://www.freeinfosociety.com/media/pdf/4551.pdf (accessed on 30 September 2020).
- Townend, B.R. Story of the tooth-worm. Bull. Hist. Med. 1944, 15, 37–58. [Google Scholar]
- Suddick, R.P.; Harris, N.O. Historical perspectives of oral biology: A series. Crit. Rev. Oral Biol. Med. 1990, 1, 135–151. [Google Scholar] [CrossRef] [PubMed]
- Dawson, W.R. Book review: The papyrus ebers; the greatest Egyptian medical document. J. Egypt. Archeol. 1938, 24, 250–251. [Google Scholar] [CrossRef]
- Seguin-Orlando, A.; Korneliussen, T.S.; Sikora, M.; Malaspinas, A.-S.; Manica, A.; Moltke, I.; Albrechtsen, A.; Ko, A.; Margaryan, A.; Moiseyev, V.; et al. Genomic structure in europeans dating back at least 36,200 years. Science 2014, 346, 1113–1118. [Google Scholar] [CrossRef]
- Reisine, S.; Litt, M. Social and psychological theories and their use for dental practice. Int. Dent. J. 1993, 43 (Suppl. 1), 279–287. [Google Scholar]
- Featherstone, J.D. The continuum of dental caries—Evidence for a dynamic disease process. J. Dent. Res. 2004, 83, C39–C42. [Google Scholar] [CrossRef]
- Pitts, N.B. A review of the current knowledge of the progress of approximal lesions. In Proceedings of the Scientific Proceedings of the 10th Asian Pacific Dental Congress, Singapore, 26–31 March 1981; Singapore Dental Association: Singapore, 1983; pp. 31–36. [Google Scholar]
- Amaechi, B.T. Remineralization therapies for initial caries lesions. Curr. Oral Health Rep. 2015, 2, 95–101. [Google Scholar] [CrossRef]
- Zero, D.T. Dentifrices, mouthwashes, and remineralization/caries arrestment strategies. BMC Oral Health 2006, 6, S9. [Google Scholar] [CrossRef] [PubMed]
- Holmgren, C.; Gaucher, N.; Decerle, N.; Doméjean, S. Minimal intervention dentistry II: Part 3. Management of non-cavitated (initial) occlusal caries lesions—Non-invasive approaches through remineralization and therapeutic sealants. Br. Dent. J. 2014, 216, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, N.; Nyvad, B. Caries ecology revisited: Microbial dynamics and the caries process. Caries Res. 2008, 42, 409–418. [Google Scholar] [CrossRef] [PubMed]
- Margolis, H.C.; Moreno, E.C. Composition and cariogenic potential of dental plaque fluid. Crit. Rev. Oral Biol. Med. 1994, 5, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Margolis, H.C.; Moreno, E.C. Kinetics of hydroxyapatite dissolution in acetic, lactic, and phosphoric acid solutions. Calcif. Tissue Int. 1992, 50, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Vogel, G.L.; Carey, C.M.; Chow, L.C.; Gregory, T.M.; Brown, W.E. Micro-analysis of mineral saturation within enamel during lactic acid demineralization. J. Dent. Res. 1988, 67, 1172–1180. [Google Scholar] [CrossRef]
- Ten Cate, J.M.; Featherstone, J.D. Mechanistic aspects of the interactions between fluoride and dental enamel. Crit. Rev. Oral Biol. Med. 1991, 2, 283–296. [Google Scholar] [CrossRef]
- Lee, Y.E.; Baek, H.J.; Choi, Y.H.; Jeong, S.H.; Park, Y.D.; Song, K.B. Comparison of remineralization effect of three topical fluoride regimens on enamel initial carious lesions. J. Dent. 2010, 38, 166–171. [Google Scholar] [CrossRef]
- Amaechi, B.T.; van Loveren, C. Fluorides and non-fluoride remineralization systems. Monogr. Oral Sci. 2013, 23, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Featherstone, J.D. Prevention and reversal of dental caries: Role of low level fluoride. Community Dent. Oral Epidemiol. 1999, 27, 31–40. [Google Scholar] [CrossRef]
- Iheozor-Ejiofor, Z.; Worthington, H.V.; Walsh, T.; O’Malley, L.; Clarkson, J.E.; Macey, R.; Alam, R.; Tugwell, P.; Welch, V.; Glenny, A.M. Water fluoridation for the prevention of dental caries. Cochrane Database Syst. Rev. 2015, 2015, CD010856. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, E.C.; Cai, F.; Shen, P.; Walker, G.D. Retention in plaque and remineralization of enamel lesions by various forms of calcium in a mouthrinse or sugar-free chewing gum. J. Dent. Res. 2003, 82, 206–211. [Google Scholar] [CrossRef] [PubMed]
- Kitasako, Y.; Sadr, A.; Hamba, H.; Ikeda, M.; Tagami, J. Gum containing calcium fluoride reinforces enamel subsurface lesions in situ. J. Dent. Res. 2012, 91, 370–375. [Google Scholar] [CrossRef] [PubMed]
- Hamba, H.; Nikaido, T.; Inoue, G.; Sadr, A.; Tagami, J. Effects of CPP-ACP with sodium fluoride on inhibition of bovine enamel demineralization: A quantitative assessment using micro-computed tomography. J. Dent. 2011, 39, 405–413. [Google Scholar] [CrossRef]
- Kidd, E.A.M.; Fejerskov, O. What constitutes dental caries? Histopathology of carious enamel and dentin related to the action of cariogenic biofilms. J. Dent. Res. 2004, 83, C35–C38. [Google Scholar] [CrossRef]
- Mandel, I.D. The functions of saliva. J. Dent. Res. 1987, 66, 623–627. [Google Scholar] [CrossRef]
- Hara, A.T.; Zero, D.T. The caries environment: Saliva, pellicle, diet, and hard tissue ultrastructure. Dent. Clin. North Am. 2010, 54, 455–467. [Google Scholar] [CrossRef]
- Zero, D.T. Sugars—The arch criminal? Caries Res. 2004, 38, 277–285. [Google Scholar] [CrossRef]
- Sheiham, A.; James, W.P.T. Diet and dental caries: The pivotal role of free sugars reemphasized. J. Dent. Res. 2015, 94, 1341–1347. [Google Scholar] [CrossRef]
- Marsh, P.D. Microbial ecology of dental plaque and its significance in health and disease. Adv. Dent. Res. 1994, 8, 263–271. [Google Scholar] [CrossRef]
- Zero, D.T. Adaptations in dental plaque. In Cariology for the Nineties; Bowen, W.H., Tabak, L., Eds.; University of Rochester Press: Rochester, NY, USA, 1993; pp. 333–350. [Google Scholar]
- Aas, J.A.; Griffen, A.L.; Dardis, S.R.; Lee, A.M.; Olsen, I.; Dewhirst, F.E.; Leys, E.J.; Paster, B.J. Bacteria of dental caries in primary and permanent teeth in children and young adults. J. Clin. Microbiol. 2008, 46, 1407–1417. [Google Scholar] [CrossRef] [PubMed]
- Kleinberg, I. A mixed-bacteria ecological approach to understanding the role of the oral bacteria in dental caries causation: An alternative to Streptococcus mutans and the specific-plaque hypothesis. Crit. Rev. Oral Biol. Med. 2002, 13, 108–125. [Google Scholar] [CrossRef] [PubMed]
- Arif, N.; Sheehy, E.C.; Do, T.; Beighton, D. Diversity of Veillonella spp. from sound and carious sites in children. J. Dent. Res. 2008, 87, 278–282. [Google Scholar] [CrossRef] [PubMed]
- Moynihan, P.J.; Kelly, S.A. Effect on caries of restricting sugars intake: Systematic review to inform WHO guidelines. J. Dent. Res. 2014, 93, 8–18. [Google Scholar] [CrossRef] [PubMed]
- Sheiham, A.; James, W.P. A reappraisal of the quantitative relationship between sugar intake and dental caries: The need for new criteria for developing goals for sugar intake. BMC Public Health 2014, 14, 863. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.-L.; Nascimento, M.; Burne, R.A. Progress toward understanding the contribution of alkali generation in dental biofilms to inhibition of dental caries. Int. J. Oral Sci. 2012, 4, 135–140. [Google Scholar] [CrossRef]
- Pollick, H.F. Salt fluoridation: A review. J. Calif. Dent. Assoc. 2013, 41, 395–404. [Google Scholar]
- Marinho, V.C.; Higgins, J.P.; Logan, S.; Sheiham, A. Topical fluoride (toothpastes, mouthrinses, gels or varnishes) for preventing dental caries in children and adolescents. Cochrane Database Syst. Rev. 2003, 4, CD002782. [Google Scholar] [CrossRef]
- Walsh, T.; Worthington, H.V.; Glenny, A.M.; Appelbe, P.; Marinho, V.C.; Shi, X. Fluoride toothpastes of different concentrations for preventing dental caries in children and adolescents. Cochrane Database Syst. Rev. 2010, 1, CD007868, Update in: Cochrane Database Syst Rev 2019, 3, CD007868. [Google Scholar] [CrossRef]
- Zero, D.T. The role of dietary control. In Dental Caries: The Disease and its Clinical Management, 2nd ed.; Fejerskov, O., Kidd, E., Eds.; Blackwell Munksgaard: Oxford, UK, 2008; pp. 329–352. [Google Scholar]
- Pollard, M.A.; Imfeld, T.; Higham, S.M.; Agalamanyi, E.A.; Curzon, M.E.; Edgar, W.M.; Borgia, S. Acidogenic potential and total salivary carbohydrate content of expectorants following the consumption of some cereal-based foods and fruits. Caries Res. 1996, 30, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Paes Leme, A.F.; Koo, H.; Bellato, C.M.; Bedi, G.; Cury, J.A. The role of sucrose in cariogenic dental biofilm formation—New insight. J. Dent. Res. 2006, 85, 878–887. [Google Scholar] [CrossRef] [PubMed]
- Cury, J.A.; Rebelo, M.A.; Del Bel Cury, A.A.; Derbyshire, M.T.; Tabchoury, C.P. Biochemical composition and cariogenicity of dental plaque formed in the presence of sucrose or glucose and fructose. Caries Res. 2000, 34, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Zero, D.T.; Fontana, M.; Martínez-Mier, E.A.; Ferreira-Zandoná, A.; Ando, M.; González-Cabezas, C.; Bayne, S. The biology, prevention, diagnosis and treatment of dental caries: Scientific advances in the United States. J. Am. Dent. Assoc. 2009, 140 (Suppl. 1), 25S–34S. [Google Scholar] [CrossRef] [PubMed]
- Hall, H.D.; Schneyer, C.A. Salivary gland atrophy in rat induced by liquid diet. Proc. Soc. Exp. Biol. Med. Soc. Exp. Biol. Med. 1964, 117, 789–793. [Google Scholar] [CrossRef] [PubMed]
- Wierichs, R.J.; Meyer-Lueckel, H. Systematic review on noninvasive treatment of root caries lesions. J. Dent. Res. 2015, 94, 261–271. [Google Scholar] [CrossRef] [PubMed]
- Clarkson, B.H.; Exterkate, R.A.M. Noninvasive dentistry: A dream or reality? Caries Res. 2015, 49 (Suppl. 1), 11–17. [Google Scholar] [CrossRef]
- Marsh, P.D.; Head, D.A.; Devine, D.A. Prospects of oral disease control in the future—An opinion. J. Oral Microbiol. 2014, 6, 261–276. [Google Scholar] [CrossRef]
- Dirks, O.B.; van Amerongen, J.; Winkler, K.C. A reproducible method for caries evaluation. J. Dent. Res. 1951, 30, 346–359. [Google Scholar] [CrossRef]
- Marthaler, T.M. A standardized system of recording dental conditions. Helv. Odontol. Acta 1966, 10, 1–18. [Google Scholar]
- Black, G.V. A Work on Operative Dentistry: The Technical Procedures in Filling Teeth; Medico-Dental Publishing: Chicago, IL, USA, 1917; p. 5. [Google Scholar]
- Ismail, A.I.; Sohn, W.; Tellez, M.; Amaya, A.; Sen, A.; Hasson, H.; Pitts, N.B. The international caries detection and assessment system (ICDAS): An integrated system for measuring dental caries. Community Dent. Oral Epidemiol. 2007, 35, 170–178. [Google Scholar] [CrossRef]
- ICDAS Website. Available online: https://www.icdas.org/. (accessed on 20 November 2020).
- Fejerskov, O.; Kidd, E. (Eds.) Dental Caries: The Disease and its Clinical Management, 2nd ed.; Blackwell Munksgaard: Oxford, UK, 2008. [Google Scholar]
- Fisher, J.; Glick, M. The FDI World Dental Federation. A new model for caries classification and management: The FDI World Dental Federation caries matrix. J. Am. Dent. Assoc. 2012, 143, 546–551. [Google Scholar] [CrossRef] [PubMed]
- Pitts, N.B.; Ekstrand, K.R. International caries detection and assessment system (ICDAS) and its international caries classification and management system (ICCMS)—Methods for staging of the caries process and enabling dentists to manage caries. Community Dent. Oral Epidemiol. 2013, 41, e41–e52. [Google Scholar] [CrossRef] [PubMed]
- Ismail, A.; Pitts, N.B.; Tellez, M. The international caries classification and management system (ICCMSTM) an example of a caries management pathway. BMC Oral Health 2015, 15, S9. [Google Scholar] [CrossRef] [PubMed]
- Ismail, A.; Tellez, M.; Pitts, N.B.; Ekstrand, K.R.; Ricketts, D.; Longbottom, C.; Eggertsson, H.; Deery, C.; Fisher, J.; Young, D.A.; et al. Caries management pathways preserve dental tissues and promote oral health. Community Dent. Oral Epidemiol. 2013, 41, e12–e40. [Google Scholar] [CrossRef] [PubMed]
- Ormond, C.; Douglas, G.; Pitts, N. The use of the international caries detection and assessment system (ICDAS) in a national health service general dental practice as part of an oral health assessment. Prim. Dent. Care 2010, 17, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Pitts, N.B. Discovering dental public health: From fisher to the future. Community Dent. Health 1994, 11, 172–178. [Google Scholar]
- Pitts, N.B. Modern concepts of caries measurement. J. Dent. Res. 2004, 83, 43–47. [Google Scholar] [CrossRef]
- Pitts, N.B. How the detection, assessment, diagnosis and monitoring of caries integrate with personalized caries management. Monogr. Oral Sci. 2009, 21, 1–14. [Google Scholar] [CrossRef]
- Pitts, N.B.; Fyffe, H.E. The effect of varying diagnostic thresholds upon clinical caries data for a low prevalence group. J. Dent. Res. 1988, 67, 592–596. [Google Scholar] [CrossRef]
- Pitts, N.; Melo, P.; Martignon, S.; Ekstrand, K.; Ismail, A. Caries risk assessment, diagnosis and synthesis in the context of a European core curriculum in cariology. Eur. J. Dent. Educ. 2011, 15 (Suppl. 1), 23–31. [Google Scholar] [CrossRef]
- Zandoná, A.F.; Zero, D.T. Diagnostic tools for early caries detection. J. Am. Dent. Assoc. 2006, 137, 1675–1684. [Google Scholar] [CrossRef] [PubMed]
- Ricketts, D.; Lamont, T.; Innes, N.P.; Kidd, E.; Clarkson, J.E. Operative caries management in adults and children. Cochrane Database Syst. Rev. 2013, 3, CD003808, Update in: Cochrane Database Syst. Rev. 2019, 7, CD003808. [Google Scholar] [CrossRef] [PubMed]
- ISO24234:2015 Dentistry — Dental amalgam; ISO: Geneva, Switzerland, 2015.
- FDA, About Dental Amalgam Fillings. Available online: https://www.fda.gov/medical-devices/dental-amalgam/about-dental-amalgam-fillings (accessed on 28 August 2020).
- SCENIHR (Scientific Committee on Emerging and Newly-Identified Health Risks). Opinion on the Safety of Dental Amalgam and Alternative Dental Restoration Materials for Patients and Users. European Union, 29 April 2015. Available online: https://ec.europa.eu/health/sites/health/files/scientific_committees/emerging/docs/scenihr_o_046.pdf (accessed on 28 August 2020).
- Council Decision (EU) 2017/939 of 11 May 2017 on the conclusion on behalf of the European Union of the Minamata Convention on Mercury. Off. J Eu Oj L 2017, 142, 4–39. Available online: http://data.europa.eu/eli/dec/2017/939/oj (accessed on 28 August 2020).
- Europejski Trybunał Praw Człowieka. Konwencja o Ochronie Praw Człowieka i Podstawowych Wolności sporządzona w Rzymie dnia 4 listopada 1950 r., zmieniona następnie Protokołami nr 3, 5 i 8 oraz uzupełniona Protokołem nr 2. Dz. U. 1993, 61, 284. Available online: https://www.echr.coe.int/Documents/Convention_POL.pdf (accessed on 28 August 2020).
- Schwartz, R.S.; Robbins, J.W. Post placement and restoration of endodontically treated teeth: A literature review. J. Endodon. 2004, 30, 289–301. [Google Scholar] [CrossRef] [PubMed]
- Peroz, I.; Blankenstein, F.; Lange, K.-P.; Naumann, M. Restoring endodontically treated teeth with post and cores—A review. Quintessence Int. 2005, 36, 737–746. [Google Scholar]
- Shutzky-Goldberg, I.; Shutzky, H.; Gorfil, C.; Smidt, A. Restoration of endodontically treated teeth review and treatment recommendations. Int. J. Dent. 2009, 2009, 150251. [Google Scholar] [CrossRef]
- Schilder, H.; Goodman, A.; Winthrop, A. The termomechanical properties of gutta-percha. Determination of phase transition temperatures for gutta-percha. Oral Surg. Oral Med. Oral Pathol. 1974, 38, 109–114. [Google Scholar] [CrossRef]
- Combe, E.C.; Cohen, B.D.; Cumming, K. Alpha- and beta-forms of gutta-percha in products for root canal filling. Int. Endodon. J. 2001, 34, 447–451. [Google Scholar] [CrossRef]
- Ferreira, C.M.; Silva, J.B.A., Jr.; Monteiro de Paula, R.C.; Andrade Feitosa, J.P.; Negreiros Cortez, D.G.; Zaia, A.A.; de Souza-Filho, F.J. Brazilian gutta-percha points. Part I: Chemical composition and X-ray diffraction analysis. Braz. Oral Res. 2005, 19, 193–197. [Google Scholar] [CrossRef]
- Ferreira, C.M.; Gurgel-Filho, E.D.; Silva, J.B.A., Jr.; Monteiro de Paula, R.C.; Pessoa Andrade Feitosa, J.; Figueiredo de Almeida Gomes, B.P.; de Souza-Filho, F.J. Brazilian gutta-percha points. Part II: Thermal properties. Braz. Oral Res. 2007, 21, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Dobrzańska, J.; Gołombek, K.; Dobrzański, L.B. Polymer materials used in endodontic treatment—In vitro testing. AMSE 2012, 58, 110–115. [Google Scholar]
- Dobrzańska, J. Analiza Szczelności Wypełnień Kanałów Korzeniowych. Ph.D. Thesis, Śląski Uniwersytet Medyczny w Katowicach, Zabrze, Poland, 2011. [Google Scholar]
- Sunay, H.; Tanalp, J.; Dikbas, I.; Bayirli, G. Cross-sectional evaluation of the periapical status and quality of root canal treatment in a selected population of urban Turkish adults. Int. Endodon. J. 2007, 40, 139–145. [Google Scholar] [CrossRef]
- Meuwissen, R.; Eschen, S. Twenty years of endodontic treatment. J. Endodon. 1983, 9, 390–393. [Google Scholar] [CrossRef]
- Lazarski, M.P.; Walker, W.A.; Flores, C.M.; Schindler, W.G.; Hargreaves, K.M. Epidemiological evaluation of the outcomes of nonsurgical root canal treatment in a large cohort of insured dental patients. J. Endodon. 2001, 27, 791–796. [Google Scholar] [CrossRef] [PubMed]
- Kirkevang, L.L.; Horsted-Bindslev, P.; Orstavik, D.; Wenzel, A. Frequency and distribution of endodontically treated teeth and apical periodontitis in an urban Danish population. Int. Endodon. J. 2001, 34, 198–205. [Google Scholar] [CrossRef] [PubMed]
- Tsuneishi, M.; Yamamoto, T.; Yamanaka, R.; Tamaki, N.; Sakamoto, T.; Tsuji, K.; Watanabe, T. Radiographic evaluation of periapical status and prevalence of endodontic treatment in an adult Japanese population. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2005, 100, 631–635. [Google Scholar] [CrossRef]
- Chen, S.C.; Chuech, L.H.; Hsiao, C.K.; Tsai, M.Y.; Ho, S.C.; Chiang, C.P. An epidemiologic study of tooth retention after nonsurgical endodontic treatment in a large population in Taiwan. J. Endodon. 2007, 33, 226–229. [Google Scholar] [CrossRef]
- Salehrabi, R.; Rotstein, I. Endodontic treatment outcomes in a large patient population in the USA: An epidemiological study. J. Endodon. 2004, 30, 846–850. [Google Scholar] [CrossRef]
- Genco, R.J.; Borgnakke, W.S. Risk factors for periodontal disease. Periodontol. 2000 2013, 62, 59–94. [Google Scholar] [CrossRef]
- Martinez-Canut, P.; Llobell, A.; Romero, A. Predictors of long-term outcomes in patients undergoing periodontal maintenance. J. Clin. Periodontol. 2017, 44, 620–631. [Google Scholar] [CrossRef] [PubMed]
- Van Dyke, T.E.; Dave, S. Risk factors for periodontitis. J. Int. Acad. Periodontol. 2005, 7, 3–7. [Google Scholar] [PubMed]
- Hasan, A.; Palmer, R.M. A clinical guide to periodontology: Pathology of periodontal disease. Br. Dent. J. 2014, 216, 457–461. [Google Scholar] [CrossRef] [PubMed]
- Isola, G.; Polizzi, A.; Iorio-Siciliano, V.; Alibrandi, A.; Ramaglia, L.; Leonardi, R. Effectiveness of a nutraceutical agent in the non-surgical periodontal therapy: A randomized, controlled clinical trial. Clin. Oral Invest. 2020. (Published online 17 June 2020). [Google Scholar] [CrossRef] [PubMed]
- Neiva, R.F.; Steigenga, J.; Al-Shammari, K.F.; Wang, H.-L. Effects of specific nutrients on periodontal disease onset, progression and treatment. J. Clin. Periodontol. 2003, 30, 579–589. [Google Scholar] [CrossRef]
- Marsh, P.D.; Zaura, E. Dental biofilm: Ecological interactions in health and disease. J. Clin. Periodontol. 2017, 44 (Suppl. 18), S12–S22. [Google Scholar] [CrossRef]
- Highfield, J. Diagnosis and classification of periodontal disease. Aust. Dent. J. 2009, 54, S11–S26. [Google Scholar] [CrossRef]
- Lee, J.-H.; Oh, J.-Y.; Choi, J.-K.; Kim, Y.-T.; Park, Y.-S.; Jeong, S.-N.; Choi, S.-H. Trends in the incidence of tooth extraction due to periodontal disease: Results of a 12-year longitudinal cohort study in South Korea. J. Periodont. Implant. Sci. 2017, 47, 264–272. [Google Scholar] [CrossRef]
- McCaul, L.K.; Jenkins, W.M.M.; Kay, E.J. The reasons for extraction of permanent teeth in Scotland: A 15-year follow-up study. Br. Dent. J. 2001, 190, 658–662. [Google Scholar] [CrossRef]
- Carnevale, G.; Pontoriero, R.; Lindhe, J. Treatment of furcation-involved teeth. In Clinical Periodontology and Impant Dentistry; Lindhe, J., Karring, T., Lang, N.P., Eds.; Munksgaard: Copenhagen, Denmark, 1997; pp. 682–710. [Google Scholar]
- Papapanou, P.N.; Toneti, M.S. Diagnosis and epidemiology of periodontal osseous lesions. Periodontol. 2000 2000, 22, 8–21. [Google Scholar] [CrossRef]
- Nordland, P.; Garrett, S.; Kiger, R.; Vanooteghem, R.; Hutchens, L.H.; Egelberg, J. The effect of plaque control and root debridement in molar teeth. J. Clin. Periodontol. 1987, 14, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Hirschfeld, L.; Wasserman, B.A. Long-term survey of tooth loss in 600 treated periodontal patients. J. Periodontol. 1978, 49, 225–237. [Google Scholar] [CrossRef] [PubMed]
- McGuire, M.K.; Nunn, M.E. Prognosis versus actual outcome. III. The effectiveness of clinical parametrs in accurately predicting tooth survival. J. Periodontol. 1966, 67, 666–674. [Google Scholar] [CrossRef] [PubMed]
- De Vries, K. Primary care: Gingivitis. Aust. J. Pharm. 2015, 96, 64. [Google Scholar]
- Azaripour, A.; Weusmann, J.; Eschig, C.; Schmidtmann, I.; Van Noorden, C.J.F.; Willershausen, B. Efficacy of an aluminium triformate mouthrinse during the maintenance phase in periodontal patients: A pilot double blind randomized placebo-controlled clinical trial. BMC Oral Health 2016, 16, 57. [Google Scholar] [CrossRef] [PubMed]
- Pradeep, K.; Rajababu, P.; Satyanarayana, D.; Sagarm, V. Gingival recession: Review and strategies in treatment of recession. Case Rep. Dent. 2012, 2012, 563421. [Google Scholar] [CrossRef] [PubMed]
- Scottish Dental Clinical Effectiveness Programme. Prevention and Treatment of Periodontal Diseases in Primary Care, Dental Clinical Guidance. Dundee Dental Education Centre: Dundee, 2014. Available online: https://www.sdcep.org.uk/wp-content/uploads/2015/01/SDCEP+Periodontal+Disease+Full+Guidance.pdf (accessed on 30 September 2020).
- Roos-Jansåker, A.-M.; Egelberg, S.R.J. Treatment of peri-implant infections: A literature review. J. Clin. Periodontol. 2003, 30, 467–485. [Google Scholar] [CrossRef]
- Wiebe, C.B.; Putnins, E.E. The periodontal disease classification system of the American academy of periodontology—An update. J. Can. Den. Assoc. 2000, 66, 594–597. [Google Scholar]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.C.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Periodontol. 2018, 89, S1–S8. [Google Scholar] [CrossRef]
- Scannapieco, F.A.; Gershovich, E. The prevention of periodontal disease—An overview. Periodontol. 2000 2020, 84, 9–13. [Google Scholar] [CrossRef]
- Armitage, G.C. Periodontal diagnoses and classification of periodontal diseases. Periodontol. 2000 2004, 34, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Preshaw, P.M. Detection and diagnosis of periodontal conditions amenable to prevention. BMC Oral Health 2015, 15, S1–S5. [Google Scholar] [CrossRef] [PubMed]
- Walter, C.; Schmidt, J.C.; Dula, K.; Sculean, A. Cone beam computed tomography (CBCT) for diagnosis and treatment planning in periodontology: A systematic review. Quintessence Int. 2016, 47, 26–37. [Google Scholar] [CrossRef]
- Woelber, J.P.; Fleiner, J.; Rau, J.; Ratka-Krüger, P.; Hannig, C. Accuracy and usefulness of CBCT in periodontology: A systematic review of the literature. Int. J. Periodontics. Restor. Dent. 2018, 38, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Walter, C.; Schmidt, J.C.; Rinne, C.A.; Mendes, S.; Dula, K.; Sculean, A. Cone beam computed tomography (CBCT) for diagnosis and treatment planning in periodontology: Systematic review update. Clin. Oral Investig. 2020, 24, 2943–2958. [Google Scholar] [CrossRef]
- Acar, B.; Kamburoğlu, K. Use of cone beam computed tomography in periodontology. World J. Radiol. 2014, 6, 139–147. [Google Scholar] [CrossRef]
- Du Bois, A.H.; Kardachi, B.; Bartold, P.M. Is there a role for the use of volumetric cone beam computed tomography in periodontics? Aust. Dent. J. 2012, 57 (Suppl. 1), 103–108. [Google Scholar] [CrossRef]
- Basic Periodontal Examination (BPE). The British Society of Periodontology. 2011. Available online: https://www.bsperio.org.uk/assets/downloads/BPE_Guidelines_2011.pdf (accessed on 20 November 2020).
- Vandana, K.L.; Haneet, R.K. Cementoenamel junction: An insight. J. Indian Soc. Periodontol. 2014, 18, 549–554. [Google Scholar] [CrossRef]
- Dufty, J.; Gkranias, N.; Donos, N. Necrotising ulcerative gingivitis: A literature review. Oral Health Prev. Dent. 2017, 15, 321–327. [Google Scholar] [CrossRef]
- Furuta, M.; Fukai, K.; Aida, J.; Shimazaki, Y.; Ando, Y.; Miyazaki, H.; Kambara, M.; Yamashita, Y. Periodontal status and self-reported systemic health of periodontal patients regularly visiting dental clinics in the 8020 promotion foundation study of Japanese dental patients. J. Oral Sci. 2019, 61, 238–245. [Google Scholar] [CrossRef]
- Lang, N.; Bartold, P.M.; Cullinan, M.; Jeffcoat, M.; Mombelli, A.; Murakami, S.; Page, R.; Papapanou, P.; Tonetti, M.; Van Dyke, T. Consensus report: Aggressive periodontitis. Ann. Periodontol. 1999, 4, 53. [Google Scholar] [CrossRef]
- Kinane, D.F.; Marshall, G.J. Peridonatal manifestations of systemic disease. Aust. Dent. J. 2008, 46, 2–12. [Google Scholar] [CrossRef] [PubMed]
- Mohd-Dom, T.; Ayob, R.; Mohd-Nur, A.; Abdul-Manaf, M.R.; Ishak, N.; Abdul-Muttalib, K.; Aljunid, S.M.; Ahmad-Yaziz, Y.; Abdul-Aziz, H.; Kasan, N.; et al. Cost analysis of periodontitis management in public sector specialist dental clinics. BMC Oral Health 2014, 14, 56. [Google Scholar] [CrossRef] [PubMed]
- Brånemark, P.-I.; Adell, R.; Breine, U.; Hansson, B.O.; Lindström, J.; Ohlsson, A. Intraosseous anchorage of dental prosthesis. I Experimental studies. Scand. J. Plast. Reconstr. Surg. 1969, 3, 81–100. [Google Scholar] [CrossRef] [PubMed]
- Brånemark, P.-I.; Hansson, B.O.; Adell, R.; Breine, U.; Lindström, J.; Hallén, O.; Ohman, A. Osseointegrated implants in the treatment of the edentulous jaw. Experience from a 10-year period. Scand. J. Plast. Reconstr. Surg. Suppl. 1977, 16, 1–132. [Google Scholar]
- Brånemark, P.-I.; Hansson, B.O.; Adell, R.; Breine, U.; Lindström, J.; Hallén, O.; Ohman, A. Osseointegrated Implants in the Treatment of the Edentulous Jaw; Almqvist and Wiksell: Stockholm, Sweden, 1977. [Google Scholar]
- Brånemark, P.-I. Osseointegration and its experimental studies. J. Prosthet. Dent. 1983, 50, 399. [Google Scholar] [CrossRef]
- Brånemark, P.-I.; Rydevik, B.L.; Skalak, R. (Eds.) Osseointegration in Skeletal Reconstruction and Joint Replacement; Quintessence Publishing Co.: Carol Stream, IL, USA, 1997. [Google Scholar]
- Kagermann, H.; Wahlster, W.; Helbig, J. Recommendations for Implementing the Strategic Initiative Industrie 4.0: Final Report of the Industrie 4.0 Working Group; Federal Ministry of Education and Research: Bonn, Germany, 2013.
- Rüßmann, M.; Lorenz, M.; Gerbert, P.; Waldner, M.; Justus, J.; Engel, P.; Harnisch, M. Industry 4.0: The Future of Productivity and Growth in Manufacturing Industries; Boston Consulting Group: Boston, MA, USA, 2015. [Google Scholar]
- Hermann, M.; Pentek, T.; Otto, B. Design principles for industrie 4.0 scenarios. In Proceedings of the 2016 49th Hawaii International Conference on System Sciences (HICSS), Koloa, HI, USA, 5–8 January 2016; pp. 3928–3937. [Google Scholar] [CrossRef]
- Jose, R.; Ramakrishna, S. Materials 4.0: Materials big data enabled materials discovery. Appl. Mater. Today 2018, 10, 127–132. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzańska-Danikiewicz, A.D. Why are carbon-based materials important in civilization progress and especially in the industry 4.0 stage of the industrial revolution. Mater. Perform. Charact. 2019, 8, 337–370. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzański, L.B. Dentistry 4.0 concept in the design and manufacturing of prosthetic dental restorations. Processes 2020, 8, 525. [Google Scholar] [CrossRef]
- Beuer, F.; Schweiger, J.; Edelhoff, D. Digital dentistry: An overview of recent developments for CAD/CAM generated restorations. Br. Dent. J. 2008, 204, 505–511. [Google Scholar] [CrossRef]
- Nejatian, T.; Almassi, S.; Shamsabadi, A.F.; Vasudeva, G.; Hancox, Z.; Singh Dhillon, A.; Sefat, F. Digital dentistry. In Advanced Dental Biomaterials; Khurshid, Z., Najeeb, S., Zafar, M.S., Sefat, F., Eds.; Woodhead Publishing: London, UK, 2019; pp. 507–540. [Google Scholar] [CrossRef]
- Blatz, M.B.; Conejo, J. The current state of chairside digital dentistry and materials. Dent. Clin. North Am. 2019, 63, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Sulaiman, T.A. Materials in digital dentistry—A review. J. Esthet. Restor. Dent. 2020, 32, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Valizadeh, S.; Valilai, O.F.; Houshmand, M.; Vasegh, Z. A novel digital dentistry platform based on cloud manufacturing paradigm. Int. J. Comp. Integr. Manufac. 2019, 32, 1024–1042. [Google Scholar] [CrossRef]
- Rekow, E.D. Digital dentistry: The new state of the art—Is it disruptive or destructive? Dent. Mater. 2020, 36, 9–24. [Google Scholar] [CrossRef] [PubMed]
- U533; Kaye, G. Does Digital Dentist Mean Anything Today? 6 December 2017. Available online: https://www.dentaleconomics.com/science-tech/article/16389518/does-digital-dentist-mean-anything-today (accessed on 9 October 2020).
- Dobrzański, L.A. Role of materials design in maintenance engineering in the context of industry 4.0 idea. JAMME 2019, 96, 12–49. [Google Scholar] [CrossRef]
- Dobrzański, L.A. (Ed.) Metale i ich stopy. In Open Access Library; VII, 2; International OCSCO World Press: Gliwice, Poland, 2017. [Google Scholar]
- Dobrzański, L.A. Significance of materials science for the future development of societies. J. Mater. Process. Technol. 2006, 175, 1–3, 133–148. [Google Scholar] [CrossRef]
- Wilson, C.E.; Dhert, W.J.A.; van Blitterswijk, C.A.; Verbout, A.J.; de Bruijn, J.D. Evaluating 3D bone tissue engineered constructs with different seeding densities using the alamarBlue™ assay and the effect on in vivo bone formation. J. Mater. Sci. Mater. Med. 2002, 13, 1265–1269. [Google Scholar] [CrossRef] [PubMed]
- Folkman, J. Tumor angiogenesis: Therapeutic implications. N. Eng. J. Med. 1971, 285, 1182–1186. [Google Scholar] [CrossRef]
- Noga, M.; Pawlak, A.; Dybala, B.; Dabrowski, B.; Swieszkowski, W.; Lewandowska-Szumiel, M. Biological Evaluation of Porous Titanium Scaffolds (Ti-6Al-7Nb) with HAp/Ca-P Surface Seeded with Human Adipose Derived Stem Cells; E-MRS Fall Meeting: Warszawa, Poland, 2013. [Google Scholar]
- Rouwkema, J.; Rivron, N.C.; van Blitterswijk, C.A. Vascularization in tissue engineering. Trends Biotechnol. 2008, 26, 434–441. [Google Scholar] [CrossRef]
- Bramfeldt, H.; Sabra, G.; Centis, V.; Vermette, P. Scaffold vascularization: A challenge for three-dimensional tissue engineering. Curr. Med. Chem. 2010, 17, 3944–3967. [Google Scholar] [CrossRef]
- Bose, S.; Roy, M.; Bandyopadhyay, A. Recent advances in bone tissue engineering scaffolds. Trends Biotechnol. 2012, 30, 546–554. [Google Scholar] [CrossRef] [PubMed]
- Jain, R.K.; Au, P.; Tam, J.; Duda, D.G.; Fukumura, D. Engineering vascularized tissue. Nat. Biotechnol. 2005, 23, 821–823. [Google Scholar] [CrossRef] [PubMed]
- Prendergast, P.; Huiskes, R. Microdamage and osteocyte-lacuna strain in bone: A microstructural finite element analysis. J. Biomech. Eng. 1996, 118, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Bettinger, C.J.; Borenstein, J.T.; Langer, R. Microfabrication techniques in scaffold development. In Nanotechnology and Tissue Engineering: The Scaffold; Laurencin, C.T., Nair, L.S., Eds.; CRC Press Taylor & Francis Group: Boca Raton, FL, USA, 2008. [Google Scholar]
- Bentolila, V.; Boyce, T.M.; Fyhrie, D.P.; Drumb, R.; Skerry, T.M.; Schaffler, M.B. Intracortical remodeling in adult rat long bones after fatigue loading. Bone 1998, 23, 275–281. [Google Scholar] [CrossRef]
- Ramirez, J.M.; Hurt, W.C. Bone remodeling in periodontal lesions. J. Periodontol. 1977, 48, 74–77. [Google Scholar] [CrossRef]
- Wang, X.; Ni, Q. Determination of cortical bone porosity and pore size distribution using a low field pulsed NMR approach. J. Orthop. Res. 2003, 21, 312–319. [Google Scholar] [CrossRef]
- Kufahl, R.H.; Saha, S.A. A theoretical model for stress-generated fluid flow in the canaliculi-lacunae network in bone tissue. J. Biomech. 1990, 23, 171–180. [Google Scholar] [CrossRef]
- Sietsema, W.K. Animal models of cortical porosity. Bone 1995, 17 (Suppl. 4), S297–S305. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzańska-Danikiewicz, A.D.; Czuba, Z.P.; Dobrzański, L.B.; Achtelik-Franczak, A.; Malara, P.; Szindler, M.; Kroll, L. The new generation of the biological-engineering materials for applications in medical and dental implant-scaffolds. AMSE 2018, 91, 56–85. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzańska-Danikiewicz, A.D.; Czuba, Z.P.; Dobrzański, L.B.; Achtelik-Franczak, A.; Malara, P.; Szindler, M.; Kroll, L. Metallic skeletons as reinforcement of new composite materials applied in orthopaedics and dentistry. AMSE 2018, 92, 53–85. [Google Scholar] [CrossRef]
- Dikova, T.; Dzhendov, D.; Simov, M. Microstructure and hardness of fixed dental prostheses manufactured by additive technologies. JAMME 2015, 71, 60–69. [Google Scholar]
- Dobrzański, L.A. (Ed.) Biomaterials in Regenerative Medicine; IntechOpen: Rijeka, Croatia, 2018. [Google Scholar] [CrossRef]
- Dobrzański, L.A. (Ed.) Powder Metallurgy—Fundamentals and Case Studies; InTech: Rijeka, Croatia, 2017. [Google Scholar]
- Dobrzański, L.A.; Dobrzańska-Danikiewicz, A.D. (Eds.) Metalowe Materiały Mikroporowate I Lite Do Zastosowań Medycznych I Stomatologicznych; International OCSCO World Press: Gliwice, Poland, 2017. [Google Scholar]
- Dobrzański, L.A.; Dobrzańska-Danikiewicz, A.D.; Achtelik-Franczak, A.; Dobrzański, L.B. Comparative analysis of mechanical properties of scaffolds sintered from Ti and Ti6Al4V powders. AMSE 2015, 73, 69–81. [Google Scholar]
- Brandt, M. (Ed.) Laser Additive Manufacturing; Materials, Design, Technologies and Applications; Woodhead Publishing: Sawston, UK, 2017. [Google Scholar]
- Dikova, T. Properties of Co-Cr dental alloys fabricated using additive technologies. In Biomaterials in Regenerative Medicine; Dobrzański, L.A., Ed.; IntechOpen: Rijeka, Croatia, 2018; pp. 141–159. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzańska-Danikiewicz, A.D.; Gaweł, T.G.; Achtelik-Franczak, A. Selective laser sintering and melting of pristine titanium and titanium Ti6Al4V alloy powders and selection of chemical environment for etching of such materials. Arch. Met. Mater. 2015, 60, 2039–2045. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzańska-Danikiewicz, A.D.; Achtelik-Franczak, A.; Dobrzański, L.B.; Szindler, M.; Gaweł, T.G. Porous selective laser melted Ti and Ti6Al4V materials for medical applications. In Powder Metallurgy—Fundamentals and Case Studies; Dobrzański, L.A., Ed.; IntechOpen: Rijeka, Croatia, 2017; pp. 161–181. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Matula, G.; Dobrzańska-Danikiewicz, A.D.; Malara, P.; Kremzer, M.; Tomiczek, B.; Kujawa, M.; Hajduczek, E.; Achtelik-Franczak, A.; Dobrzański, L.B.; et al. Composite materials infiltrated by aluminium alloys based on porous skeletons from alumina, mullite and titanium produced by powder metallurgy techniques. In Powder Metallurgy—Fundamentals and Case Studies; Dobrzański, L.A., Ed.; IntechOpen: Rijeka, Croatia, 2017; pp. 95–137. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzańska-Danikiewicz, A.D.; Achtelik-Franczak, A.; Dobrzański, L.B.; Hajduczek, E.; Matula, G. Fabrication technologies of the sintered materials including materials for medical and dental application. In Powder Metallurgy—Fundamentals and Case Studies; Dobrzański, L.A., Ed.; IntechOpen: Rijeka, Croatia, 2017; pp. 17–52. [Google Scholar] [CrossRef]
- Majkowska, B.; Jażdżewska, M.; Wołowiec, E.; Piekoszewski, W.; Klimek, L.; Zieliński, A. The possibility of use of laser-modified Ti6Al4V alloy in friction pairs in endoprostheses. Arch. Met. Mater. 2015, 60, 755–758. [Google Scholar] [CrossRef]
- Das, S.; Wohlert, M.; Beaman, J.J.; Bourell, D.L. Producing metal parts with selective laser sintering/hot isostatic pressing. JOM 1998, 50, 17–20. [Google Scholar] [CrossRef]
- Duan, B.; Wang, M.; Zhou, W.Y.; Cheung, W.L.; Li, Z.Y.; Lu, W.W. Three-dimensional nanocomposite scaffolds fabricated via selective laser sintering for bone tissue engineering. Acta Biomater. 2010, 6, 4495–4505. [Google Scholar] [CrossRef]
- Herzog, D.; Seyda, V.; Wycisk, E.; Emmelmann, C. Additive manufacturing of metals. Acta Mater. 2016, 117, 371–392. [Google Scholar] [CrossRef]
- Frazier, W.E. Metal additive manufacturing: A review. J. Mater. Eng. Perform. 2014, 23, 1917–1928. [Google Scholar] [CrossRef]
- Malara, P.; Dobrzański, L.B.; Dobrzańska, J. Computer-aided designing and manufacturing of partial removable dentures. JAMME 2015, 73, 157–164. [Google Scholar]
- Żmudzki, J.; Chladek, G.; Kasperski, J. Biomechanical factors related to occlusal load transfer in removable complete dentures. Biomech. Model Mechanobiol. 2015, 14, 679–691. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzańska-Danikiewicz, A.D.; Achtelik-Franczak, A.; Szindler, M. Structure and properties of the skeleton microporous materials with coatings inside the pores for medical and dental applications. In Frontiers in Materials Processing, Applications, Research and Technology; Muruganant, M., Chirazi, A., Raj, B., Eds.; Springer: Singapore, 2018; pp. 297–320. [Google Scholar] [CrossRef]
- Dikova, T.; Dzhendov, D.; Simov, M.; Katreva-Bozukova, I.; Angelova, S.; Pavlova, D.; Abadzhiev, M.; Tonchev, T. Modern trends in the development of the technologies for production of dental constructions. J. IMAB Ann. Proc. (Sci. Pap.) 2015, 21, 974–981. [Google Scholar] [CrossRef]
- Gupta, S.; Kumar, S. Lasers in dentistry—An overview. Trends Biomaterartif. Organs. 2011, 25, 119–123. [Google Scholar]
- Olmos, L.; Cabezas-Villa, J.L.; Bouvard, D.; Lemus-Ruiz, J.; Jiménez, O.; Falcón-Franco, L.A. Synthesis and characterisation of Ti6Al4V/xTa alloy processed by solid state sintering. Powder Met. 2020, 63, 64–74. [Google Scholar] [CrossRef]
- Esen, Z.; Bor, S. Processing of titanium foams using magnesium spacer particles. Scr. Mater. 2007, 56, 341–344. [Google Scholar] [CrossRef]
- Dobrzański, L.B. Mechanical properties comparison of engineering materials produced by additive and substractive technologies for dental prosthetic restoration application. In Biomaterials in Regenerative Medicine; Dobrzański, L.A., Ed.; IntechOpen: Rijeka, Croatia, 2018; pp. 111–140. [Google Scholar] [CrossRef]
- Dobrzański, L.A. The concept of biologically active microporous engineering materials and composite biological-engineering materials for regenerative medicine and dentistry. AMSE 2016, 80, 64–85. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzańska-Danikiewicz, A.D.; Gaweł, T.G. Individual implants of a loss of palate fragments fabricated using SLM equipment. JAMME 2016, 77, 24–30. [Google Scholar] [CrossRef]
- Bram, M.; Schiefer, H.; Bogdanski, D.; Köller, M.; Buchkremer, H.P.; Stöver, D. Implant surgery: How bone bonds to PM titanium. Met. Pow. Rep. 2006, 61, 26–28, 30–31. [Google Scholar] [CrossRef]
- Bram, M.; Stiller, C.; Buchkremer, H.P.; Stover, D.; Bauer, H. High-porosity titanium, stainless steel, and superalloy parts. Adv. Eng. Mat. 2000, 2, 196–199. [Google Scholar] [CrossRef]
- Reis de Vasconcellos, L.M.; Varella de Oliveira, M.; Lima de Alencastro Graça, M.; Oliveira de Vasconcellos, L.G.; Carvalho, Y.R.; Cairo, C.A.A. Porous titanium scaffolds produced by powder metallurgy for biomedical applications. Mat. Res. 2008, 11, 275–280. [Google Scholar] [CrossRef]
- Ryan, G.; Pandit, A.; Apatsidis, D.P. Fabrication methods of porous metals for use in orthopaedic applications. Biomaterials 2006, 27, 2651–2670. [Google Scholar] [CrossRef]
- Dobrzański, L.B.; Achtelik-Franczak, A.; Dobrzańska, J.; Pietrucha, P. Application of polymer impression masses for the obtaining of dental working models for the stereolithographic 3D printing. AMSE 2019, 95, 31–40. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzański, L.B.; Dobrzańska-Danikiewicz, A.D. Additive and hybrid technologies for products manufacturing using powders of metals, their alloys and ceramics. AMSE 2020, 102, 59–85. [Google Scholar] [CrossRef]
- Dobrzańska-Danikiewicz, A.D. The state of the art analysis and methodological assumptions of evaluation and development prediction for materials surface technologies. JAMME 2011, 49, 121–141. [Google Scholar]
- Dobrzańska-Danikiewicz, A.D. Metodologia komputerowo zintegrowanego prognozowania rozwoju inżynierii powierzchni materiałów. In Open Access Library; 1, 7; Dobrzański, L.A., Ed.; International OCSCO World Press: Gliwice, Poland, 2012. [Google Scholar]
- Dobrzańska-Danikiewicz, A.D. Księga Technologii Krytycznych Kształtowania Struktury I Własności Powierzchni Materiałów Inżynierskich; International OCSCO World Press: Gliwice, Poland, 2013. [Google Scholar]
- Dobrzańska-Danikiewicz, A.D. Foresight of material surface engineering as a tool building a knowledge based economy. Mater. Sci. Forum 2012, 706–709, 2511–2516. [Google Scholar] [CrossRef]
- Harrison, T. The Emergence of the Fourth Industrial Revolution in Dentistry, 25 April 2018. Available online: https://www.dentistryiq.com/practice-management/industry/article/16366877/the-emergence-of-the-fourth-industrial-revolution-in-dentistry (accessed on 9 October 2020).
- Dobrzański, L.B.; Achtelik-Franczak, A.; Dobrzańska, J.; Dobrzański, L.A. The digitisation for the immediate dental implantation of incisors with immediate individual prosthetic restoration. JAMME 2019, 97, 57–68. [Google Scholar] [CrossRef]
- Galanis, C.C.; Sfantsikopoulos, M.M.; Koidis, P.T.; Kafantaris, N.M.; Mpikos, P.G. Computer methods for automating preoperative dental implant planning: Implant positioning and size assignment. Comp. Methods Programs Biomed. 2007, 86, 30–38. [Google Scholar] [CrossRef]
- Miyazaki, T.; Hotta, Y. CAD/CAM systems available for the fabrication of crown and bridge restorations. Aust. Dent. J. 2011, 56, 97–106. [Google Scholar] [CrossRef]
- Malara, P.; Dobrzański, L.B. Computer-aided design and manufacturing of dental surgical guides based on cone beam computed tomography. AMSE 2015, 76, 140–149. [Google Scholar]
- Malara, P.; Dobrzański, L.B. Designing and manufacturing of implantoprosthetic fixed suprastructures in edentulous patients on the basis of digital impressions. AMSE 2015, 76, 163–171. [Google Scholar]
- Ender, A.; Zimmermann, M.; Attin, T.; Mehl, A. In vivo precision of conventional and digital methods for obtaining quadrant dental impressions. Clin. Oral Investig. 2016, 20, 1495–1504. [Google Scholar] [CrossRef]
- Van Noort, R. The future of dental devices is digital. Dent. Mater. 2012, 28, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Dobrzańska-Danikiewicz, A.; Dobrzański, L.A.; Gaweł, T.G. Scaffolds applicable as implants of a loss palate fragments. In International Conference on Processing & Manufacturing of Advanced Materials. Processing, Fabrication, Properties, Applications; THERMEC’2016: Graz, Austria, 2016; p. 193. [Google Scholar]
- Liacouras, P.; Garnes, J.; Roman, N.; Petrich, A.; Grant, G.T. Designing and manufacturing an auricular prosthesis using computed tomography, 3-dimensional photographic imaging, and additive manufacturing: A clinical report. J. Prosthet. Dent. 2011, 105, 78–82. [Google Scholar] [CrossRef]
- Maroulakos, M.; Kamperos, G.; Tayebi, L.; Halazonetis, D.; Ren, Y. Applications of 3D printing on craniofacial bone repair: A systematic review. J. Dent. 2019, 80, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Warnke, P.H.; Douglas, T.; Wollny, P.; Sherry, E.; Steiner, M.; Galonska, S.; Becker, S.T.; Springer, I.N.; Wiltfang, J.; Sivananthan, S. Rapid prototyping: Porous titanium alloy scaffolds produced by selective laser melting for bone tissue engineering. Tissue Eng. Part C Methods 2009, 15, 115–124. [Google Scholar] [CrossRef]
- Kruth, J.-P.; Vandenbroucke, B.; Van Vaerenbergh, J.; Naert, I. Digital manufacturing of biocompatible metal frameworks for complex dental prostheses by means of SLS/SLM. In International Conference on Advanced Research and Rapid Prototyping (VRAP) 2005; da Silva Bartolo, P.J., Ed.; Taylor & Francis: Leiden, The Netherlands; Balkema Publishers: Leiria, Portugal, 2005; pp. 139–145. [Google Scholar]
- Traini, T.; Mangano, C.; Sammons, R.L.; Mangano, F.; Macchi, A.; Piatelli, A. Direct laser metal sintering as a new approach to fabrication of an isoelastic functionally graded material for manufacture of porous titanium dental implants. Dent. Mater. 2004, 24, 1525–1533. [Google Scholar] [CrossRef]
- Revilla-Leon, M.; Ozcan, M. Additive manufacturing technologies used for 3D metal printing in dentistry. Curr. Oral Health Rep. 2017, 4, 201–208. [Google Scholar] [CrossRef]
- Moraru, E.; Dontu, O.; Petre, A.; Vairenau, D.; Constantinescu, F.; Besnea, D. Some technological particularities on the execution of dental prostheses realized by selective laser deposition. J. Optoelect. Adv. Mater. 2018, 20, 208–213. [Google Scholar]
- Mangano, F.; Chambrone, L.; van Noort, R.; Miller, C.; Hatton, P.; Mangano, C. Direct metal laser sintering titanium dental implants: A review of the current literature. Int. J. Biomater. 2014, 2014, 461534. [Google Scholar] [CrossRef]
- Barazanchi, A.; Li, K.C.; Al-Amleh, B.; Lyons, K.; Waddell, N. Additive technology: Update on current materials and applications in dentistry. J. Prosthodont. 2017, 26, 153–163. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzański, L.B.; Achtelik-Franczak, A.; Dobrzańska, J. Application solid laser-sintered or machined Ti6Al4V alloy in manufacturing of dental implants and dental prosthetic restorations according to dentistry 4.0 concept. Processes 2020, 8, 664. [Google Scholar] [CrossRef]
- Dobrzański, L.B.; Achtelik-Franczak, A.; Dobrzańska, J.; Dobrzański, L.A. Comparison of the structure and properties of the solid Co-Cr-W-Mo-Si alloys used for dental restorations CNC machined or selective laser-sintered. Mater. Perform. Charact. 2020, 9, 556–578. [Google Scholar] [CrossRef]
- Puskar, T.; Jevremovic, D.; Williams, R.J.; Eggbeer, D.; Vukelic, D.; Budak, I. A comparative analysis of the corrosive effect of artificial saliva of variable pH on DMLS and Cast Co-Cr-Mo dental alloy. Materials 2014, 7, 6486–6501. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.-B.; Kim, W.-C.; Kim, H.-Y.; Kim, J.-H. An evaluation of marginal fit of three-unit fixed dental prostheses fabricated by direct metal laser sintering system. Dent. Mater. 2013, 29, e91–e96. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.-H.; Park, J.-M.; Kim, M.; Heo, S.-J.; Myung, J.-Y. Comparison of digital intraoral scanner reproducibility and image trueness considering repetitive experience. J. Prosthet. Dent. 2018, 119, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Su, T.S.; Sun, J. Comparison of repeatability between intraoral digital scanner and extraoral digital scanner: An in-vitro study. J. Prosthodont. Res. 2015, 59, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Persson, A.; Andersson, M.; Odén, A.; Englund, G.S. A three-dimensional evaluation of a laser scanner and a touch-probe scanner. J. Prosthet. Dent. 2006, 95, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Mandelli, F.; Gherlone, E.; Gastaldi, G.; Ferrari, M. Evaluation of the accuracy of extraoral laboratory scanners with a single-tooth abutment model: A 3d analysis. J. Prosthodont. Res. 2017, 61, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Renne, W.; Ludlow, M.; Fryml, J.; Schurch, Z.; Mennito, A.; Kessler, R.; Lauer, A. Evaluation of the accuracy of 7 digital scanners: An in vitro analysis based on 3-dimensional comparisons. J. Prosthet. Dent. 2017, 118, 36–42. [Google Scholar] [CrossRef]
- Ender, A.; Attin, R.; Mehl, A. In vivo precision of conventional and digital methods of obtaining complete-arch dental impressions. J. Prosthet. Dent. 2016, 115, 313–320. [Google Scholar] [CrossRef]
- Fasbinder, D.J. Digital dentistry: Innovation for restorative treatment. Compend. Contin. Educ. Dent. 2010, 31, 2–12. [Google Scholar]
- Lenguas Silva, A.L.; Ortega Aranegui, R.; Samara Shukeirm, G.; Lopez Bermejo, M.A. Tomografía computerizada de haz conico. Aplicaciones clínicas en odontología; comparacion con otras técnicas. Cient. Dent. 2010, 7, 147–159. [Google Scholar]
- Garg, V.; Bagaria, A.; Bhat, S.S.; Bhardwaj, S.; Hedau, L.R. Application of cone beam computed tomography in dentistry—A review. J. Adv. Med. Dent. Sci. Res. 2019, 7, 73–76. [Google Scholar]
- Bornstein, M.M.; Scarfe, W.C.; Vaughn, V.M.; Jacobs, R. Cone beam computed tomography in implant dentistry: A systematic review focusing on guidelines, indications, and radiation dose risks. J. Oral Maxillofoc. Implant. 2014, 29, 55–77. [Google Scholar] [CrossRef] [PubMed]
- Ho, M.H.; Lee, S.Y.; Chen, H.H.; Lee, M.C. Three-dimensional finite element analysis of the effect of post on stress distribution in dentin. J. Prosth. Dent. 1994, 72, 367–372. [Google Scholar] [CrossRef]
- Reimann, Ł.; Żmudzki, J.; Dobrzański, L.A. Strength analysis of a three-unit dental bridge framework with the finite element method. Acta Bioeng. Biomech. 2015, 17, 51–59. [Google Scholar] [CrossRef]
- Tanaka, M.; Naito, T.; Yokota, M.; Kohno, M. Finite element analysis of the possible mechanism of cervical lesion formation by occlusal force. J. Oral Rehab. 2003, 30, 60–67. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzańska-Danikiewicz, A.D.; Malara, P.; Achtelik-Franczak, A.; Dobrzański, L.B.; Gaweł, T.G. Implanto-Skafold Lub Proteza Elementów Anatomicznych Układu Stomatognatycznego Oraz Twarzoczaszki. Patent nr PL229148, 9 January 2018. [Google Scholar]
- Dobrzański, L.A.; Dobrzańska-Danikiewicz, A.D.; Malara, P.; Achtelik-Franczak, A.; Dobrzański, L.B.; Gaweł, T.G. Implanto-Skafold Kostny. Patent nr PL229149, 9 January 2018. [Google Scholar]
- Dobrzański, L.B.; Dobrzański, L.A.; Dobrzańska, J.; Achtelik-Franczak, A. Wysokorozwinięty Powierzchniowo Implant Stomatologiczny. Zgłoszenie patentowe P.434312, 15 June 2020. [Google Scholar]
- Dobrzański, L.B.; Dobrzański, L.A.; Dobrzańska, J.; Achtelik-Franczak, A. Wysokorozwinięty Powierzchniowo Implant Kostny W Tym Twarzoczaszki. Zgłoszenie patentowe P.434314, 15 June 2020. [Google Scholar]
- Dobrzański, L.A.; Dobrzańska-Danikiewicz, A.D. Foresight of the surface technology in manufacturing. In Handbook of Manufacturing Engineering and Technology; Nee, A.Y.C., Ed.; Springer-Verlag: London, UK, 2015; pp. 2587–2637. [Google Scholar]
- Dobrzański, L.A.; Dobrzańska-Danikiewicz, A.D.; Szindler, M.; Achtelik-Franczak, A.; Pakieła, W. Atomic layer deposition of TiO2 onto porous biomaterials. AMSE 2015, 75, 5–11. [Google Scholar]
- Dobrzański, L.A.; Dobrzańska-Danikiewicz, A.D. Inżynieria Powierzchni Materiałów: Kompendium Wiedzy I Podręcznik Akademicki; International OCSCO World Press: Gliwice, Poland, 2018. [Google Scholar]
- Vujicic, M. Our dental care system is stuck. J. Am. Dent. Assoc. 2018, 149, 167–169. [Google Scholar] [CrossRef]
- Kassebaum, N.J.; Smith, A.G.C.; Bernabé, E.; Fleming, T.D.; Reynolds, A.E.; Vos, T.; Murray, C.J.L.; Marcenes, W. Global, regional, and national prevalence, incidence, and disability-adjusted life years for oral conditions for 195 countries, 1990–2015: A systematic analysis for the global burden of diseases, injuries, and risk factors. J. Prosth. Res. 2017, 96, 380–387. [Google Scholar] [CrossRef]
- Cohen, L.; Dahlen, G.; Escobar, A.; Fejerskov, O.; Johnson, N.; Manji, F. Dentistry in crisis: Time to change, la cascada declaration. Aust. Dent. J. 2017, 62, 258–260. [Google Scholar] [CrossRef]
- OECD. Health at a Glance 2019: OECD Indicators; OECD Publishing: Paris, France, 2019. [Google Scholar] [CrossRef]
- Banerjee, A.; Doméjean, S. The contemporary approach to tooth preservation: Minimum intervention (MI) caries management in general practice. Prim. Dent. J. 2013, 2, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Brantley, C.F.; Bader, J.D.; Shugars, D.A.; Nesbit, S.P. Does the cycle of rerestoration lead to larger restorations? J. Am. Dent. Assoc. 1995, 126, 1407–1413. [Google Scholar] [CrossRef] [PubMed]
- Fejerskov, O.; Escobar, G.; Jøssing, M.; Baelum, V. A functional natural dentition for all—and for life? The oral healthcare system needs revision. J. Oral Rehab. 2013, 40, 707–722. [Google Scholar] [CrossRef] [PubMed]
- Elderton, R.J. Clinical studies concerning re-restoration of teeth. Adv. Dent. Res. 1990, 4, 4–9. [Google Scholar] [CrossRef]
- Ten Cate, J.M. Review on fluoride, with special emphasis on calcium fluoride mechanisms in caries prevention. Eur. J. Oral Sci. 1997, 105, 461–465. [Google Scholar] [CrossRef] [PubMed]
- Twetman, S.; Axelsson, S.; Dahlgren, H.; Holm, A.-K.; Källestål, C.; Lagerlöf, F.; Lingström, P.; Mejàre, I.; Nordenram, G.; Norlund, A.; et al. Caries-preventive effect of fluoride toothpaste: A systematic review. Acta Odontol. Scand. 2003, 61, 347–355. [Google Scholar] [CrossRef]
- Ismail, A.I.; Hasson, H. Fluoride supplements, dental caries and fluorosis; A systematic review. J. Am. Dent. Assoc. 2008, 139, 1457–1468. [Google Scholar] [CrossRef]
- WHO. Guideline: Sugars Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Lawrence, H.P.; Sheiham, A. Caries progression in 12- to 16-year-old schoolchildren in fluoridated and fluoride-deficient areas in Brazil. Community Dent. Oral Epidemiol. 1997, 25, 402–411. [Google Scholar] [CrossRef]
- Slade, G.D.; Sanders, A.E.; Do, L.; Roberts-Thomson, K.; Spencer, A.J. Effects of fluoridated drinking water on dental caries in Australian adults. J. Dent. Res. 2013, 92, 376–382. [Google Scholar] [CrossRef]
- Kunzel, W.; Fischer, T. Rise and fall of caries prevalence in German towns with different F concentrations in drinking water. Caries Res. 1997, 31, 166–173. [Google Scholar] [CrossRef]
- Marthaler, T.M. Changes in the prevalence of dental caries: How much can be attributed to changes in diet? Caries Res. 1990, 24 (Suppl. 1), 3–15. [Google Scholar] [CrossRef]
- Leite, T.A.; de Paula, M.S.; Ribeiro, R.A.; Leite, I.C.G. Dental caries and sugar consumption in a group of public nursery school children. Rev. Odontol. Univ. São Paulo 1999, 13, 13–18. (In Portuguese) [Google Scholar] [CrossRef]
- Sivaneswaran, S.; Barnard, P.D. Changes in the pattern of sugar (sucrose) consumption in Australia 1958–1988. Comm. Dent. Health 1993, 10, 353–363. [Google Scholar]
- Holt, R.D. Foods and drinks at four daily time intervals in a group of young children. Br. Dent. J. 1991, 170, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Burt, B.A.; Eklund, S.A.; Morgan, K.J.; Larkin, F.E.; Guire, K.E.; Brown, L.O.; Weintraub, J.A. The effects of sugars intake and frequency of ingestion on dental caries increment in a three-year longitudinal study. J. Dent. Res. 1988, 67, 1422–1429. [Google Scholar] [CrossRef]
- Rodrigues, C.S.; Sheiham, A. The relationships between dietary guidelines, sugar intake and caries in primary teeth in low income Brazilian 3-year-olds: A longitudinal study. Int. J. Paediatr. Dent. 2000, 10, 47–55. [Google Scholar] [CrossRef]
- Masson, L.F.; Blackburn, A.; Sheehy, C.; Craig, L.C.; Macdiarmid, J.I.; Holmes, B.A.; McNeill, G. Sugar intake and dental decay: Results from a national survey of children in Scotland. Br. J. Nutr. 2010, 104, 1555–1564. [Google Scholar] [CrossRef]
- Arnadottir, I.B.; Rozier, R.G.; Saemundsson, S.R.; Sigurjons, H.; Holbrook, W.P. Approximal caries and sugar consumption in Icelandic teenagers. Comm. Dent. Oral Epidemiol. 1998, 26, 115–121. [Google Scholar] [CrossRef]
- Ruottinen, S.; Karjalainen, S.; Pienihakkinen, K.; Lagstrom, H.; Niinikoski, H.; Salminen, M.; Ronnemaa, T.; Simell, O. Sucrose intake since infancy and dental health in 10-year-old children. Caries Res. 2004, 38, 142–148. [Google Scholar] [CrossRef]
- Rugg-Gunn, A.J.; Hackett, A.F.; Appleton, D.R.; Jenkins, G.N.; Eastoe, J.E. Relationship between dietary habits and caries increment assessed over two years in 405 English adolescent school children. Arch. Oral Biol. 1984, 29, 983–992. [Google Scholar] [CrossRef]
- Van Loveren, C. Sugar restriction for caries prevention: Amount and frequency. Which is more important? Caries Res. 2019, 53, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Te Morenga, L.; Mallard, S.; Mann, J. Dietary sugars and body weight: Systematic review and meta-analyses of randomised controlled trials and cohort studies. BMJ 2012, 346, e7492. [Google Scholar] [CrossRef] [PubMed]
- Newens, K.J.; Walton, J. A review of sugar consumption from nationally representative dietary surveys across the world. J. Hum. Nutr. Diet. 2016, 29, 225–240. [Google Scholar] [CrossRef] [PubMed]
- James, W.P.T. Taking action on sugar. Lancet Diabet. Endocrinol. 2016, 4, 92–94. [Google Scholar] [CrossRef]
- Sheiham, A.; James, W.P.T. A new understanding of the relationship between sugars, dental caries and fluoride use: Implications for limits on sugars consumption. Pub. Health Nutr. 2014, 17, 2176–2184. [Google Scholar] [CrossRef]
- Broadbent, J.M.; Thomson, W.M.; Poulton, R. Trajectory patterns of dental caries experience in the permanent dentition to the fourth decade of life. J. Dent. Res. 2008, 87, 69–72. [Google Scholar] [CrossRef]
- Broadbent, J.M.; Foster Page, L.A.; Thomson, W.M.; Poulton, R. Permanent dentition caries through the first half of life. Br. Dent. J. 2013, 215, E12. [Google Scholar] [CrossRef]
- Lobstein, T. Sugar: A shove to industry rather than a nudge to consumers? Lancet Diabet. Endocrinol. 2016, 4, 86–87. [Google Scholar] [CrossRef]
- McKee, M.; Stuckler, D. Realising an election manifesto for public health in the UK. Lancet 2015, 385, 665–666. [Google Scholar] [CrossRef]
- Moodie, R.; Stuckler, D.; Monteiro, C.; Sheron, N.; Neal, B.; Thamarangsi, T.; Lincoln, P.; Casswell, S. Profits and pandemics: Prevention of harmful effects of tobacco, alcohol, and ultra-processed food and drink industries. Lancet 2013, 381, 670–679. [Google Scholar] [CrossRef]
- Burt, B.A.; Pai, S. Is sugar consumption still a major determinant of dental caries? a systematic review. In NIH Consensus Development Conference on Diagnosis and Management of Dental Caries Throughout Life; Horowitz, A.M., Elliott, J.M., Eds.; National Institutes of Health: Bethesda, MD, USA, 2001; pp. 71–78. [Google Scholar]
- Grammatikaki, E.; Wollgast, J.; Caldeira, S. Feeding Infants and Young Children. A Compilation of National Food-Based Dietary Guidelines and Specific Products Available in the EU Market; Joint Research Centre: Ispra, Italy, 2019; Available online: https://ec.europa.eu/jrc/sites/jrcsh/files/processed_cereal_baby_food_online.pdf (accessed on 28 August 2020).
- Birch, S.; Listl, S. The Economics of Oral Health and Health Care; Max Planck Institute for Social Law and Social Policy Discussion Paper: Munich, Germany, 2015. [Google Scholar] [CrossRef]
- Ramos-Gomez, F.; van Loveren, C. Caries prevention through life course approach, evidence-based caries prevention. In Evidence-Based Caries Prevention; Eden, E., Ed.; Springer International Publishing: Cham, Switzerland, 2016; pp. 143–161. [Google Scholar] [CrossRef]
- Calzón Fernández, S.; Fernández Ajuria, A.; Martín, J.J.; Murphy, M.J. The impact of the economic crisis on unmet dental care needs in Spain. J. Epidemiol. Comm. Health 2015, 69, 880–885. [Google Scholar] [CrossRef] [PubMed]
- Spencer, A.J. What options do we have for organising, providing and funding better public dental care? Aust. Health Policy Inst. Comm. Pap. Ser. 2001, 02, 1–80. [Google Scholar]
- Baelum, V.; van Palestein Helderman, V.W.H.; Hugoson, A.; Yee, R.; Fejerskov, O. A global perspective on changes in the burden of caries and periodontitis: Implications for dentistry. J. Oral Rehab. 2007, 34, 872–906. [Google Scholar] [CrossRef] [PubMed]
- Holst, D.; Sheiham, A.; Petersen, P. Regulating entrepreneurial behaviour in oral care health services. In European Observatory on Health Care Systems Series: Regulating Entrepreneurial Behaviour in European Care Health Systems; Saltman, R., Busse, R., Mossialos, E., Eds.; Open University Press: Buckingham, Philadelphia, PA, USA, 2002; pp. 215–231. [Google Scholar]
- Bader, J.D.; Shugars, D.A. What do we know about how dentists make caries-related treatment decisions? Comm. Dent. Oral Epidemiol. 1997, 25, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, M.; Haapasalo, M.; Imazato, S.; Il Lee, J.; Momoi, Y.; Murakami, S.; Whelton, H.; Wilson, N. Dentistry in the 21st century: Challenges of a globalising world. Int. Dent. J. 2014, 64, 333–342. [Google Scholar] [CrossRef] [PubMed]
- WMA Declaration of Geneva; Adopted by the 2nd General Assembly of the World Medical Association, Geneva, Switzerland, September 1948 and amended by the 22nd World Medical Assembly, Sydney, Australia, August 1968 and the 35th World Medical Assembly, Venice, Italy, October 1983 and the 46th WMA General Assembly, Stockholm, Sweden, September 1994 and editorially revised by the 170th WMA Council Session, Divonne-les-Bains, France, May 2005 and the 173rd WMA Council Session, Divonne-les-Bains, France, May 2006 and amended by the 68th WMA General Assembly, Chicago, United States, October 2017. Available online: https://www.wma.net/policies-post/wma-declarationof-geneva/ (accessed on 30 September 2020).
- Yee, R.; Sheiham, A. The burden of restorative dental treatment for children in third world countries. Int. Dent. J. 2002, 52, 1–9. [Google Scholar] [CrossRef]
- Fejerskov, O.; Baelum, V. Changes in oral health profiles and demography necessitate a revision of the structure and organisation of the oral healthcare system. Gerodontol 2014, 31, 1–3. [Google Scholar] [CrossRef]
- Bernabé, E.; Masood, M.; Vujicic, M. The impact of out-of-pocket payments for dental care on household finances in low and middle income countries. BMC Public Health 2017, 17, 109. [Google Scholar] [CrossRef]
- FDI World Dental Federation. Available online: https://www.fdiworlddental.org/about-fdi (accessed on 2 September 2020).
- Practising Dentists. Available online: https://ec.europa.eu/eurostat/databrowser/view/tps00045/default/map?lang=en (accessed on 2 September 2020).
- Statista 2020. Available online: https://www.statista.com/statistics/186273/number-of-active-dentists-in-the-us-since-1993/ (accessed on 30 September 2020).
- Novel Coronavirus (COVID-19) Infection Map. Available online: https://hgis.uw.edu/virus/ (accessed on 25 November 2020).
- Van Doremalen, N.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.N.J.; Gerber, S.I.; Lloyd-Smith, J.O.; et al. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N. Eng. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef]
- Meng, L.; Hua, F.; Bian, Z. Coronavirus disease 2019 (COVID-19): Emerging and future challenges for dental and oral medicine. J. Dent. Res. 2020, 99, 481–487. [Google Scholar] [CrossRef]
- Raport Amnesty International MJM. Pracownicy Medyczni Na Całym Świecie Są Uciszani, Narażani I Atakowani. Available online: https://amnesty.org.pl/pracownicy-medyczni-na-calym-swiecie-sa-uciszani-narazani-i-atakowani/ (accessed on 14 July 2020).
- Fallahi, H.R.; Keyhan, S.O.; Zandian, D.; Kim, S.G.; Cheshmi, B. Being a front-line dentist during the Covid-19 pandemic: A literature review. Maxillofac. Plast. Reconstr. Surg. 2020, 42, 12. [Google Scholar] [CrossRef] [PubMed]
- Guidance for Dental Settings, Interim Infection Prevention and Control Guidance for Dental Settings During the Coronavirus Disease 2019 (COVID-19) Pandemic. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/dental-settings.html (accessed on 28 August 2020).
- Management of Acute Dental Problems During COVID-19 Pandemic. Available online: https://www.sdcep.org.uk/published-guidance/acute-dental-problems-covid-19/ (accessed on 28 August 2020).
- Dental care and coronavirus (COVID-19). Available online: https://www.dentalhealth.org/Pages/FAQs/Category/coronavirus (accessed on 28 August 2020).
- Guidance on COVID-19, Guidance on Managing Infection Related Risks in Dental Services, V1.1 15.05.2020. Available online: https://www.fdiworlddental.org/sites/default/files/media/documents/guidance_on_managing_infection_related_risks_in_dental_services_0.pdf (accessed on 28 August 2020).
- COVID-19 and Dental Practice; What Has Been Done in China? Available online: https://www.fdiworlddental.org/sites/default/files/media/documents/covid-19_and_dental_practice_what_has_been_done_in_china.pdf (accessed on 28 August 2020).
- Khader, Y.; Al Nsour, M.; Al-Batayneh, O.B.; Saadeh, R.; Bashier, H.; Alfaqih, M.; Al-Azzam, S.; AlShurman, B.A. Dentists’ awareness, perception, and attitude regarding covid-19 and infection control: Cross-sectional study among jordanian dentists. JMIR Public Health Surveill. 2020, 6, e18798. [Google Scholar] [CrossRef] [PubMed]
- Dobrzański, L.B.; Dobrzański, L.A.; Dobrzańska, J.; Rudziarczyk, K.; Achtelik-Franczak, A. Akcesorium Do Ochrony Osobistej Personelu Dentystycznego Przed Koronawirusem SARS-CoV-2 I Innymi Drobnoustrojami Chorobotwórczymi. Zgłoszenie patentowe P.434391, 19 June 2020. [Google Scholar]
- Dobrzański, L.B.; Dobrzański, L.A.; Dobrzańska, J. Clean DENT work space—A medical aerosol absorption system generated during medical procedures in the patient’s mouth during dental, ENT and general medical procedures in order to effectively protect personnel and patients against viruses (including SARS-cov-2) and other microorganisms. Wniosek o dofinansowanie Projektu nr POIR.01.01.01-00-0637/20, 4 June 2020. [Google Scholar]
- Dobrzański, L.B.; Dobrzański, L.A.; Dobrzańska, J.; Rudziarczyk, K.; Achtelik-Franczak, A. Accessory for personal protection of dental staff against SARS-CoV-2 coronavirus and other pathogenic microorganisms. ICAN—International Invention Innovation Competition in Canada: Overall Selection of the Top 20 Best Inventions in iCAN 2020. Available online: https://www.tisias.org/uploads/6/9/5/1/69513309/the_finals_award_winners_-_list.pdf (accessed on 2 September 2020).
- Dobrzański, L.B.; Dobrzański, L.A.; Dobrzańska, J.; Rudziarczyk, K.; Achtelik-Franczak, A. Accessory for Personal Protection of Dental Staff Against SARS-CoV-2 Coronavirus And Other Pathogenic Microorganisms. Sahasak Nimavum 2020 International Competition for Invention and Innovation: Gold Medal. Available online: http://slicexpo.com/sn-2020-results/ (accessed on 2 September 2020).
- Steinke, H. Der Hippokratische eid: Ein schwieriges erbe. Horizonte medizingeschichte, schweizerische ärztezeitung. Bull. Médecins Suisses—Boll. Med. Svizz. 2016, 97, 1699–1701. [Google Scholar]
- Murgic, L.; Hébert, P.C.; Sovic, S.; Pavlekovic, G. Paternalism and autonomy: Views of patients and providers in a transitional (post-communist) country. BMC Med. Ethics 2015, 29, 65. [Google Scholar] [CrossRef] [PubMed]
- Will, J.F. A brief historical and theoretical perspective on patient autonomy and medical decision making: Part II: The autonomy model. Chest 2011, 139, 1491–1497. [Google Scholar] [CrossRef]
- Baumann, A.; Audibert, G.; Guibet Lafaye, C.; Puybasset, L.; Mertes, P.M.; Claudot, F. Elective non-therapeutic intensive care and the four principles of medical ethics. J. Med. Ethics 2013, 39, 139–142, Erratum in 2013, 39, 409. [Google Scholar] [CrossRef] [PubMed]
- Jotterand, F. The hippocratic oath and contemporary medicine: Dialectic between past ideals and present reality? J. Med. Philos. 2005, 30, 107–128. [Google Scholar] [CrossRef] [PubMed]
- Gillon, R. Medical ethics: Four principles plus attention to scope. BMJ 1994, 309, 184. [Google Scholar] [CrossRef] [PubMed]
- Beauchamp, T.L.; Childress, J.F. Principles of Biomedical Ethics, 8th ed.; Oxford University Press: New York, NY, USA, 2019. [Google Scholar]
- Holm, S. Not just autonomy—The principles of American biomedical ethics. J. Med. Ethics 1995, 21, 6. [Google Scholar] [CrossRef]
- Beauchamp, T.L.; Childress, J.F. Principles of Biomedical Ethics, 1st ed.; Oxford University Press: New York, NY, USA, 1979. [Google Scholar]
- Veatch, R.M. The impossibility of a morality internal to medicine. J. Med. Philos. A Forum Bioeth. Philos. Med. 2001, 26, 621–642. [Google Scholar] [CrossRef]
- Nash, D.A. Ethics in dentistry: Review and critique of principles of ethics and code of professional conduct. J. Am. Dent. Assoc. 1984, 109, 597–603. [Google Scholar] [CrossRef] [PubMed]
- Seear, J.E.; Walters, L. Law and Ethics in Dentistry Paperback, 3rd ed.; Butterworth-Heinemann Ltd.: Oxford, UK, 1991. [Google Scholar]
- Jessri, M.; Fatemitabar, S.A. Implication of ethical principles in chair-side dentistry. Iran. J. Allergy Asthma Immunol. 2007, 6 (Suppl. 5), 53–59. [Google Scholar]
- Nash, D.A. On ethics in the profession of dentistry and dental education. Eur. J. Dent. Educ. 2007, 11, 64–74. [Google Scholar] [CrossRef] [PubMed]
- Dobrzański, L.A.; Dobrzański, L.B.; Dobrzańska-Danikiewicz, A.D.; Dobrzańska, J.; Kraszewska, M. The synergistic ethics interaction with nanoengineering, dentistry and dental engineering. In Ethics in Nanotechnology; Jeswani, G., Van De Voorde, M., Eds.; De Gruyter: Berlin, Germany, 2020; (prepared for printing). [Google Scholar]
- Dobrzański, L.A.; Dobrzański, L.B.; Dobrzańska-Danikiewicz, A.D.; Dobrzańska, J.; Kraszewska, M. Development prospects of the dentistry 4.0, dental engineering and nanotechnology triad towards ethical imperatives. In Ethics in Nanotechnology; Jeswani, G., Van De Voorde, M., Eds.; De Gruyter: Berlin, Germany, 2020; (prepared for printing). [Google Scholar]
- Davis, M. Thinking Like an Engineer: Studies in the Ethics of a Profession; Oxford University Press: New York, NY, USA; Oxford, UK, 1998. [Google Scholar]
- Davis, M. Engineering Ethics; Routledge: London, UK, 2005. [Google Scholar] [CrossRef]
- Martin, M.W.; Schinzinger, R. Ethics in Engineering, 4th ed.; McGraw-Hill: Boston, MA, USA, 2005. [Google Scholar]
- Harris, C.E.; Pritchard, M.S.; Rabins, M.J. Engineering Ethics: Concepts and Cases, 4th ed.; Wadsworth: Belmont, CA, USA, 2008. [Google Scholar]
- Hansson, S.O. Ethical criteria of risk acceptance. Erkenntnis 2003, 59, 291–309. [Google Scholar] [CrossRef]
- Hahn, D.; Payne, W.; Lucas, E. Focus on Health, 11th ed.; McGrow Hill Humanities: New York, NY, USA, 2013; pp. 125–153. [Google Scholar]
- Barro, Ó.; Arias-González, F.; Lusquiños, F.; Comesaña, R.; del Val, J.; Riveiro, A.; Badaoui, A.; Gómez-Baño, F.; Pou, J. Effect of four manufacturing techniques (casting, laser directed energy deposition, milling and selective laser melting) on microstructural, mechanical and electrochemical properties of co-CR dental alloys, before and after PFM firing process. Metals 2020, 10, 1291. [Google Scholar] [CrossRef]
- Bartoszewski, W. Warto Być Przyzwoitym; Wydawnictwo W drodze: Poznań, Poland, 2019. (In Polish) [Google Scholar]








































{kind=link}
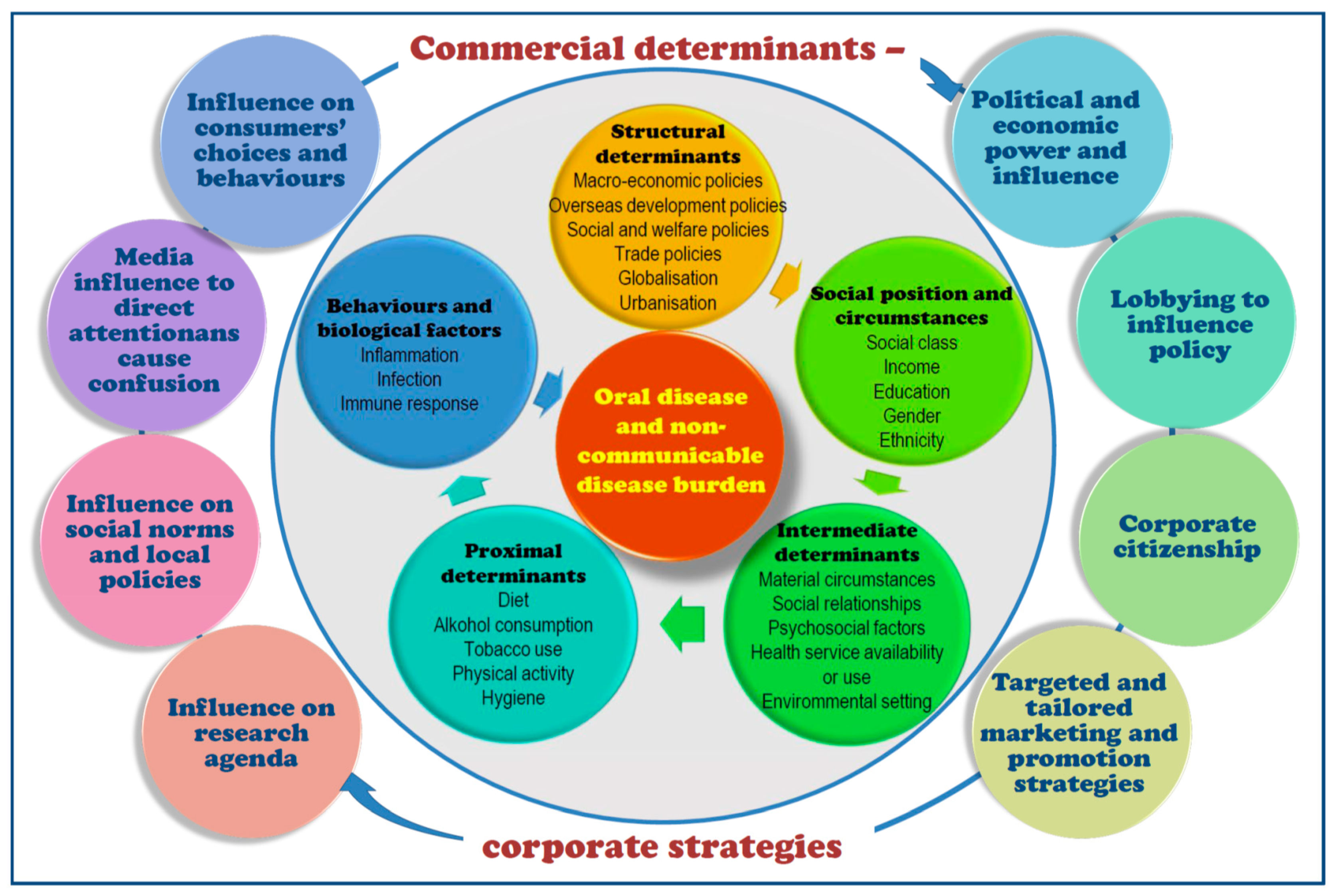{kind=link}
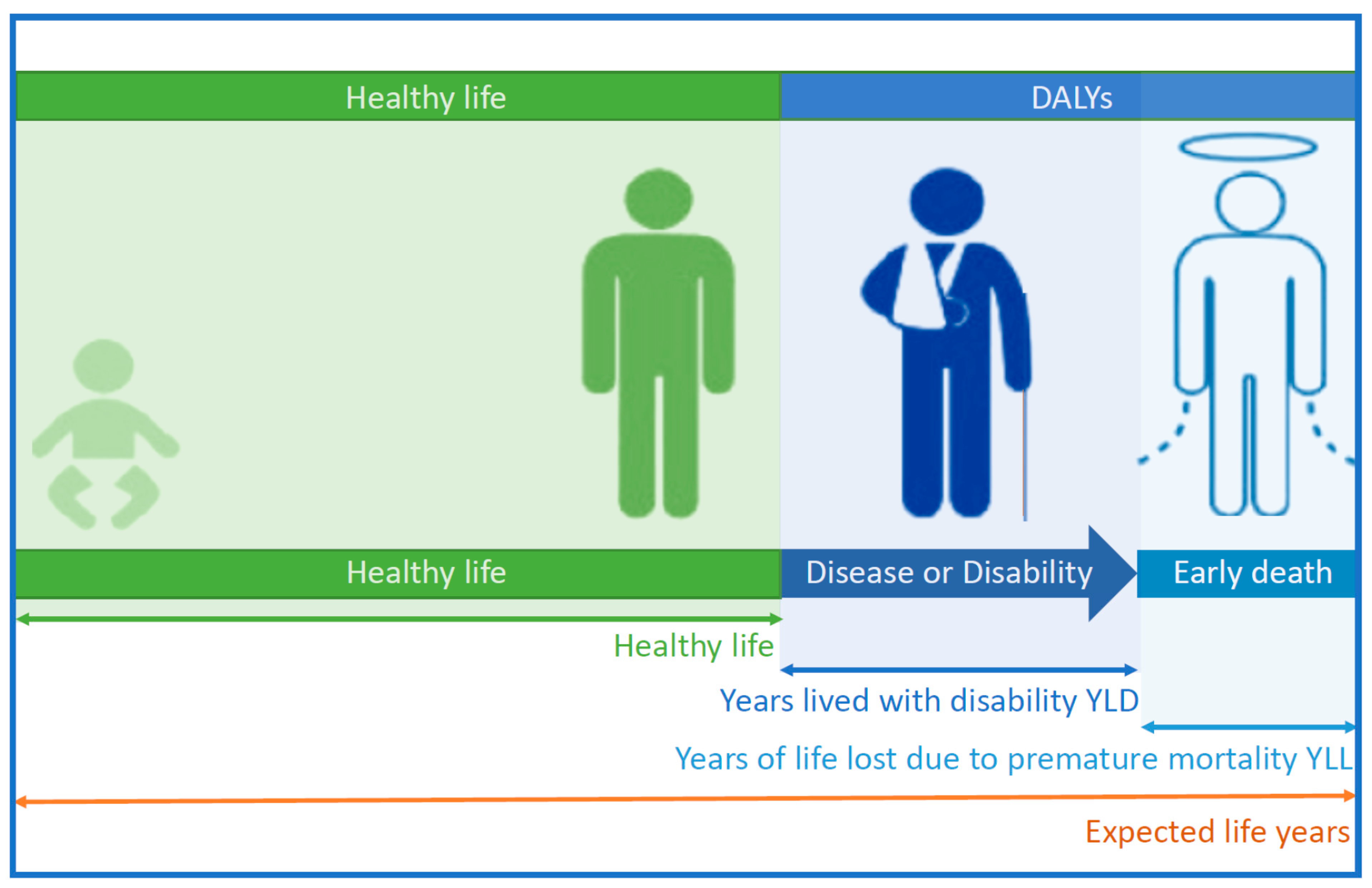{kind=link}
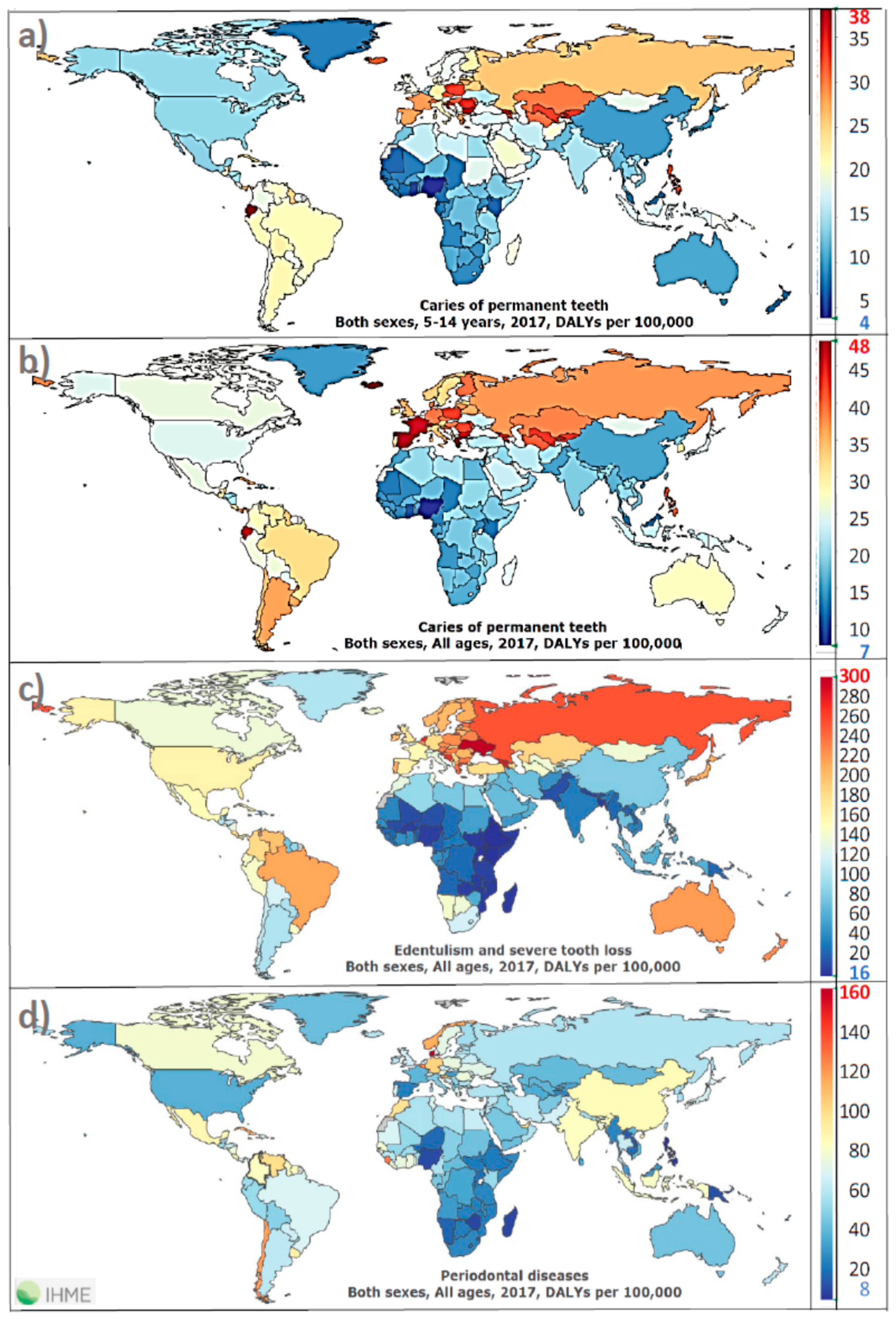{kind=link}
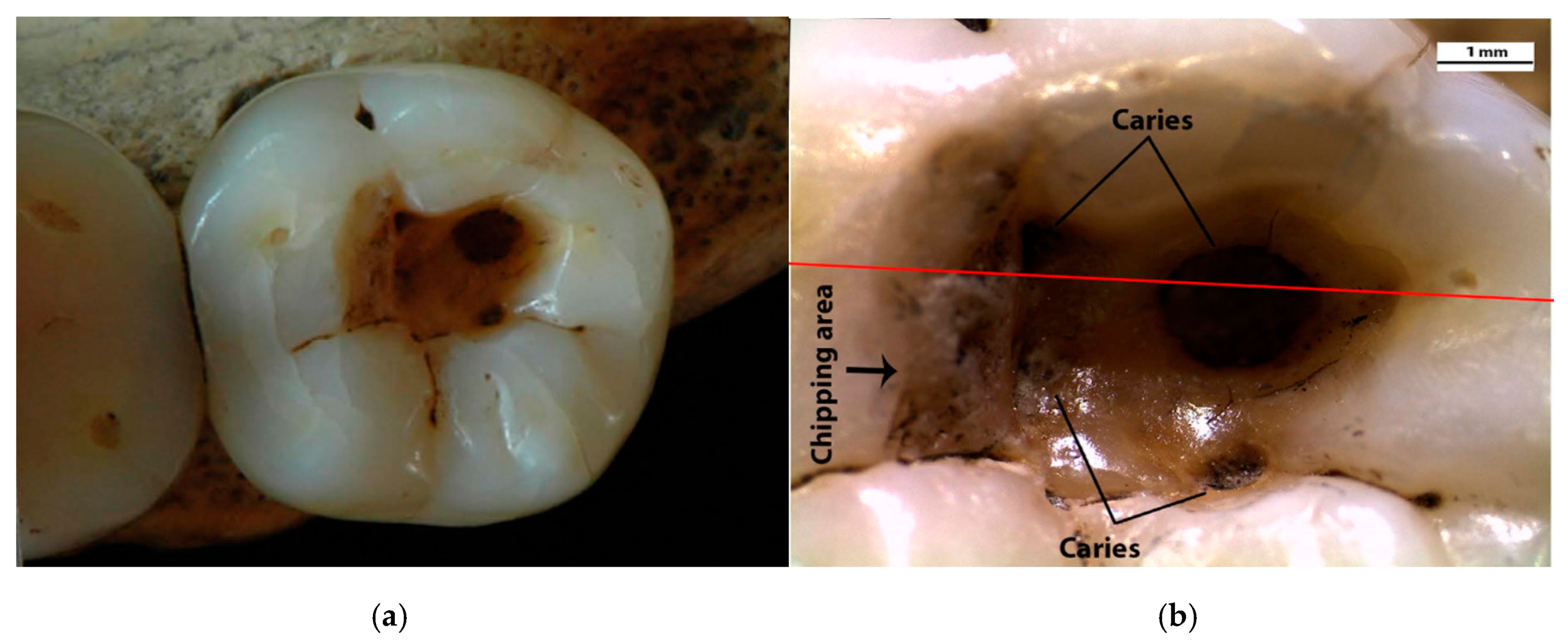{kind=link}
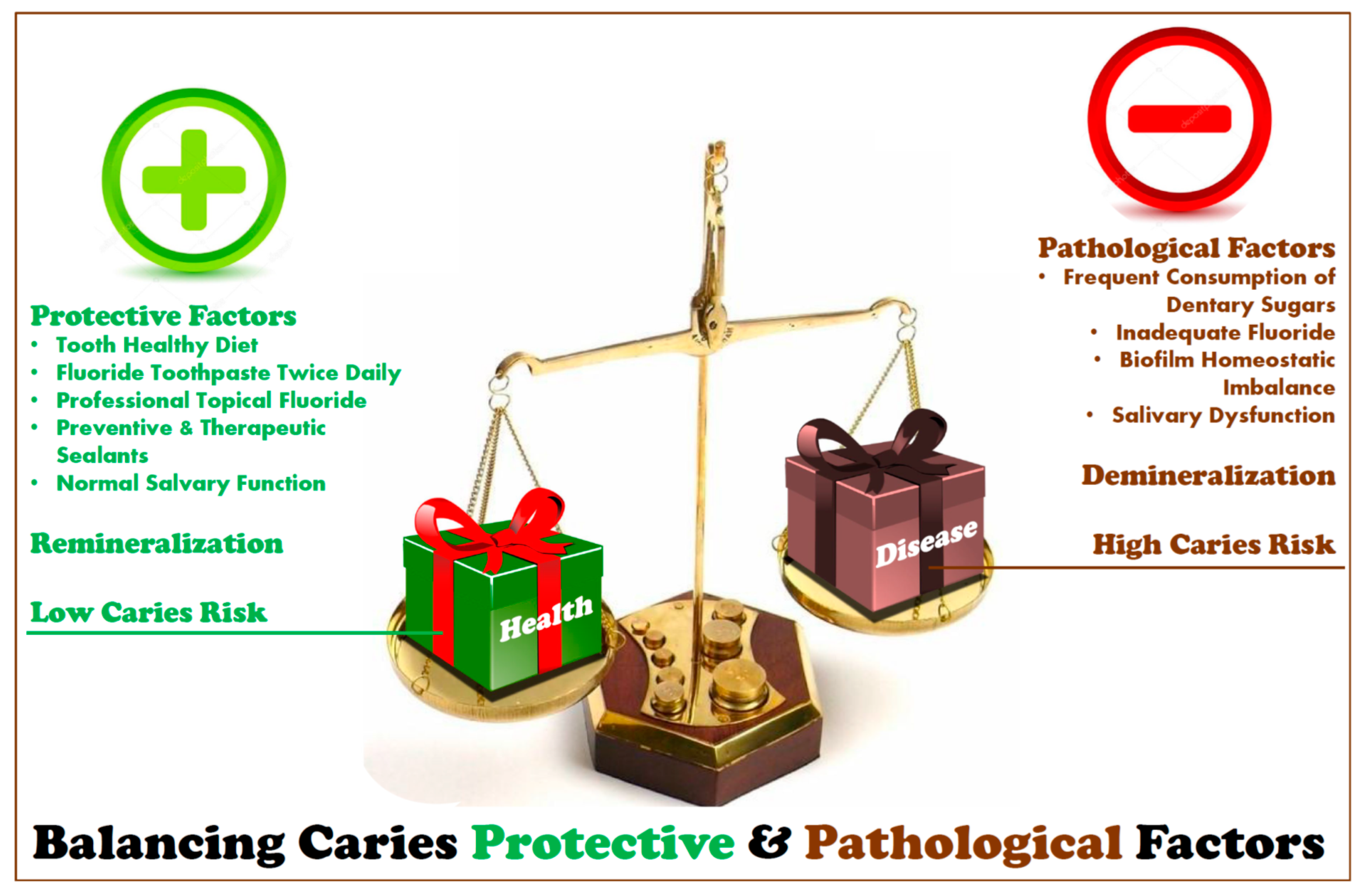{kind=link}
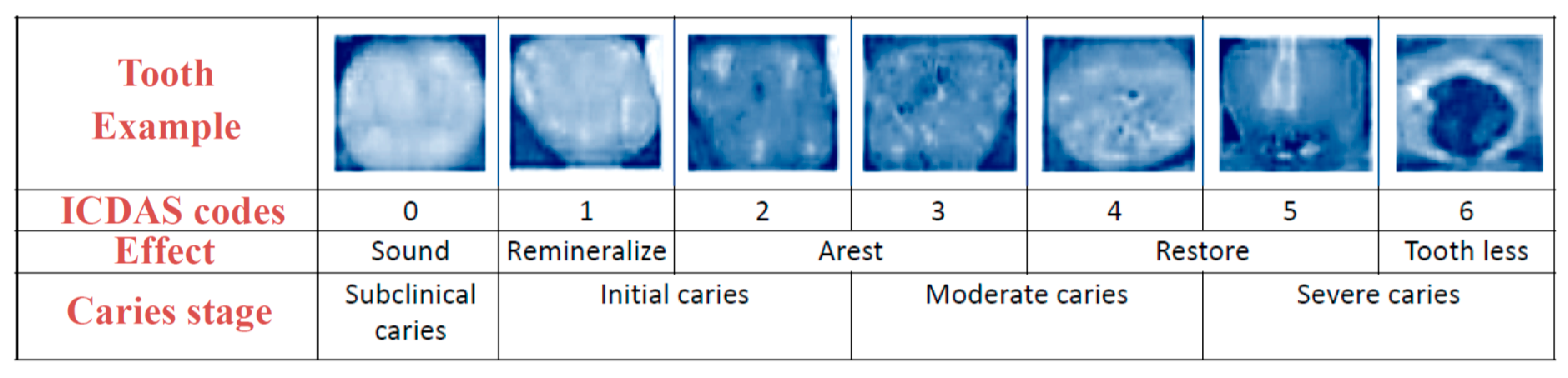{kind=link}
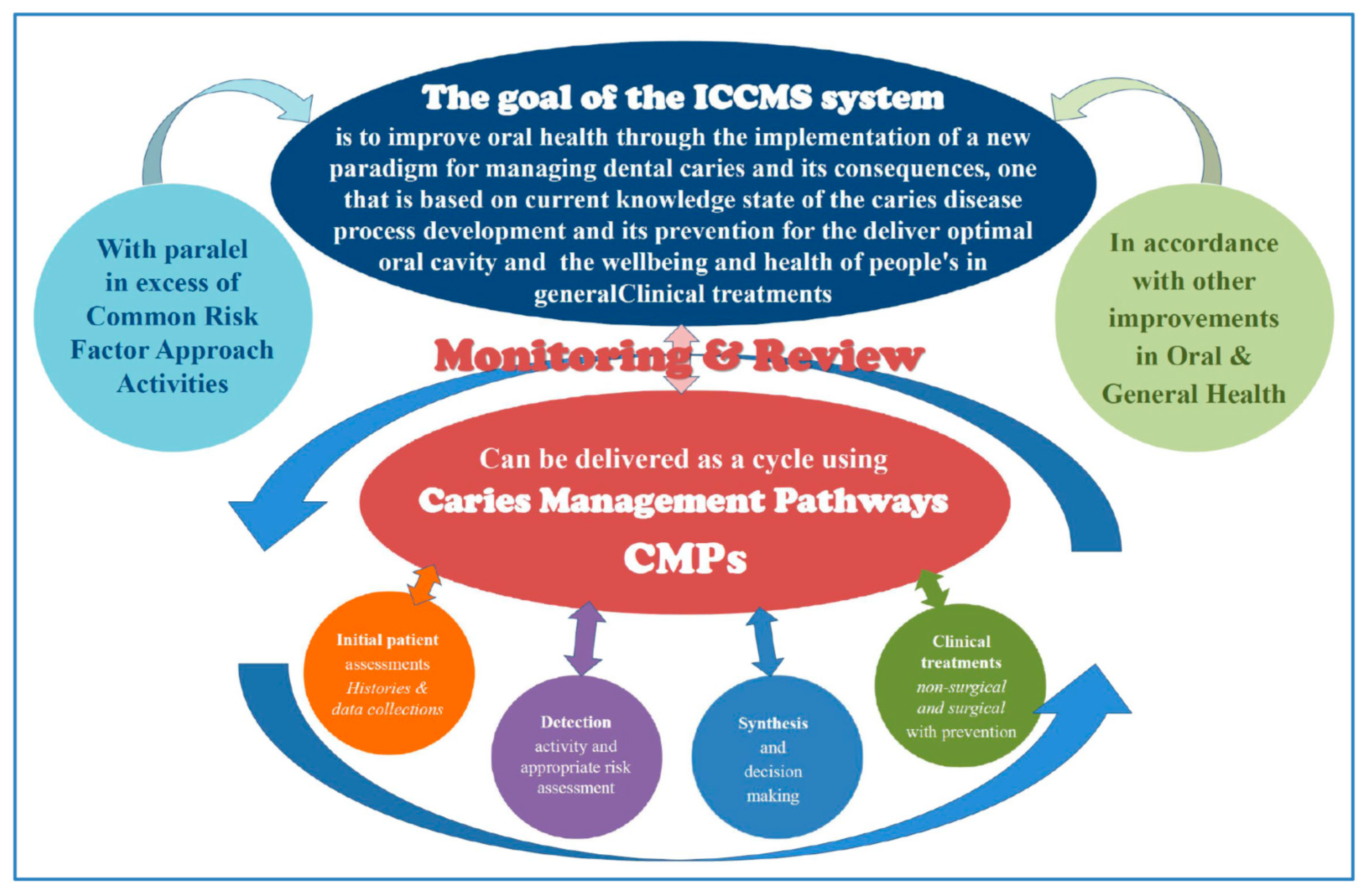{kind=link}
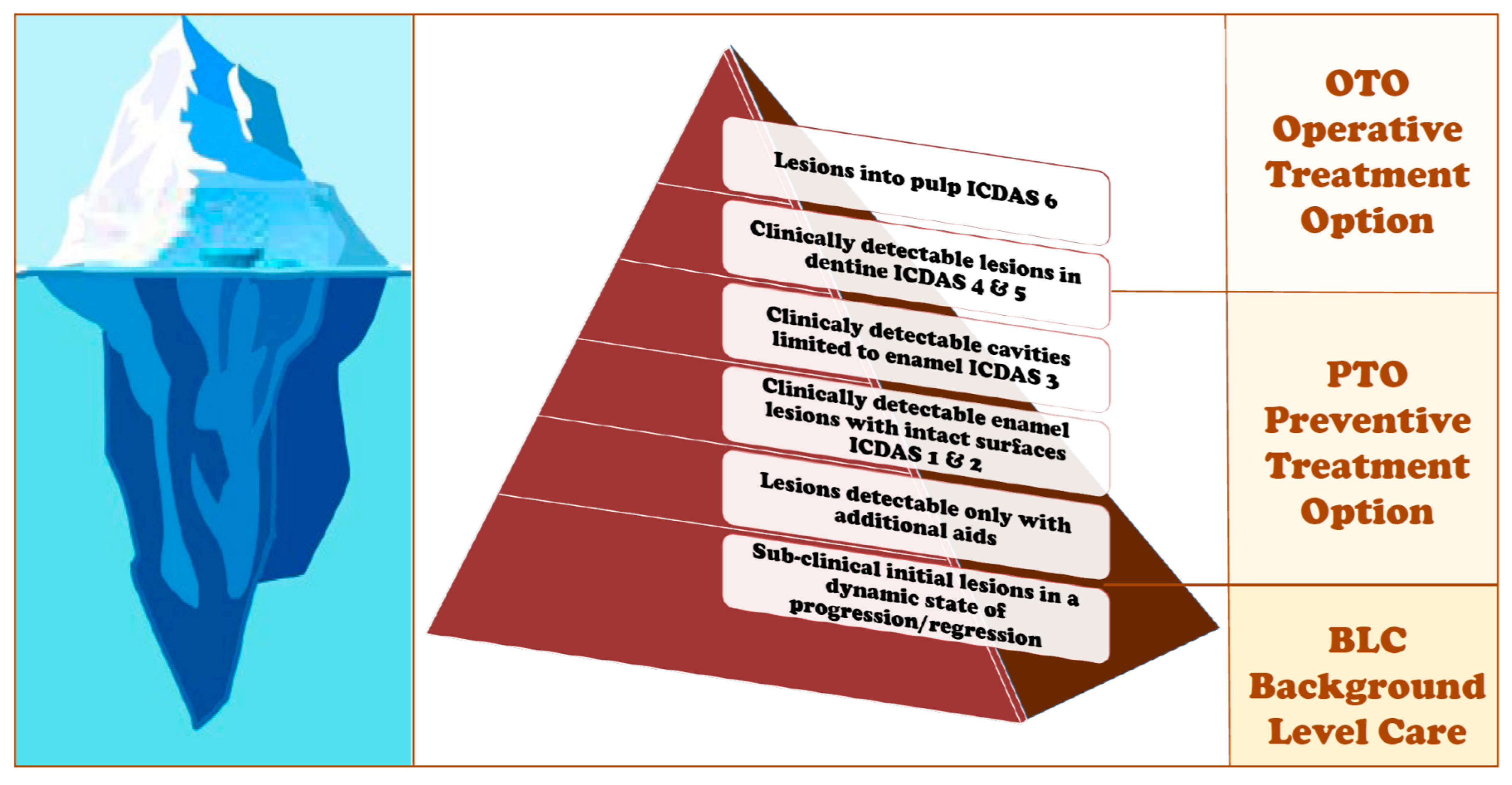{kind=link}
{kind=link}
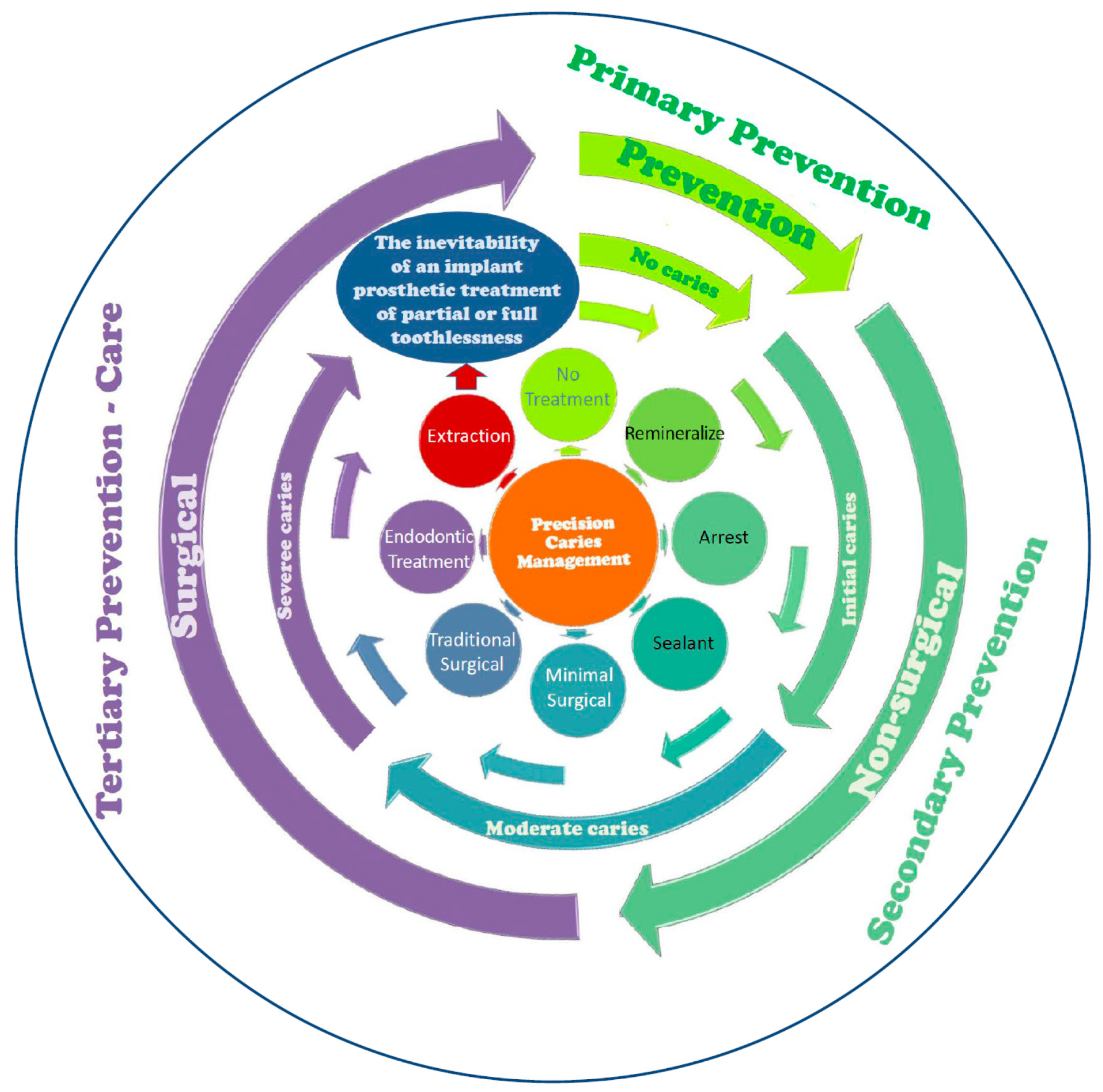{kind=link}
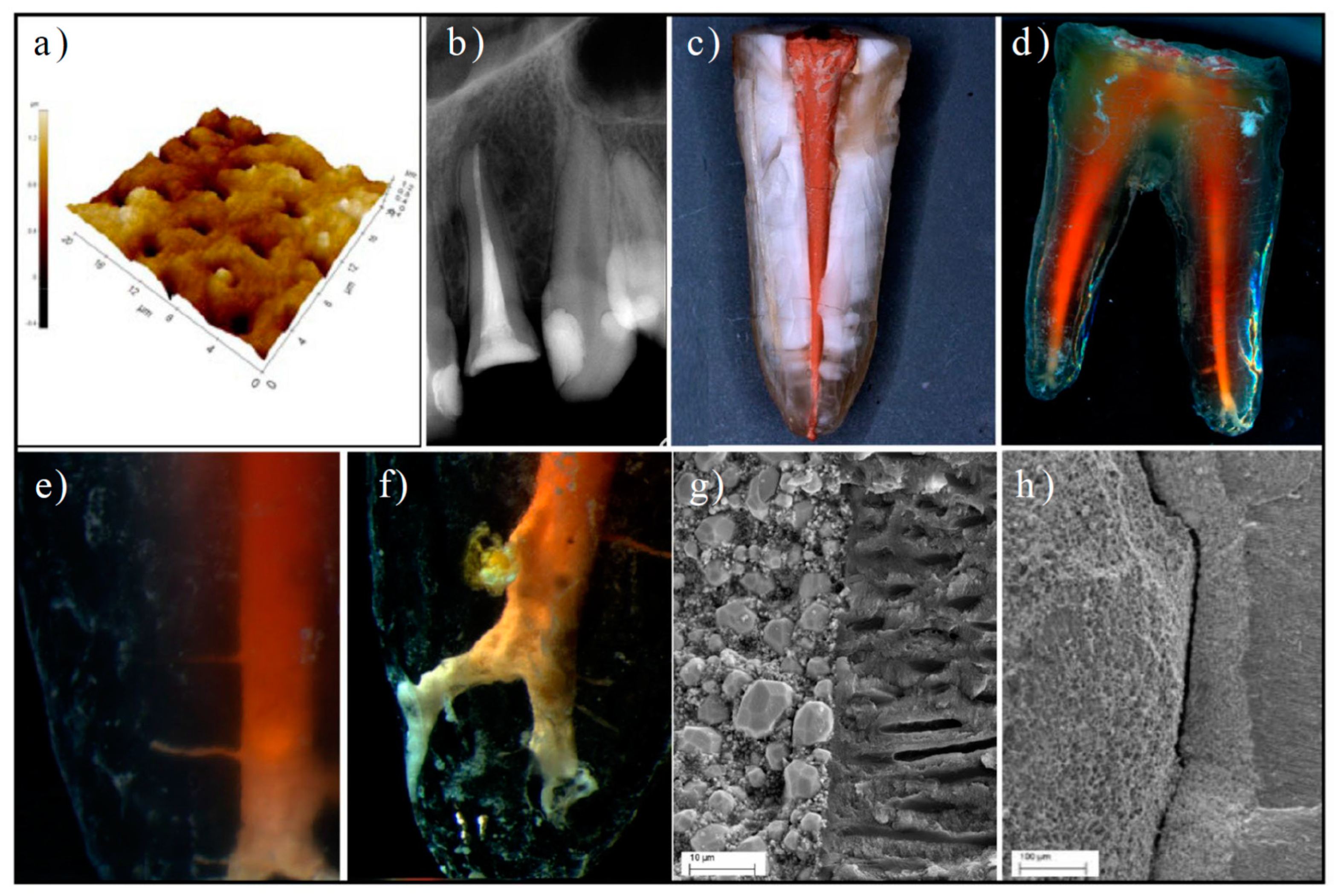{kind=link}
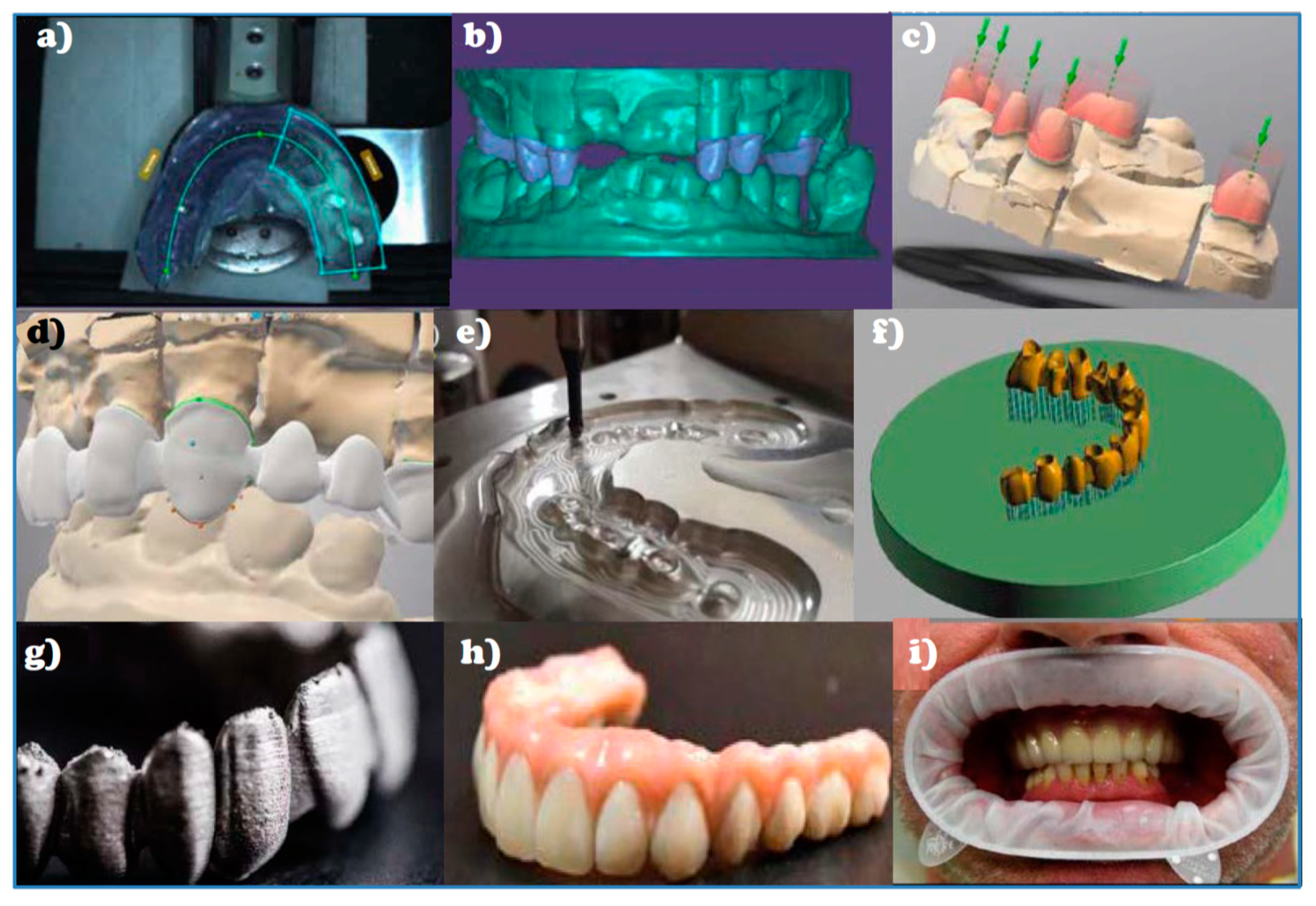{kind=link}
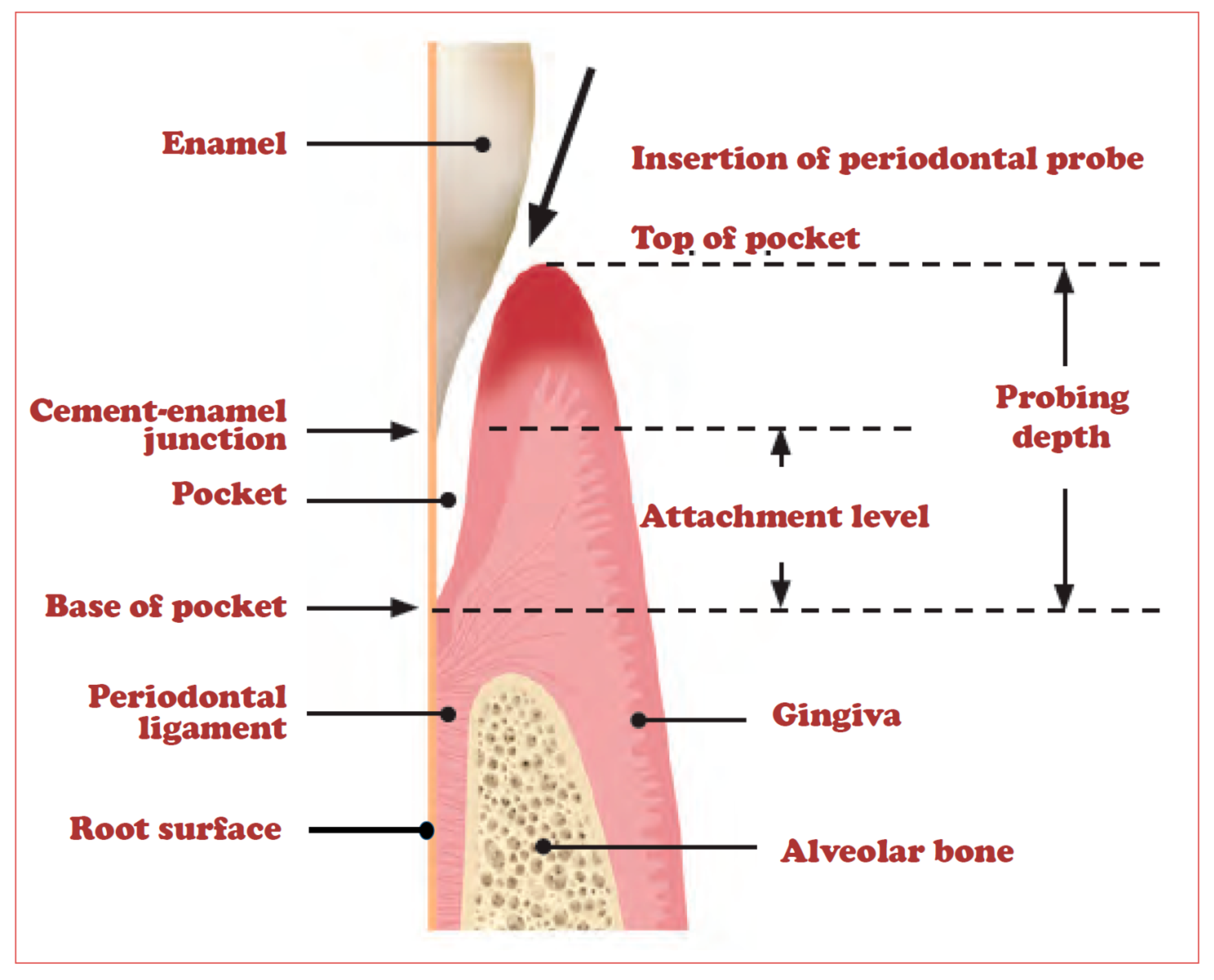{kind=link}
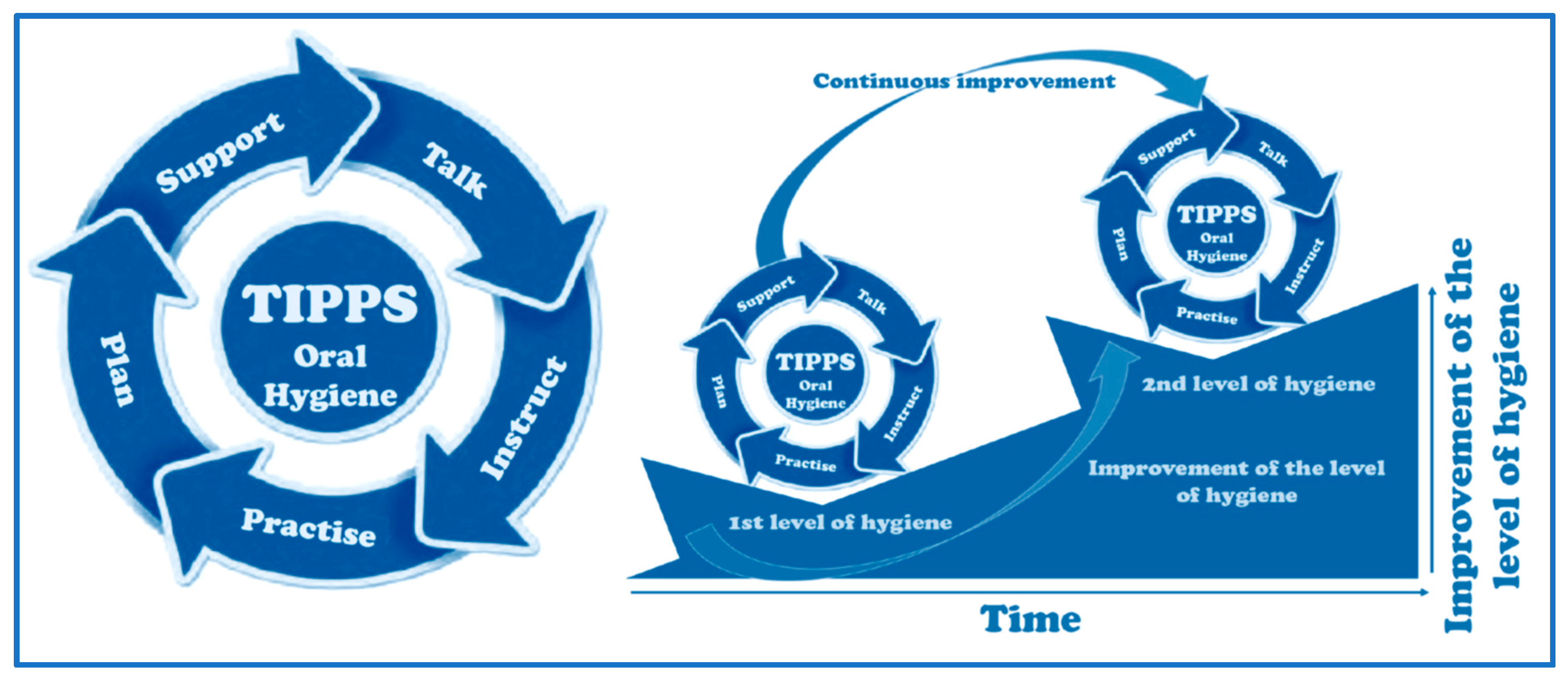{kind=link}
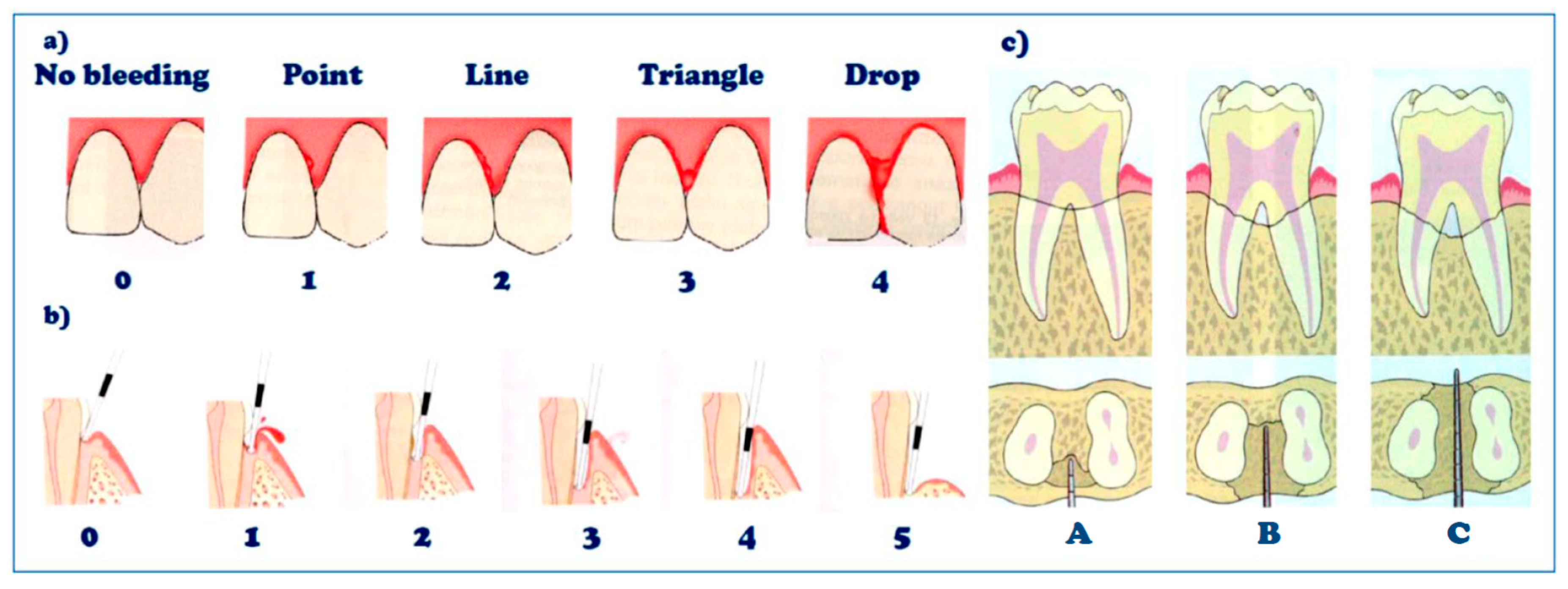{kind=link}
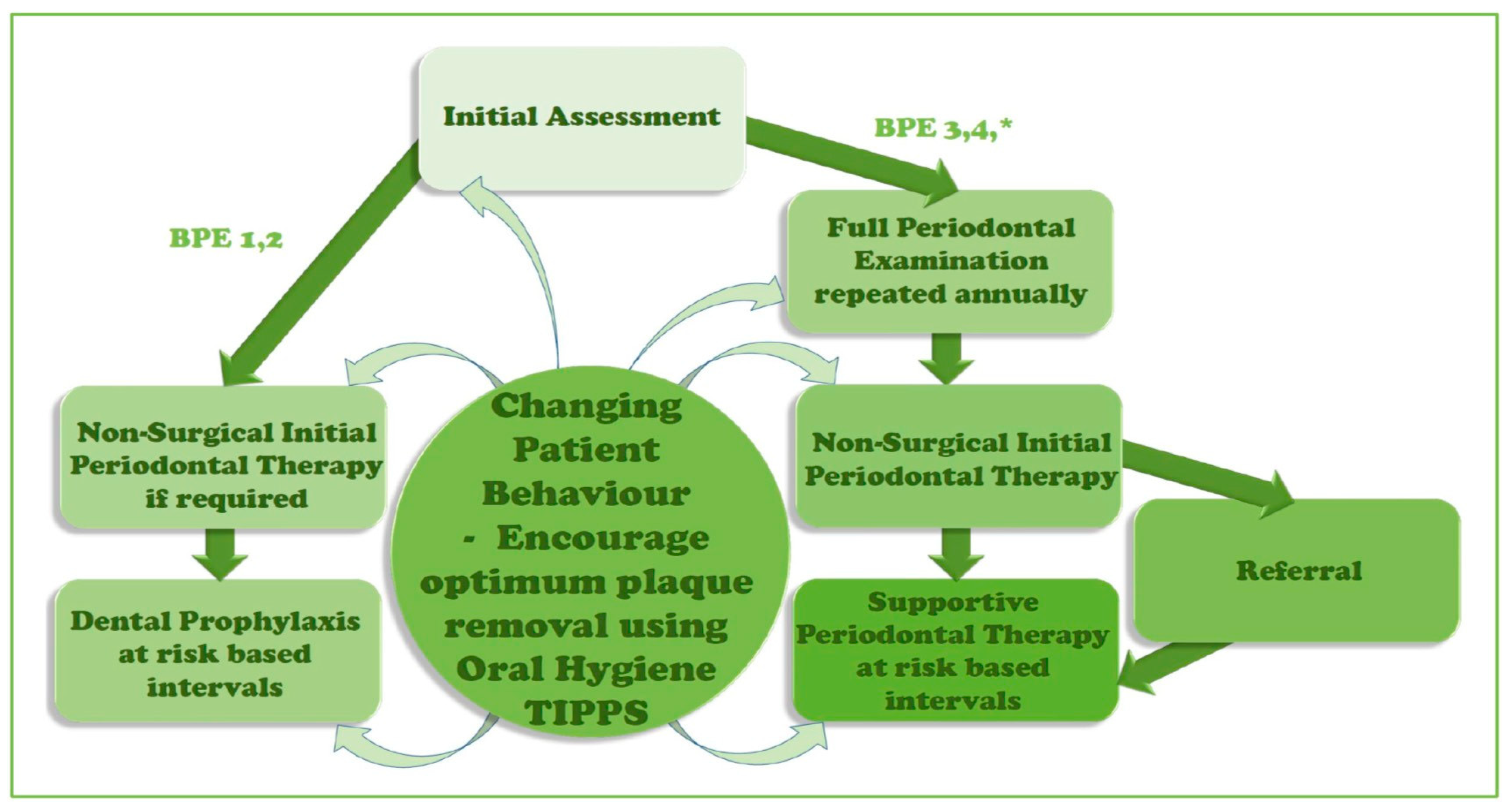{kind=link}
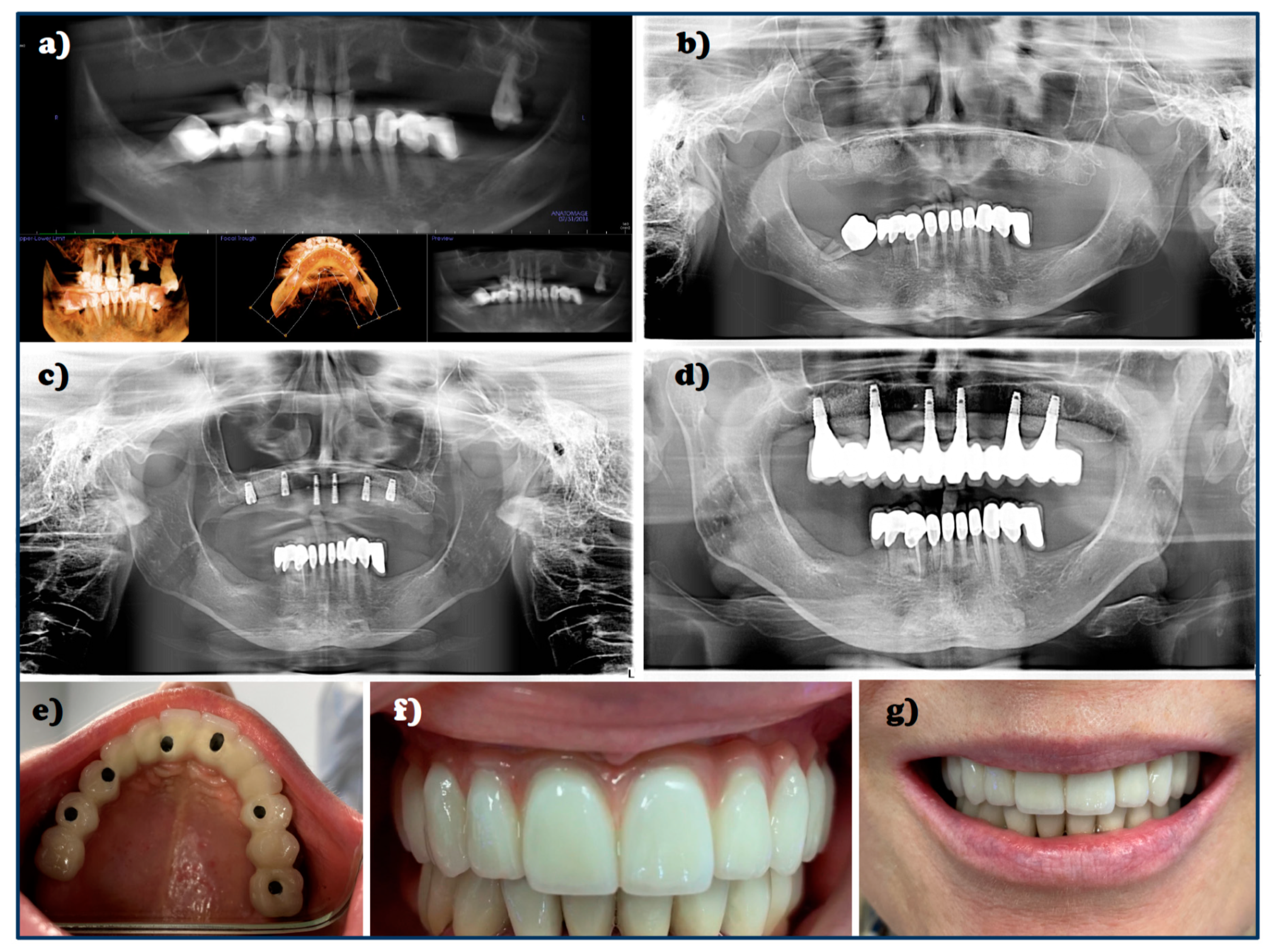{kind=link}
{kind=link}
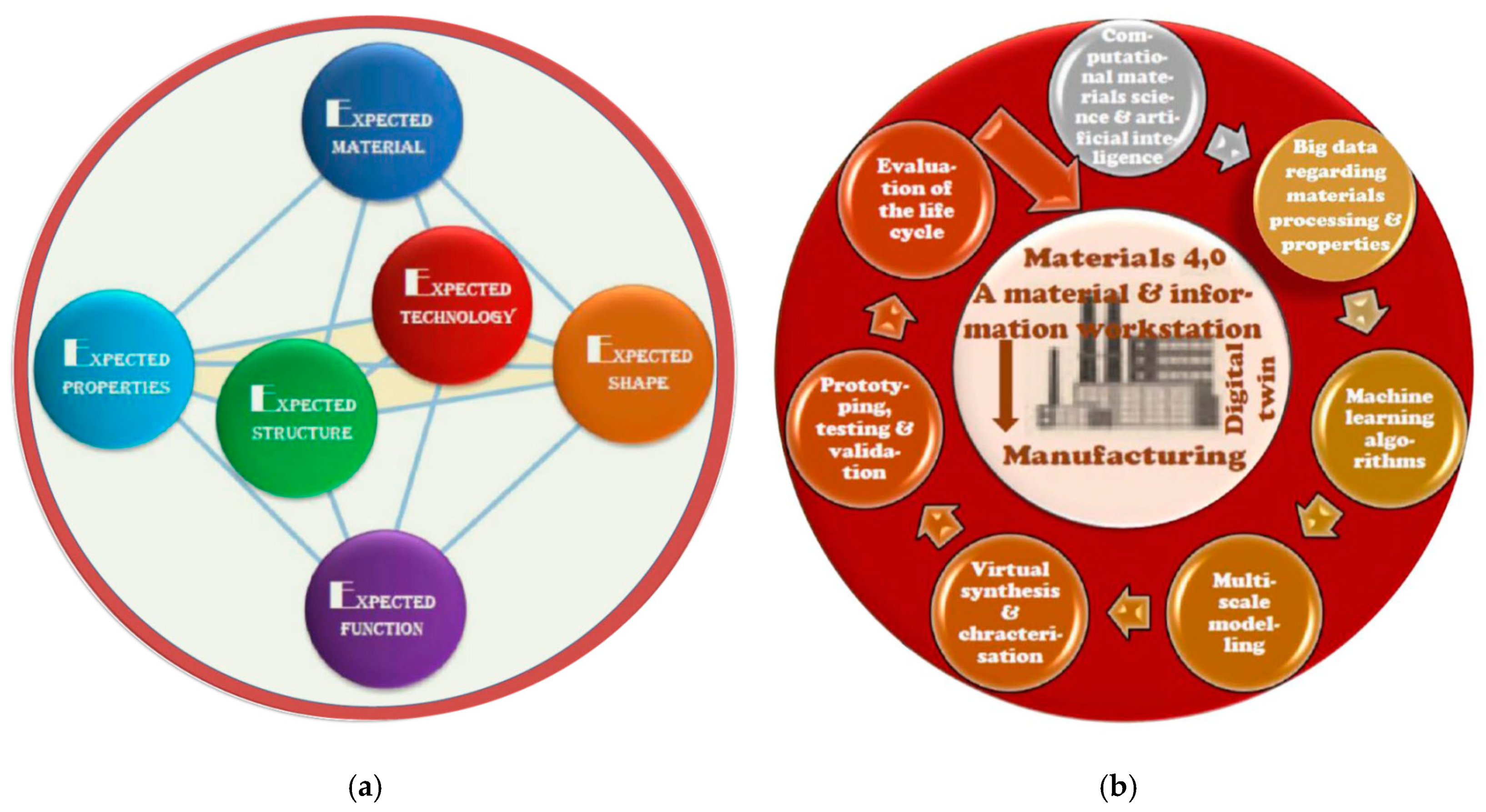{kind=link}
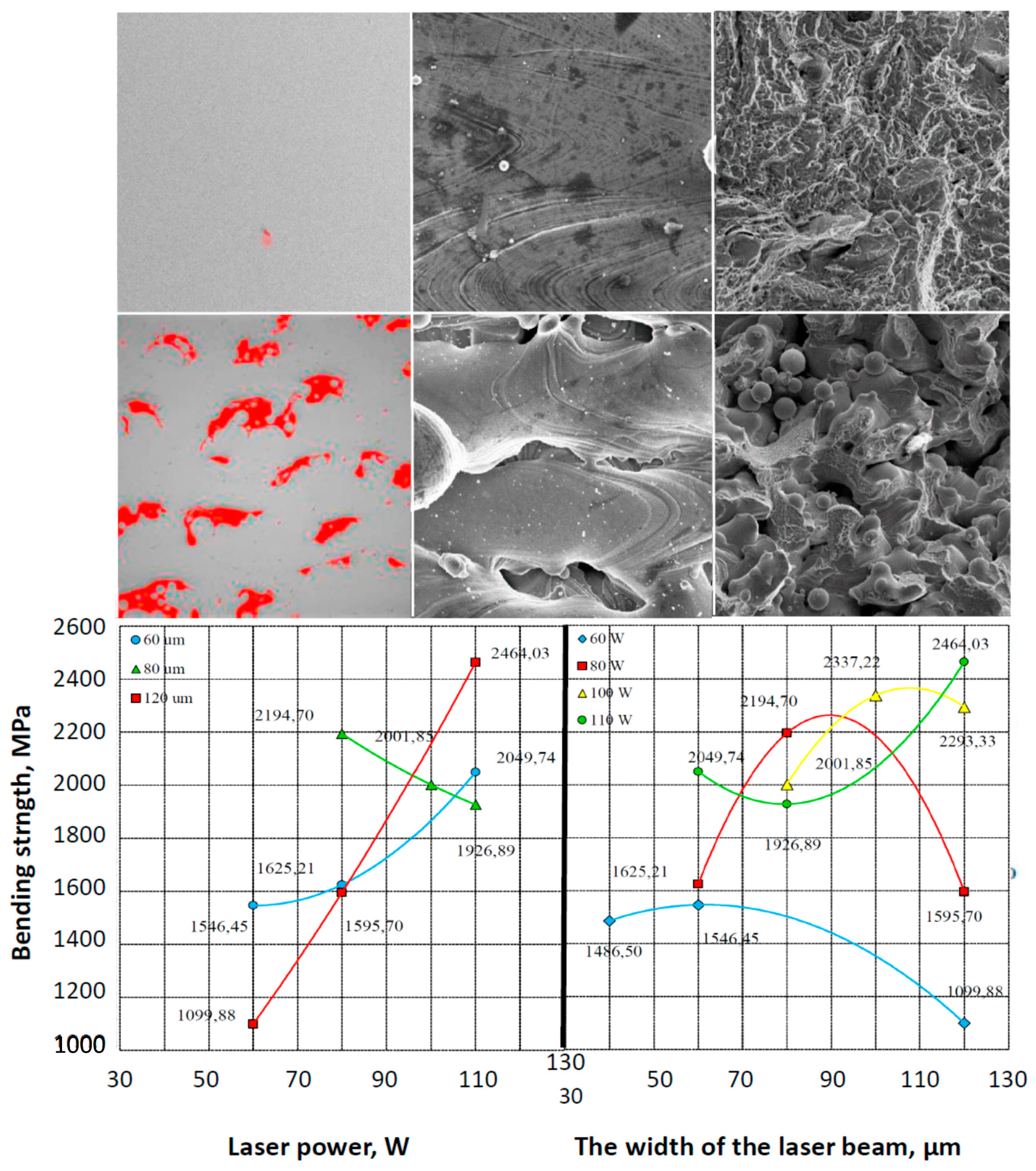{kind=link}
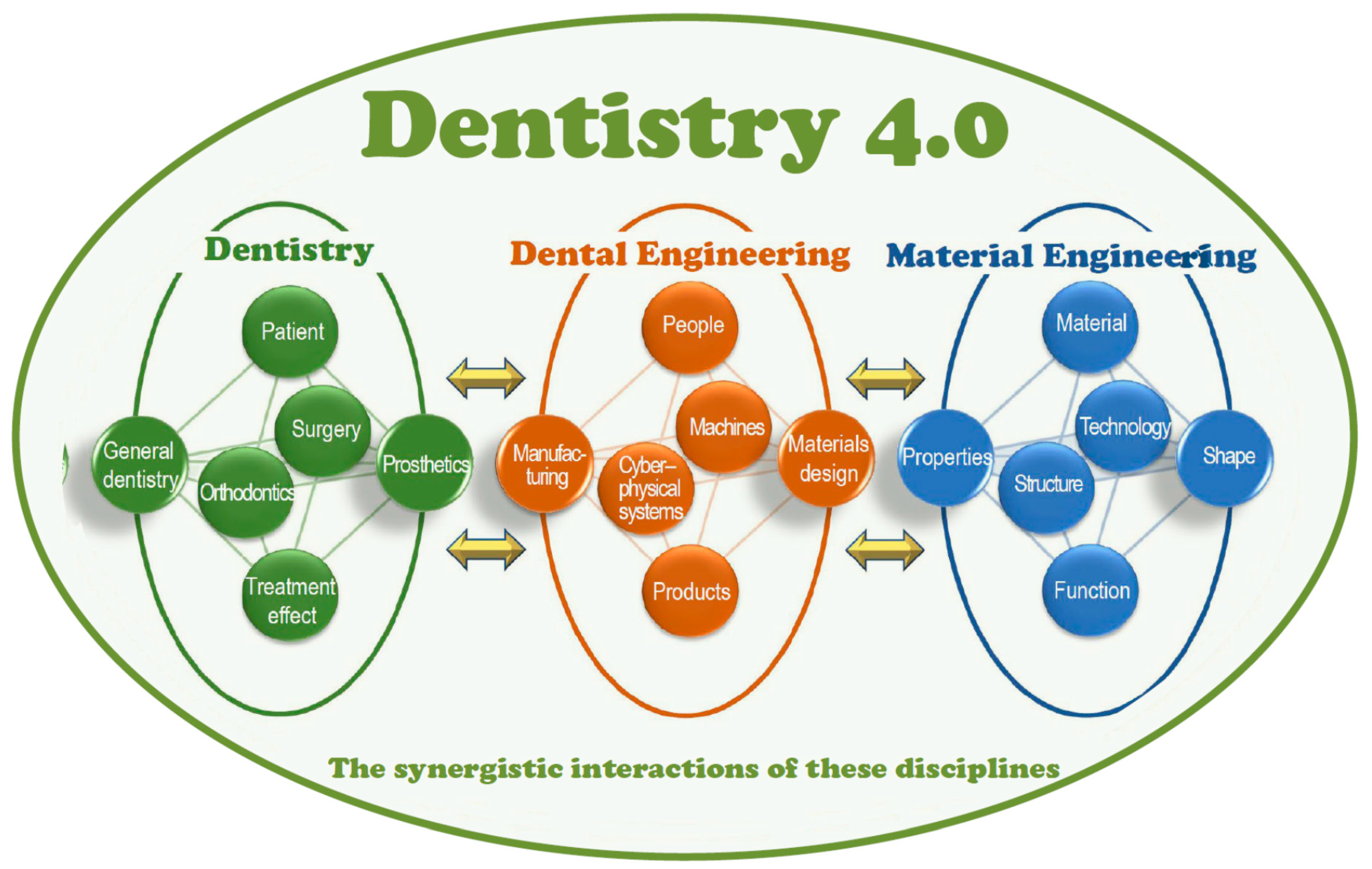{kind=link}
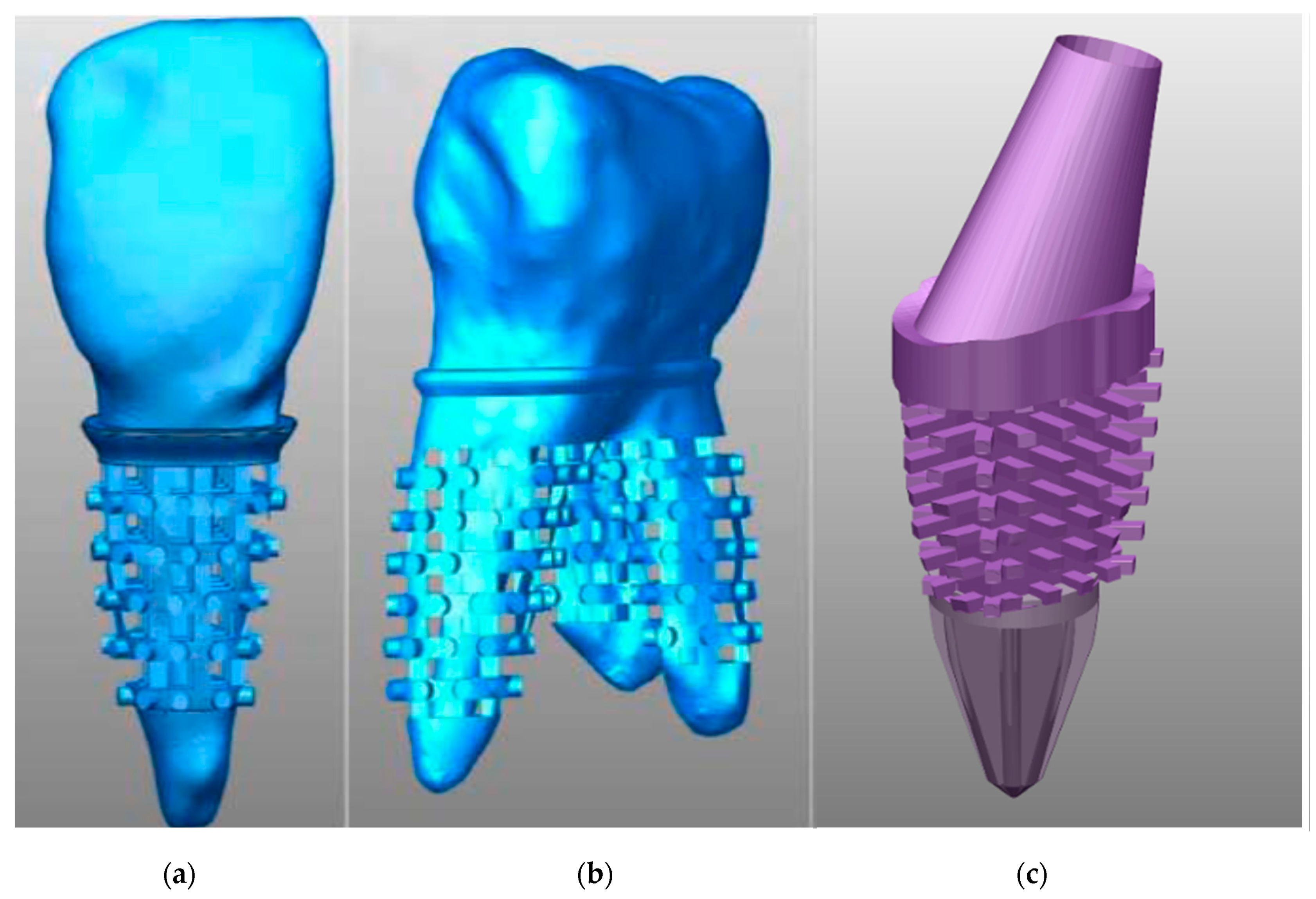{kind=link}
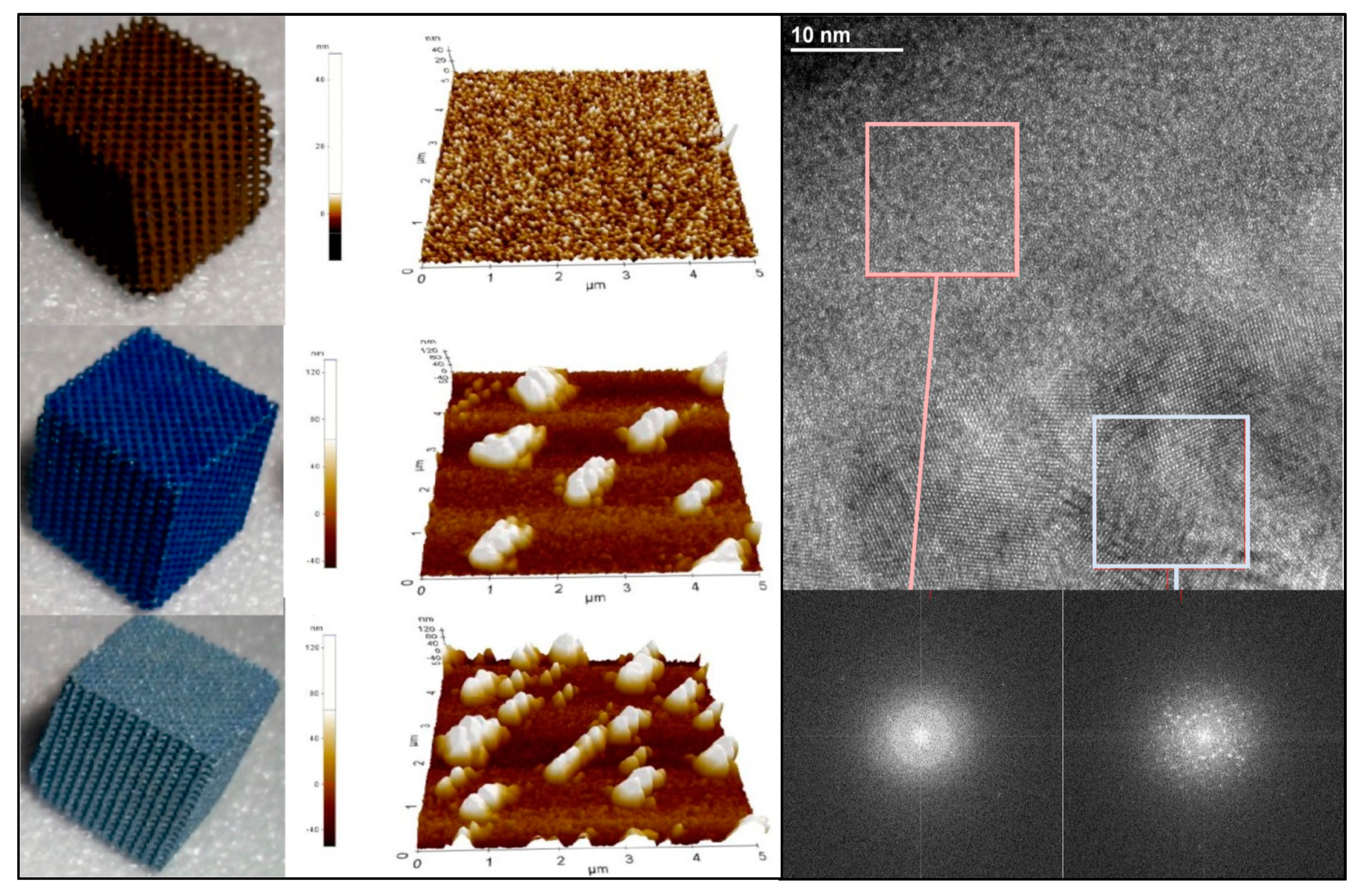{kind=link}
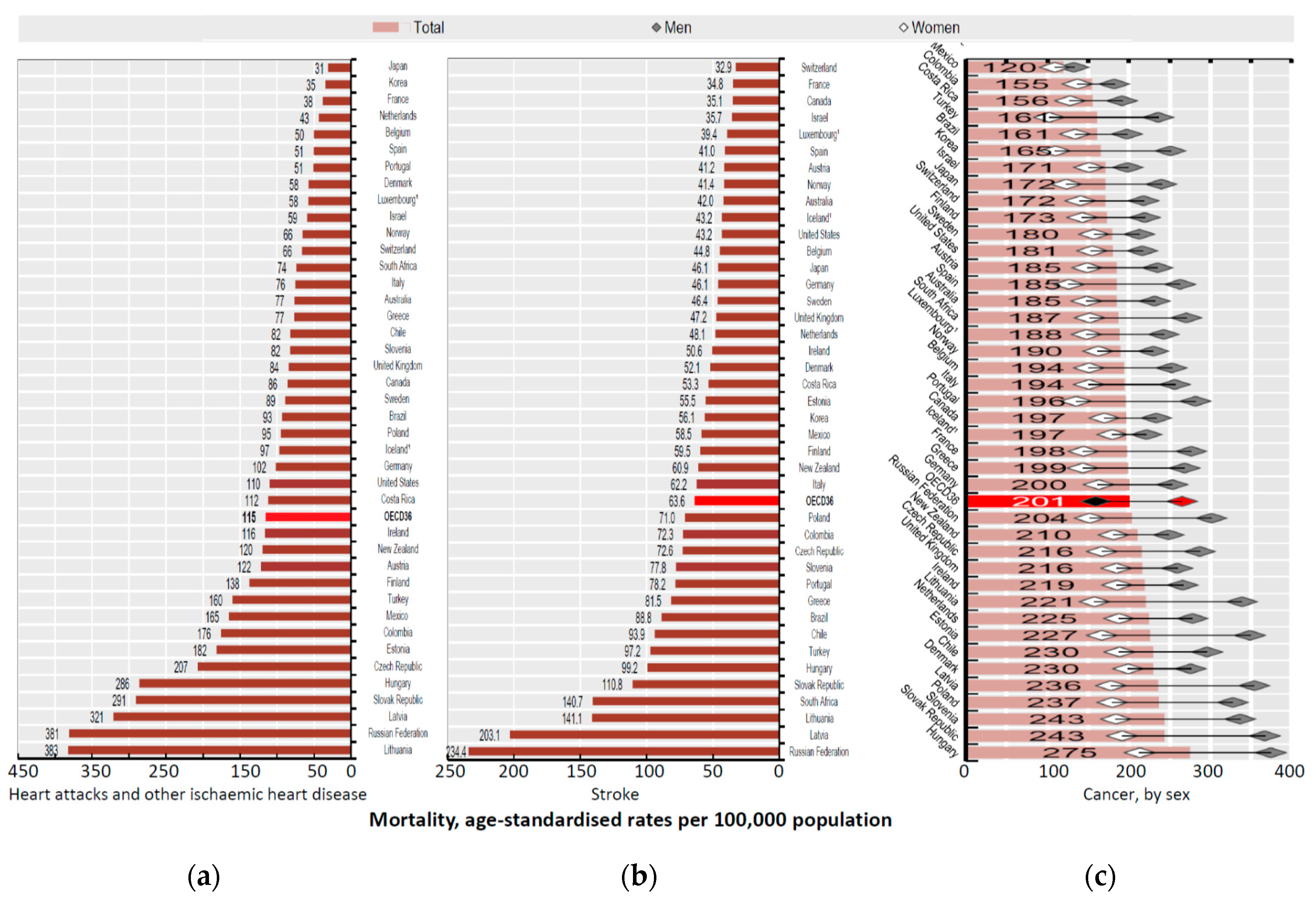{kind=link}
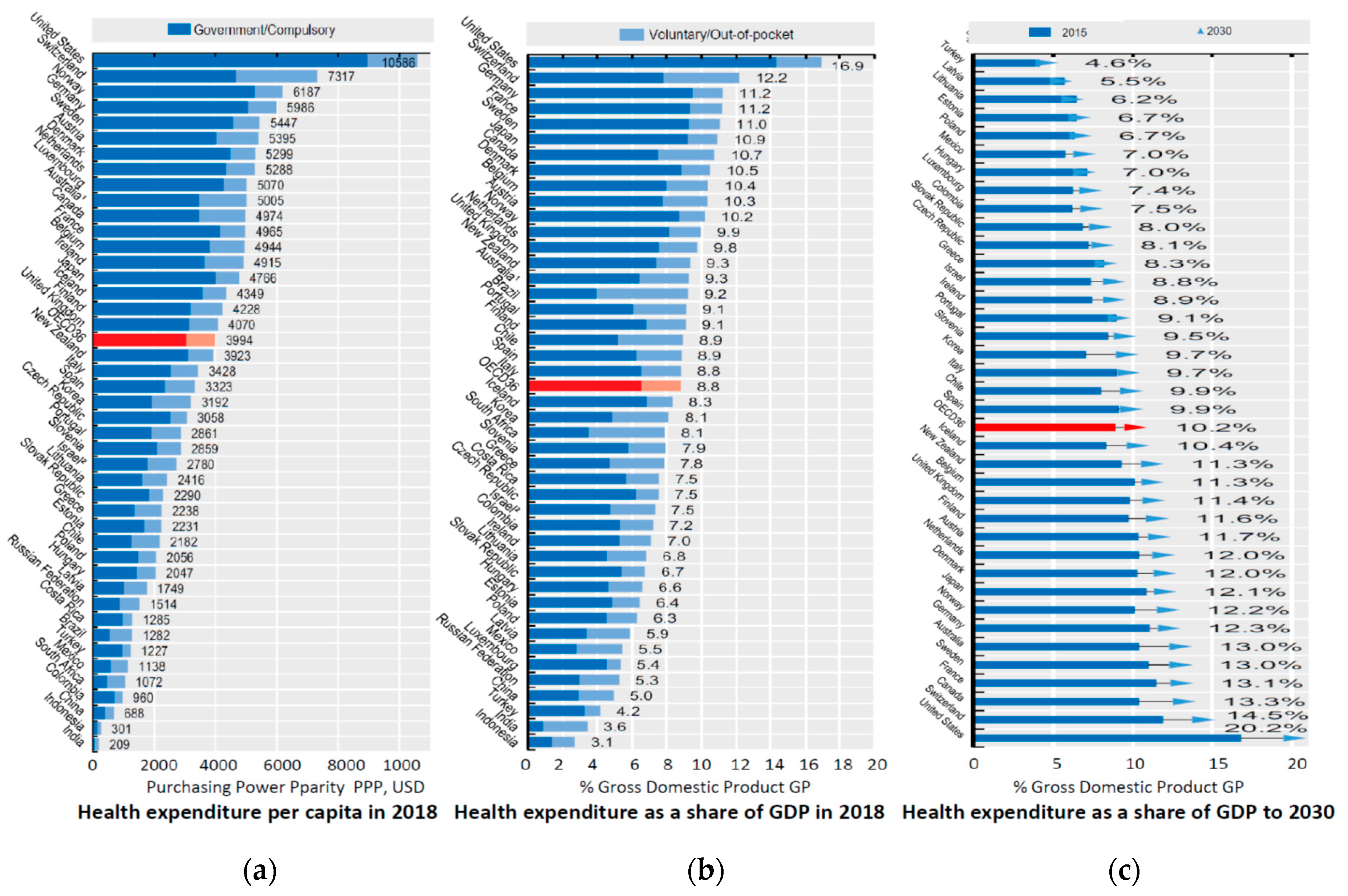{kind=link}
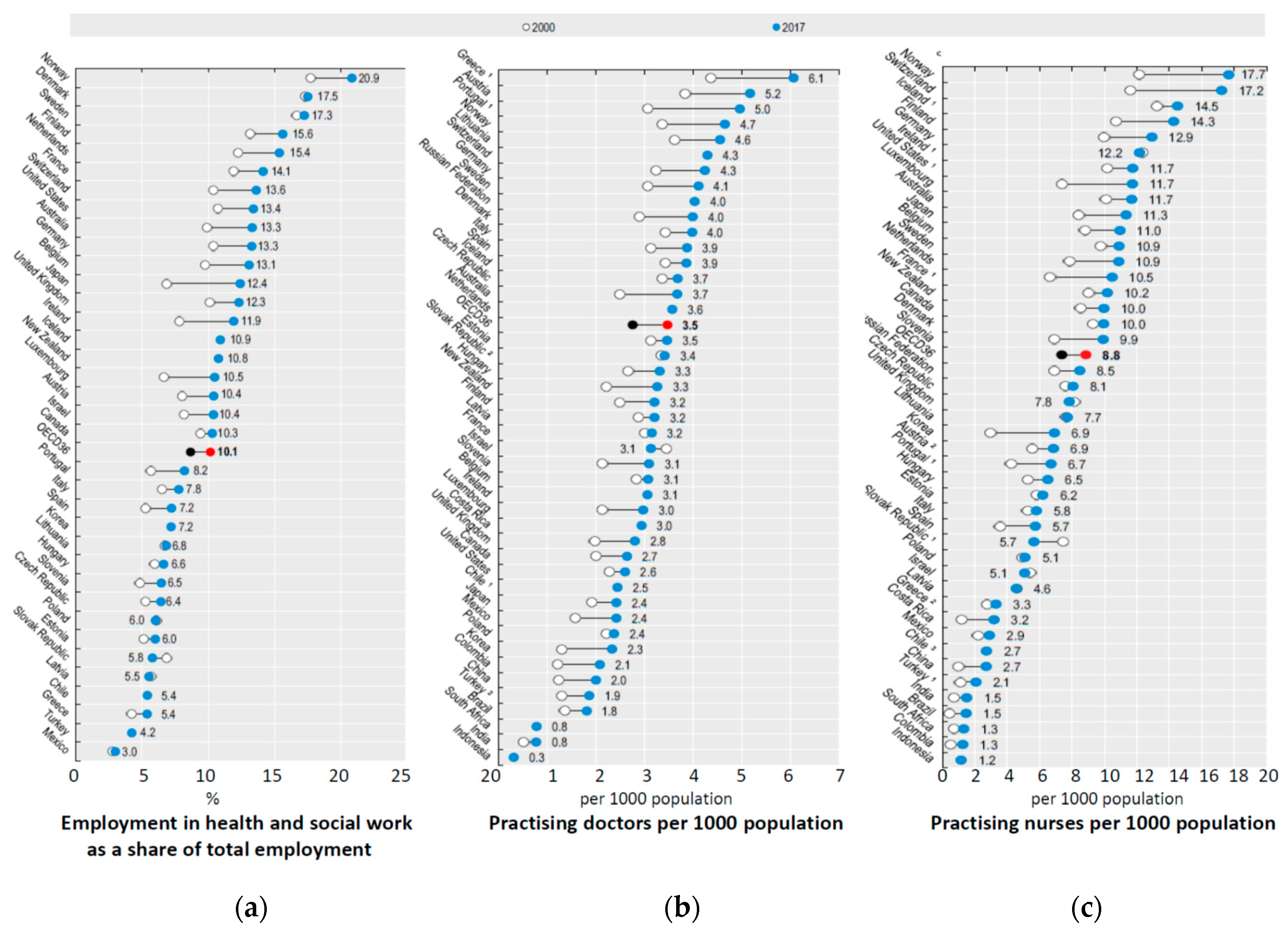{kind=link}
{kind=link}
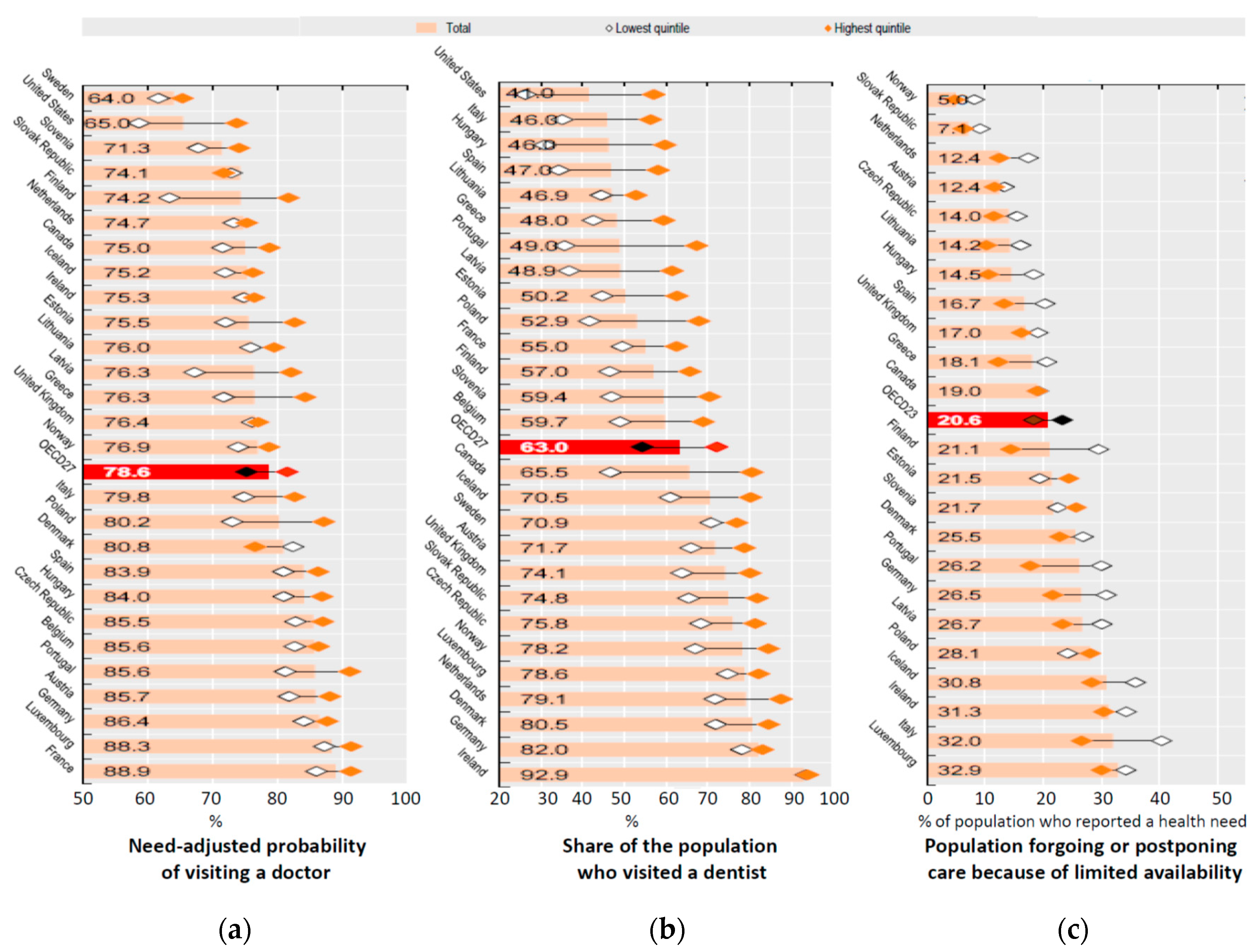{kind=link}
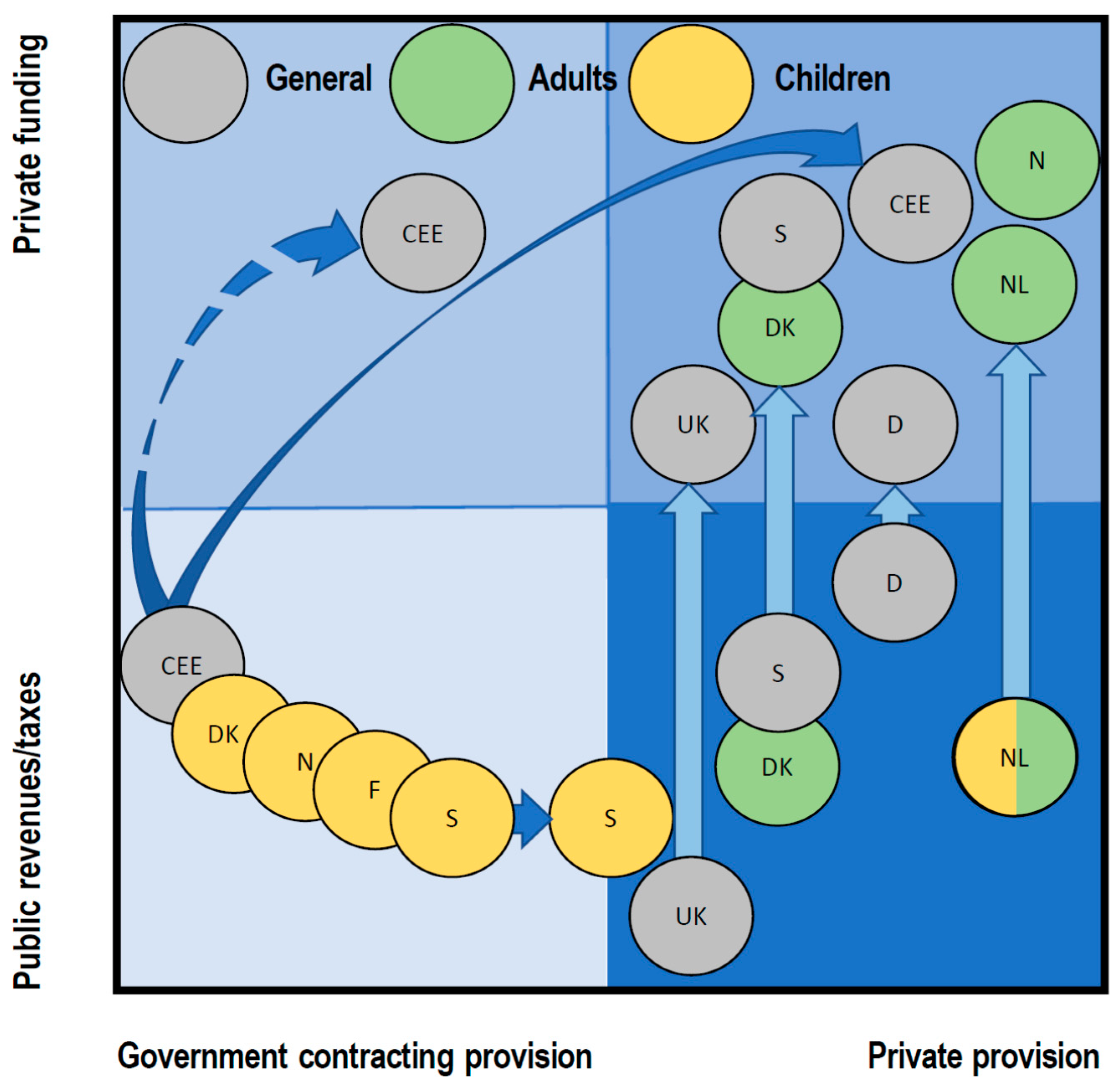{kind=link}
{kind=link}
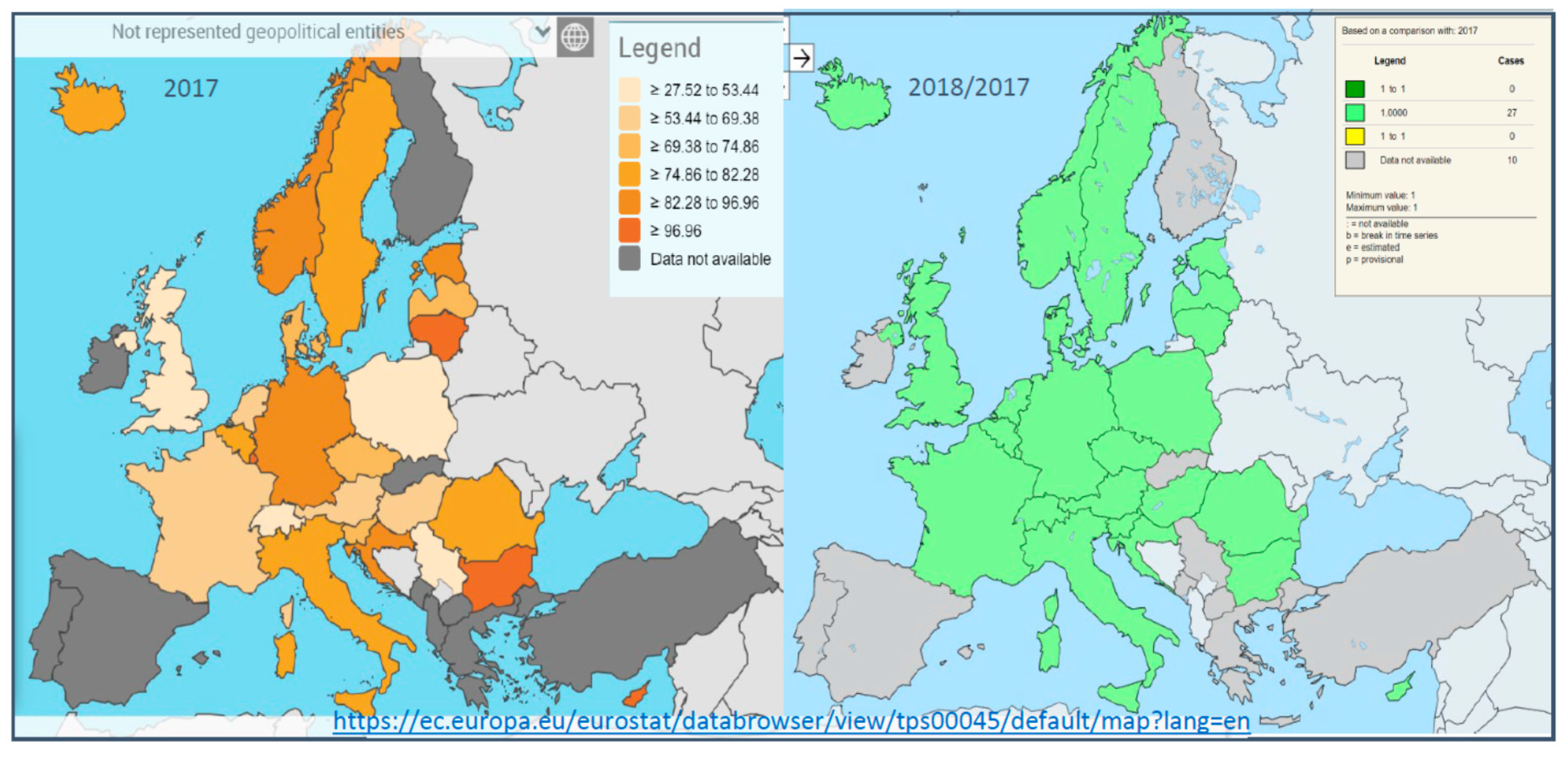{kind=link}
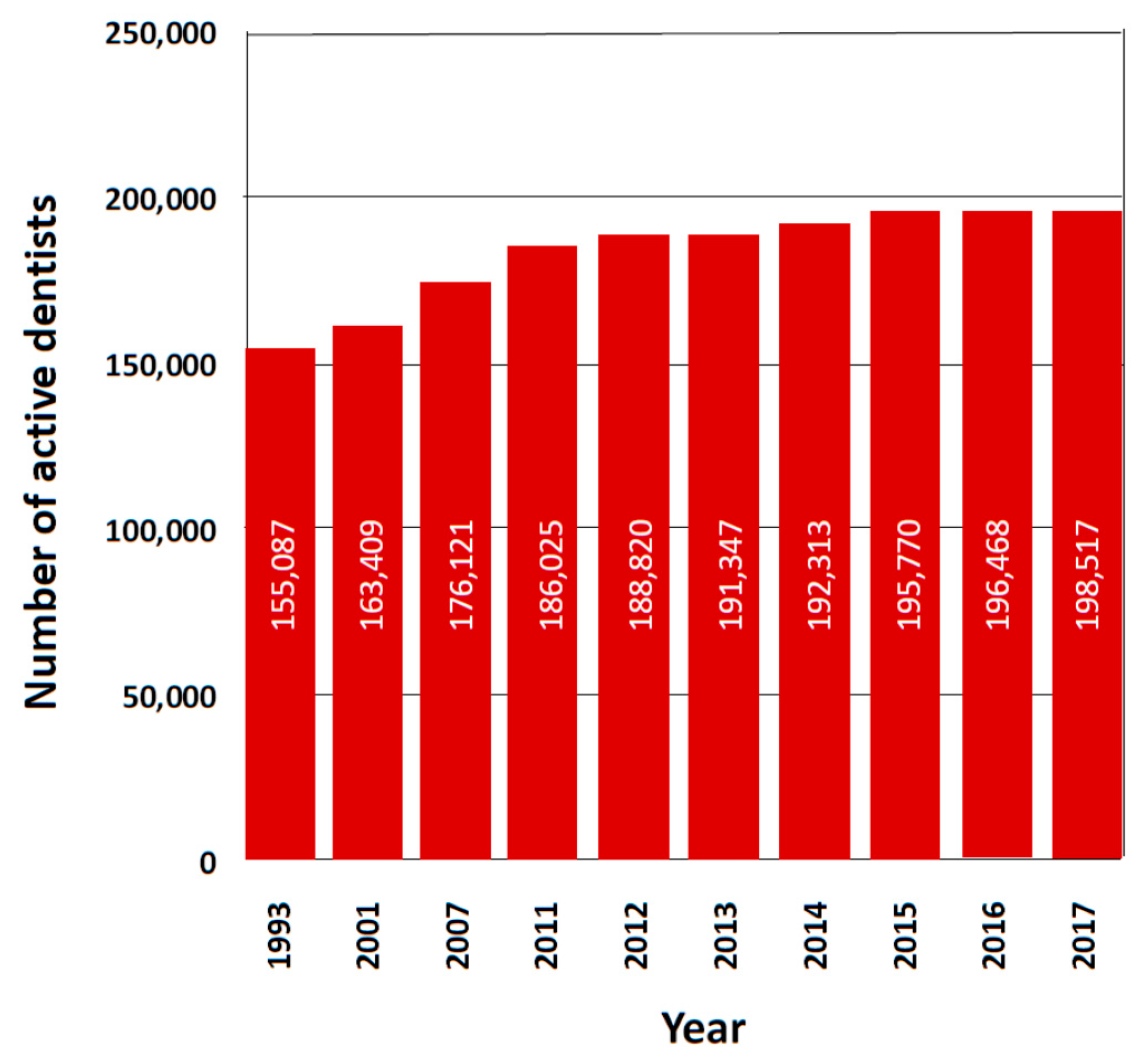{kind=link}
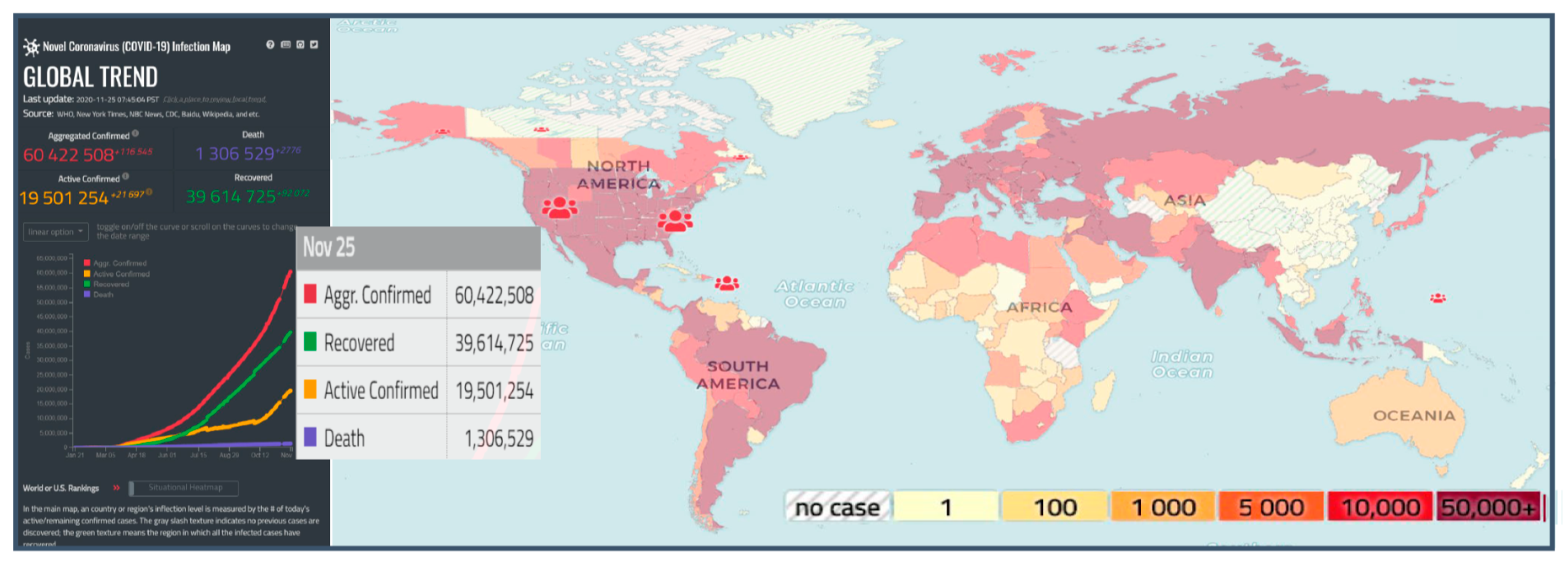{kind=link}
{kind=link}
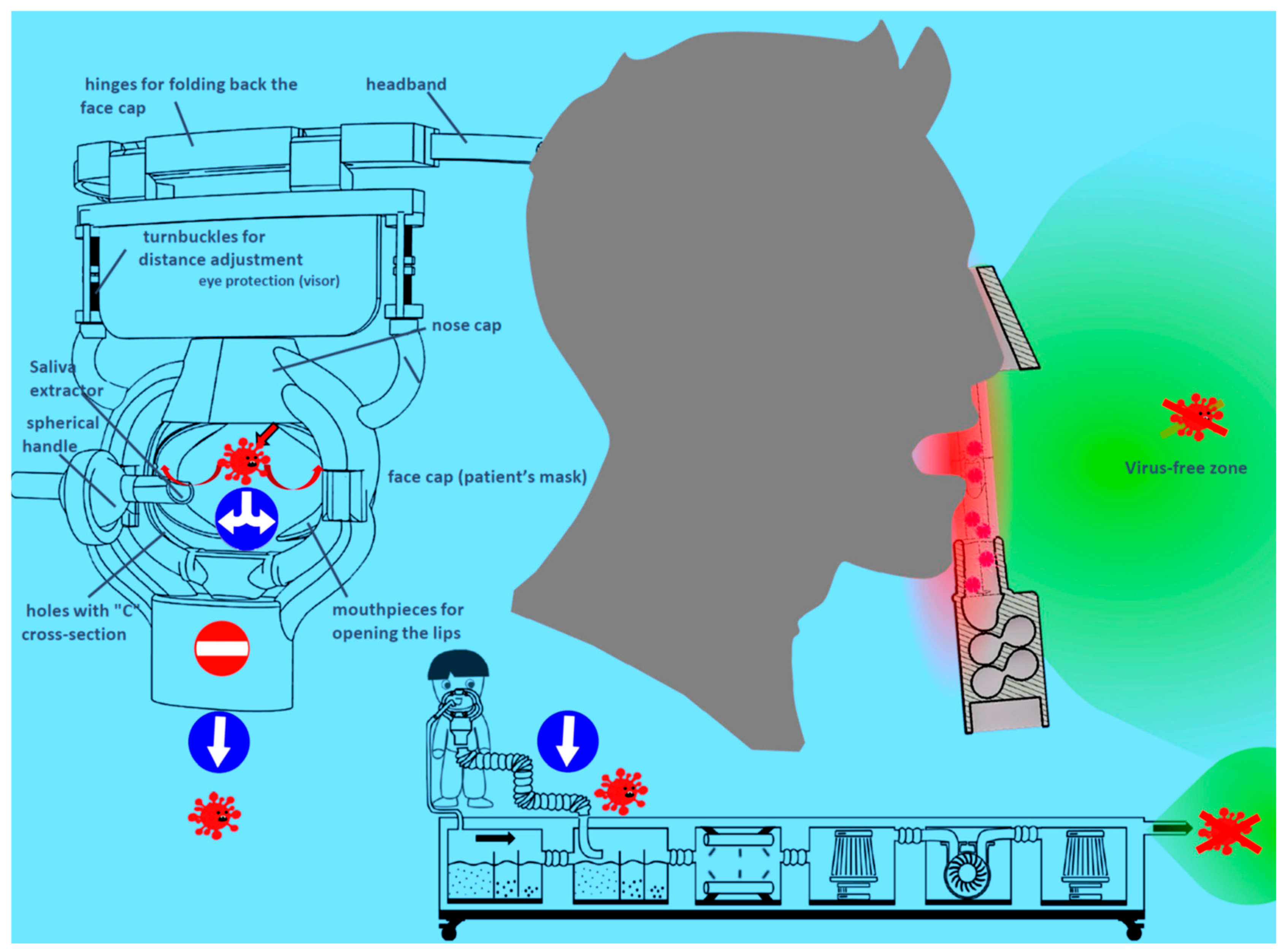{kind=link}
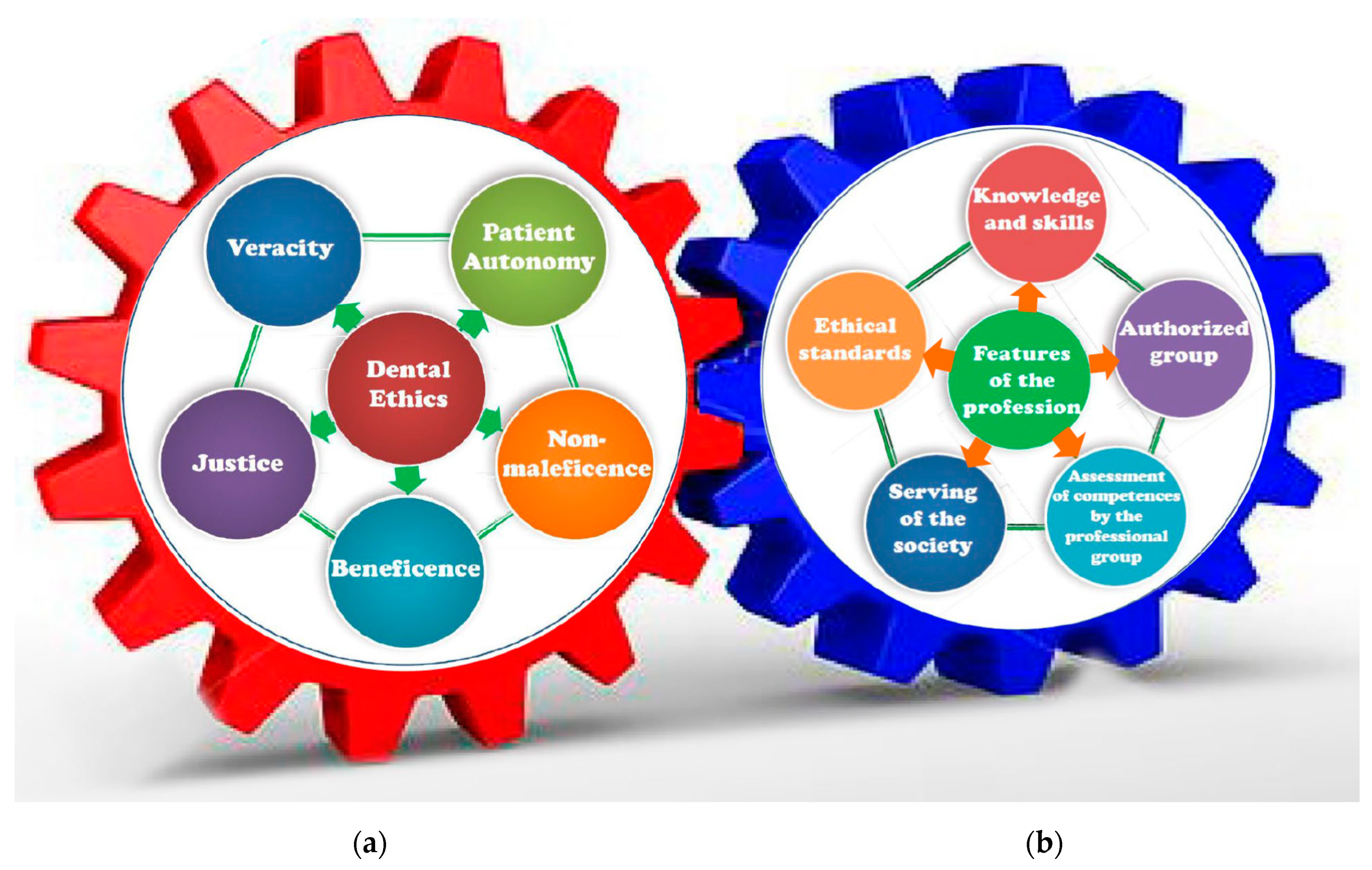{kind=link}
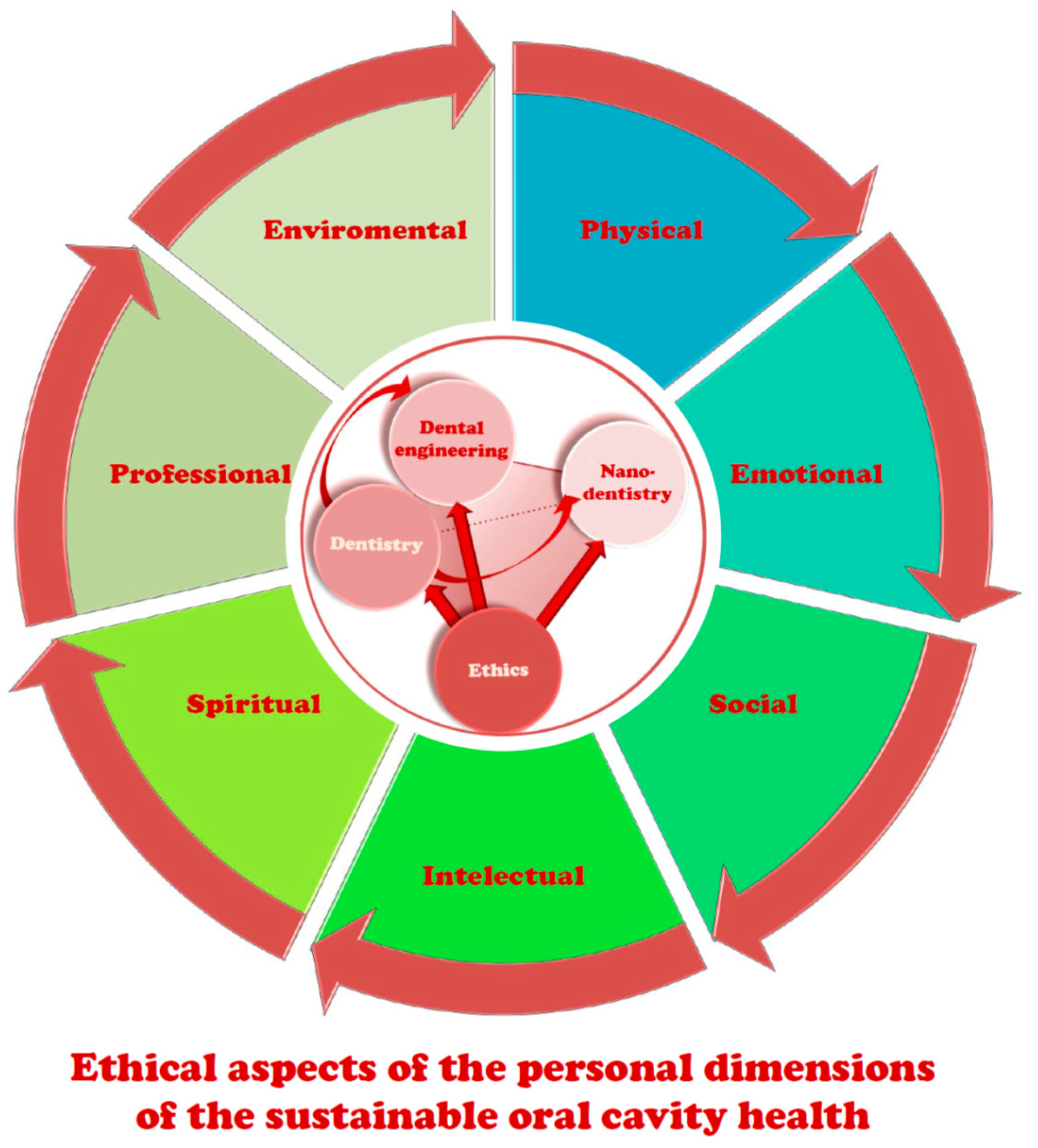{kind=link}
{kind=link}
| No. | Classification Basis | Classification |
|---|---|---|
| 1 | Treatment of Caries | D = decayed or caries lesions, M = missing owing to extraction, F = filled or restored caries lesions |
| 2 | Morphology (Location of the Lesion) | Occlusal caries, smooth-surface caries and root caries |
| 3 | Prior Condition of the Tooth | Primary caries, secondary (recurrent) caries |
| 4 | Severity and Rate of Caries Progression | Acute caries, chronic caries, active caries and arrested caries |
| 5 | Extent of the Lesion | Incipient caries, advanced caries |
| 6 | Chronology or Age | Early childhood caries, adolescent caries, adult caries |
| 7 | Etiology (Causes or Origins of Caries) | Baby bottle tooth decay |
| 8 | Affected tissues | Enamel, dentin, cementum |
| Disease Development Stages | Basic Symptoms in the Subsequent Stages of the Disease Development |
|---|---|
| Gingivitis | This is caused by plaque; there are red, swollen tissues that bleed when brushing and probing. |
| Chronic periodontitis | There is a slow destruction of the connective epithelium and attachment of the connective tissue of the tooth, bone destruction with a loss of bone mass, and the formation of periodontal pockets. |
| Aggressive periodontitis | The degree of destruction of the attachment of connective tissue and bone is severe at the rapid progression of the disease; severe condition in the group of younger patients is related to a family history of aggressive periodontitis. |
| Necrotizing ulcerative gingivitis (NUG) | Necrotizing ulcerative periodontitis (NUP) is present in the presence of the loss of connective tissue and bone destruction, manifested by the painful ulceration of the ends of the interdental papillae with visible gray necrotic tissue accompanied by halitosis. |
| Periodontal abscess | There is acute or chronic and asymptomatic freely draining infection of the periodontal pocket. |
| Perio-endo lesions | The source of the bacteria is from the periodontium or the root canal system, while lesions may heal or may be independent. |
| Gingival enlargement | Irritation from plaque or tartar, as well as repeated rubbing or trauma, as well as fluctuating hormone levels or the use of certain medications, cause the gingivae to thicken. |
| Periodontal Diseases and Conditions | ||
|---|---|---|
| Periodontal Health, Gingival Diseases and Conditions | Forms of Periodontitis | Periodontal Manifestations of Systemic Diseases And Developmental and Acquired Conditions |
|
|
|
| ||
|
and Related Health Problems codes |
|
| ||
|
|
|
| 1 Severity: Interdental clinical attachment level (CAL) at site with greatest loss; radiographic bone loss and tooth loss. 2 Complexity of management: probing depths, pattern of bone loss, furcation lesions, number of remaining teeth, tooth mobility, ridge defects, masticatory dysfunction. 3 Add to stage as descriptor: localized <30% teeth, generalized 30% teeth. 4 Risk of progression: direct evidence by paradiographs or CAL loss, or indirect (bone loss/age ratio). 5 Anticipated treatment response: case phenotype, smoking, hyperglycemia. | ||
| No | Steps by the dentist to assess BPE |
|---|---|
| 1 | A World Health Organization WHO BPE probe is used. This has a “ball end” 0.5 mm in diameter, and a black band from 3.5 to 5.5 mm. Light probing force should be used (20–25 g). |
| 2 | The dentition is divided into 6 sextants: upper right (17 to 14), upper anterior (13 to 23), upper left (24 to 27). lower right (47 to 44), lower anterior (43 to 33), lower left (34 to 37). |
| 3 | All teeth in each sextant are examined (with the exception of 3rd molars). |
| 4 | For a sextant to qualify for recording, it must contain at least 2 teeth (if only 1 tooth is present in a sextant, the score for that tooth is included in the recording for the adjoining sextant). |
| 5 | The probe should be “walked around” the sulcus/pockets in each sextant, and the highest score recorded. As soon as a code 4 is identified in a sextant, the clinician may then move directly on to the next sextant, though it is better to continue to examine all sites in the sextant. This will help to gain a fuller understanding of the periodontal condition, and will make sure that furcation involvements are not missed. If a code 4 is not detected, then all sites should be examined to ensure that the highest score in the sextant is recorded before moving on to the next sextant. |
| Code BPE | Description | |||
|---|---|---|---|---|
| 0 | No pockets > 3.5 mm, no calculus/overhangs, no bleeding after probing (black band completely visible). | |||
| 1 | No pockets > 3.5 mm, no calculus/overhangs, but bleeding after probing (black band completely visible). | |||
| 2 | No pockets > 3.5 mm, but supra- or subgingival calculus/overhangs (black band completely visible). | |||
| 3 | Probing depth 3.5–5.5 mm (black band partially visible, indicating pocket of 4–5 mm). | |||
| 4 | Probing depth > 5.5 mm (black band entirely within the pocket, indicating pocket of 6 mm or more). | |||
| * | Furcation involvement. | |||
| Comments: Both the number and the * should be recorded if a furcation is detected—e.g., the score for a sextant could be 3 * (e.g., indicating probing depth 3.5–5.5 mm plus furcation involvement in the sextant). | ||||
| An example BPE score grid: | 4 | 3 | 3 * | |
| - | 2 | 4 * | ||
| Indicator Type | Description or Specification | |
|---|---|---|
| BOP Bleeding on Probing (Papilla Bleeding Index PBI) | Assesses the presence of bleeding gums; a patient with less than 10% bleeding is counted as having a healthy mouth cavity; this indicator is assessed using a WHO or North Carolina probe; the probe should “go around” the pocket on each side and if there is bleeding, the site is noted on the plot (at the mesial, distal, buccal, palatal and lingual surfaces); after using the appropriate computer software, the system calculates the proportion of bleeding areas. | |
| PI Plaque Index (Approximal Plaque Index API) | Assesses the presence of plaque; this indicator is assessed using a WHO or North Carolina probe or by plate staining; the probe should “go around” the tooth on each side and if plaque is present, the site is noted on the plot (at the mesial, distal, buccal, palatal and lingual surfaces); after using the appropriate computer software, the system calculates the proportion of biofilm area. | |
| PPDs Periodontal Probing Depths | Assesses the depth of the pockets; this index is assessed using the North Carolina probe; the probe should “go around” the pocket on each side and record the measurement results in millimeters on a plot with the location (at the mesial, distal, buccal, palatal and lingual surfaces). | |
| REC Gum Recession Index | Assesses gingival recessions; this index is assessed using the North Carolina probe; the results of measurements of the distance in millimeters from the cement-enamel junction (CEJ) [232] to the gingival margin should be made and recorded. | |
| MOB Mobility Index | Assesses the degree of tooth mobility: the other end of the mirror and a metal probe can be used to determine this index; While holding the lock with two tools, move it in all directions. | |
| Code | Grade on a scale of 0–3. | |
| 0 | No movable property. | |
| 1 | Gentle mobility. | |
| 2 | The tooth moves horizontally >1 mm. | |
| 3 | The tooth moves horizontally and vertically >2 mm. | |
| FUR Furcation Index | Assesses the degree of furcation using a furcation probe. | |
| Code | Measure with an appropriate furcation probe. | |
| A | Measurement with a furcation probe 1–3 mm. | |
| B | Measurement with a furcation probe 4–6 mm. | |
| C | Measurement with furcation probe >7 mm. | |
| Diagnosis | Preventive and/or Therapeutic Measures Necessary to Be Taken by a Dentist | Treatment Phase | ||
|---|---|---|---|---|
| Code BPE | Description | |||
| 0 | normal | No need for periodontal treatment. | 0 | No treatment required |
| 1 | bleeding after probing | OHI | I | Hygienic training |
| 2 | dental stone supra- or subgingival, iatrogenic injuries | OHI, the removal of plaque retentive factors, including all supra- and subgingival calculus. | II | I + scaling supra- and subgingival |
| 3 | depth of periodontal pockets 3.5–5.5 mm | OHI, RSD | ||
| 4 | depth of periodontal pockets >6 mm | OHI, RSD. Assess the need for more complex treatment; referral to a specialist may be indicated. | III | I = II + surgical treatment |
| * | furcations | OHI, RSD. Assess the need for more complex treatment; referral to a specialist may be indicated. | ||
| Comments: As a general rule, radiographs to assess alveolar bone levels should be obtained for teeth or sextants where BPE codes 3 or 4 are found. | ||||
| Abbreviations: OHI—oral hygiene instruction; RSD—root surface debridement. | ||||
| No | Type of Method Known in the Literature, State-of-the-Art Including Own Solution | Potential | Attracti-Veness |
|---|---|---|---|
| 1 | Installation of air filtering devices in the treatment room | 6.7 | 4.0 |
| 2 | Equipment operating with HEPA or carbon filters or with UV radiation | 5.95 | 4.0 |
| 3 | Dental saliva extractor attachments | 3.3 | 5.8 |
| 4 | “Extract from the treatment area” devices | 3.7 | 6.6 |
| 5 | Patient enclosures in the form of glass or PMMA boxes | 1.45 | 3.9 |
| 6 | Original solution eliminating the threat at the source with the set of devices for virus elimination | 9.0 | 8.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dobrzański, L.A.; Dobrzański, L.B.; Dobrzańska-Danikiewicz, A.D.; Dobrzańska, J. The Concept of Sustainable Development of Modern Dentistry. Processes 2020, 8, 1605. https://doi.org/10.3390/pr8121605
Dobrzański LA, Dobrzański LB, Dobrzańska-Danikiewicz AD, Dobrzańska J. The Concept of Sustainable Development of Modern Dentistry. Processes. 2020; 8(12):1605. https://doi.org/10.3390/pr8121605
Chicago/Turabian StyleDobrzański, Leszek A., Lech B. Dobrzański, Anna D. Dobrzańska-Danikiewicz, and Joanna Dobrzańska. 2020. "The Concept of Sustainable Development of Modern Dentistry" Processes 8, no. 12: 1605. https://doi.org/10.3390/pr8121605
APA StyleDobrzański, L. A., Dobrzański, L. B., Dobrzańska-Danikiewicz, A. D., & Dobrzańska, J. (2020). The Concept of Sustainable Development of Modern Dentistry. Processes, 8(12), 1605. https://doi.org/10.3390/pr8121605