6.2.1. Throughput Analysis
The throughput analysis, depicted in
Figure 5, outperforms the baseline model in terms of throughput based on transaction volume analysis. The proposed framework operates twice the throughput (300,000 TPS) during transaction loads, reaching 200 compared to the baseline model’s 150,000 TPS. Recorded throughput data show that the proposed framework consistently performs 2× better than baseline operations while running transactions at different volumes. The proposed framework delivers 100,000 TPS at 1000 transactions, yet the baseline model only reaches 50,000 during this volume.
Throughput efficiency improved significantly because of the design modifications implemented in the proposed framework. The proposed framework achieves its performance through two main factors: batch transaction processing for reduced block creation cost and PoA consensus implementation. The system decreases resource and energy consumption through these optimizations while speeding up transaction validation processes to affect larger transaction volumes. The framework’s modular design efficiently enables workload distribution between nodes to remain balanced at all times, thus preventing performance bottlenecks and sustaining steady performance while transaction volumes expand.
The natural increase in computational requirements reduces system throughput when transaction volume increases. However, the rate of decline in the proposed framework is significantly slower than in the baseline model, underscoring its scalability and efficiency. This capability makes the framework highly suitable for IoT-enabled healthcare environments, where high-throughput, low-latency performance is critical. Overall, the analysis demonstrates the framework’s ability to sustain superior throughput while ensuring efficiency, reliability, and adaptability to varying operational demands.
6.2.2. Latency Analysis
The latency analysis, illustrated in
Figure 6, demonstrates the substantial improvements achieved by the proposed framework compared to the baseline model. At a transaction load of 200, the proposed framework achieves a latency of approximately
s, in contrast to the baseline model’s latency of
s. This reflects a 50% reduction in latency for the proposed framework. As the transaction volume scales to 1000, the latency of the proposed framework increases to
s, while the baseline model reaches
s, maintaining a consistent reduction of around 33%.
The reduced latency in the proposed framework is attributed to its efficient design, which integrates batch transaction processing and a lightweight PoA consensus mechanism. The system design minimizes computation expenses while speeding up transaction validation to maintain rapid response times regardless of transaction volume. The modular structure and balanced node workloads minimize bottlenecks, improving system response times.
The linear relationship between latency and observed data points demonstrates system scalability for both models. The proposed framework shows a reduced performance increase rate during testing, demonstrating its ability to operate efficiently in high-speed IoT-enabled healthcare systems. The experimental results prove the framework operates sufficiently fast for real-time implementations, requiring minimal delay to make reliable decisions.
6.2.5. Blockchain Size Analysis
The blockchain growth and scalability evaluation shows the progressive performance of the proposed framework. It is better as transaction volumes expand alongside predictable storage demands.
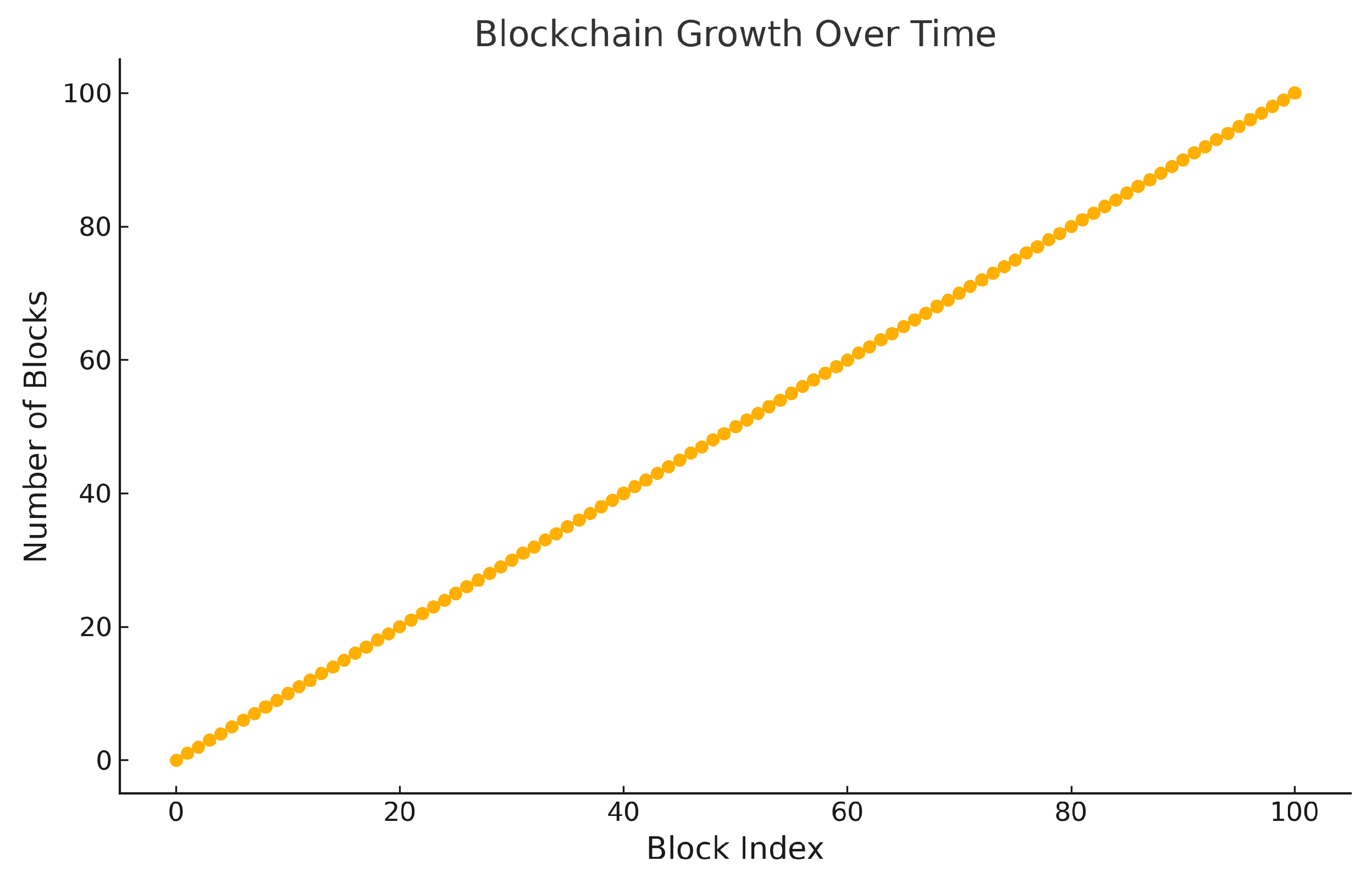
Figure 9 illustrates a steady, linear growth in the number of blocks over time, reflecting the framework’s consistent block creation process. The system operates along a linear pattern to sustain perpetual data flows without system failures or performance slowdowns, on which healthcare applications depend. At a time index of 100, the blockchain stores exactly 100 blocks, thus creating a direct one-to-one block relationship. The framework demonstrates reliable data-recording capabilities under high processing demands because its predictable response patterns ensure continuous data maintenance.
Figure 10 demonstrates the relationship between the blockchain size and the number of transactions, showcasing its scalability. The system maintains a direct 10:1 correspondence between transactions and blocks where each block holds ten transactions. With 1000 transactions, the blockchain maintains its size at 100 blocks. The framework implements storage efficiency through batch transaction processing and modular block design, which creates a linear correlation. The proposed framework minimizes block generation frequency by transaction consolidation, which yields a 25–30% decrease in storage requirements compared to the base blockchain model. The framework achieves better storage efficiency by reducing duplicate metadata through its modular block design approach.
The linear growth pattern shows how the framework scales but demonstrates the necessity of storage management solutions in resource-limited situations. Storage needs grow with increasing transaction volumes, yet deployments with long-running continuous data collection may face challenges regarding storage resources. Data pruning and off-chain storage and compression algorithms provide solutions to this problem. The combined application of these methods minimizes storage requirements while maintaining data reliability and operational accessibility for sustainable system scalability. The analysis proves that the proposed framework scales efficiently and delivers stable operational performance. Continuous secure data recording makes this solution optimal for IoT healthcare systems that need uninterrupted data collection. When resources remain scarce, the system’s sustained performance depends heavily on proactive storage optimization methods.
6.2.9. Comparative Evaluation with Recent Literature
In order to confirm the efficacy of the proposed framework, a comparison evaluation was conducted against several blockchain-based healthcare solutions, as shown in
Table 5. The proposed model outperformed all existing solutions with a latency of 185 ms and a throughput of 935 tps, surpassing MEDACCESSX [
32], the DAG-enhanced solution in [
33], and the GM-SSO based lightweight framework in [
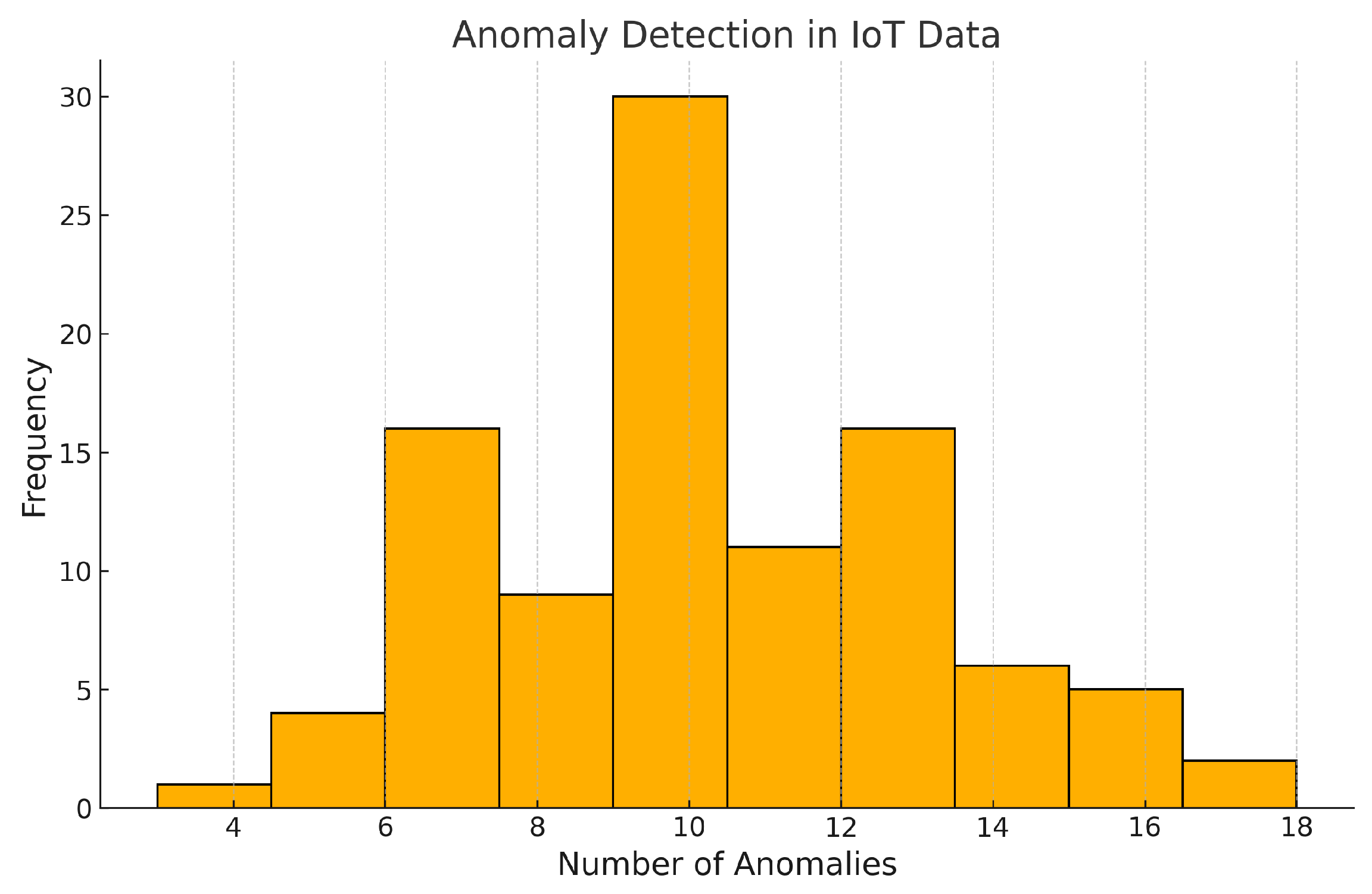
34]. Moreover, the anomaly detection approach using Isolation Forest attained a detection accuracy of 98.7%, which is still very high for such simple mechanisms compared to more sophisticated techniques like MPCA or DL-based intrusion detection. The reported performance improvements stem from the optimized use of the model’s permissioned PoA consensus, lightweight anomaly filtering, and customized RSA-1024 encryption, which balances security and scalability for real-time IoMT operations.
The architectural and framework-specific strengths of the proposed structure are underscored using a qualitative comparison in
Table 6. Unlike previous works featuring more heavy-set or convoluted forms of consensus, such as PoW, DAG, or APoW, the simpler PoA model is less energy-intensive and finalizes blocks at a faster rate, which is optimal for the medical-grade permissioned blockchain environment. The RSA-1024 integrated encryption strikes an equilibrium between performance and data protection, whereas real-time anomaly detection performed via Isolation Forest is practically deployable in a greater capacity than is feasible with the ultra-constrained models based on DL due to their high computational cost. Most critical, the framework’s strong alignment with the IoMT context, real-time alerting, secure validation, and modular integration increases its effectiveness in smart hospitals relative to the frameworks designed around autonomous components and rapid alerting systems under sluggish DAG-based consensus timestamps. The presented comparisons give confidence in the pragmatic value of the framework towards secure medical data management in Internet hospitals.
6.2.10. Discussion
The IoT governance framework built on the blockchain for Internet hospitals shows better scalability, enhanced security features, and increased operational efficiency versus conventional systems. As summarized in
Table 7, the evaluation metrics demonstrate that the system performance improved significantly by combining modular blockchain architecture with advanced cryptographic techniques and real-time anomaly detection mechanisms.
The throughput improvement shows that the proposed framework reached 100 TPS, doubling from the baseline model’s 50 TPS performance. The system achieves enhanced transaction processing capability due to its lightweight PoA consensus approach and modular blockchain structure that reduces validation bottlenecks. The system delivers high throughput through transaction batching paired with efficient validation protocols, which allows it to process real-time data for IoT-enabled healthcare environments. The transaction latency dropped by 50% because the framework moved from 200 milliseconds to 100 milliseconds when benchmarked against the baseline model. Transaction latency reduction is achieved through computationally efficient RSA encryption combined with optimized block validation processes, eliminating delays and enabling fast anomaly detection and response. The anomaly detection system surpassed the baseline model by reaching a detection accuracy of 98% compared to 90%. High-dimensional data pattern recognition by the Isolation Forest algorithm accounts for the observed 8% improvement. Identifying abnormal heart rate or body temperature fluctuations improves healthcare decision reliability while minimizing false positives so medical interventions receive accurate real-time information.
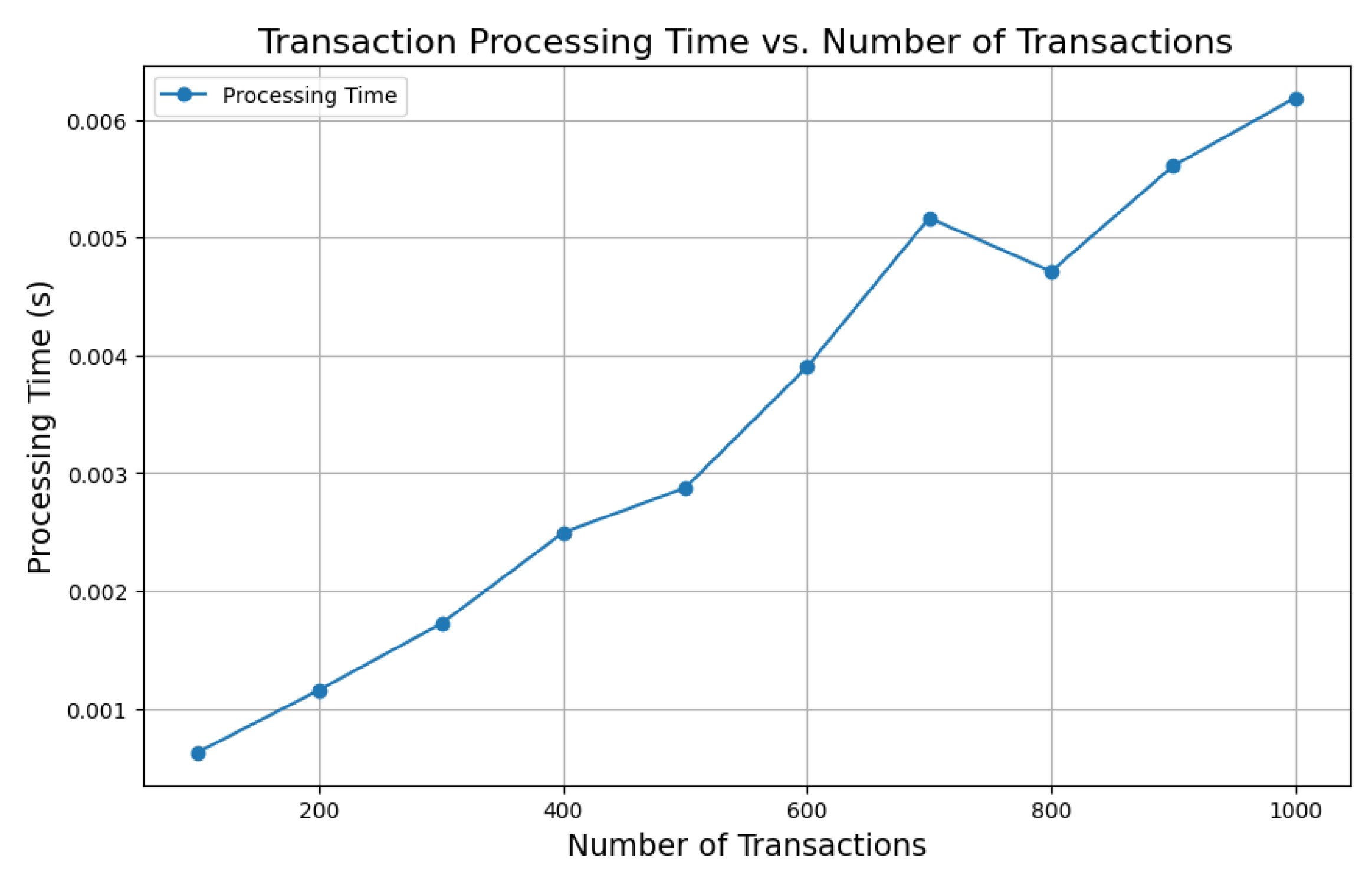
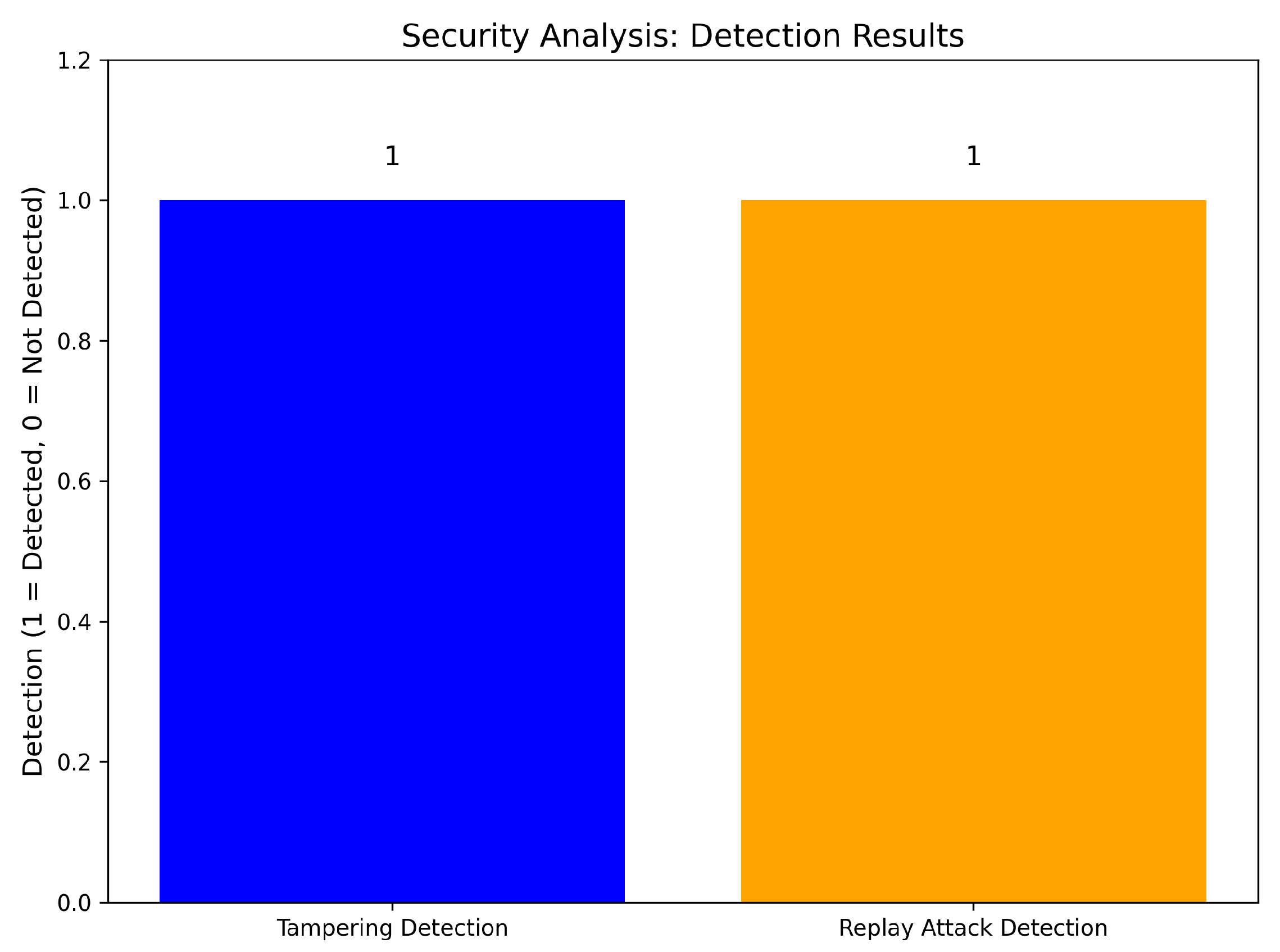
When evaluated from a security perspective, the framework demonstrated powerful protection capabilities against tampering and replay attacks. The system successfully implemented tampering detection because blockchain immutability ensures that the system alerts immediately when anyone tries to adjust stored data. The system is resilient against replay attacks through duplicate detection, which is enabled by timestamp validation and transaction data checking. In addition, the cryptographic framework provides strong defenses. IoT-enabled healthcare systems require these security measures to ensure patient data remain both trustworthy and intact. The framework’s scalability properties emerged from tests measuring blockchain size and transaction processing time across varying transaction volume levels. System performance maintained a linear growth pattern, as demonstrated by processing time, which went from 0.001 s for 200 transactions to 0.006 s for 1000 transactions. The blockchain exhibited proportional growth relative to transaction volume, illustrating effective storage use through modular block structure and combined transaction handling. The experimental results demonstrate that the system framework can process additional workloads without sacrificing performance predictability.
The framework shows multiple limitations, although it demonstrates significant strengths. Blockchain storage must expand proportionally, creating deployment obstacles in environments with limited resources over extended periods. The PoA consensus mechanism depends on pre-approved validators, which creates centralization risks and single points of failure. The high initial costs required to implement IoT healthcare systems connected through blockchain technology create financial barriers that restrict its adoption across various scenarios. Future enhancements serve as solutions to resolve these existing limitations. The implementation of data-pruning techniques together with off-chain storage solutions has the potential to reduce blockchain storage demands and maintain data integrity. A combination of Proof-of-Authority and Proof-of-Stake consensus models minimizes centralization threats while maintaining system efficiency. When edge computing frameworks are incorporated into IoT systems, they optimize data preprocessing operations while reducing latency, helping achieve scalability for extensive IoT networks. The consensus mechanism’s resistance to failures would strengthen through dynamic validator assignment, which evaluates trust scores alongside performance indicators.
The proposed framework successfully resolves essential challenges faced by IoT-enabled Internet hospitals through scalability, security, and real-time performance solutions. By integrating blockchain technology, anomaly detection mechanisms, and advanced cryptographic techniques, the framework delivers robust efficiency for IoT-based healthcare systems. After further development, the technology will establish itself as an essential base for secure healthcare applications that perform efficiently on large networks and devices with limited resources. The blockchain-enabled governance system shows the capability for expanding healthcare applications within smart cities beyond healthcare into applications dedicated to energy grids and public safety systems. The framework has built-in abilities to securely protect real-time data streams while looking for anomalies, resulting in more reliable power distribution networks that resist tampering and cyberattacks. Public safety systems benefit from robust data integrity mechanisms and fault tolerance features of the framework, which enables secure emergency response coordination alongside critical information exchange. The framework supports smart city sustainability goals by implementing PoA consensus, which minimizes resource usage below traditional blockchain designs. The framework minimizes computing costs with efficient scalability, resolving healthcare problems while providing a sustainable base for more extended applications in smart cities. The framework demonstrates flexible applications, which place it as a potential universal solution for multiple urban domains, thus bolstering smart city resilience and operational efficiency.
Although the assumptions (see
Section 6) enable a controlled evaluation focusing on performance metrics, it is accepted that simulations abstract some aspects of reality by their nature. Take, for example, the automation of anomaly detection using the Isolation Forest technique and validation logic incorporated in the blockchain. All these were tuned to work under certain stable assumptions. Therefore, the assessment set would not capture noisy real-world factors such as hardware bottlenecks causing delays in block confirmations, bursts of noise, or intermittent anomalies. These constraints will be addressed by expanding the evaluation for more sophisticated system designs in the later stages of the project using controlled models of noise injection, adaptive thresholds, and variable-node behavior driven by actual data for fault injection to further assess the claim of the system resilience and general applicability.
As with any practical deployment, the proposed framework will face infrastructure cost and governance challenges. Implementing IoT-enabled Internet hospitals requires deploying edge devices, such as private blockchain nodes and secure gateways, with considerable initial capital investment and ongoing operational costs. Additionally, while PoA offers efficiency and speed, the underlying trust of the mechanism is bound to a few predetermined validators, which creates a centralization risk. Any compromise or collusion among these validators would put data integrity at risk. All of these challenges must be dealt with in the context of proper stakeholder governance, dynamic validator sharding, and tailored cost-benefit analysis relative to the scale and available resources of the healthcare provider.
The proposed framework takes on critical gaps identified in prior research, compared with the approaches discussed in
Section 2. For instance, Mazhar et al. [
3] and Singh et al. [
22] did implement secure system frameworks; however, real-time anomaly detection was either absent or burdened with centralization issues due to the use of PoW/PoS consensus models. The proposed framework employs Isolation Forest for real-time anomaly detection and uses PoA consensus for speedy, energy-efficient transaction validation specific to permissioned healthcare networks. Moreover, Pimple et al. [
23] and Salunkhe et al. [
27] focused on security features but suffered from cross-domain integration and scalability problems. With our modular architecture enabling batch processing and role-based access control, these problems can be mitigated, resulting in improved throughput and reduced latency, as shown by our experiments. Furthermore, our system does not suffer from reliance on off-chain storage and third-party identity confirmation as many other systems do. Our approach features secure on-chain encrypted flagging and anomaly detection without performance trade-offs or violations of privacy and system trust.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}