Abstract
This study presents an alternative process for designing and manufacturing customized trays for dental-whitening treatments. The process is based on a digitized approach consisting of three main stages: design of a reference model, its manufacturing by AM, and thermoforming of the tray. The aim of the study was to develop a high-performance tray, able to guarantee comfort, safety, and efficacy for whitening treatments. To evaluate the patient’s experience, some tests under real operating conditions were performed. Twenty people carried out a nighttime treatment of 14 days. Each patient was asked to assess the overall level of satisfaction and the comfort of the tray and its ability to retain the gel. Tooth whitening was also determined according to the VITAPAN scale. All patients involved in the study were satisfied and provided positive feedback about comfort and tightness of the tray. At the end of the treatment, 15 out of 20 patients achieved shade A1 on the VITAPAN scale. The mean improvement in color shades was about 7. These results confirmed the great potential of the proposed dental tray. Its use was proven to guarantee a high level of quality, flexibility, and customization of dental-whitening treatments, improving comfort, safety, and efficacy.
1. Introduction
Dental-whitening treatments became popular in the late 1990s [1]. They have become increasingly successful as people wish to have attractive smiles and whiter teeth. Therefore, whitening treatments are now very widespread and common [2]. Consequently, increased demand for the treatments has fostered the use of dental-whitening products and procedures. The main categories of whitening products include toothpastes, gels, and strips. Typically, whitening toothpastes consist of common toothpastes including abrasive particles characterized by a greater hardness or even by the same hardness but in higher concentrations. Differently, gels and strips are mainly based on hydrogen- or carbamide-peroxide agents. According to the concentration of these whitening agents, the treatments can be classified as at-home or in-office. Treatments are of the first type when the whitening product includes up to 6% hydrogen peroxide and up to 16% carbamide peroxide. In the case of a higher concentration of these agents, the treatments are classified as in-office and must be performed under professional supervision [3]. At-home treatments are gaining popularity since they are easy enough for the patient to perform at home. Although whitening gels based on a low concentration of peroxide agents are well-established and considered quite safe and effective, some side effects still need to be considered. The main and most common effects reported by the patients are increased tooth sensitivity and gingival irritation.
Tooth sensitivity is considered by patients to be the least annoying of the two. In general, it is correlated to the characteristics of the teeth and the type of whitening gel. Since contact of the gel with the tooth is inevitable during the treatment, the solution to this problem is to stop the treatment for a few days [4]. The second side effect is due to the contact of the gel with the soft tissues of the gum. This is unnecessary and should be avoided or at least minimized by shielding the gingiva and tongue [5]. This problem can be related to the type of tray that is used for containing the whitening gel and/or to the amount of gel used to fill the tray. Dental trays that are accurately and properly designed and produced may protect the soft tissues of the gingiva and tongue, and may consequently prevent the swallowing of amounts of the gel or water used to rinse the gel residues. There are two types of tray: non-customized and customized. Non-customized trays have shapes that fit all or specific sizes of dental arches. They are generally flexible and made of materials such as silicone. On the one hand, they are simple and low-cost products, but on the other hand, they are not always comfortable and cause gel leakage, given their generic form. Customized trays are individually designed for a specific patient. Therefore, they are comfortable as they fit perfectly on the arch, and hold the gel inside more effectively. In addition, they also allow the deposition of the whitening gel exactly where it is needed [6]. Literature reports that customized trays allow for the creation and positioning of reservoirs where teeth whitening is required or desired [1]. Customized trays are typically handmade. A plaster of the patient’s dentition is modified manually to create reservoirs, spacers, and scalloping. Subsequently, the modified plaster is used for thermoforming a thermoplastic disc [7,8]. This procedure has a notable production time. Furthermore, the precision and the control of the details of the tray is highly dependent on the dexterity of the operator. A digital approach could provide an advantage in terms of timing, precision, control, and flexibility of the process. In fact, if the patient has discomfort it is possible to modify the tray more easily than recreating the plaster. Moreover, all the models are stored in a digital format and can be retrieved, in case of necessity, and furtherly customized if needed.
The work presented in this paper was developed in collaboration with AirNivol®, an Italian company that designs and manufactures invisible orthodontic aligners. The process presented is fully digital and includes automatized activities. The approach proposed is based on the concept of Dentistry 4.0 and combines esthetic dentistry, 3D intraoral scanning, computer-aided design, additive manufacturing, and dental engineering. The main objective of the presented work was to increase the trays’ quality, flexibility, safety, efficacy, and level of customization. In addition, the study also aimed to produce better-performing trays, which ensure comfort through a perfect fitting and protect the gingiva using reservoirs properly modelled in the tray. In order to evaluate their performance, the customized trays were tested by 20 patients who performed the whitening treatment using a carbamide-peroxide gel. A protocol was defined and used to collect data about the treatments. Subsequent analysis of the collected data was carried out to evaluate the quality and effectiveness of the trays.
2. Materials and Methods
2.1. Design and Manufacturing of the Trays
The digital process for the production of the customized dental trays consists of three main phases: the design of the reference model of the tray, the manufacturing of the reference model using 3D printing technology, and the final production of the tray obtained through a thermoforming process (Figure 1).
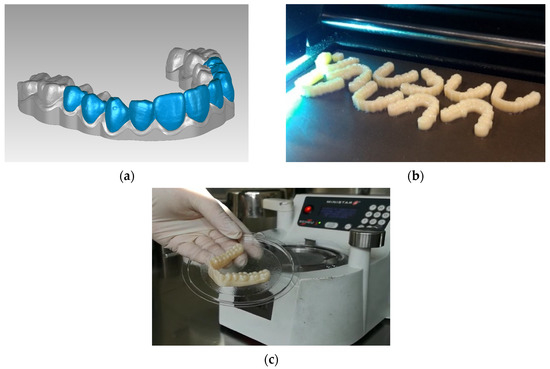
Figure 1.
Phases of the digital process for the production of the customized dental trays: design of the reference model (a), 3D printing of the reference model (b), and thermoforming of the dental tray (c).
The production of customized trays consists of designing the reference model that is manufactured and used for thermoforming the trays. The design activity includes five main steps that are described below (Figure 2).
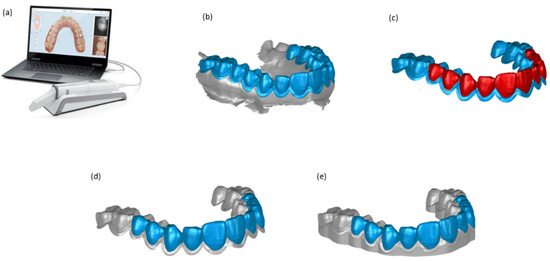
Figure 2.
The five steps of the digital process for generating the reference model of a tray: 3D scanning (a), tray area selection (b), whitening area selection (c), offset creation for reservoirs (d), creation of the final STL file (e).
The first step consists of the intraoral scanning of the patient’s dentition. This is a procedure that is used by an increasing number of dentists for digitally capturing visible intraoral surfaces. 3D optical dental scanners are typically used for performing this task. For the present study, a TRIOS 3 Basic intraoral scanning supplied by 3Shape© was used. The result obtained after the scanning process is a 3D model in form of polygonal mesh representing the shape of the patient’s teeth and gums (Figure 2a).
The acquired model is then treated with MeshLab, a software for processing and editing polygonal meshes, in order to create the reference model to be used for the forming stage. By using a manual tool of the software, the operator selects and deletes the portion of the gum acquired by the optical scanner that is not needed for the reference model (Figure 2b). A small area all around the gingival margin is left to protect the gum and also at prevent leaking of the whitening gel.
The third step consists of selecting the area of the teeth to whiten (Figure 2c). Typically, whitening treatments are performed on the frontal teeth, which are those visible when talking and smiling.
Subsequently, an offset of 0.2 mm is applied to this area on the mesh (Figure 2d). When the offset is applied, the selected area moves outwards by a distance of 0.2 mm, normal to each mesh facet. This creates an empty volume corresponding to the reservoirs, which will be filled with the gel. The value selected for the offset is the result of preliminary studies and tests that we carried out on a variety of trays. In this way, the reservoirs of the whitening gel are generated exactly in the positions required. Figure 3 shows a schematic section of the tray with the reservoir on a tooth.
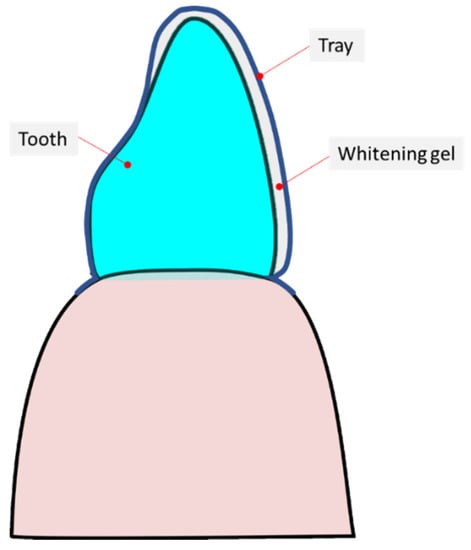
Figure 3.
Schematic of the tray when it is worn and is on the tooth.
In the last step, the boundary of the obtained model is extruded and the bottom is closed (Figure 2e). Through the extrusion, the 3D sketch of the boundary is stretched and vertical walls are created. Finally, the bottom is closed to build a closed volume and it is saved as an STL file. This file is necessary for the next phase of the process and for manufacturing the reference model of the custom dental tray. As can be seen from the images in Figure 2, the teeth selected for inserting the reservoirs are those from 11 to 15 and from 21 to 25 for the maxillary arch, and from 41 to 45 and from 31 to 35 for the mandibular arch (FDI nomenclature). In particular, the vestibular zones of the teeth are fully selected and their palatal zone are only partially selected. The reason for this is that only the teeth that are visible when talking or smiling are whitened. Therefore the gel is applied on these teeth, and not on all teeth. This optimizes the use of the gel and reduces the side effects associated with unwanted leakages. The tray can be furtherly customized depending on the characteristics of the patient’s dentition and the reservoirs can be positioned in correspondence with the teeth, or portions of them, according to the needs.
The reference model is produced using additive manufacturing technology. In particular, a Stratasys Objet J700-Dental machine is used. This is a 3D printing machine, based on material jetting technology. Material jetting (MJ) is a process that creates 3D geometries by line-wise dispensing of a photopolymer from hundreds of tiny nozzles placed on a printing head, which moves along directions parallel to the build platform. The droplets are directly cured and solidified as they are deposited on the build platform using one or more ultraviolet (UV) lamps [9]. The MJ process allows for multi-material 3D printing within the same part by simultaneously dispensing different materials, one of which is commonly employed to build supports and then removed with the post-processing step [10]. The reference model is produced using a water-soluble photo resin as supporting material and VeroDent™ photo resin (MED670™) as the material of the reference model. The latter is removed by a post-processing machine with a rotating basket and a cold-water jet. The result consists of the cleaned reference model ready to be used.
The tray is then thermoformed onto the 3D printed reference model using an LDPE (low-density polyethylene) disc supplied by Scheu Dental®, known under the trade name of Copyplast [11]. This material is characterized by an intermediate level of stiffness (elastic modulus = 175 MPa). In fact, its deformability is less than that of rubbery materials such as silicone, but it is not too rigid, to avoid discomfort when in contact with the soft tissues of the gums. The thermoforming process is performed, by using a Ministar S® machine supplied by Scheu-Dental®, according to the manufacturers’ recommendations for heating, pressure, and cooling time. After the thermoforming process, excess material must be removed. An operator manually removes the material that is below the gingival zone that was created in the design phase to protect the gum and prevent the whitening gel from leaking. When trimming operations are concluded, the tray is ready to be worn by the patient (Figure 4).

Figure 4.
(a,b) show a tray manufactured from different points of view. The small portion of the gingival margin, aimed at protecting the gum and also at preventing the leaking of the whitening gel is clearly visible.
2.2. Evaluation of the Dental Trays
Some tests under real operating conditions were performed. The aim was to evaluate the performances of the trays produced using the proposed digital process concerning the patients’ experience and also concerning the effectiveness of their usage for whitening the teeth. The dental trays were tested by 20 people, 11 male and 9 female, aged between 18 and 60 years. Informed consent was obtained before their inclusion in the evaluation. Any detail that could disclose the identity of an individual participant was omitted. For each participant, an at-home treatment was carried out under the supervision of a dental practitioner, according to the DIRECTIVE 2011/84/EU [12]. As a first step, a clinical examination was performed to ensure that there were no risk factors or other oral conditions of concern. In addition, it was checked that the patient could be exposed to the whitening agents, as intended, in terms of frequency and duration. Each participant carried out a nighttime whitening treatment based on a commercial 10% carbamide peroxide gel (OpalescenceTM PF10) for 14 days. About 0.3 mL of gel per arch and per night was used. The patients were asked to distribute the whitening gel on the upper and lower arch trays. Each patient was asked to fill out a daily report and to answer a final questionnaire, aimed at assessing the overall level of satisfaction associated with the treatment, the level of comfort of the trays, and their ability to retain the gel. At the end of each treatment, the dentist evaluated the quality of the dental whitening obtained and the variation between the initial and final colors. For the evaluation, 16 shades of the VITA classical A1-D4 color scale were reorganized from the lightest (B1) to the darkest (C4) color value. For each patient, the shade values of the middle third of the central incisor were detected, as suggested by the American Dental Association’s guidelines, and recorded using intraoral open and closed mouth photos. All photos were taken in daylight and under the same settings and environmental conditions [13,14].
3. Results
This section summarizes the results reported from the patients’ answers to the questionnaires and the teeth shade values reported by the dentist. All analysed data have been treated anonymously.
Figure 5 reports some results concerning the level of comfort of the trays reported by the patients and the overall level of satisfaction associated with the treatment based on their use.
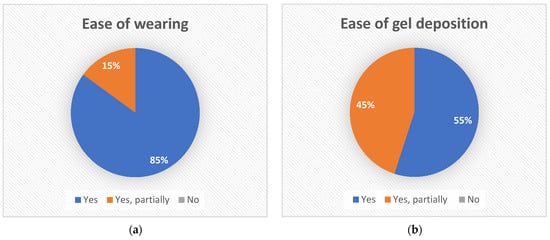
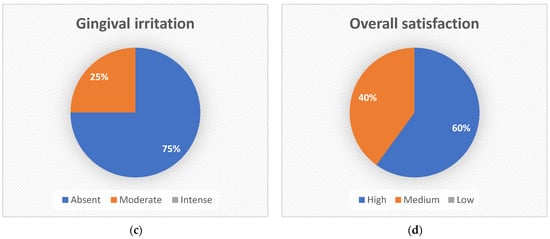
Figure 5.
Results of the evaluation of the tray and of the whitening treatment: ease of wearing (a), ease of gel deposition (b), gingival irritation (c), and overall level of satisfaction (d).
The first chart reports the patients’ experience concerning how easy it was donning and doffing the trays (Figure 5a). Seventeen out of 20 patients (85%) reported that the tray was easy to wear, the remaining three patients reported that it was somewhat easy. No patients reported difficulties.
The second question concerned the gel deposition (Figure 5b). Eleven out of 20 patients (55%) reported that the gel deposition was easy and 9 out of 20 that it was somewhat easy. No patients reported any difficulty.
Patients were also asked if they suffered gingival irritation during treatment for even one day (Figure 5c). Seventy-five percent of the patients did not report any gingival irritation, 25% reported a moderate irritation, and none reported an intense irritation. It should be noted that those patients who reported moderate irritation, suffered from it for just one or a few days during the treatment.
Finally, the overall level of satisfaction associated with the treatment and with the use of the custom dental tray was evaluated (Figure 5d). All patients were satisfied with the treatment. Twelve out of 20 patients reported a high level of satisfaction, the remaining eight a medium level, and none was not satisfied.
The 20 patients participating in the evaluation were also asked to report any leak of the whitening gel for each day of treatment. Only five patients reported moderate gel leak. Two patients reported it happened only two out of 14 days of treatment, and three patients for only one day. To be more specific, all five patients reported that the leak occurred on the first day of treatment. We can speculate that this was probably due to the use of an excessive amount of gel and the need for some patients to practice using and depositing the gel in the trays. Table 1 shows the results of the daily report referring to gingival irritation and gel leakage for all 14 days of the treatment. The 20 patients were treated anonymously and ranged from P1 to P20. Gingival irritation was also reported by only five patients and for a maximum of three of the 14 days of treatment.

Table 1.
Daily report referring to gel leakage and gingival irritation for all 14 days of the treatment duration, for all 20 patients in the evaluation.
Dental whitening was obtained for all the patients at the end of the treatment. The color variations were evaluated and are reported in Figure 6. Seventy-five percent of the patients, i.e., 15 out of 20, reached A1 color, which is the second lightest shade on the VITAPAN scale; two patients reached A2 color, and the remaining three reached A3 color (Figure 6a).
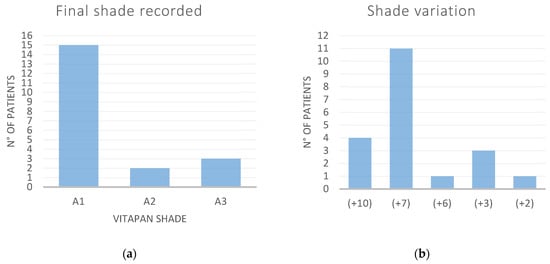
Figure 6.
Results of dental-whitening treatments recorded for the 20 patients participating in the study: final shade recorded (a) and shade variation (b).
Figure 6b reports the shade variation calculated as the difference between the shades recorded before and after the treatment, according to the sequence, with numerical equivalents, shown in the figure. In most patients (15) the color of the teeth improved by 7 or 10 grades, in one patient by 6 grades, in three, by 3 grades, and in only one patient, by 2 grades. The average shade improvement recorded at the end of the treatment was 6.7.
An additional analysis of the collected data is reported in Figure 7, where the graph correlates the shade variations and the treatment hours reported by the patients, for all the patients that reached A1 color at the end of the treatment.
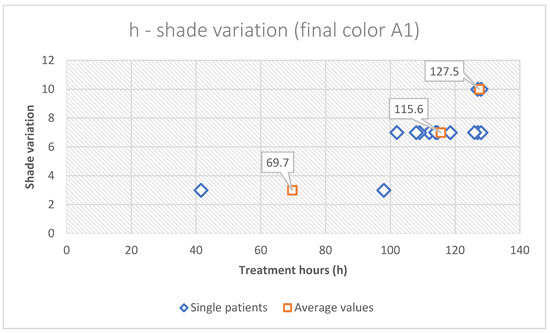
Figure 7.
Results correlating shade variation and treatment hours for all the 15 patients that concluded the whitening treatment with A1 shade. The average values of the hours of treatment, for each shade variation reached (3, 7, and 10), are reported (orange squares).
It is possible to estimate that to reach A1 color, a treatment duration of about 115 h corresponded to a shade variation of 7 grades (from A3 to A1 shade) in the reordered VITAPAN scale. Therefore, this suggests that optimal results can be obtained using the trays for an average time of 8 h per night for 14 days.
4. Discussion
For dental-whitening treatments, custom trays have great potential to guarantee a perfect fitting on the patients’ dentition, to protect the gums, and to improve comfort levels and personalize whitening by applying the gel where necessary. However, the process of designing and manufacturing custom trays is not always easy and is still manual and artisanal.
The study presented in the paper proposes a digital process for designing and manufacturing custom trays for dental-whitening treatments. Forty custom trays, considering the two arches of the 20 patients participating in the study, were designed, manufactured, and tested by the patients. The results of the tests were generally very positive for all treatments. The trays were considered easy to wear for almost all patients (85%) and none reported difficulties in donning and doffing them.
Gingival irritation was also evaluated. This aspect was monitored and evaluated carefully because it is one of the major indications of discomfort caused by the whitening treatments. The results showed that for 75% of the patients gingival irritation was absent and that for the remaining 25%, the irritation was mild. None suffered from intense irritation. Furthermore, of this 25% only one patient suffered from gingival irritation for three days, three for two days, and one for a single day out of the total 14 days of the treatment.
Since one of the main objectives of the study was to verify the general patients’ experience in the use of the trays, the patients were also asked to report the easiness of the gel deposition into the trays. Fifty-five percent of them said that it was easy, and 45% said it was somewhat easy. This result is less positive than the previous ones reported. However, no one rated the gel deposition as highly difficult.
Furthermore, another aspect that was considered important in assessing the quality of the tray was the gel leak while using the tray. Five patients reported leaks of the gel, but for all of them this was on the first day of treatment. It should be highlighted that this could be associated with the use of an excessive quantity of the whitening gel and with the need of some patients to practice using and dispensing the gel in the tray. In fact, no patient reported leaking gel during the night use, but all did it while donning the tray on their teeth, immediately after filling it with the whitening gel.
The overall level of satisfaction of the patients was also reported; 60% were fully satisfied, 40% reported a medium level of satisfaction, and no one declared to be unsatisfied at all. It should be noted that all patients who reported a medium level of overall satisfaction, also reported partial difficulty in depositing the whitening gel. This aspect could be linked to the method of dispensing the gel through the use of a syringe, rather than to the characteristics of the tray. The deposition of the gel, therefore, may have had an impact on the evaluation of the overall level of the patients’ satisfaction.
Finally, although the main objectives of the presented study were the evaluation of the level of comfort of the tray, its fitting on patients’ dentition, and its ability to retain the gel, dental whitening was also evaluated. For this purpose, a commercial 10% carbamide peroxide gel was used for 14 days. Seventy-five percent of the patients, after a nighttime whitening treatment lasting for 14 days, reached the A1 shade, and most of them improved their shade of 7 or 10 grades. In particular, the results showed that to reach the color-shade A1, a treatment duration of approximately 115 h gives shade variation of 7 grades (from shade A3 to A1) in the reordered VITAPAN scale. This result is to be considered positive if compared to previous studies. In [15], for example, a two-week whitening treatment based on a 10% carbamide peroxide gel and bleaching trays was carried out by 20 patients (18–56 years) and the mean shade variation was about of 5 grades. In [16], instead, the shade variation was measured after three weeks of a nighttime treatment based on the gel OpalescenceTM PF10 (i.e., the same used in our study) and a custom-fitted soft plastic nightguard. At the end of the treatment, only 50% of the patients showed a variation of 4 grades.
Furthermore, it is worth noting that previous studies have shown that dental bleaching depends on a large number of factors, such as the type of gel used, the concentration of the bleaching agent, the characteristics and age of the patients, and the type and duration of the treatment [17,18,19]. For these reasons, the results for dental whitening are to be considered highly specific and they cannot be extended to any type of condition.
However, the best whitening results obtained in the presented study, compared to previous ones [15,16], would suggest that the developed custom tray, through the proper holding of the gel in place on the surface of the teeth, guarantees the efficacy of the whitening treatment as well as ensuring excellent comfort.
5. Conclusions
The paper describes the development of an alternative process to design and manufacture customized trays for dental-whitening treatments. The process, based on the concept of Dentistry 4.0, is fully digital and includes automatized activities.
The results conducted on 20 patients, under the supervision of a dental practitioner, showed that the procedure described in this work is promising. The customized dental whitening trays show a great potential in terms of quality, flexibility, and level of customization of the treatments. The high rating obtained from the questionnaires about comfort, safety, and efficacy are also encouraging. Nevertheless, in our future work, we will increase the number of patients, by including an additional group of participants to compare the results of our approach with conventional whitening treatments.
Other future studies will concern the use of the trays produced using the developed digital process for in-office treatments based on more aggressive whitening gels, and the development of a method to distribute the gel inside the tray in a more comfortable and easy way.
Author Contributions
Conceptualization, F.T., B.A., A.V.R., S.B. and M.B.; methodology, F.T., B.A., A.V.R., S.B., M.M. and M.B.; software, F.T., B.A. and A.V.R.; validation, F.T., B.A., A.V.R., S.B., M.M. and M.B.; investigation, F.T., B.A., A.V.R., S.B., M.M. and M.B.; resources, A.V.R., S.B. and M.B.; data curation, F.T., B.A., A.V.R., S.B., M.M. and M.B.; writing—original draft preparation, F.T., B.A. and M.B.; writing—review and editing, F.T., B.A., A.V.R., S.B., M.M. and M.B.; project administration, A.V.R., S.B. and M.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Carey, C.M. Tooth whitening: What we now know. J. Evid.-Based Dent. Pract. 2014, 14, 70–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haywood, V.B.; Sword, R.J. Tray bleaching status and insights. J. Esthet. Restor. Dent. 2021, 33, 27–38. [Google Scholar] [CrossRef] [PubMed]
- Knezović Zlatarić, D.; Žagar, M.; Illeš, D. A clinical study assessing the short-term efficacy of combined in-office/at-home whitening treatment. J. Esthet. Restor. Dent. 2019, 31, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Alkahtani, R.; Stone, S.; German, M.; Waterhouse, P. A review on dental whitening. J. Dent. 2020, 100, 103423. [Google Scholar] [CrossRef] [PubMed]
- Epple, M.; Meyer, F.; Enax, J. A critical review of modern concepts for teeth whitening. Dent. J. 2019, 7, 79. [Google Scholar] [CrossRef] [Green Version]
- ADA Council on Scientific Affairs Tooth whitening/bleaching: Treatment considerations for dentists and their patients. Am. Dent. Assoc. 2009, 9. Available online: http://www.bamatis.com/docs/HOD_whitening_rpt.pdf (accessed on 20 June 2022).
- Sibilla, P.; Cogo, E.; Turrini, R.; Calura, G.; Fradeani, M. The timing and operational management of the variables of bleaching in cases of rehabilitation in the esthetic field. Int. J. Esthet. Dent. 2014, 9, 436–445. [Google Scholar]
- Cogo, E.; Sibilla, P.; Turrini, R.; Marcuzzi, F.; Calura, G. Realizzare Le Mascherine per Gli Sbiancamenti Domiciliari: La Tecnica MO.BI. Dent. Cadmos 2013, 81, 593–600. [Google Scholar] [CrossRef]
- Yap, Y.L.; Wang, C.; Sing, S.L.; Dikshit, V.; Yeong, W.Y.; Wei, J. Material jetting additive manufacturing: An experimental study using designed metrological benchmarks. Precis. Eng. 2017, 50, 275–285. [Google Scholar] [CrossRef]
- Tamburrino, F.; Barone, S.; Paoli, A.; Razionale, A.V. Post-processing treatments to enhance additively manufactured polymeric parts: A review. Virtual Phys. Prototyp. 2021, 16, 221–254. [Google Scholar] [CrossRef]
- Product Datasheet COPYPLAST ®; Scheu Dental GmbH: Iserlohn, Germany, 2016.
- Doménech, G. New european legislation on pharmacovigilance. Pharm. Policy Law 2011, 13, 7–27. [Google Scholar] [CrossRef]
- Oliverio, T.; Cremonini, F.; Lombardo, L.; Siciliani, G. Tooth whitening in association with clear aligner treatment. J. Clin. Orthod. 2019, 53, 508–517. [Google Scholar] [PubMed]
- Bersezio, C.; Martín, J.; Angel, P.; Bottner, J.; Godoy, I.; Avalos, F.; Fernández, E. Teeth whitening with 6% hydrogen peroxide and its impact on quality of life: 2 years of follow-up. Odontology 2019, 107, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Morgan, S.; Jum’Ah, A.A.; Brunton, P. Assessment of efficacy and post-bleaching sensitivity of home bleaching using 10% carbamide peroxide in extended and non-extended bleaching trays. Br. Dent. J. 2015, 218, 579–582. [Google Scholar] [CrossRef] [PubMed]
- Medeiros, M.C.D.S.; de Lima, K.C. Effectiveness of nightguard vital bleaching with 10% carbamide peroxide-A clinical study. J. Can. Dent. Assoc. 2008, 74, 163. [Google Scholar]
- Mohan, N.; Westland, S.; Brunton, P.; Ellwood, R.; Pretty, I.A.; Luo, W. A clinical study to evaluate the efficacy of a novel tray based tooth whitening system. J. Dent. 2008, 36, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Haywood, V.B. Treating sensitivity during tooth whitening. Compend. Contin. Educ. Dent. 2005, 26, 11–20. [Google Scholar] [PubMed]
- Majeed, A.; Farooq, I.; Grobler, S.R.; Rossouw, R.J. Tooth-bleaching: A review of the efficacy and adverse effects of various tooth whitening products. J. Coll. Physicians Surg. Pak. 2015, 25, 891–896. [Google Scholar] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).