Abstract
Informal caregivers play a fundamental role in caring for people that need assistance and provide an effective service in managing their loved ones’ health. Because of this, they have little time to attend to themselves and perform self-care practices. Some of these practices can improve mental health. By snowball sampling, we recruited 15 informal caregivers, 12 females and three males. Using the Wilcoxon signed-rank test, we analyzed the impact of the reminders on a self-care scale. We used the Mindful Self-Care Scale, comparing the same population without reminders and with reminders. Results indicated that total self-care scores with reminders increased statistically significantly, T = 13, Z = −2.481, p ≤ 0.013, with a large effect size (r = 0.64). This study shows a significant self-care increase in informal caregivers after using reminders. Future development of a reminders-based approach could focus on increasing self-care and the time caregivers take for themselves, empowering them to take a more active role in meeting their own needs.
1. Introduction
As our population ages, the need for support from others increases. In addition, longer life expectancy due to advances in healthcare leads to a rise in chronic diseases and a higher number of dependent people. Support needs include managing diseases [1] like dementia, where people have difficulties carrying out the activities of daily living [2]. Most of the time, a family member is in charge of the care. These caregivers are referred to as informal caregivers since they are not paid for their work and frequently lack the necessary skills and knowledge to provide care [3,4].
Informal caregivers help with a wide range of tasks, including treating physical and emotional needs, managing medications, and keeping track of medical appointments [5]. Informal care represents a role and a responsibility that is added on to other roles and responsibilities such as work. Out of people who combine work with informal care, some need care and support of their own because they suffer in terms of personal well-being, such as having high stress and functioning problems due to their involvement in informal care [6,7,8].
In addition, informal caregivers, especially those who care for people with dementia, often lack formal training or relevant work experience and awareness of available resources to assist them in caring for their family members [9]. This lack of training highlights the importance of developing interventions to meet the needs of informal caregivers who want to provide adequate and appropriate care [10]. Due to these facts, most informal caregivers are not confident in their care, directly affecting the caregiver burden level [11]. High-level confidence positively impacts informal caregivers’ lives, considering that an informal caregiver can have more favorable responses, such as perceptions of their ability to meet and cope with caregiving demands. This confidence decreases informal caregivers’ stress, enhancing their overall health, which is important [12], considering that high requirements of informal caregiving often lead to a high rate of physical, mental, and social health decline [13]. Previous research has found that the stressful experience of caring for a family member significantly affects physical and mental health [14]. Somatic symptoms, depression, anxiety, loneliness, stress, and occupational and socio-economic challenges contribute to informal caregivers’ lower quality of life [5].
These informal caregiver requirements have been investigated. The health of informal caregivers, particularly mental health, time demands, difficulties in managing multiple medications and their side effects, having to coordinate different health professionals, dealing with the emotional burden, lack of leisure time, impact on social relationships, lack of information and knowledge about the illness and treatment, and difficulties in accessing resources to support caregivers were among the most studied [15,16,17].
Informal caregivers play a fundamental role in caring for people that need assistance in health care and provide an effective service in managing their loved ones’ health. However, because of this, they have little time to attend to their own health [18]. This points out the importance of build-up interventions focusing on informal caregivers’ needs to minimize stress and promote well-being. Some strategies have been implemented to help reduce care’s negative consequences and improve caregivers’ quality of life. These measures include psychoeducational, psychotherapy, self-help, or multi-component therapies that provide disease or self-care knowledge, problem-solving strategies, communication skills, social support, or mindfulness [1,19,20,21,22].
However, these interventions are typically costly, unavailable to everyone, and informal caregivers do not have time for them [14,23]. Interventions that combine many activities to improve various outcomes, such as social support, psychological skills, and a healthy lifestyle, have also explained a decreasing burden and increased healthy lifestyle behaviors. These interventions show the importance of promoting and undertaking self-care, especially in the case of informal caregivers, as it is associated with positive physical health, emotional well-being, and mental health [24].
Self-care is broadly defined as the everyday process of being aware of and attending to one’s elementary physical and emotional needs through engaging in helpful behaviors, including shaping one’s daily routine, relationships, and the environment as needed to promote it [24]. Practicing frequently, maintains and enhances both short-term and long-term wellbeing holistically. According to a previous literature review, human-computer interaction (HCI) technologies can help informal caregivers by supporting them in caring for patients, especially when patients can no longer actively participate in their own care [25]. This support can be undertaken via relieving informal caregivers with auditory/video reminders for patients [26] or by making required information visible, allowing the caregiver to know when to act [27].
The role of reminders in improving certain self-care behaviors has been extensively studied, especially in the medical informatics community, as reminders have been used to help persons with dementia or with diabetes to remember to take their medicine [26,28]. However, no study was found using reminders to improve informal caregivers‘self-care practices directly. As reminders are elements that offer customization, as they may contribute to improving these practices. Therefore, we must consider using reminders that can be easily incorporated into one’s life. Beyond the barrier of factors that may deter someone from taking care of their physical and physiological well-being. It is important to increase individual self-care by meeting these needs proactively and regularly, as high requirements of caregiving often lead to a high rate of physical, mental, and social health impact [13].
With the technology currently available, there is a potential for customization and prompting; alerts and reminders are more effective than providing static content as they adapt to a participant’s context and usage [29]. Generally, setting up reminders makes sense, as we cannot remember everything. In addition, offloading some of our obligations to a device can free up mental space for other tasks.
When deciding whether we want to schedule or receive reminders, we have to weigh the benefits of remembering against the costs of feeling distracted, annoyed, and guilty. Even positive reminders cause a context switching of our attention, as reminders bring us into a different state of mind. Perhaps waking up to notifications that instantly put a person in a specific frame of mind can be a positive. Unfortunately, that can also be guilt, stress, or feeling overwhelmed [30]. Not only do we feel guilty about missing out on important tasks, meetings, and events, but that feeling of guilt pulls us away from what we are currently focusing on. Damgaard et al. [31] report that we are not just overwhelmed and distracted by reminders. If there are too many, the sheer number of them means we are more likely to miss the ones we do want to pay attention to. Damgaard et al. [32] also report that although many participants state that they are delighted to get a reminder, there is a risk of hostility from a significant percentage of individuals who feel strongly or extremely negatively about reminders. Those who were bothered by the reminder cited the following reasons: it was too early in the morning, they were waiting for other important results, they were contacted at work, they felt they were being treated as senile, or they thought the reminder was unnecessary; however, for others, the reminder came at a good time and helped them remember; and for others, the reminder came at a good time and helped them remember, others felt annoyed with the frequency or did not see enough value in being reminded every month and maybe even guilty doing as suggested.
Unfortunately, there is no perfect frequency at which to send a reminder. Each receiver has an individual tolerance level. Fortunately, as long as the reminders are set up by the user and remain customizable, this timing issue can at least be minimized. Even though these negative effects of reminders are relative to the general population, they may affect the informal caregiver burden.
This study investigates differences in informal caregivers’ total mindful self-care scores between those without and with reminders as a personalized technology. It was hypothesized that reminders succeed in increasing the frequency of general self-care practices in the informal caregivers’ population.
2. Methods
2.1. Sample
This study is targeted at informal caregivers who meet the following criteria: are of at least 18 years of age, are cognitively competent, and who provide daily assistance to their family member that need help, where they do not need to perform a minimum number of hours as informal caregivers and do not have to have a specific type of family relationship to qualify for the study. In addition, they need to have access to their mobile device, and it has to have a reminder feature capability. Formal caregivers (professional caregivers) were excluded from this study, as our target was informal caregivers, and uncorrectable hearing or vision impairments prevented study participation. The study coordinator screened participants for these criteria before consent.
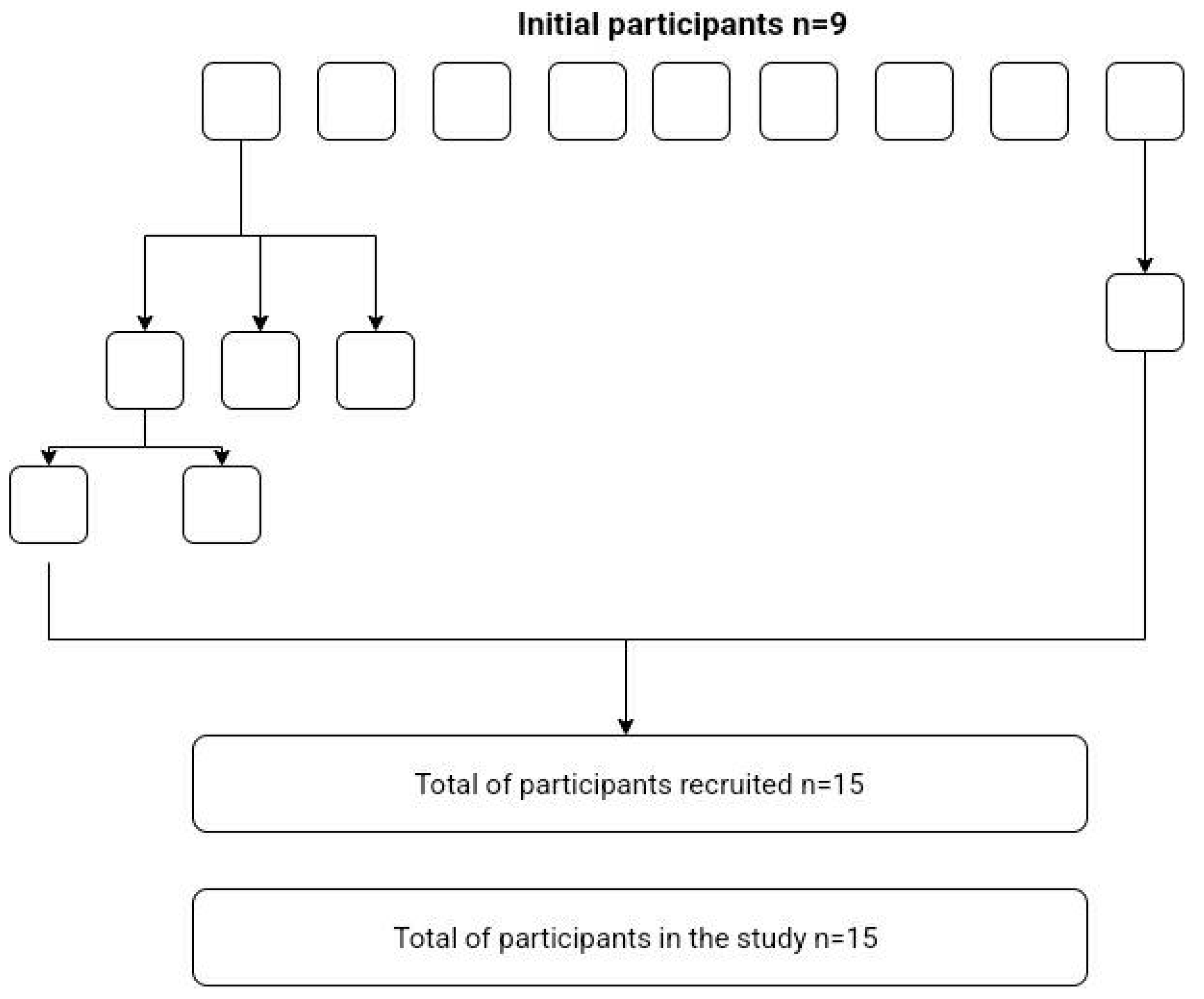
Participants were recruited using the snowball method, starting with the closest family members and friends. Snowball sampling is one method of sampling in qualitative research where researchers usually start with a small number of initial contacts (seeds) who fulfill the study’s requirements and are invited to join. The willing participants are then asked to indicate other people who fulfill the research criteria and might be willing volunteers, who in turn recommend more people, and so on [33]. The initial group of recruited participants was nine; some of these initial participants recruited four additional participants, and additionally, one of these participants recruited more two participants. With this, we recruited a total of 15 participants for the study, and all of the 15 participants agreed to participate. Figure 1 explains the process of recruiting participants.
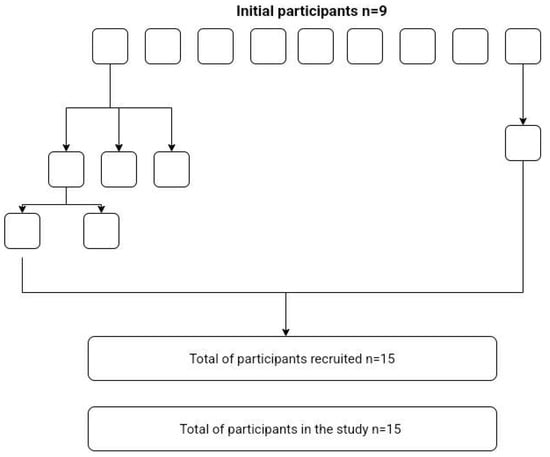
Figure 1.
Process of recruiting participants.
A total of 15 participants provided online consent, and all completed the study. Of the 15 participants, 12 (80%) were female, and the mean age was 58 years old (SD = 14). All of the informal caregivers cared for different individuals. Eleven (73%) informal caregiver participants combined work with caregiving. The mean years of being a caregiver was six years (SD = 4). Regarding having time for themselves, 12 participants (80%) reported having less time for themselves since they started caregiving, as their family members required much time in taking care of them and needed considerable attention. Table 1 has detailed information about the socio-demographic nature of the participants.

Table 1.
Socio-demographic data of participants.
2.2. Measurements
Informal caregiver data was collected through an online questionnaire, including demographic characteristics and the mindful self-care scale.
2.2.1. Socio-Demographic Characteristics
The information collected included the caregiver’s age, sex, time spent being a caregiver, and whether they spend less time on themselves since they started caregiving (yes/no).
2.2.2. Mindful Self-Care Scale
The Mindful Self-Care Scale (MSCS) by Cook-Cottone & Guyker [7] is a 33-item scale that measures the self-reported frequency of behaviors that measure self-care behavior. It helps to assess the areas of interventions that would improve self-care. The scale addresses six sub-domains of self-care: physical care, with eight-items; supportive relationships, with five-items; mindful awareness, with four-items; self-compassion and purpose, with six-items; mindful relaxation, with six-items; supportive structure, with four-items; and a part of these three general questions assessing the individual’s general practices of self-care.
The physical care sub-domain covers diet, hydration, and exercise habits. The supportive relationships sub-domain inquires if a person spends time with people who are good to them, if they feel supported, if they have someone who will listen, if they schedule time with supportive people, and if the people in their life respect their choices. The items related to specific practices such as meditation, mindful eating, and active practices of gratitude are assessed in the Mindful awareness sub-domain. Retained items assess a calm awareness of thoughts, feelings, and the physical body, as well as the careful and intentional selection of which thoughts and feelings are used by an individual to guide their actions. Acceptance of failure and challenge as part of the process, the ability to engage in supportive and comforting self-talk, permission to feel feelings, and an acknowledgment that failure and challenges are part of the human experience were among the items in the Self-compassion and purpose sub-domain. The items clustered together in the Mindful relaxation sub-domain represent specific activities that might assist an individual with relaxation, such as doing something creative or engaging the senses to relax. Items within the Supportive structure sub-domain deal with rest and environmental factors, including keeping work areas organized, maintaining a comfortable and pleasing living environment, striking a balance between others’ demands and one’s own needs, and keeping a manageable work schedule.
It uses a Likert-type scale (a rating of 1 to 5) to check the frequency of behavior (how much or how often) within the past week.
The scores of the Mindful Self-Care Scale’s (MSCS) items were used as dependent variables that measure the self-reported frequency of behaviors that subsequently measure self-care behavior. This self-care behavior will be tested without reminders and with reminders. The independent variable with reminders has alerts to informal caregivers so they do not forget to take time for themselves and to perform self-care practices.
For the Mindful Self-Care Scale [7], responses were recorded on a 5-point Likert scale which measured self-reported frequency with reminders and without reminders over the past week. The average mean of each sub-domain was calculated by using the formula: total/number of items in the sub-domain. The averages for each sub-domain were further added to get a total score of mindful self-care with and without reminders. This calculation methodology was used by applying Cook-Cottone and Guyker’s model.
2.3. Procedure
The management protocol for the informal caregivers was straightforward: we asked them to answer the questionnaires and to add a mobile phone reminder for two weeks. After that time, we asked them to complete the questionnaires again.
Therefore, in the experimental study, informal caregivers of people that need assistance were tested under two conditions—without reminders (baseline) and with reminders, using repeated measures in the same order. Participants first provided informed consent and were provided with information about the study. After they consented to participate, they began the study with the first questionnaire.
The first questionnaire, without reminders, was used as a baseline. Participants answered an online questionnaire about their self-care practices (MSCS) over the past seven days. Each section had separate clear instructions and participants were free to contact the researcher in case of queries and concerns. The respondents were thanked for their time and debriefed upon completing the form.
After this, participants were asked to add reminders on their mobile phones by saying a generalized phrase for “Do not forget to take time for yourself” for two weeks, considering that our goal was for the informal caregiver to increase their self-care by doing something that they enjoyed. This generalized phrase was the same for all participants. The timing of the was up to the participants so as to be convenient to them. Reminders were set for once every day for two weeks post-baseline. Data was collected after two weeks, yielding a total of two data collection time points.
At the end of the second week with reminders, participants were asked to complete a questionnaire about their self-care practice (MSCS), and also about the use of reminders over the past seven days. The questionnaires were only given to the participants after the second week to give them time to adapt the use of reminders.
Results were then calculated based on the scoring instructions given for each test. Statistical calculations were done using the Statistical Package for the Social Sciences (SPSS). The total score of the self-care scale was calculated and an overall relationship between self-care without reminders and with reminders was computed.
The SPSS Statistics 26 software was used for all statistical analyses. We used a Wilcoxon signed-rank, a non-parametric test because the level of measurement was ordinal, and we analyzed the differences between two conditions and used repeated measures. The results describe the self-care total score with and without reminders, as we were only interested in analyzing the results from the total score and not from each sub-domain as we wanted to conclude if, in general, the reminders had a significant effect.
All participants answered all of the questionnaires.
3. Results
Differences between Mindful Self-Care Scale Total Score with Reminders and without Reminders
The values obtained for the difference in the total score between the two conditions suggest a significant positive result, i.e., that there is a significant change in self-behavior scores with the addition of reminders. Table 2 shows the differences between the Mindful self-care total score without reminders and with reminders.
Table 2.
Differences between Mindful self-care scale total score without reminders and with reminders.
For the ranking of mindful self-care total scores, one caregiver showed no preference for either method, which was discarded from this analysis. The remaining 14 informal caregivers were rank-ordered by the size of their difference scores between conditions. A Wilcoxon test was used to evaluate these differences, indicating that they were statistically significant, T = 13, Z = −2.481, p ≤ 0.013, with a large effect size (r = 0.64). A significant increase was shown with reminders; the total of the ranks where informal caregivers favored the use of reminders was 92, and the total for those without reminders was 13.
4. Discussion
The main goal of this paper was to explore the differences in informal caregivers’ total mindful self-care scores without reminders versus with reminders. The hypothesis was considered for research, as there is a lack of previous literature that explicitly shows the relationship between the use of reminders and the frequency of self-care. In this study, the null hypothesis was rejected, suggesting a significant positive result between the use of reminders and self-care scores. It means that reminders help increase the frequency of general self-care practices in the population.
We surmised that self-care behavior changes were due to the reminder approach that guided this intervention. Throughout this, informal caregivers learned more about (1) self-reflection, which may have helped them to identify self-care behavior; (2) self-care—they were guided to be aware of their self-care practices and encouraged to perform these self-care behaviors; and (3) they were encouraged to be open to new approaches, such as reminders, and identified positive changes that may have occurred as a result of increasing their self-care behavior, and increased awareness about the time they spent on themselves. Self-care is associated with positive physical health, emotional well-being, and mental health [7].
These findings can be related to the potential of reminders to maintain self-care awareness and decrease the forgetting of appointments. It could be that, since informal caregivers are busy providing care to others and have little time of their own, remembering to take time for themselves becomes more difficult. Reminders prevent this from happening, allowing them to take a break from caregiving that depends on if it is possible for the informal caregiver to interrupt the current care service; however, reminders can help informal caregivers to take a break from informal caregivers, as are those who scheduled the reminders. Our study shows that adding reminders to caregivers’ mobile phones can be an important strategy for informal caregivers to manage their time, improving their self-care behavior.
5. Study Limitations
The study could not control for possible confounding variables such as personal factors and individual differences, like sex, that could have influenced their reporting of self-care scores. Since we used the snowball sampling method to recruit participants starting with the closest family members and friends, obtaining a diverse sample remained a challenge. Male caregivers were fewer than female caregivers, although we did try to increase their number. However, having more female caregivers than male caregivers can represent general caregiver demographics well, as studies find that informal caregivers tend to be primarily female [27]. Still, since there is no balance of sex, in this study, the conclusions may consider a limited generalized to the entire population, as the sex, may affect the overall total mindful self-care score, especially considering women seem to carry out personal-care tasks more often than men. Future research on the topic should integrate non-informal caregivers, such as a control group with and without reminders. This information would help clarify how non-informal caregivers would have responded to a similar exposition. In our sample, the MSCS length was not perceived as an issue, and there is no information available as to whether participants used their smartphones to answer the questions. More research is needed to clarify the best interactive design with MSCS. Another limitation was the sample size of this study. Future research may provide machine learning models of analysis to better estimate alternative key performance indicators.
6. Conclusions
The results of this study show that a two-week use of reminders improved self-care in informal caregivers. This result shows that reminders can be used to influence self-care practices regarding the improvement of the self-care of informal caregivers that might serve as a reminder to informal caregivers to engage in more self-care. The reminders approach could be designed to increase self-care and to encourage informal caregivers to take time for themselves, empowering them to take an active role in meeting their needs.
Author Contributions
Conceptualization, B.P. and P.F.C.; methodology, B.P. and P.F.C.; software, B.P.; validation, P.F.C. and É.R.G.; formal analysis, B.P. and É.R.G., investigation, B.P. and P.F.C.; resources, B.P.; data curation, B.P. and P.F.C.; writing—original draft preparation, B.P., writing—review and editing, P.F.C. and É.R.G.; visualization, B.P., P.F.C. and É.R.G.; supervision, P.F.C.; project administration, B.P.; funding acquisition, P.F.C. and É.R.G. All authors have read and agreed to the published version of the manuscript.
Funding
B.P. acknowledge support from PhD FCT grant 2020.08848. BD. P.C. and É.R.G. acknowledge support from LARSyS—Portuguese national funding agency for science, research and technology (FCT) pluriannual funding 2020–2023 (Reference: UIDB/50009/2020).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data available on request due to restrictions of privacy.
Acknowledgments
We are also grateful to all the participants that were generous with their time for this study.
Conflicts of Interest
The authors declare that they have no conflict of interest.
References
- Grossman, M.R.; Zak, D.K.; Zelinski, E.M. Mobile Apps for Caregivers of Older Adults: Quantitative Content Analysis. JMIR Mhealth Uhealth 2018, 6, e162. [Google Scholar] [CrossRef]
- Storni, C. Multiple Forms of Appropriation in Self-Monitoring Technology: Reflections on the Role of Evaluation in Future Self-Care. Int. J. Hum. Comput. Interact. 2010, 26, 537–561. [Google Scholar] [CrossRef]
- Fuentes, C.; Hernandez, C.; Escobedo, L.; Herskovic, V.; Tentori, M. Promoting Self-Reflection of Social Isolation through Persuasive Mobile Technologies: The Case of Mother Caregivers of Children with Cancer. Int. J. Hum.-Comput. Interact. 2014, 30, 802–814. [Google Scholar] [CrossRef]
- Park, M.; Choi, S.; Lee, S.J.; Kim, S.H.; Kim, J.; Go, Y.; Lee, D.Y. The roles of unmet needs and formal support in the caregiving satisfaction and caregiving burden of family caregivers for persons with dementia. Int. Psychogeriatr. 2018, 30, 557–567. [Google Scholar] [CrossRef] [PubMed]
- Heynsbergh, N.; Heckel, L.; Botti, M.; Livingston, P. Feasibility, useability and acceptability of technology-based interventions for informal cancer carers: A systematic review. BMC Cancer 2018, 18, 244. [Google Scholar] [CrossRef] [PubMed]
- Boumans, N.P.G.; Dorant, E. Double-duty caregivers: Healthcare professionals juggling employment and informal caregiving. A survey on personal health and work experiences. J. Adv. Nurs. 2014, 70, 1604–1615. [Google Scholar] [CrossRef] [PubMed]
- Mazanec, S.R.; Daly, B.J.; Douglas, S.L.; Lipson, A.R. Work productivity and health of informal caregivers of persons with advanced cancer. Res. Nurs. Health 2011, 34, 483–495. [Google Scholar] [CrossRef] [PubMed]
- Pitsenberger, D.J. Juggling work and elder caregiving: Work-life balance for aging American workers. AAOHN J. 2006, 54, 181–187. [Google Scholar] [CrossRef]
- Black, B.S.; Johnston, D.; Rabins, P.V.; Morrison, A.; Lyketsos, C.; Samus, Q.M. Unmet needs of community-residing persons with dementia and their informal caregivers: Findings from the maximizing independence at home study. J. Am. Geriatr. Soc. 2013, 61, 2087–2095. [Google Scholar] [CrossRef] [PubMed]
- DiZazzo-Miller, R.; Pociask, F.D.; Adamo, D.E. The Role of Confidence in Family Caregiving for People with Dementia. Phys. Occup. Ther. Geriatr. 2020, 38, 355–369. [Google Scholar] [CrossRef]
- Campbell, P.; Wright, J.; Oyebode, J.; Job, D.; Crome, P.; Bentham, P.; Jones, L.; Lendon, C. Determinants of burden in those who care for someone with dementia. Int. J. Geriatr. Psychiatry 2008, 23, 1078–1085. [Google Scholar] [CrossRef] [PubMed]
- Reinhard, S.C.; Given, B.; Petlick, N.H.; Bemis, A. Supporting Family Caregivers in Providing Care. In Patient Safety and Quality: An Evidence-Based Handbook for Nurses; Hughes, R.G., Ed.; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2008. [Google Scholar]
- Caputo, J.; Pavalko, E.K.; Hardy, M.A. The Long-Term Effects of Caregiving on Women’s Health and Mortality. J. Marriage Family 2016, 78, 1382–1398. [Google Scholar] [CrossRef] [PubMed]
- Brown, E.L.; Ruggiano, N.; Page, T.F.; Roberts, L.; Hristidis, V.; Whiteman, K.L.; Castro, J. CareHeroes Web and AndroidTM Apps for Dementia Caregivers: A Feasibility Study. Res. Gerontol. Nurs. 2016, 9, 193–203. [Google Scholar] [CrossRef]
- Price, M.L.; Surr, C.A.; Gough, B.; Ashley, L. Experiences and support needs of informal caregivers of people with multimorbidity: A scoping literature review. Psychol. Health 2020, 35, 36–69. [Google Scholar] [CrossRef] [PubMed]
- Queluz, F.N.F.R.; Kervin, E.; Wozney, L.; Fancey, P.; McGrath, P.J.; Keefe, J. Understanding the needs of caregivers of persons with dementia: A scoping review. Int. Psychogeriatr. 2020, 32, 35–52. [Google Scholar] [CrossRef]
- Vervloet, M.; van Dijk, L.; Santen-Reestman, J.; van Vlijmen, B.; van Wingerden, P.; Bouvy, M.; de Bakker, D. SMS reminders improve adherence to oral medication in type 2 diabetes patients who are real time electronically monitored. Int. J. Med. Inform. 2012, 81, 594–604. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, D.; Zarit, S.H.; Orrell, M. Health-Promoting Self-Care in Family Caregivers of People with Dementia: The Views of Multiple Stakeholders. Gerontologist 2019, 59, e501–e511. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.; Agbata, I.N.; Canavan, M.; McCarthy, G. Effectiveness of educational interventions for informal caregivers of individuals with dementia residing in the community: Systematic review and meta-analysis of randomised controlled trials. Int. J. Geriatr. Psychiatry 2015, 30, 130–143. [Google Scholar] [CrossRef]
- Lök, N.; Bademli, K. Pilot testing of the “First You Should Get Stronger” program among caregivers of older adults with dementia. Arch. Gerontol. Geriatr. 2017, 68, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Losada, A.; Márquez-González, M.; Romero-Moreno, R.; Mausbach, B.T.; Lopez, J.; Fernández-Fernández, V.; Nogales-González, C. Cognitive-behavioral therapy (CBT) versus acceptance and commitment therapy (ACT) for dementia family caregivers with significant depressive symptoms: Results of a randomized clinical trial. J. Consult. Clin. Psychol. 2015, 83, 760–772. [Google Scholar] [CrossRef] [PubMed]
- Sharma, N.; Chakrabarti, S.; Grover, S. Gender differences in caregiving among family-caregivers of people with mental illnesses. World J. Psychiatry 2016, 6, 7. [Google Scholar] [CrossRef]
- Brown, E.L.; Ruggiano, N.; Li, J.; Clarke, P.J.; Kay, E.S.; Hristidis, V. Smartphone-Based Health Technologies for Dementia Care: Opportunities, Challenges, and Current Practices. J. Appl. Gerontol. 2019, 38, 73–91. [Google Scholar] [CrossRef]
- Cook-Cottone, C.P.; Guyker, W.M. The Development and Validation of the Mindful Self-Care Scale (MSCS): An Assessment of Practices that Support Positive Embodiment. Mindfulness 2018, 9, 161–175. [Google Scholar] [CrossRef]
- Nunes, F.; Verdezoto, N.; Fitzpatrick, G.; Kyng, M.; Grönvall, E.; Storni, C. Self-Care Technologies in HCI: Trends, Tensions, and Opportunities. ACM Trans. Comput.-Hum. Interact. 2015, 22, 6. [Google Scholar] [CrossRef]
- Washington, K.T.; Meadows, S.E.; Elliott, S.G.; Koopman, R.J. Information needs of informal caregivers of older adults with chronic health conditions. Patient Educ. Couns. 2011, 83, 37–44. [Google Scholar] [CrossRef]
- Soares, A.C.; Rêgo, A.D.S.; Rodrigues, T.F.C.D.S.; Cardoso, L.C.B.; Rossaneis, M.A.; Carreira, L.; Radovanovic, C.A.T. Construction and validation of self-care educational technology for caregivers. Rev. Bras. Enferm. 2021, 74, e20200215. [Google Scholar] [CrossRef]
- Suwa, S.; Yumoto, A.; Ueno, M.; Yamabe, T.; Hoshishiba, Y.; Sato, M. Practitioners’ identification of informal caregivers’ difficulties with activities of daily living interventions for older people with dementia in Japan. Psychogeriatrics 2021, 21, 466–477. [Google Scholar] [CrossRef]
- Fuller-Tyszkiewicz, M.; Richardson, B.; Little, K.; Teague, S.; Hartley-Clark, L.; Capic, T.; Khor, S.; Cummins, R.A.; Olsson, C.A.; Hutchinson, D. Efficacy of a Smartphone App Intervention for Reducing Caregiver Stress: Randomized Controlled Trial. JMIR Ment. Health 2020, 7, 7. [Google Scholar] [CrossRef]
- McLean, S.; Gee, M.; Booth, A.; Salway, S.; Nancarrow, S.; Cobb, M.; Bhanbhro, S. Targeting the Use of Reminders and Notifications for Uptake by Populations (TURNUP): A systematic review and evidence synthesis. Health Serv. Deliv. Res. 2014, 2, 1–184. [Google Scholar] [CrossRef]
- Damgaard, M.T.; Gravert, C. Now or never! The effect of deadlines on charitable giving: Evidence from two natural field experiments. J. Behav. Exp. Econ. 2017, 66, 78–87. [Google Scholar] [CrossRef]
- Damgaard, M.T.; Gravert, C. The hidden costs of nudging: Experimental evidence from reminders in fundraising. J. Public Econ. 2018, 157, 15–26. [Google Scholar] [CrossRef]
- Parker, C.; Scott, S.; Geddes, A. Snowball Sampling. In Research Methods Foundations; Atkinson, P., Delamont, S., Cernat, A., Sakshaug, J.W., Williams, R.A., Eds.; Sage: Newcastle upon Tyne, UK, 2019. [Google Scholar]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).