
Evaluation of MyRelief Serious Game for Better Self-Management of Health Behaviour Strategies on Chronic Low-Back Pain

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
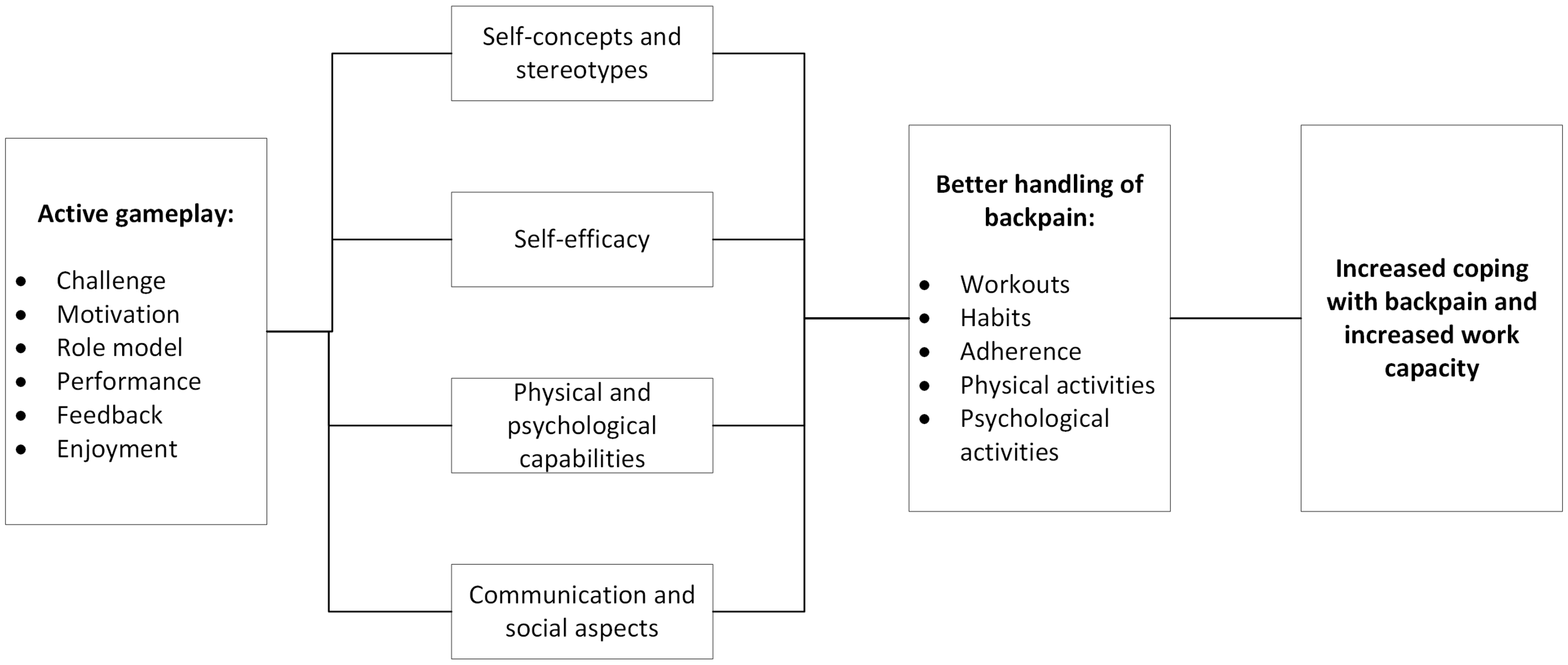
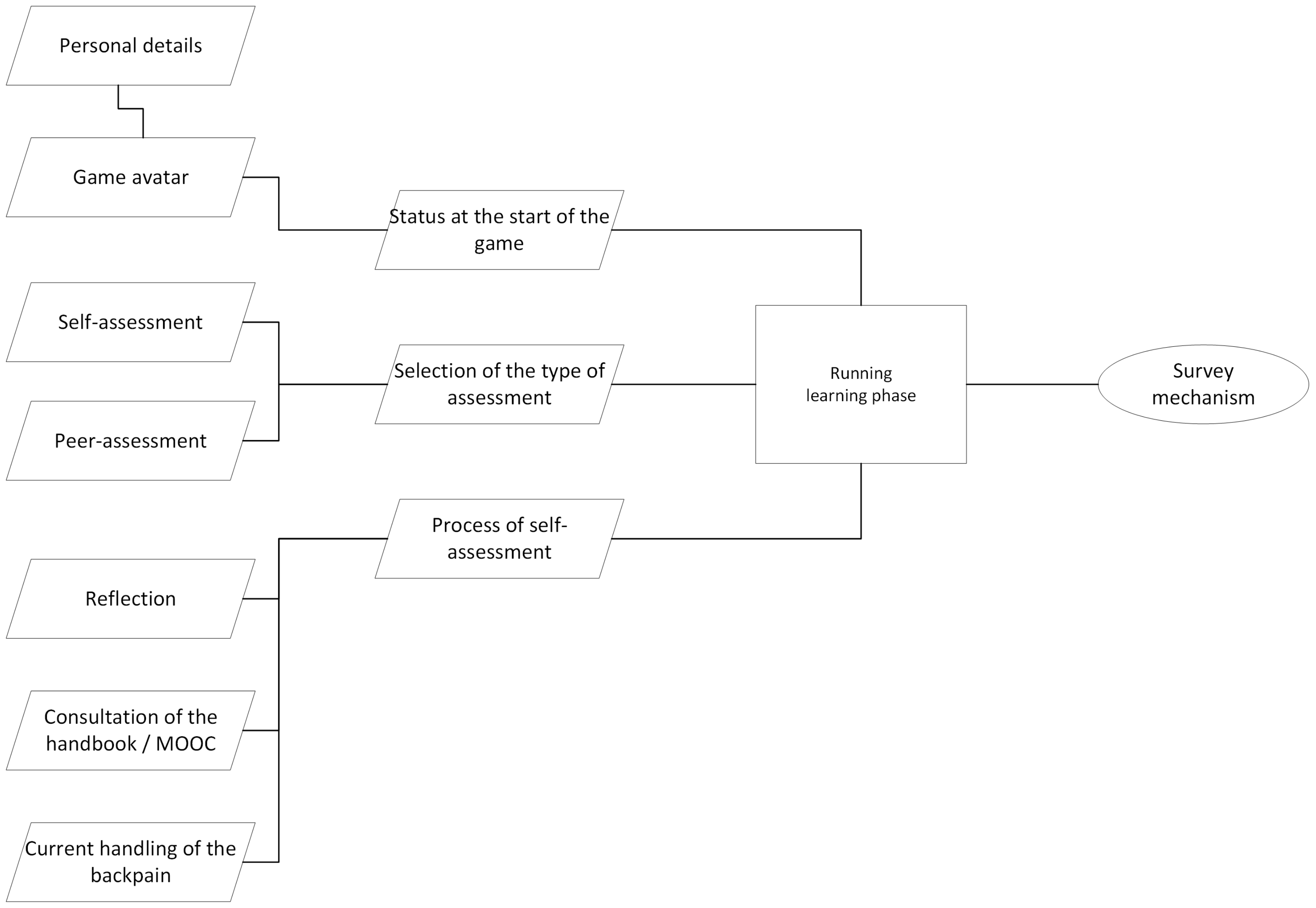
2.1. The Challenge Model
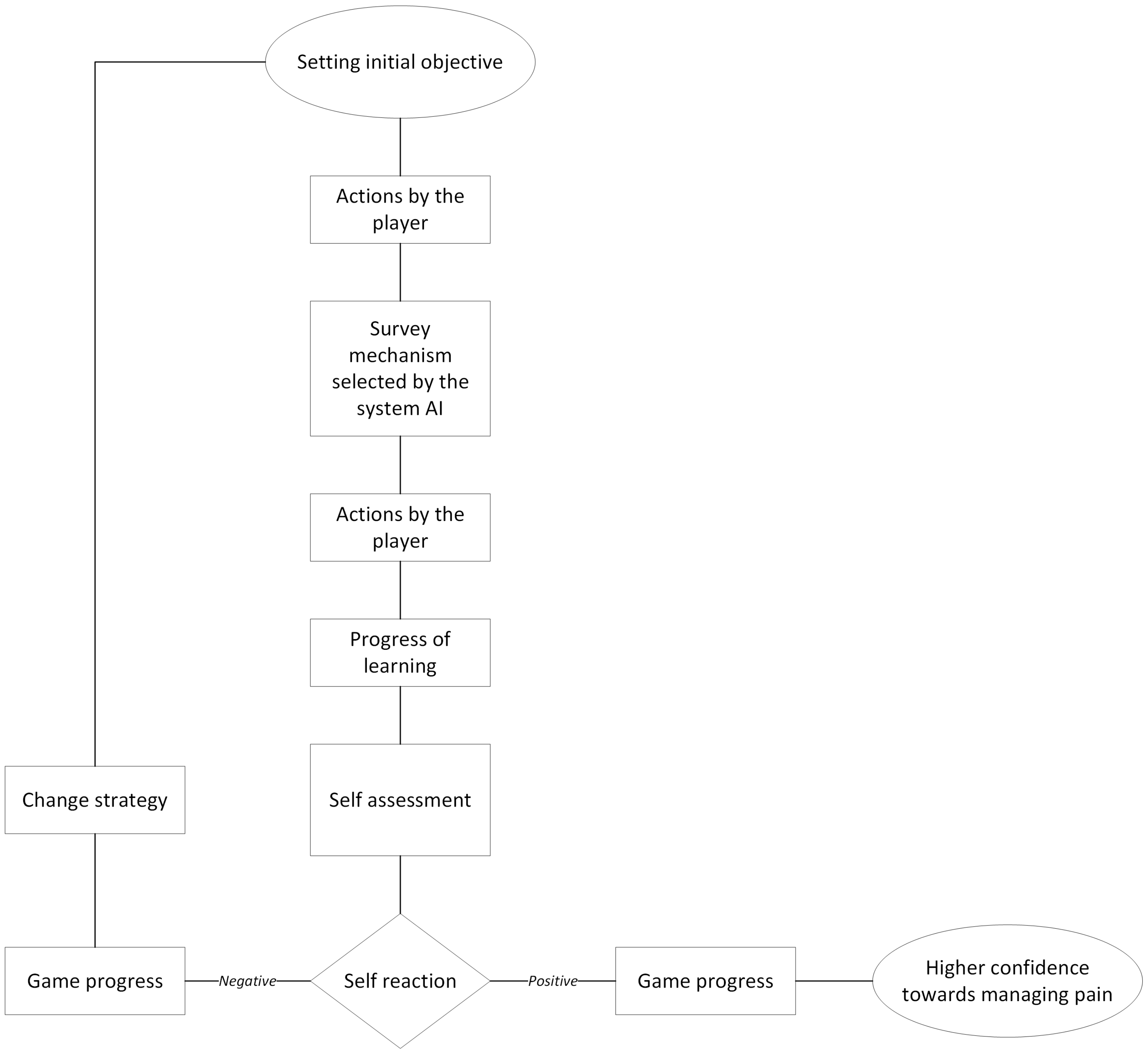
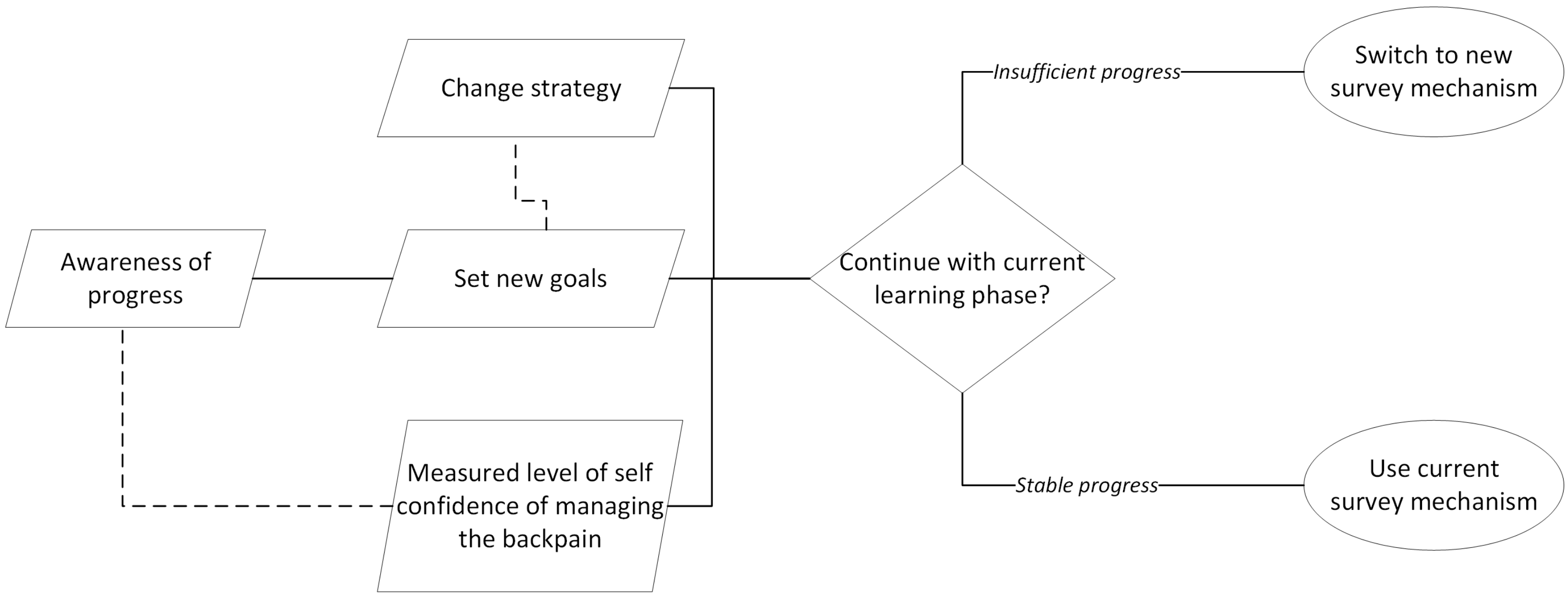
2.2. Knowledge Transfer Model
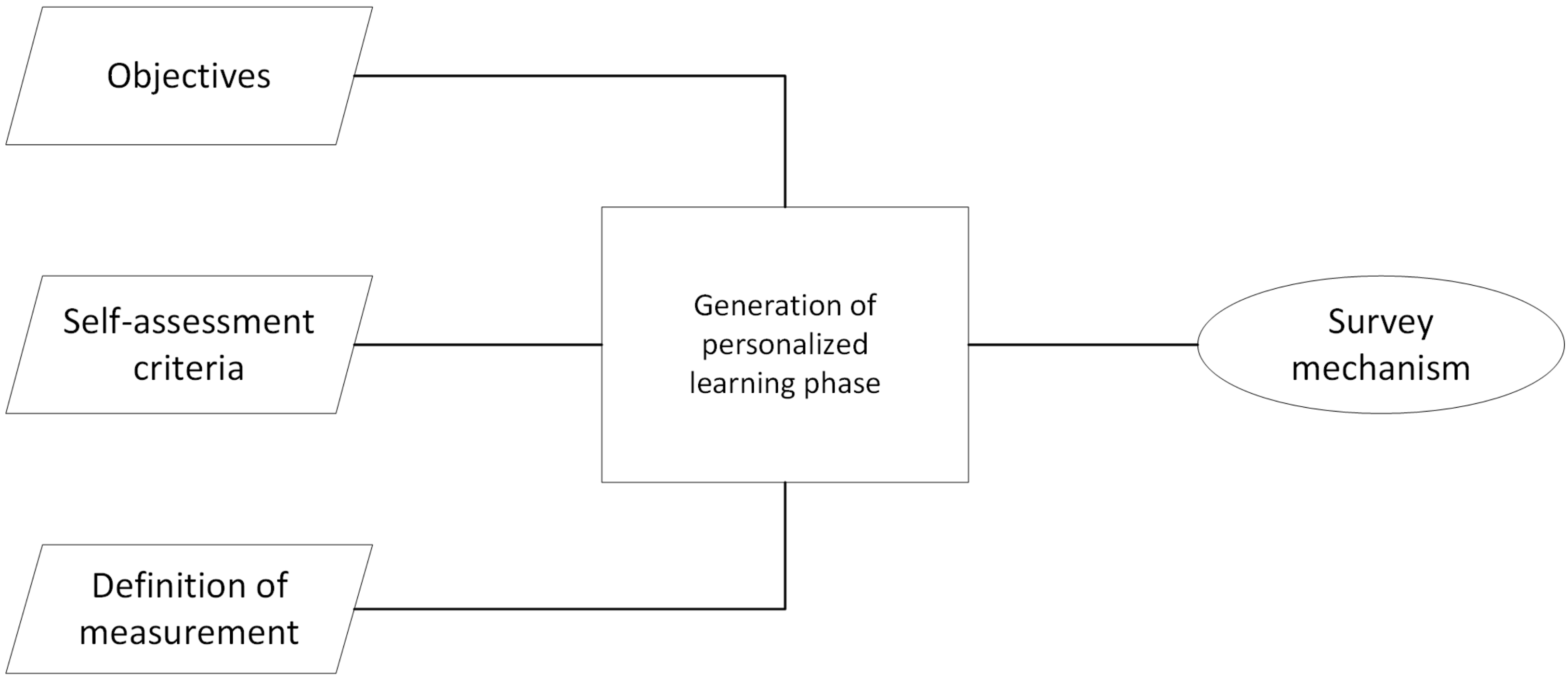
2.3. Ontology Based Approach
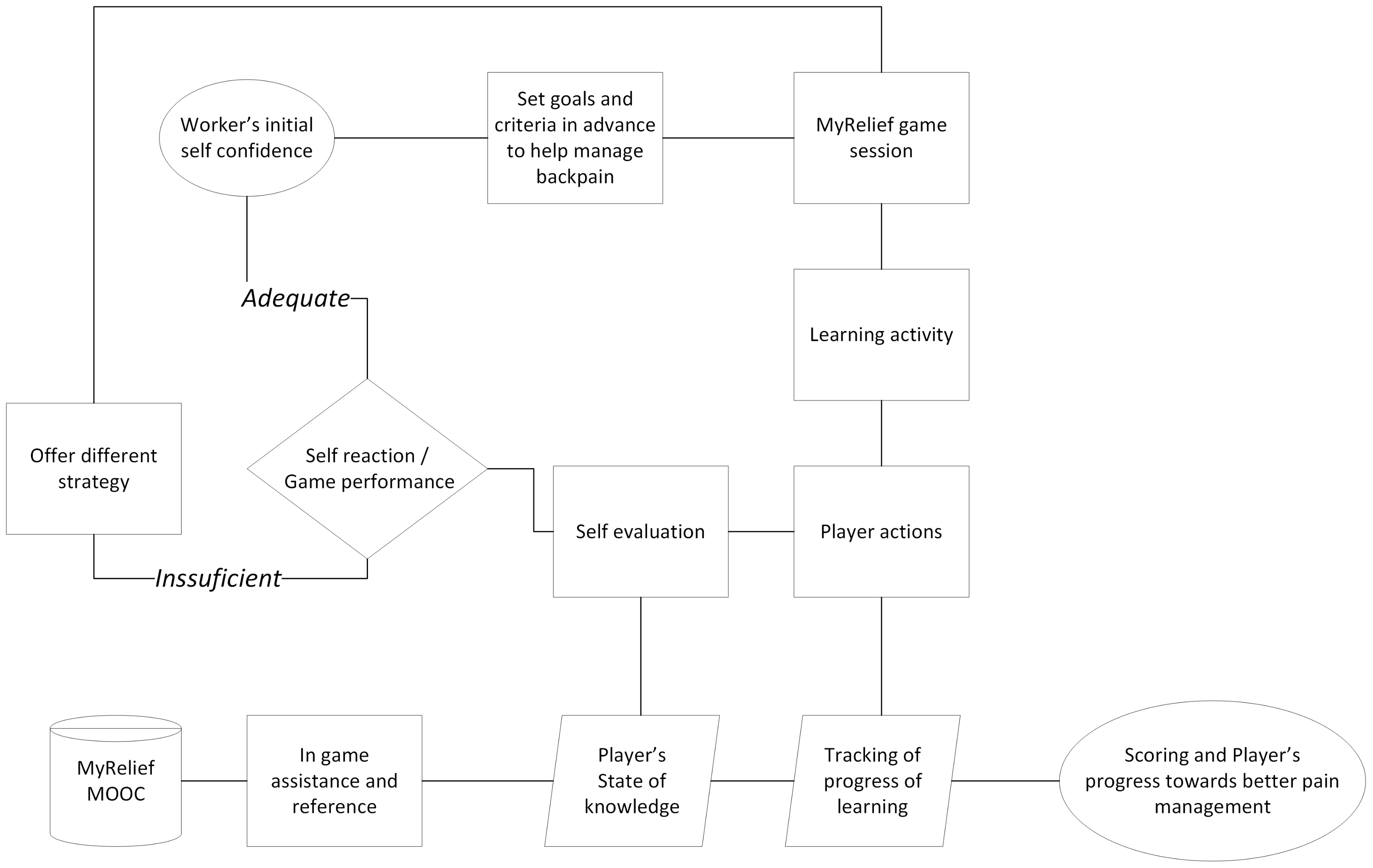
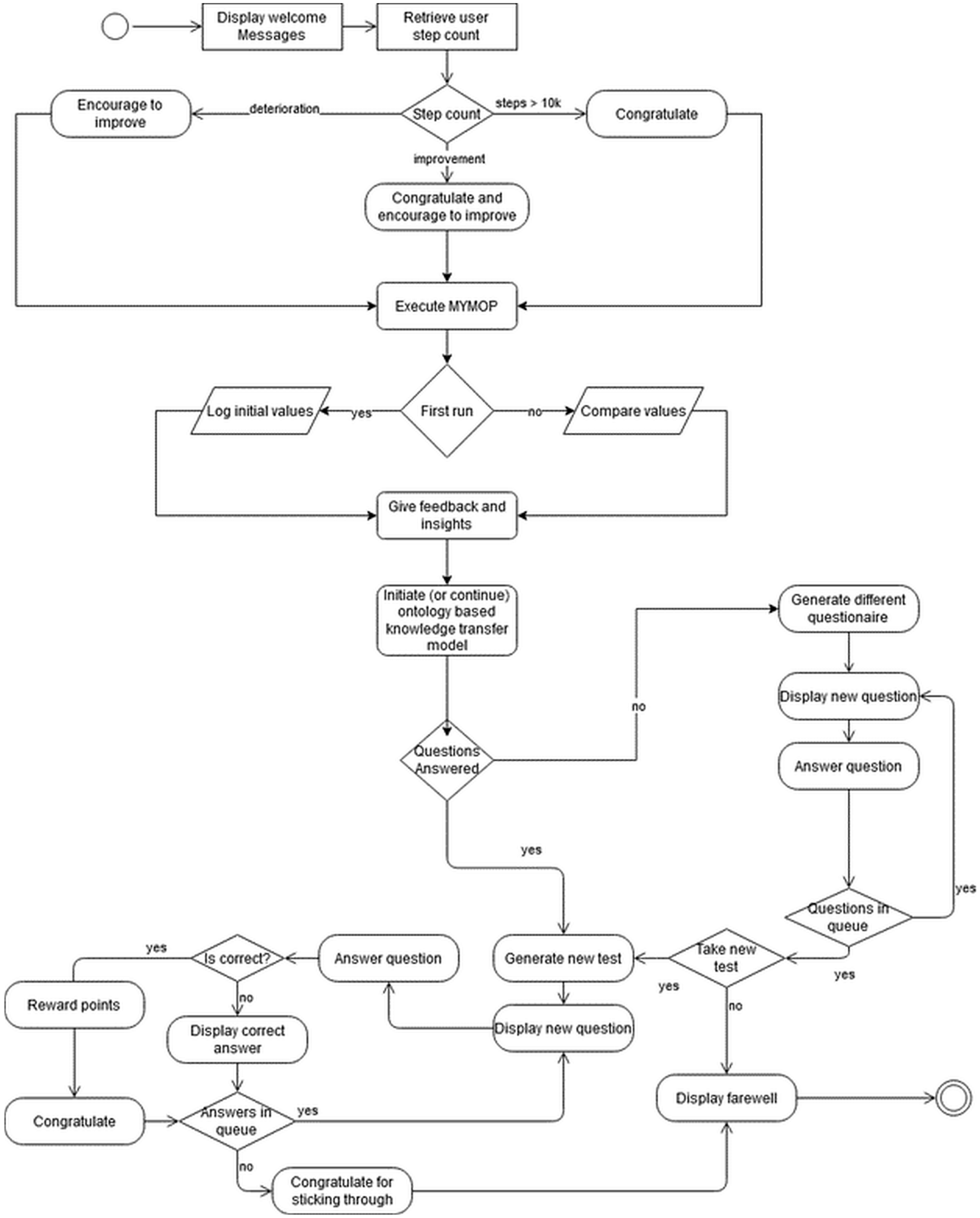
2.4. Logical Flow of The App
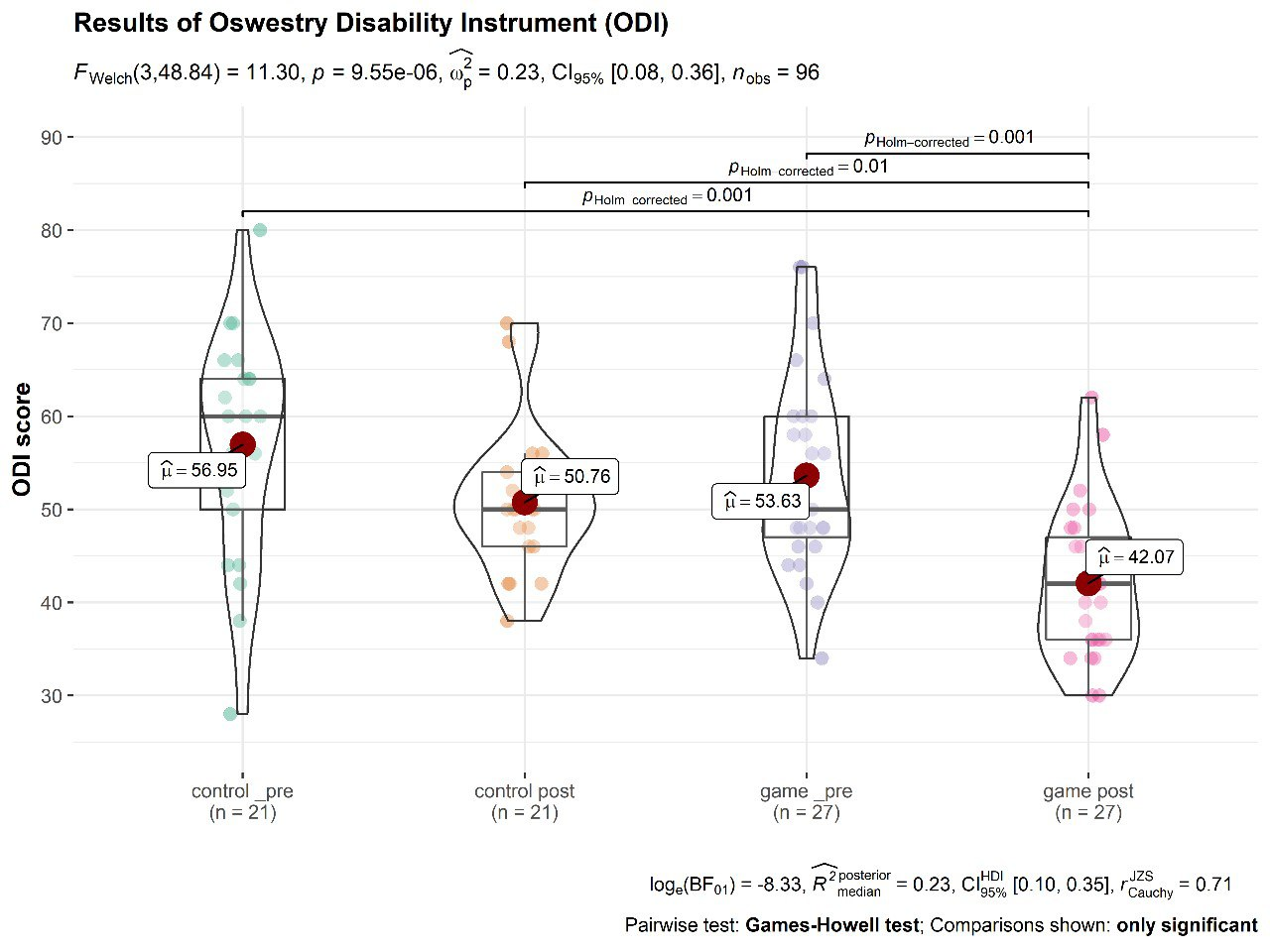
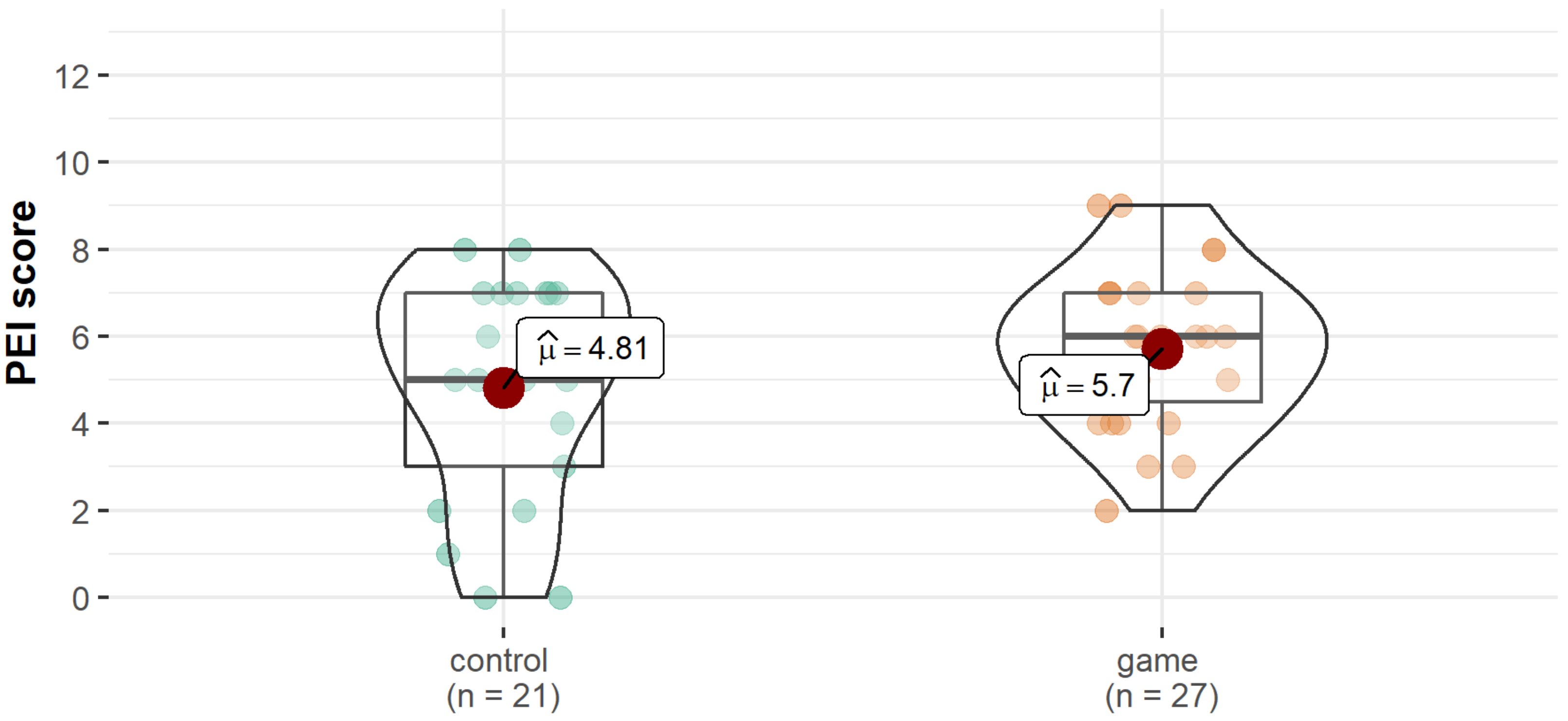
2.5. Evaluation of Functional Disability
2.6. Statistical Analysis
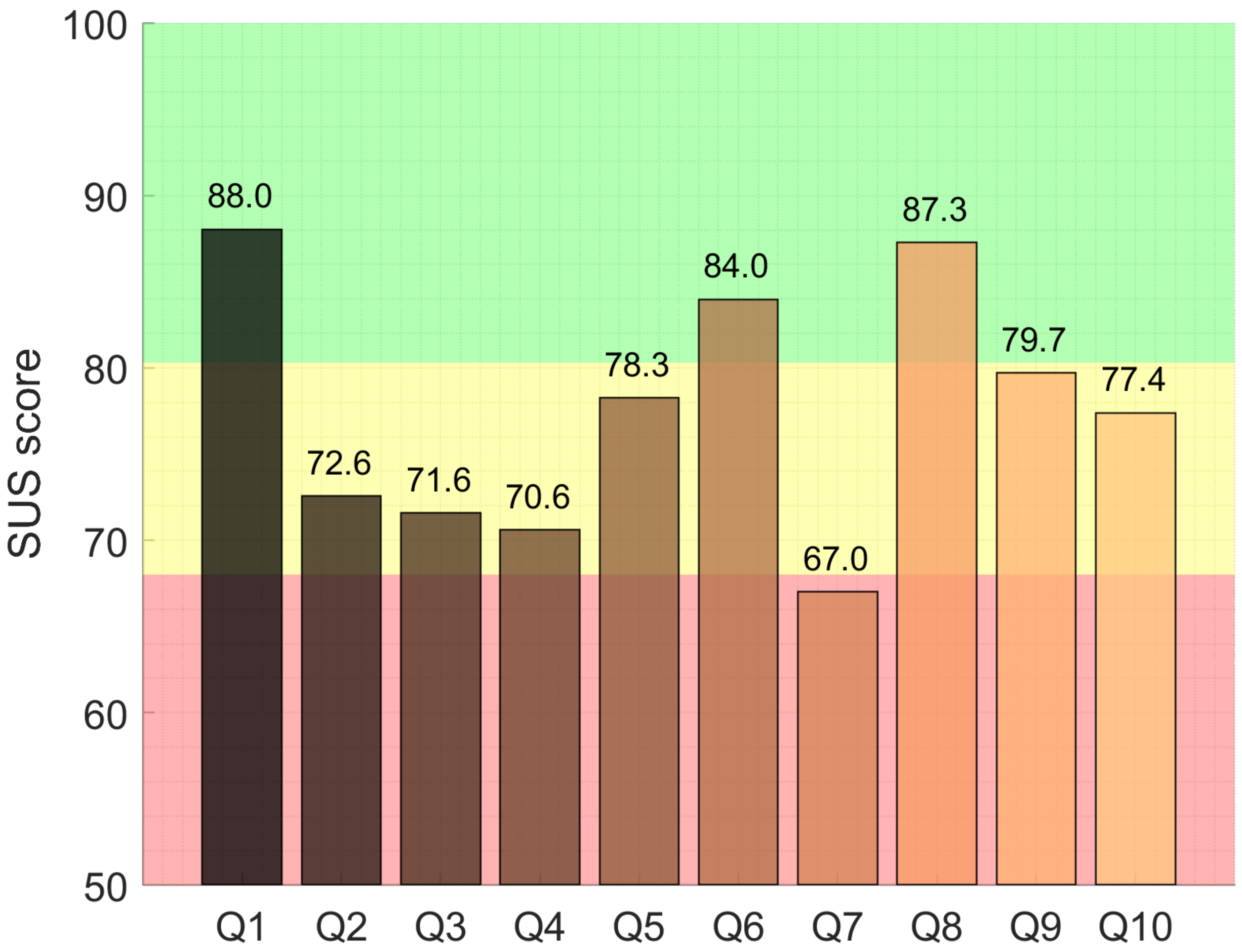
2.7. Evaluation of Usability
3. Participants and Results
3.1. Participants
3.2. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| LBP | Lower Back Pain |
| VR | Virtual Reality |
| CP | Chronic Pain |
| Xbox | Xbox game console |
| cLBP | Chronic Low Back Pain |
| ODI | Oswestri Disability Index |
| Wii | Nintendo Wii game console |
| AI | Artificial Inteligence |
| MYMOP | Measure Yourself Medical Outcome Profile |
| MOOC | Massive Online Open Course |
| KTM | Knowledge Transfer Model |
| PEI | Patient Enablement Instrument |
| SUS | System Usability Scale |
References
- Husky, M.M.; Ferdous Farin, F.; Compagnone, P.; Fermanian, C.; Kovess-Masfety, V. Chronic back pain and its association with quality of life in a large French population survey. Health Qual. Life Outcomes 2018, 16, 195. [Google Scholar] [CrossRef] [PubMed]
- Kinnaird, E.; Kimergård, A.; Jennings, S.; Drummond, C.; Deluca, P. From pain treatment to opioid dependence: A qualitative study of the environmental influence on codeine use in UK adults. BMJ Open 2019, 9, e025331. [Google Scholar] [CrossRef] [PubMed]
- Devleesschauwer, B.; Maertens de Noordhout, C.; Smit, G.S.A.; Duchateau, L.; Dorny, P.; Stein, C.; Van Oyen, H.; Speybroeck, N. Quantifying burden of disease to support public health policy in Belgium: Opportunities and constraints. BMC Public Health 2014, 14, 1196. [Google Scholar] [CrossRef] [PubMed]
- Hartvigsen, J.; Hancock, M.J.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; Hoy, D.; Karppinen, J.; Pransky, G.; Sieper, J.; et al. What low back pain is and why we need to pay attention. Lancet 2018, 391, 2356–2367. [Google Scholar] [CrossRef]
- Maher, C.; Underwood, M.; Buchbinder, R. Non-specific low back pain. Lancet 2017, 389, 736–747. [Google Scholar] [CrossRef]
- Matz, P.G.; Meagher, R.; Lamer, T.; Tontz, W.L.; Annaswamy, T.M.; Cassidy, R.C.; Cho, C.H.; Dougherty, P.; Easa, J.E.; Enix, D.E.; et al. Guideline summary review: An evidence-based clinical guideline for the diagnosis and treatment of degenerative lumbar spondylolisthesis. Spine J. 2016, 16, 439–448. [Google Scholar] [CrossRef]
- Marley, J.; Tully, M.A.; Porter-Armstrong, A.; Bunting, B.; O’Hanlon, J.; Atkins, L.; Howes, S.; McDonough, S.M. The effectiveness of interventions aimed at increasing physical activity in adults with persistent musculoskeletal pain: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2017, 18, 482. [Google Scholar] [CrossRef]
- Nicholl, B.I.; Sandal, L.F.; Stochkendahl, M.J.; McCallum, M.; Suresh, N.; Vasseljen, O.; Hartvigsen, J.; Mork, P.J.; Kjaer, P.; Søgaard, K.; et al. Digital Support Interventions for the Self-Management of Low Back Pain: A Systematic Review. J. Med. Internet Res. 2017, 19, e7290. [Google Scholar] [CrossRef]
- Eichenberg, C.; Schott, M. Serious Games for Psychotherapy: A Systematic Review. Games Health J. 2017, 6, 127–135. [Google Scholar] [CrossRef]
- Maskeliūnas, R.; Kulikajevas, A.; Blažauskas, T.; Damaševičius, R.; Swacha, J. An interactive serious mobile game for supporting the learning of programming in javascript in the context of eco-friendly city management. Computers 2020, 9, 102. [Google Scholar] [CrossRef]
- Swacha, J.; Maskeliūnas, R.; Damaševičius, R.; Kulikajevas, A.; Blažauskas, T.; Muszyńska, K.; Miluniec, A.; Kowalska, M. Introducing sustainable development topics into computer science education: Design and evaluation of the eco jsity game. Sustainability 2021, 13, 4244. [Google Scholar] [CrossRef]
- Maskeliunas, R.; Damaševičius, R.; Lethin, C.; Paulauskas, A.; Esposito, A.; Catena, M.; Aschettino, V. Serious game iDO: Towards better education in dementia care. Information 2019, 10, 355. [Google Scholar] [CrossRef]
- Vasiljevas, M.; Damaševičius, R.; Połap, D.; Woźniak, M. Gamification of Eye Exercises for Evaluating Eye Fatigue; LNAI, Lecture Notes in Computer Science (Including Subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics); Springer: Cham, Switzerland, 2019; pp. 104–114. [Google Scholar]
- Maskeliūnas, R.; Blažauskas, T.; Damaševičius, R. Depression Behavior Detection Model Based on Participation in Serious Games; LNAI, Lecture Notes in Computer Science (Including Subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics); Springer: Cham, Switzerland, 2017; Volume 10314, pp. 423–434. [Google Scholar]
- Palazzo, C.; Klinger, E.; Dorner, V.; Kadri, A.; Thierry, O.; Boumenir, Y.; Martin, W.; Poiraudeau, S.; Ville, I. Barriers to home-based exercise program adherence with chronic low back pain: Patient expectations regarding new technologies. Ann. Phys. Rehabil. Med. 2016, 59, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Trost, Z.; Zielke, M.; Guck, A.; Nowlin, L.; Zakhidov, D.; France, C.R.; Keefe, F. The promise and challenge of virtual gaming technologies for chronic pain: The case of graded exposure for low back pain. Pain Manag. 2015, 5, 197–206. [Google Scholar] [CrossRef]
- Tack, C. Virtual reality and chronic low back pain. Disabil. Rehabil. Assist. Technol. 2019, 16, 637–645. [Google Scholar] [CrossRef]
- Jin, W.; Choo, A.; Gromala, D.; Shaw, C.D.; Squire, P. A Virtual Reality Game for Chronic Pain Management: A Randomized, Controlled Clinical Study. Stud. Health Technol. Inform. 2016, 220, 154–160. [Google Scholar]
- Mbada, C.E.; Salami, A.J.; Dada, O.O.; Gambo, I.P.; Odole, A.C.; Adejumobi, A.S.; Olatoye, F.S.; Makinde, M.O.; Bateye, O.; Fatoye, F.A. Development and feasibility testing of a back extension-glide virtual reality game for low-back pain. Int. J. Telemed. Clin. Pract. 2020, 3, 243–256. [Google Scholar] [CrossRef]
- Alazba, A.; Al-Khalifa, H.; AlSobayel, H. RabbitRun: An Immersive Virtual Reality Game for Promoting Physical Activities Among People with Low Back Pain. Technologies 2018, 7, 2. [Google Scholar] [CrossRef]
- Alazba, A.; Al-Khalifa, H.; AlSobayel, H. A Proposed Game for Promoting Physical Activities among People with Low Back Pain using Virtual Reality. In Proceedings of the 11th PErvasive Technologies Related to Assistive Environments Conference, Corfu, Greece, 26–29 June 2018; 2018; pp. 141–144. [Google Scholar] [CrossRef]
- Stamm, O.; Dahms, R.; Reithinger, N.; Ruß, A.; Müller-Werdan, U. Virtual reality exergame for supplementing multimodal pain therapy in older adults with chronic back pain: A randomized controlled pilot study. Virtual Real. 2022, 1–15. [Google Scholar] [CrossRef]
- Hennessy, R.W.; Rumble, D.; Christian, M.; Brown, D.A.; Trost, Z. A Graded Exposure, Locomotion-Enabled Virtual Reality App During Walking and Reaching for Individuals With Chronic Low Back Pain: Cohort Gaming Design. JMIR Serious Games 2020, 8, e17799. [Google Scholar] [CrossRef]
- Thomas, J.S.; France, C.R.; Applegate, M.E.; Leitkam, S.T.; Walkowski, S. Feasibility and Safety of a Virtual Reality Dodgeball Intervention for Chronic Low Back Pain: A Randomized Clinical Trial. J. Pain 2016, 17, 1302–1317. [Google Scholar] [CrossRef] [PubMed]
- Ašeriškis, D.; Damaševičius, R. Gamification of a project management system. In Proceedings of the ACHI 2014—7th International Conference on Advances in Computer-Human Interactions, Barcelona, Spain, 23–27 March 2014; pp. 200–207. [Google Scholar]
- Trombetta, M.; Bazzanello Henrique, P.P.; Brum, M.R.; Colussi, E.L.; De Marchi, A.C.B.; Rieder, R. Motion Rehab AVE 3D: A VR-based exergame for post-stroke rehabilitation. Comput. Methods Programs Biomed. 2017, 151, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Šalkevicius, J.; Damaševičius, R.; Maskeliunas, R.; Laukienė, I. Anxiety level recognition for virtual reality therapy system using physiological signals. Electronics 2019, 8, 1039. [Google Scholar] [CrossRef]
- Boutevillain, L.; Dupeyron, A.; Rouch, C.; Richard, E.; Coudeyre, E. Facilitators and barriers to physical activity in people with chronic low back pain: A qualitative study. PLoS ONE 2017, 12, e0179826. [Google Scholar] [CrossRef] [PubMed]
- Ishaque, S.; Johnson, J.A.; Vohra, S. Individualized health-related quality of life instrument Measure Yourself Medical Outcome Profile (MYMOP) and its adaptations: A critical appraisal. Qual. Life Res. 2018, 28, 879–893. [Google Scholar] [CrossRef]
- MyRelief MOOC in the Udemy Platform. Available online: https://www.udemy.com/course/self-management-strategies-for-people-with-low-back-pain/ (accessed on 20 March 2022).
- Damaševičius, R. Towards Empirical Modelling of Knowledge Transfer in Teaching/Learning Process; Communications in Computer and Information Science; Springer: Cham, Switzerland, 2014; Volume 465, pp. 359–372. [Google Scholar]
- Stemberkova, R.; Maresova, P.; David, O.O.; Adeoye, F. Knowledge management model for effective technology transfer at universities. Ind. High. Educ. 2021, 35, 638–649. [Google Scholar] [CrossRef]
- Tankelevičiene, L.; Damaševičius, R. Towards the development of genuine intelligent ontology-based e-Learning systems. In Proceedings of the 2010 IEEE International Conference on Intelligent Systems, IS 2010—Proceedings, London, UK, 7–9 July 2010; pp. 79–84. [Google Scholar]
- Chiarotto, A.; Maxwell, L.J.; Terwee, C.B.; Wells, G.A.; Tugwell, P.; Ostelo, R.W. Roland-Morris Disability Questionnaire and Oswestry Disability Index: Which Has Better Measurement Properties for Measuring Physical Functioning in Nonspecific Low Back Pain? Systematic Review and Meta-Analysis. Phys. Ther. 2016, 96, 1620–1637. [Google Scholar] [CrossRef]
- Smeets, R.; Köke, A.; Lin, C.W.; Ferreira, M.; Demoulin, C. Measures of function in low back pain/disorders: Low Back Pain Rating Scale (LBPRS), Oswestry Disability Index (ODI), Progressive Isoinertial Lifting Evaluation (PILE), Quebec Back Pain Disability Scale (QBPDS), and Roland-Morris Disability Questionnaire. Arthritis Care Res. 2011, 63, S158–S173. [Google Scholar] [CrossRef]
- Kim, G.m.; Yi, C.h.; Cynn, H.s. Factors Influencing Disability due to Low Back Pain Using the Oswestry Disability Questionnaire and the Quebec Back Pain Disability Scale. Physiother. Res. Int. 2014, 20, 16–21. [Google Scholar] [CrossRef]
- Pawlikowska, T.R.; Walker, J.J.; Nowak, P.R.; Szumilo-Grzesik, W. Patient involvement in assessing consultation quality: A quantitative study of the Patient Enablement Instrument in Poland. Heal. Expect. 2010, 13, 13–23. [Google Scholar] [CrossRef]
- Molgaard Nielsen, A.; Hartvigsen, J.; Kongsted, A.; Öberg, B.; Enthoven, P.; Abbott, A.; Lauridsen, H.H. The patient enablement instrument for back pain: Reliability, content validity, construct validity and responsiveness. Heal. Qual. Life Outcomes 2021, 19, 116. [Google Scholar] [CrossRef] [PubMed]
- Enthoven, P.; Peolsson, A.; Landén Ludvigsson, M.; Wibault, J.; Peterson, G.; Öberg, B. Validity, internal consistency and self-rated change of the patient enablement instrument in patients with chronic musculoskeletal pain. J. Rehabil. Med. 2019, 51, 587–597. [Google Scholar] [CrossRef]
- Lewis, J.R. The System Usability Scale: Past, Present, and Future. Int. J. Hum. Comput. Interact. 2018, 34, 577–590. [Google Scholar] [CrossRef]
- Vlachogianni, P.; Tselios, N. Perceived usability evaluation of educational technology using the System Usability Scale (SUS): A systematic review. J. Res. Technol. Educ. 2021, 1–18. [Google Scholar] [CrossRef]
- Skarbalienė, A.; Jurgutis, A.; Strandberg, E.L.; Pawlikowska, T. Patient involvement in assessing consultation quality: Validation of patient enablement instrument (PEI) in Lithuanian general practice. BMC Fam. Pract. 2019, 20, 167. [Google Scholar] [CrossRef] [PubMed]
- Adžić, Z.O.; Katić, M.; Kern, J.; Lazić, Đ.; Nekić, V.C.; Soldo, D. Patient, Physician, and Practice Characteristics Related to Patient Enablement in General Practice in Croatia: Cross-sectional Survey Study. Croat. Med J. 2008, 49, 813. [Google Scholar] [CrossRef] [PubMed]
- Rööst, M.; Zielinski, A.; Petersson, C.; Strandberg, E.L. Reliability and applicability of the Patient Enablement Instrument (PEI) in a Swedish general practice setting. BMC Fam. Pract. 2015, 16, 31. [Google Scholar] [CrossRef]
- Hudon, C.; Fortin, M.; Rossignol, F.; Bernier, S.; Poitras, M.E. The Patient Enablement Instrument-French version in a family practice setting: A reliability study. BMC Fam. Pract. 2011, 12, 71. [Google Scholar] [CrossRef]
- Pekonen, A.; Eloranta, S.; Stolt, M.; Virolainen, P.; Leino-Kilpi, H. Measuring patient empowerment—A systematic review. Patient Educ. Couns. 2020, 103, 777–787. [Google Scholar] [CrossRef]
- Howie, J.G.; Heaney, D.J.; Maxwell, M.; Walker, J.J. A comparison of a Patient Enablement Instrument (PEI) against two established satisfaction scales as an outcome measure of primary care consultations. Fam. Pract. 1998, 15, 165–171. [Google Scholar] [CrossRef]
- Mercer, S.W.; Neumann, M.; Wirtz, M.; Fitzpatrick, B.; Vojt, G. General practitioner empathy, patient enablement, and patient-reported outcomes in primary care in an area of high socio-economic deprivation in Scotland—A pilot prospective study using structural equation modeling. Patient Educ. Couns. 2008, 73, 240–245. [Google Scholar] [CrossRef] [PubMed]










Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maskeliūnas, R.; Damaševičius, R.; Kulikajevas, A.; Marley, J.; Larsson, C. Evaluation of MyRelief Serious Game for Better Self-Management of Health Behaviour Strategies on Chronic Low-Back Pain. Informatics 2022, 9, 40. https://doi.org/10.3390/informatics9020040
Maskeliūnas R, Damaševičius R, Kulikajevas A, Marley J, Larsson C. Evaluation of MyRelief Serious Game for Better Self-Management of Health Behaviour Strategies on Chronic Low-Back Pain. Informatics. 2022; 9(2):40. https://doi.org/10.3390/informatics9020040
Chicago/Turabian StyleMaskeliūnas, Rytis, Robertas Damaševičius, Audrius Kulikajevas, Joane Marley, and Caroline Larsson. 2022. "Evaluation of MyRelief Serious Game for Better Self-Management of Health Behaviour Strategies on Chronic Low-Back Pain" Informatics 9, no. 2: 40. https://doi.org/10.3390/informatics9020040
APA StyleMaskeliūnas, R., Damaševičius, R., Kulikajevas, A., Marley, J., & Larsson, C. (2022). Evaluation of MyRelief Serious Game for Better Self-Management of Health Behaviour Strategies on Chronic Low-Back Pain. Informatics, 9(2), 40. https://doi.org/10.3390/informatics9020040