
Design Requirements of Breast Cancer Symptom-Management Apps

Abstract
1. Introduction
2. Background
2.1. Symptom Burden and Survivorship Needs
2.2. Digital Readiness and Equity Considerations
2.3. State of the Evidence
3. Problem Definition
4. Requirements Identification
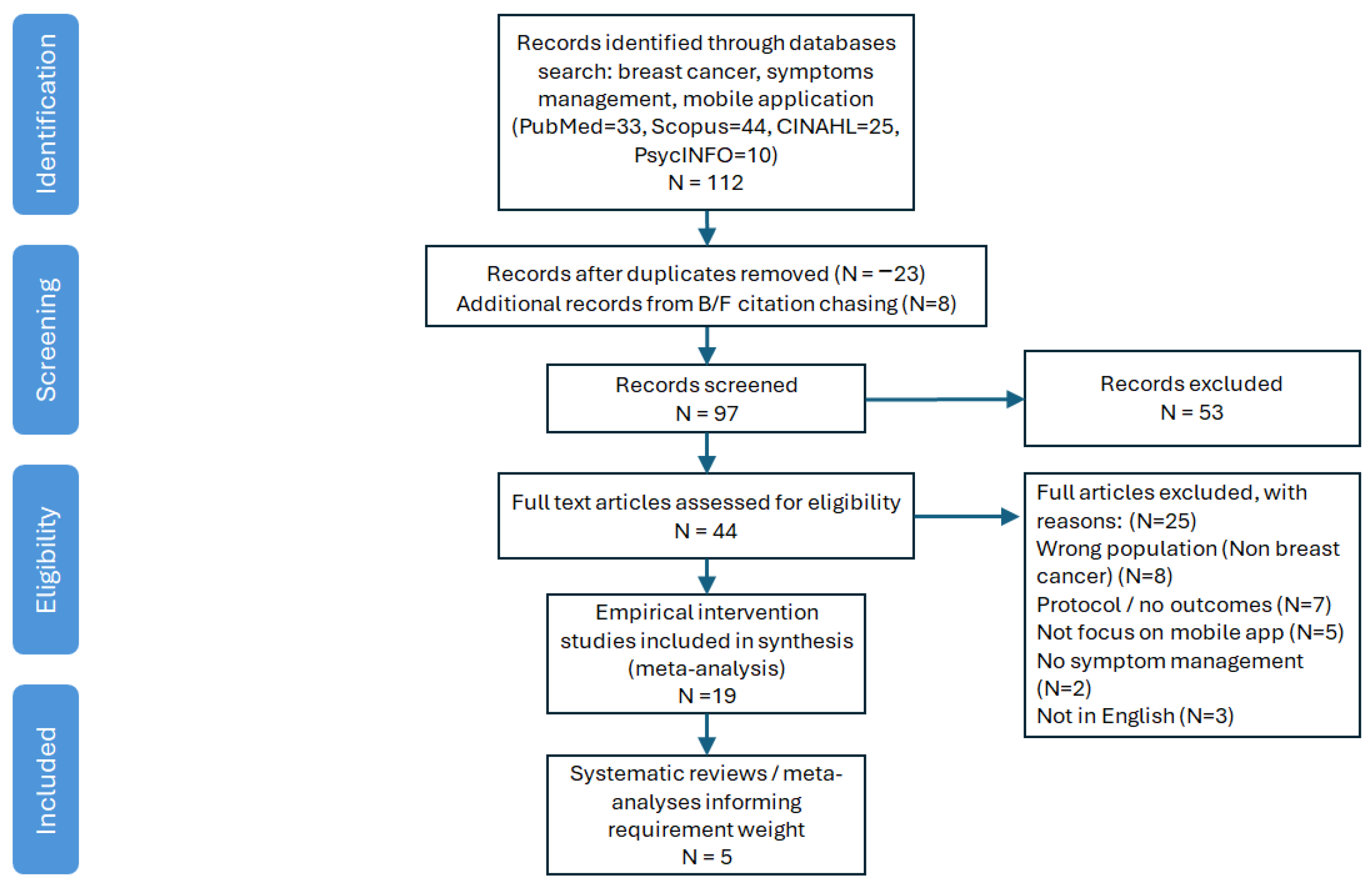
4.1. Literature Search Process and Systematic Review
4.2. Literature-Derived Requirements
- Evidence tagging: every feature reported in ≥2 empirical trials or highlighted in ≥1 systematic review was tagged with its primary patient-need (capture, respond, empower) and evidence strength (number of supporting studies).
- Requirement clustering: tagged features were clustered into functional requirements (FR) and non-functional requirements (NFR) using standard ISO/IEC 25010 categories.
- Criticality weighting: each requirement was assigned a weight (1 = nice-to-have, 3 = critical) proportional to (i) the volume of evidence and (ii) the magnitude of outcome benefit reported.
5. Screening, Evaluation and Benchmarking Leading Mobile Apps
5.1. Marketplace Screening
- OWise Breast Cancer
- Outcomes4Me Cancer Care
- Wave Health/chemoWave (same developer ecosystem)
- Breast Cancer Manager
- CancerAid
5.2. Scoring Framework
- Mental-health support (FR7)—an app scored 5 only if it offered a validated mood diary plus guided CBT/mindfulness modules; mood tracking alone warranted ≤ 3.
- AI-driven coaching (FR8)—a 5 required machine-learning-based insight or prediction (e.g., adaptive treatment guidance); simple rule-based tips scored ≤ 3.
- VR distraction (FR6)—because no breast-cancer-specific VR apps are in the stores, all evaluated products scored 0 here, highlighting an innovation gap.
- Key observations
- Interoperability remains the decisive differentiator: OWise is the only product with live HL7 FHIR feeds into hospital EHRs.
- Mental-health features (FR7) are still embryonic. Only Wave Health and Outcomes4Me offer mood tracking; none deliver structured CBT or mindfulness curricula.
- AI personalisation (FR8) is emerging: Outcomes4Me uses AI to translate NCCN guidelines into lay recommendations, while Wave Health correlates self-reported behaviours with symptom trends. Both score ≥ 3, but neither performs predictive toxicity forecasting as described in BorjAlilu et al. [62].
- VR symptom distraction (FR6) is entirely absent in the consumer marketplace, reinforcing Tian et al.’s [60] call for VR integration.
5.3. Gap Analysis and Implications for Design
- Bidirectional FHIR-based integration to close the alert loop with oncology teams.
- Modular mental-health tools (mood diary, CBT, mindfulness) with evidence-based content libraries.
- Pluggable AI engine for personalised coaching and early-warning analytics, leveraging accumulated symptom trajectories.
- Optional VR module for patients who can access a headset, fulfilling FR6.
6. Requirements for Future Design of Breast Cancer Symptom-Management Apps
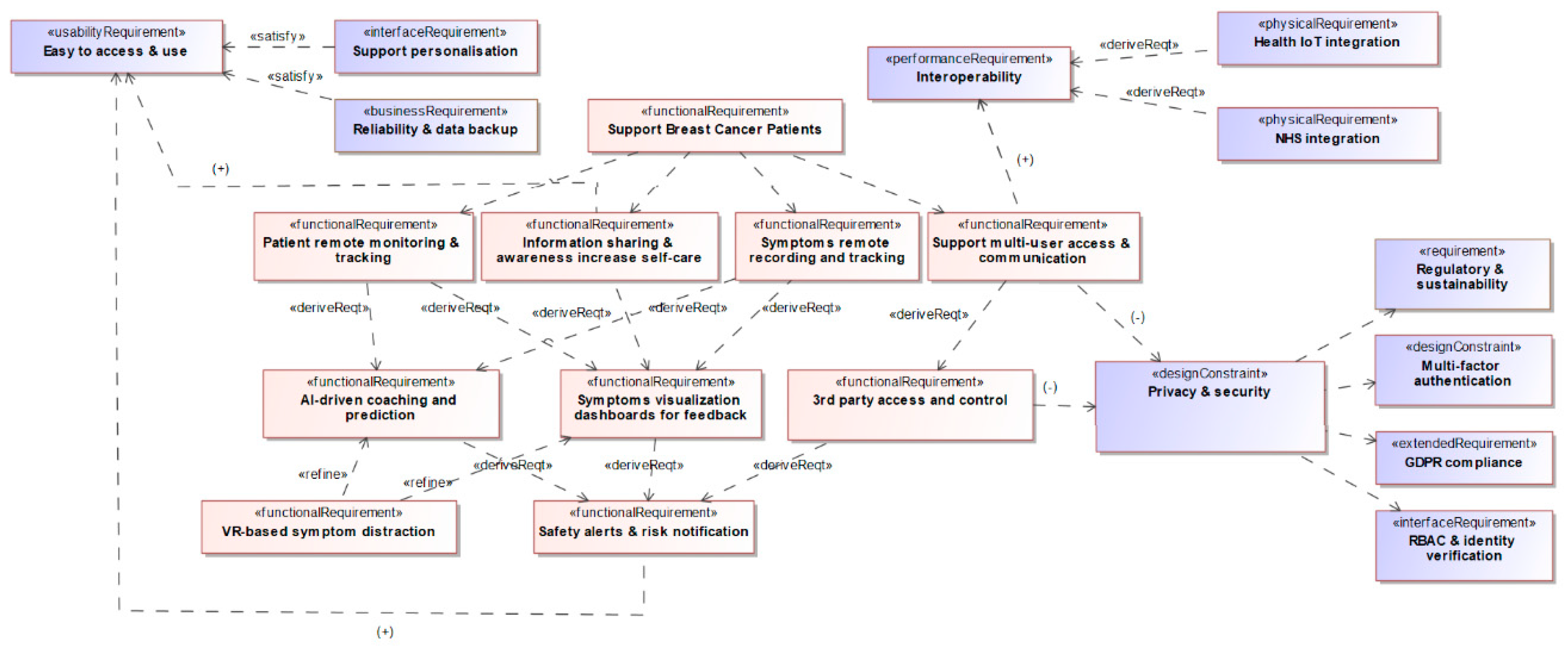
6.1. Requirements Modelling
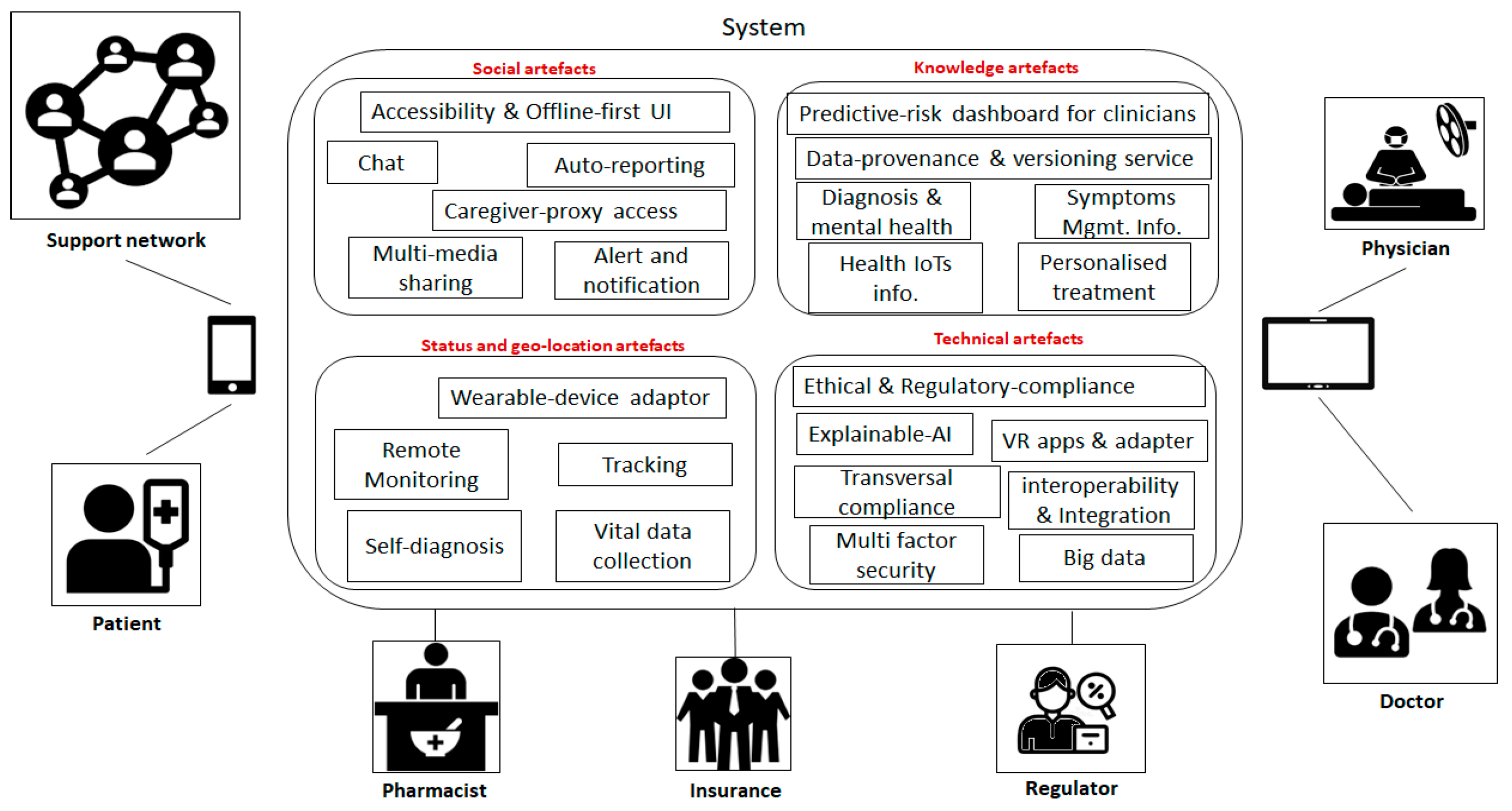
6.2. Conceptual Design of Breast Cancer Symptom-Management Apps
- Predictive-risk dashboard for clinicians. Built with SMART-on-FHIR widgets, the dashboard streams patient-reported outcomes (PROs) and wearable metrics directly into the electronic health record (EHR), eliminating the need for parallel portals and allowing oncologists to act on new information within the workflow they already use.
- Data-provenance and versioning service. Every model update, training dataset, and parameter change is time-stamped, thereby supporting post-market surveillance and reproducibility—capabilities explicitly called for in the FDA’s AI/ML Software-as-a-Medical-Device (SaMD) Action Plan.
- Diagnosis & mental-health guidance. A digital cognitive behavioural therapy (CBT) workbook and mood diary respond to evidence that CBT, integrated with activity pacing, mitigates cancer-related fatigue and depression.
- Virtual-reality (VR) apps & adapter. An adaptor layer lets approved VR modules deliver distraction therapy when pain or anxiety scores surge; randomised trials report clinically significant reductions in pain among hospitalised cancer patients using immersive VR.
- Ethical & regulatory-compliance module and transversal compliance layer. These components orchestrate informed consent workflows, enforce retention schedules, and log every data access or algorithmic recommendation, thereby operationalising GDPR and HIPAA mandates and enabling regulator auditability.
- Explainable-AI service. Each model output includes a human-readable rationale (“Neuropathy risk ↑ because activity ↓ and numbness reported ×3 days”), addressing widespread concerns about algorithmic opacity in oncology decision support.
- Interoperability & Integration framework. SMART-on-FHIR APIs export data to EHRs, pharmacy systems, and payer platforms, while multi-factor security governs authentication across stakeholders. Prior demonstrations of SMART-on-FHIR PRO apps confirm that such integration can be achieved with negligible clinician burden.
- Big-data infrastructure. De-identified, longitudinal datasets underpin continuous model retraining and health-services research, with the versioning service ensuring that each analytical result is reproducible.
7. Discussion
7.1. What Today’s Evidence Tells Us
7.2. Strengths in the Current Commercial Offer
7.3. Persistent Capability Gaps
7.4. Equity and Accessibility Issues
7.5. Data Privacy and Regulatory Considerations
7.6. Design Implications
- Adopt bidirectional SMART-on-FHIR connectors so that symptom streams, alert acknowledgements and treatment tweaks are automatically written back to the clinical record.
- Embed configurable, nurse-led escalation logic mapped to CTCAE grades, thereby aligning digital triage with existing oncology governance.
- Incorporate modular mental-health toolkits (mood diary plus short CBT or mindfulness mini-courses) and optional VR “distraction sessions” for pain/fatigue peaks.
- Deploy validated predictive models (e.g., neuropathy risk within next cycle) blended with explainable visual summaries to preserve clinician trust and user agency.
- Build for inclusivity—two-tap data entry, multi-language support, dark mode, and carer delegation; rigorous user-testing with older and socio-economically diverse survivors will be indispensable.
7.7. Limitation and Summary
8. Conclusions and Future Work
- Evidence-backed requirements are known and achievable. Multi-symptom diaries, threshold alerts, context-sensitive education, two-way messaging and user-centred usability standards already demonstrate clinical and experiential benefit across at least five RCTs and multiple cohort studies.
- Commercial offerings still miss the features that matter most to clinicians. Real-time EHR integration, predictive analytics and psychosocial modules are either absent or immature, curtailing both clinical adoption and long-term patient engagement.
- Closing these gaps is technically feasible but demands cross-sector alignment. Interoperability standards (FHIR/SMART), SaMD-level quality management and co-design with digitally marginalised groups provide a ready blueprint; the remaining barriers are organisational rather than technological.
- Build a SMART-on-FHIR pilot that streams PROs into an oncology EHR and returns automated triage advice, with nurse escalation, within a single workflow.
- Integrate a hybrid AI engine that couples a validated toxicity-prediction model with rule-based behavioural nudges, wrapped in an explainable dashboard for both patients and clinicians.
- Embed a tiered mental-health suite, combining a five-item mood screener, CBT micro-sessions and optional VR distraction, and evaluate impact on HADS and fatigue scores in a six-month mixed-methods trial.
- Conduct a digital-equity field study in partnership with community oncology centres to test proxy-access, offline caching and language-localisation features among older and rural populations.
- Prepare a regulatory pathway under UK MHRA Software Group IIb and FDA SaMD guidelines, including continuous post-market algorithm surveillance.
Author Contributions
Funding
Conflicts of Interest
References
- Jenkins, V.; Starkings, R.; Teoh, M.; May, S.; Bloomfield, D.; Zammit, C.; Elwell-Sutton, D.; Betal, D.; Finlay, J.; Nicholson, K.; et al. Patients’ views and experiences on the supported self-management/patient-initiated follow up pathway for breast cancer. Support. Care Cancer 2023, 31, 658. [Google Scholar] [CrossRef] [PubMed]
- Macmillan Cancer Support. Macmillan Cancer Support—Evaluation of the Transforming Cancer Follow-up Programme in Northern Ireland; Macmillan Cancer Support: London, UK, 2015; Available online: https://www.macmillan.org.uk/_images/transforming-cancer-follow-up-programme_tcm9-283698.pdf (accessed on 1 June 2025).
- Stewart, C. Registrations of Newly Diagnosed Cases of Breast Cancer in England in 2018, by Age Group and Gender. 2020. Available online: https://www.statista.com/statistics/312771/breast-cancer-cases-england-age/ (accessed on 1 June 2025).
- International Agency for Research on Cancer. GLOBOCAN 2020: Estimated Number of Incident Cases (United Kingdom). 2020. Available online: https://gco.iarc.fr/today/online-analysis-multi-bars?v=2020&population=826&cancer=39&statistic=5&population_group=0&ages_group%5B%5D=0&ages_group%5B%5D=17&nb_items=10&group_cancer=1&include_nmsc=1 (accessed on 1 June 2025).
- NHS Improvement. Stratified Pathways of Care: From Concept to Innovation (Executive Summary); NHS Improvement: London, UK, 2012. Available online: https://www.england.nhs.uk/improvement-hub/wp-content/uploads/sites/44/2017/11/Stratified-Pathways-of-Care.pdf (accessed on 4 March 2025).
- NHS Improvement. Innovation to Implementation: Stratified Pathways of Care for People Living with or Beyond Cancer; NHS Improvement: London, UK, 2016. Available online: https://www.england.nhs.uk/wp-content/uploads/2016/04/stratified-pathways-update.pdf (accessed on 4 March 2025).
- Calvert, M.J.; O’Connor, D.J.; Basch, E.M. Harnessing the patient voice in real-world evidence: The essential role of patient-reported outcomes. Nat. Rev. Drug Discov. 2019, 18, 731–732. [Google Scholar] [CrossRef] [PubMed]
- Fjell, M.; Langius-Eklöf, A.; Nilsson, M.; Wengström, Y.; Sundberg, K. Reduced symptom burden with the support of an interactive app during neoadjuvant chemotherapy for breast cancer: A randomized controlled trial. Breast 2020, 51, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Kuhar, C.; Cepeda, T.G.; Kovač, T.; Kukar, M.; Gorenjec, N.R. Mobile app for symptom management and associated quality of life during systemic treatment in early stage breast cancer: Nonrandomized controlled prospective cohort study. JMIR mHealth uHealth 2020, 8, e17408. [Google Scholar] [CrossRef] [PubMed]
- Öztürk, E.S.; Kutlutürkan, S. The effect of a mobile application-based symptom-monitoring process on symptom control and quality of life in breast cancer patients. Semin. Oncol. Nurs. 2021, 37, 151161. [Google Scholar] [CrossRef] [PubMed]
- Fu, T.; Ooi, S.; Reidpath, D.D. Mobile health-based mindfulness interventions to reduce psychological distress in cancer survivors: A systematic review. Psycho-Oncology 2022, 31, 601–612. [Google Scholar] [CrossRef]
- Iqbal, M.J.; Javed, Z.; Sadia, H.; Qureshi, I.A.; Irshad, A.; Ahmed, R.; Malik, K.; Raza, S.; Abbas, A.; Pezzani, R.; et al. Clinical applications of artificial intelligence and machine learning in cancer diagnosis: Looking into the future. Cancer Cell Int. 2021, 21, 270. [Google Scholar] [CrossRef] [PubMed]
- Cancer Research UK. Breast Cancer Symptoms. 2020. Available online: https://www.cancerresearchuk.org/about-cancer/breast-cancer/symptoms (accessed on 1 June 2025).
- Cancer.Net. How Cancer Affects Family Life. 2021. Available online: https://www.cancer.net/coping-with-cancer/talking-with-family-and-friends/how-cancer-affects-family-life (accessed on 1 June 2025).
- Warrington, L.; Absolom, K.; Conner, M.; Kellar, I.; Clayton, B.; Ayres, M.; Velikova, G. Electronic systems for patients to report and manage side effects of cancer treatment: Systematic review. J. Med. Internet Res. 2019, 21, e10875. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. *NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®): Breast Cancer*. Version 3.2022. Available online: https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf (accessed on 25 June 2025).
- Acreman, S.; Baker, K.; Clifton, S. Development of a non-pharmacological breathlessness management pathway. BMJ Support. Palliat. Care 2012, 2 (Suppl. 1), A63. [Google Scholar] [CrossRef]
- Petrocchi, S.; Filipponi, C.; Montagna, G.; Bonollo, M.; Pagani, O.; Meani, F. A breast cancer smartphone app to navigate the breast cancer journey: Mixed methods study. JMIR Form. Res. 2021, 5, e28668. [Google Scholar] [CrossRef] [PubMed]
- Basch, E.; Deal, A.M.; Kris, M.G.; Scher, H.I.; Hudis, C.A.; Sabbatini, P.; Rogak, L.; Bennett, A.V.; Dueck, A.C.; Atkinson, T.M.; et al. Symptom monitoring with patient-reported outcomes during routine cancer treatment: A randomized controlled trial. J. Clin. Oncol. 2016, 34, 557–565. [Google Scholar] [CrossRef] [PubMed]
- Denis, F.; Yossi, S.; Septans, A.-L.; Charron, A.; Voog, E.; Dupuis, O.; Ganem, G.; Pointreau, Y.; Letellier, C. Improving survival in patients treated for lung cancer using self-evaluated symptoms reported through a web application. Am. J. Clin. Oncol. 2017, 40, 464–469. [Google Scholar] [CrossRef] [PubMed]
- Suchodolska, G.; Senkus, E. Mobile applications for early breast-cancer chemotherapy-related symptom reporting and management: A scoping review. Cancer Treat. Rev. 2022, 105, 102364. [Google Scholar] [CrossRef] [PubMed]
- Egbring, M.; Far, E.; Roos, M.; Dietrich, M.; Brauchbar, M.; Kullak-Ublick, G.A.; Trojan, A. A mobile app to stabilize daily functional activity of breast cancer patients in collaboration with the physician: A randomized controlled clinical trial. J. Med. Internet Res. 2016, 18, e238. [Google Scholar] [CrossRef] [PubMed]
- Graetz, I.; McKillop, C.N.; Stepanski, E.; Vidal, G.A.; Anderson, J.N.; Schwartzberg, L.S. Use of a web-based app to improve breast cancer symptom management and adherence for aromatase inhibitors: A randomized controlled feasibility trial. J. Cancer Surviv. 2018, 12, 431–440. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-J.; Kim, S.-M.; Shin, H.; Jang, J.-S.; Kim, Y.-I.; Han, D.-H. A mobile game for patients with breast cancer for chemotherapy self-management and quality-of-life improvement: A randomized controlled trial. J. Med. Internet Res. 2018, 20, e273. [Google Scholar] [CrossRef] [PubMed]
- Basch, E.; Stover, A.M.; Schrag, D.; Chung, A.; Jansen, J.; Henson, S.; Carr, P.; Ginos, B.; Deal, A.; Spears, P.A.; et al. Clinical utility and user perceptions of a digital system for electronic patient-reported symptom monitoring during routine cancer care: Findings from the PRO-TECT trial. JCO Clin. Cancer Inform. 2020, 4, 947–957. [Google Scholar] [CrossRef] [PubMed]
- Terstriep, S.A.; Wacker, J.; Quinlan, C.; Pochardt, K.; Basch, E.M. Use of remote symptom monitoring with breast cancer survivors using patient-reported outcome measures in MyChart. J. Clin. Oncol. 2019, 37 (Suppl. 15), e23125. [Google Scholar] [CrossRef]
- Northern Cancer Alliance. Stratified Follow-Up. 2019. Available online: https://northerncanceralliance.nhs.uk/pathway/living-with-and-beyond-cancer/ (accessed on 4 March 2025).
- Beck, S.L.; Eaton, L.H.; Echeverria, C.; Mooney, K.H. SymptomCare@Home: Developing an integrated symptom monitoring and management system for outpatients receiving chemotherapy. Comput. Inform. Nurs. 2017, 35, 520–529. [Google Scholar] [CrossRef] [PubMed]
- Iyawa, G.E.; Herselman, M.; Botha, A. Digital health innovation ecosystems: From systematic literature review to conceptual framework. Procedia Comput. Sci. 2016, 100, 244–252. [Google Scholar] [CrossRef]
- Sama, P.R.; Eapen, Z.J.; Weinfurt, K.P.; Shah, B.R.; Schulman, K.A. An evaluation of mobile health application tools. JMIR mHealth uHealth 2014, 2, e19. [Google Scholar] [CrossRef] [PubMed]
- Harris, J.; Cheevers, K.; Armes, J. The emerging role of digital health in monitoring and supporting people living with cancer and the consequences of its treatments. Curr. Opin. Support. Palliat. Care 2018, 12, 268–275. [Google Scholar] [CrossRef] [PubMed]
- Kearney, N.; McCann, L.; Norrie, J.; Taylor, L.; Gray, P.; McGee-Lennon, M.; Sage, M.; Miller, M.; Maguire, R. Evaluation of a mobile phone-based advanced symptom-management system (ASyMS©) in the management of chemotherapy-related toxicity. Support. Care Cancer 2009, 17, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Onodera, R.; Sengoku, S. Innovation process of mHealth: An overview of FDA-approved mobile medical applications. Int. J. Med. Inform. 2018, 118, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.-T. Emerging new era of mobile health technologies. Healthc. Inform. Res. 2016, 22, 253–254. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, C.; Kelly, J.; Lehane, E.; Livingstone, V.; Cotter, B.; Butt, A.; Kelly, L.; Corrigan, M.A. Validation and assessment of a technology familiarity score in patients attending a symptomatic breast clinic. World J. Surg. 2015, 39, 2441–2449. [Google Scholar] [CrossRef] [PubMed]
- Cruz, F.; Vilela, R.; Ferreira, E.; Melo, N.; Reis, P. Evidence on the use of mobile apps during the treatment of breast cancer: Systematic review. JMIR mHealth uHealth 2019, 7, e13245. [Google Scholar] [CrossRef] [PubMed]
- Faccio, F.; Renzi, C.; Crico, C.; Kazantzaki, E.; Kondylakis, H.; Koumakis, L.; Marias, K.; Pravettoni, G. Development of an eHealth tool for cancer patients: Monitoring psycho-emotional aspects with the Family Resilience (FaRe) questionnaire. ecancermedicalscience 2018, 12, 852. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.-C.; Schmidt, R.; Schmidt, S. Mobile pain apps in chronic pain management: A systematic review of effectiveness and quality. Pain. Med. 2019, 20, 1740–1759. [Google Scholar] [CrossRef]
- NHS England. Digital Technology Assessment Criteria (DTAC). 2021. Available online: https://transform.england.nhs.uk/key-tools-and-info/digital-technology-assessment-criteria-dtac/ (accessed on 1 June 2025).
- Richards, R.; Kelley, M.; Taylor, E.; Ford, A.; Sutton, C.; Sutcliffe, P. Fitness-for-purpose of mobile stroke apps: A systematic review. JMIR mHealth uHealth 2018, 6, e9909. [Google Scholar]
- Cabestany, J.; Rodriguez-Martín, D.; Pérez, C.; Sama, A. Artificial intelligence contribution to eHealth application. In Proceedings of the 2018 25th International Conference on Mixed Design of Integrated Circuits and Systems (MIXDES), Gdynia, Poland, 21–23 June 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 15–21. [Google Scholar] [CrossRef]
- Moon, Z.; Zuchowski, M.; Moss-Morris, R.; Hunter, M.S.; Norton, S.; Hughes, L.D. Disparities in access to mobile devices and e-health literacy among breast cancer survivors. Support. Care Cancer 2022, 30, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Chen, X.; Yang, J.; Wu, Q.; Zhu, J.; Chan, S.-W. Usage patterns of a mobile breast cancer e-support program and their relationship with user characteristics: Secondary data analysis. JMIR mHealth uHealth 2020, 8, e18896. [Google Scholar] [CrossRef] [PubMed]
- Checkland, P.B. Soft systems methodology. Hum. Syst. Manag. 1989, 8, 273–289. [Google Scholar] [CrossRef]
- Fayoumi, A.; Williams, R. An integrated socio-technical enterprise modelling: A scenario of healthcare system analysis and design. J. Ind. Inf. Integr. 2021, 23, 100221. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Jongerius, C.; Russo, S.; Mazzocco, K.; Pravettoni, G. Research-tested mobile apps for breast cancer care: Systematic review. JMIR mHealth uHealth 2019, 7, e10930. [Google Scholar] [CrossRef] [PubMed]
- Cınar, D.; Karadakovan, A.; Erdoğan, A.P. Effect of mobile phone app-based training on the quality of life for women with breast cancer. Eur. J. Oncol. Nurs. 2021, 52, 101960. [Google Scholar] [CrossRef] [PubMed]
- Crafoord, M.-T.; Fjell, M.; Sundberg, K.; Nilsson, M.; Langius-Eklöf, A. Engagement in an interactive app for symptom self-management during treatment in patients with breast or prostate cancer: Mixed methods study. J. Med. Internet Res. 2020, 22, e17058. [Google Scholar] [CrossRef] [PubMed]
- Kelleher, S.A.; Winger, J.G.; Fisher, H.M.; Miller, S.N.; Reed, S.D.; Thorn, B.E.; Spring, B.; Samsa, G.P.; Majestic, C.M.; Shelby, R.A.; et al. Behavioral cancer pain intervention using videoconferencing and a mobile application for medically underserved patients: Rationale, design, and methods of a prospective multisite randomized controlled trial. Contemp. Clin. Trials 2021, 102, 106287. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.; Thompson, C.; Peterson, S.; Mandrola, J.; Beg, M.S. The future of wearable technologies and remote monitoring in health care. Am. Soc. Clin. Oncol. Educ. Book 2019, 39, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Ebert, L.; Liu, X.; Wei, D.; Chan, S.-W. Mobile breast cancer e-support program for women undergoing chemotherapy: Multicenter randomized controlled trial. JMIR mHealth uHealth 2018, 6, e104. [Google Scholar] [CrossRef] [PubMed]
- Handa, S.; Okuyama, H.; Yamamoto, H.; Nakamura, S.; Kato, Y. Effectiveness of a smartphone application as a support tool for patients undergoing breast cancer chemotherapy: A randomized controlled trial. Clin. Breast Cancer 2020, 20, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.; Liu, X.; Ng, P.; Kwok, C.; Zeng, Y.; Feuerstein, M. Breast cancer application protocol: A randomized controlled trial to evaluate a self-management app for breast cancer survivors. BMJ Open 2020, 10, e034655. [Google Scholar] [CrossRef] [PubMed]
- Lidington, E.; McGrath, S.; Noble, J.; Stanway, S.; Lucas, A.; Mohammed, K.; van der Graaf, W.; Husson, O. Evaluating a digital tool for supporting breast cancer patients: A randomized controlled trial protocol (ADAPT). Trials 2020, 21, 86. [Google Scholar] [CrossRef] [PubMed]
- Aydın, A.; Gürsoy, A. Breast cancer-related apps in Google Play and App Store: Evaluation of their functionality and quality. J. Cancer Surviv. 2023, 17, 1251–1257. [Google Scholar] [CrossRef] [PubMed]
- Sohrabei, S.; Atashi, A. The impact of mobile health on breast cancer patient’s life and treatment: A systematic review. Front. Health Inform. 2021, 10, 88. [Google Scholar] [CrossRef]
- Ahmadi, M.; Shahrokhi, S.; Zadeh, M.; Alipour, J. Development of a mobile-based self-care application for patients with breast cancer-related lymphedema in Iran. Appl. Clin. Inform. 2022, 13, 935–948. [Google Scholar] [CrossRef] [PubMed]
- Tian, Q.; Xu, M.; Yu, L.; Yang, S.; Zhang, W. The efficacy of virtual reality–based interventions in breast cancer–related symptom management. Cancer Nurs. 2022, 46, E276–E287. [Google Scholar] [CrossRef] [PubMed]
- An, H.; Kang, S.; Choi, G. Technology-based self-management interventions for women with breast cancer: A systematic review. Korean J. Women Health Nurs. 2023, 29, 160–178. [Google Scholar] [CrossRef] [PubMed]
- BorjAlilu, S.; Karbakhsh, M.; Lotfi, M.; Haghshenas, E.; Kaviani, A. Mobile applications to promote mental health among breast cancer patients: A rapid review. Arch. Breast Cancer 2023, 10, 103–113. [Google Scholar] [CrossRef]
- Jiang, L.; Xu, J.; Wu, Y.; Liu, Y.; Wang, X.; Hu, Y. Effects of the “AI-ta” mobile app with intelligent design on psychological and related symptoms of young survivors of breast cancer: Randomized controlled trial. JMIR mHealth uHealth 2024, 12, e50783. [Google Scholar] [CrossRef] [PubMed]
- Mollaoğlu, M.C.; Akın, E.B.; Mollaoğlu, M.; Karadayı, K. Investigation of symptom management and functional state of women who underwent breast cancer surgery. Rev. Da Assoc. Médica Bras. 2024, 70, e20230954. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Bae, S.; Jung, Y.; Hur, M.; Kim, J.; Jung, S. Effects of a mobile health coaching intervention on symptom experience, self-management, and quality of life in breast cancer survivors: A quasi-experimental study. Medicine 2025, 104, e41894. [Google Scholar] [CrossRef] [PubMed]
- Sikorskii, A.; Given, C.W.; Given, B.; Jeon, S.; Decker, V.; Decker, D.; Champion, V. and McCorkle, R. Symptom management for cancer patients: A trial comparing two multimodal interventions. J. Pain. Symptom Manag. 2007, 34, 253–264. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; Al-Turki, Y.; Abu-Zaid, A. Usability challenges of mobile health applications for elderly breast cancer survivors: A scoping review. Cancer Treat. Res. Commun. 2022, 33, 100570. [Google Scholar] [CrossRef]
- Langius-Eklöf, A.; Crafoord, M.-T.; Christiansen, M.; Fjell, M.; Sundberg, K. Effects of an interactive mHealth innovation for early detection of patient-reported symptom distress: Protocol for a prospective randomized controlled trial. BMC Cancer 2017, 17, 466. [Google Scholar] [CrossRef] [PubMed]
- Putranto, D.; Rochmawati, E. Mobile applications for managing symptoms of patients with cancer at home: A scoping review. Int. J. Nurs. Pract. 2020, 26, e12842. [Google Scholar] [CrossRef] [PubMed]
- Richards, R.; Kinnersley, P.; Brain, K.; McCutchan, G.; Staffurth, J.; Wood, F. Use of mobile devices to help cancer patients meet their information needs in non-inpatient settings: Systematic review. JMIR mHealth uHealth 2018, 6, e10026. [Google Scholar] [CrossRef] [PubMed]
- Richards, R.; Kinnersley, P.; Brain, K.; Staffurth, J.; Wood, F. The preferences of patients with cancer regarding apps to help meet their illness-related information needs: Qualitative interview study. JMIR mHealth uHealth 2019, 7, e14187. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, A.; Nambisan, P.; Baker, E. Mobile applications for breast cancer survivorship and self-management: A systematic review. Health Inform. J. 2020, 26, 2892–2905. [Google Scholar] [CrossRef] [PubMed]
- Harder, H.; Holm, M.; Helfricht, S.; Salander, P. Breast cancer patients’ experiences of information needs and mHealth solutions during adjuvant therapy: A qualitative interview study. Eur. J. Cancer Care 2023, 32, e13756. [Google Scholar] [CrossRef]
- Masiero, M.; Filipponi, C.; Fragale, E.; Pizzoli, S.F.M.; Munzone, E.; Milani, A.; Guido, L.; Guardamagna, V.; Marceglia, S.; Prandin, R.; et al. Support for chronic pain management for breast cancer survivors through novel digital health ecosystems: Pilot usability study of the PainRELife mobile app. JMIR Form. Res. 2024, 8, e51021. [Google Scholar] [CrossRef] [PubMed]
- NHS Transformation Directorate. Breast Cancer App to Offer Patients Personalised Medical Support Throughout Their Treatment; NHS England: London, UK, 2021. Available online: https://transform.england.nhs.uk/key-tools-and-info/digital-playbooks/cancer-digital-playbook/breast-cancer-app-to-offer-patients-personalised-medical-support-throughout-their-treatment/ (accessed on 4 March 2025).
- Houghton, L.; Howland, R.; McDonald, J. Mobilizing breast cancer prevention research through smartphone apps: A systematic review of the literature. Front. Public Health 2019, 7, 298. [Google Scholar] [CrossRef] [PubMed]
- Seven, M.; Bagcivan, G.; Pasalak, S.I.; Oz, G.; Aydin, Y.; Selcukbiricik, F. Experiences of breast cancer survivors during the COVID-19 pandemic: A qualitative study. Support. Care Cancer 2021, 29, 6481–6493. [Google Scholar] [CrossRef] [PubMed]
- Warner, J.L.; Prasad, I.; Bennett, M.; Arniella, M.; Beeghly-Fadiel, A.; Mandl, K.D.; Alterovitz, G. SMART Cancer Navigator: A framework for implementing ASCO workshop recommendations to enable precision cancer medicine. JCO Precis. Oncol. 2018, 2, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Baseman, J.; Kottke, T.; Bauer, B. Security and privacy considerations in mobile health: A review. J. Healthc. Inform. Res. 2017, 1, 11–29. [Google Scholar]
- Georgiou, M. Cost of Mobile App Maintenance in 2020 and Why it’s Needed. 2020. Available online: https://www.imaginovation.net/blog/importance-mobile-app-maintenance-cost/ (accessed on 1 June 2025).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
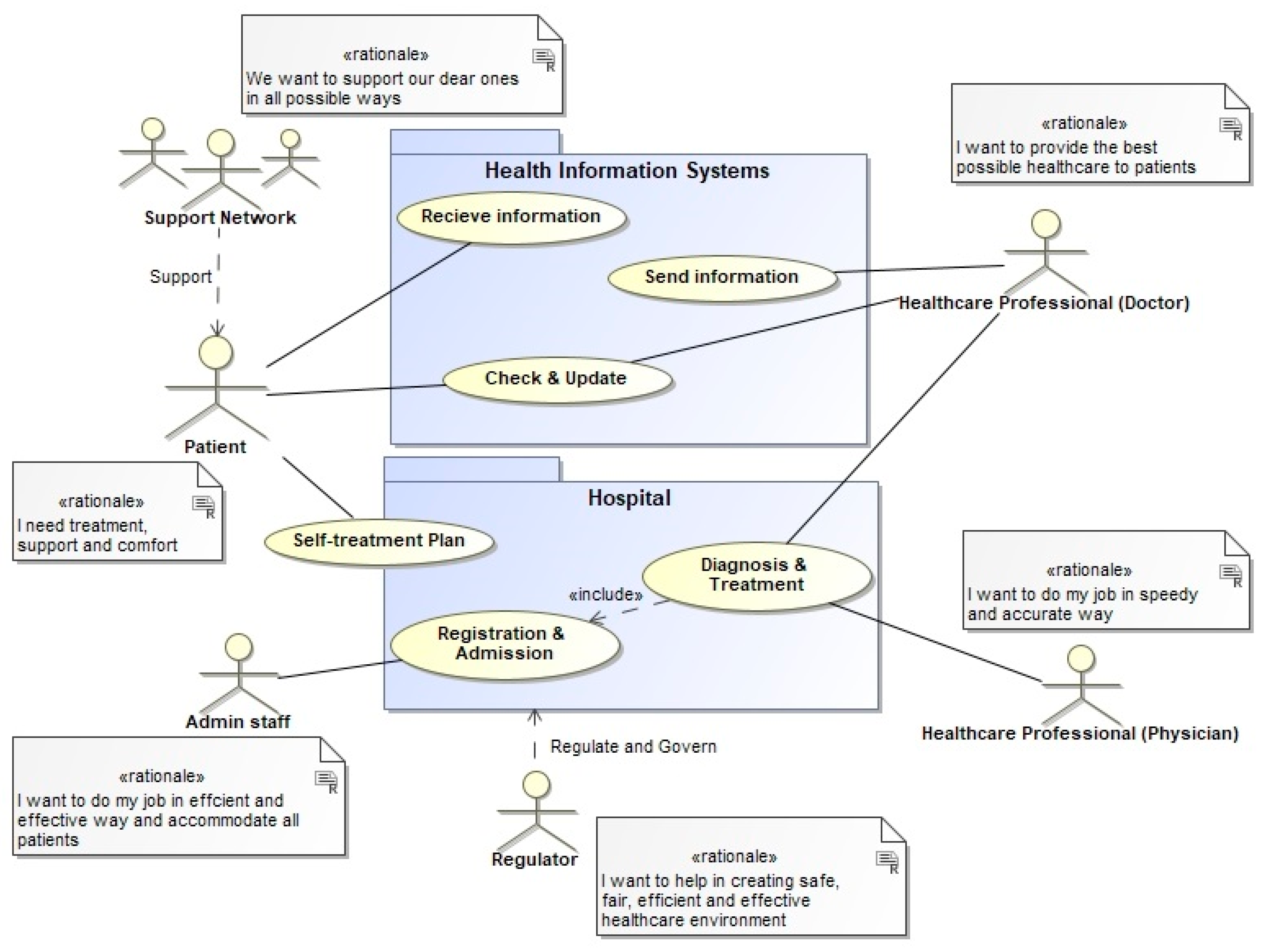
| CUSTOMER | PATIENTS AND THEIR FAMILIES |
|---|---|
| ACTOR | Breast cancer multi-disciplinary treatment team: doctors, physicians, regulator, app owner, app administrator |
| TRANSFORMATION PROCESS | Provide information, diagnostic investigations, treatments, managing symptoms, emotional support |
| WORLDVIEW | A belief that multidisciplinary and patient self-managing app enables better diagnosis, treatment, care management and support that lead to improved patient outcomes and cost reduction |
| OWNER | NHS or third-party health services provider |
| ENVIRONMENT | Knowledge base, clinical guidelines, physical and technological constraints, patient health records, patient target times |
| PERFORMANCE MEASURES | Effectiveness: goal-orientated, data completeness, data accuracy, usability. Efficiency: Cost-saving, timesaving, error-free, availability |
| # | Study (Year, Country) | Design & Sample | App/Platform | Mobile Design Highlights | Primary Outcome Category |
|---|---|---|---|---|---|
| 1 | Egbring et al. [22] (CH) | 3-arm RCT, N = 139 adjuvant chemo | (custom) | Daily CTCAE diary; physician-review arm | Functional status stabilised; more grade ≥ 2 toxicities detected |
| 2 | Graetz et al. [23] (US) | Multi-centre RCT, N = 120 | SymptomCare@Home | PRO-CTCAE diary → EHR alerts; colour dashboard | Faster nurse response, ↓ grade ≥ 2 nausea/fatigue |
| 3 | Kim et al. [24] (KR) | RCT, N = 76 metastatic | Chemo-Game | Gamified education, quizzes, med log | ↑ adherence; ↓ nausea, neuropathy |
| 4 | Zhu et al. [53] (CN) | Multi-centre RCT, N = 114 | Breast-Cancer e-Support | “Learn–Discuss–Ask” forums; nurse moderation | ↑ self-efficacy, ↓ symptom interference |
| 5 | Handa et al. [54] (JP) | RCT, N = 102 | BPSS | Cycle-based logging; shared record | 1868 AEs surfaced; no QoL change |
| 6 | Fjell et al. [8] (SE) | RCT, N = 149 neo-adjuvant | Interaktor | Real-time nurse SMS alerts; self-care library | ↓ nausea, distress; ↑ emotional QoL |
| 7 | Kuhar et al. [9] (SI) | Prospective cohort, N = 91 | mPRO Mamma | 50-symptom diary; tailored tips; reminders | ↑ global QoL week 1; ↓ pain |
| 8 | Cheng et al. [55] (HK/AU) | RCT protocol | B-CApp | Self-management CBT modules; nurse chat | (Protocol) |
| 9 | Lidington et al. [56] (UK) | RCT protocol | OWise | NHS-linked clinician portal; FHIR export | (Protocol) |
| 10 | Cınar et al. [49] (TR) | Parallel-group RCT, N = 80 | e-Symptom Tracker | Twice-daily diary; push tips | ↓ MSAS distress; ↑ QoL |
| 11 | Aydın & Gürsoy [57] (Global audit) | App-store survey | – | MARS quality & functionality scoring | 37% apps lacked evidence-base |
| 12 | Sohrabei & Atashi [58] (IR) | Systematic review | – | – | mHealth ↓ distress, ↑ empowerment |
| 13 | Ahmadi et al. [59] (IR) | Development + usability, N = 40 | BCRL Self-Care | Lymph-exercise videos; AI reminders | System Usability = 84/100 |
| 14 | Tian et al. [60] (CN) | Network meta-analysis | – | VR modules (pain, anxiety) | VR ↓ pain & fatigue vs. control |
| 15 | An et al. [61] (KR) | Systematic review (15 trials) | – | – | Highlighted need for mental-health & clinician feedback |
| 16 | BorjAlilu et al. [62] (IR) | Rapid review | – | – | Emphasised AI for mental-health support |
| 17 | Jiang et al. [63] (CN) | RCT, N = 102 young survivors | AI-TA | Intelligent follow-up; mood check-ins | ↓ distress & fatigue; ↑ self-efficacy |
| 18 | Mollaoğlu et al. [64] (TR) | X-sectional app-use study | – | Post-surgery symptom diary | Linked app use ↔ better function |
| 19 | Park et al. [65] (KR) | Quasi-exp., N = 88 survivors | mHealth-Coach | Behaviour-change AI; video chat | ↓ symptom cluster; ↑ QoL & self-management |
| ID | Requirement | Weight | Studies Supporting (n) | Representative Refs |
|---|---|---|---|---|
| FR1 | Multi-symptom diary with severity scale | 3 | 15 | Egbring [22]; Kuhar [9]; Jiang [64] |
| FR2 | Threshold-based patient & clinician alerts/triage | 3 | 9 | Graetz [23]; Fjell [8]; Park [34] |
| FR3 | Context-specific self-care library (text, video) | 3 | 14 | Kuhar [9]; Ahmadi [59] |
| FR4 | Two-way messaging/clinician portal | 2 | 8 | Cheng [55]; Lidington [56] |
| FR5 | Symptom-trend visualisation dashboards | 2 | 7 | Crafoord [50]; OWise |
| FR6 | VR-based symptom distraction | 1 | 3 | Tian [60] |
| FR7 | Mental-health modules (mood diary, CBT, mindfulness) | 2 | 6 | Jiang [63]; Park [34]; BorjAlilu [62] |
| FR8 | AI-driven coaching/prediction | 1 | 4 | Ahmadi [59]; Park [34] |
| NFR1 | Usability & accessibility (≤2 taps per entry, large UI, multi-language) | 3 | 14 | Cınar [49]; Aydın [57] |
| NFR2 | Privacy & security (GDPR/HIPAA, encryption) | 3 | 11 | Lidington [56]; Sohrabei [58] |
| NFR3 | Interoperability (HL7 FHIR, PDF export, wearables) | 2 | 8 | Graetz [23]; OWise |
| NFR4 | Reliability & data backup | 2 | 5 | Egbring [22]; Handa [54] |
| NFR5 | Regulatory sustainability (DTAC, FDA SaMD) | 1 | 4 | Lidington [56]; An [61] |
| App | Total/140 | Strengths | Key Shortfalls |
|---|---|---|---|
| OWise | 103 | Best-in-class symptom diary; clinician portal with HL7 FHIR export, real-time dashboards (OWise US); rich education library; high usability; GDPR audit passed. | No VR (FR6); AI analytics limited to trend plots (FR8 = 2); mental-health content basic (FR7 = 2). |
| Outcomes4Me | 92 | AI-driven guideline translation and treatment matcher (Apple); colour-coded symptom graphs (Outcomes4Me); genetics/clinical-trial finder; community forum. | No clinician alert loop (FR2 = 1); data export only via PDF (NFR3 = 2); mental-health tools limited to curated articles (FR7 = 2). |
| Wave Health/chemoWave | 72 | Multimodal diary (symptoms, mood, activity); correlation engine uses AI to link behaviours and symptom severity (Google Play); medication reminders; user-defined goals. | No direct clinician connectivity; education library shallow; lacks VR, advanced mental-health programmes and formal security disclosures. |
| Breast Cancer Manager | 55 | Daily journal with slider input and trend charts; medication scheduler; photo upload for visible symptoms; optional provider-view account (Apple). | Alert logic rudimentary; no AI or mental-health modules; interoperability relies on manual data sharing; interface dated (usability = 3). |
| CancerAid | 34 | “Champions” feature lets users share data with family/friends for support (Medibank); library of survivor stories; basic symptom log. | Missing clinician portal, alerts, mental-health content, AI insights; low diary flexibility; no EHR integration; lowest overall security transparency. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, X.; Fayoumi, A.; Winter, E.; Najdawi, A. Design Requirements of Breast Cancer Symptom-Management Apps. Informatics 2025, 12, 72. https://doi.org/10.3390/informatics12030072
Huang X, Fayoumi A, Winter E, Najdawi A. Design Requirements of Breast Cancer Symptom-Management Apps. Informatics. 2025; 12(3):72. https://doi.org/10.3390/informatics12030072
Chicago/Turabian StyleHuang, Xinyi, Amjad Fayoumi, Emily Winter, and Anas Najdawi. 2025. "Design Requirements of Breast Cancer Symptom-Management Apps" Informatics 12, no. 3: 72. https://doi.org/10.3390/informatics12030072
APA StyleHuang, X., Fayoumi, A., Winter, E., & Najdawi, A. (2025). Design Requirements of Breast Cancer Symptom-Management Apps. Informatics, 12(3), 72. https://doi.org/10.3390/informatics12030072