
The Mappability of Clinical Real-World Data of Patients with Melanoma to Oncological Fast Healthcare Interoperability Resources (FHIR) Profiles: A Single-Center Interoperability Study

 , , , , , and
, , , , , and
Abstract
1. Introduction
1.1. Background and Significance
1.2. Objectives
2. Materials and Methods
2.1. Real-World Electronic Health Record (EHR) Data
2.2. Data Extraction, Pre-Processing, and Validation
2.3. Data Modeling
2.4. FHIR Profile Selection
2.5. Data Model Comparison and Metrics
3. Results
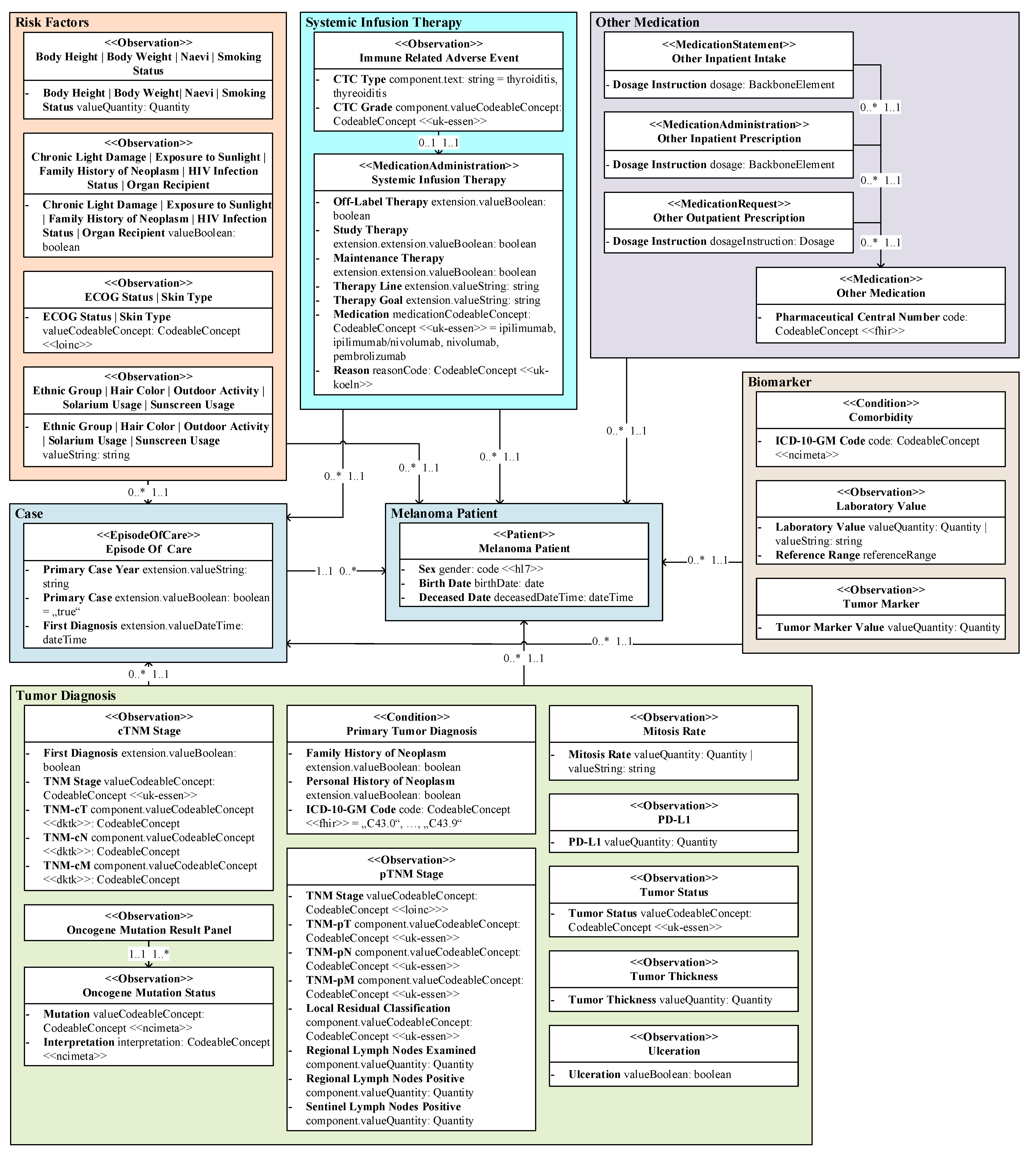
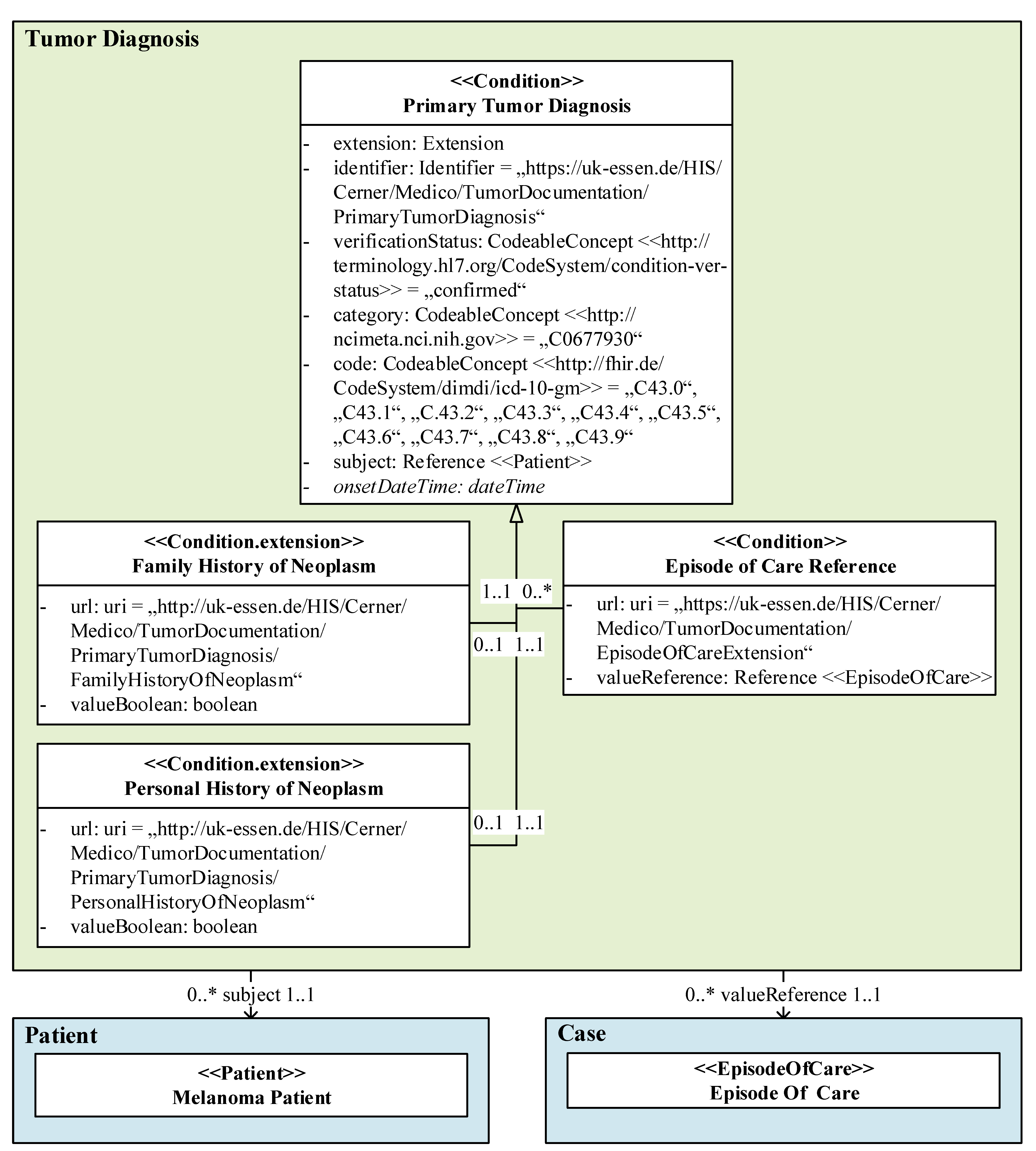
3.1. Real-World Data Model
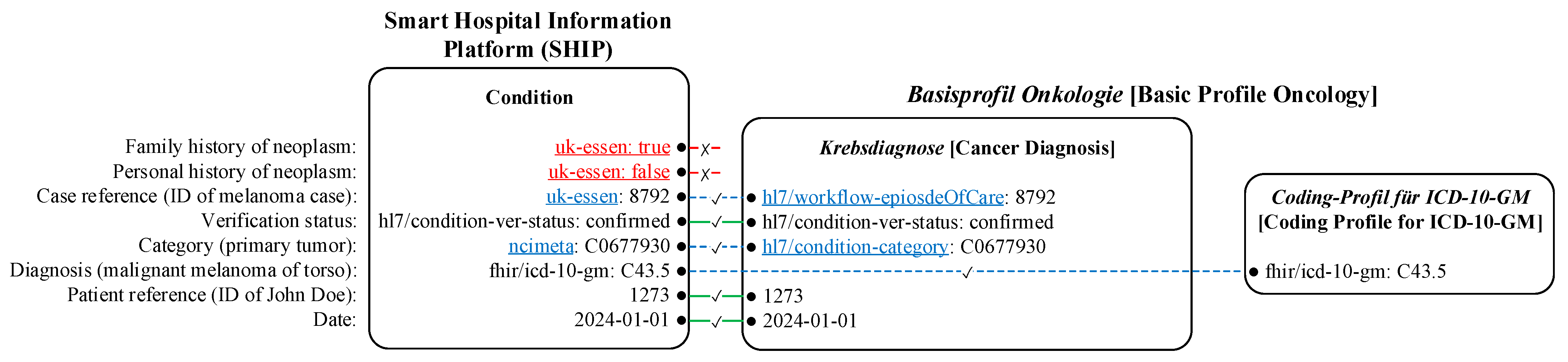
3.2. Applicability of Standardized Data Model

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feature | Real-World Data | HL7 Basisprofil Onkologie [Basic Profile Oncology] | |||
|---|---|---|---|---|---|
| (Type, Mapping Level) | Resource.Element | Type = Value | Profile or Extension | Resource.Element | Type = Value |
| Family history of neoplasm (C, N) * | Condition | ||||
| .extension | Extension | ||||
| .extension.url | uri = uk-essen | ||||
| .extension. valueBoolean | boolean | ||||
| Personal history of neoplasm (C, N) * | Condition | ||||
| .extension | Extension | ||||
| .extension.url | uri = uk-essen | ||||
| .extension. valueBoolean | boolean | ||||
| Episode of care reference (R, MA) | Condition | Condition | |||
| .extension | Extension | Krebsdiagnose [Cancer Diagnosis] | .extension:Fall | Extension | |
| Extension | |||||
| .extension.url | uri = uk-essen | Krebsdiagnose [Cancer Diagnosis] | .url | uri = hl7/workflow- episodeOfCare | |
| .extension. valueReference | Reference (EpisodeOfCare) | Episode of Care | .valueReference | Reference (EpisodeOfCare) | |
| Verification (A, Y) | Condition | Condition | |||
| .verification Status | CodeableConcept (hl7/conditionver- status) = “confirmed” | Krebsdiagnose [Cancer Diagnosis] | .verification Status | CodeableConcept (hl7/conditionver- status) = “confirmed” | |
| Category of primary neoplasm (A, MA) | Condition | Condition | |||
| .category | CodeableConcept (ncimeta) = “C0677930” | Krebsdiagnose [Cancer Diagnosis] | .category | CodeableConcept(hl7/condition-category) | |
| ICD-10- GM code (C, MA) | Condition | Condition | |||
| .code | CodeableConcept (fhir/icd-10-gm) = C43.0–C43.9 | Krebsdiagnose [Cancer Diagnosis] | .code.coding | fhir/CodingICD10 GM | |
| Data Type | |||||
| Coding-Profil für ICD-10-GM [Coding Profile for ICD-10-GM] | .system | uri = fhir/icd-10-gm | |||
| Coding-Profil für ICD-10-GM [Coding Profile for ICD-10-GM] | .code | code | |||
| Patient reference (R, Y) | Condition | Condition | |||
| .subject | Reference(Patient) | Krebsdiagnose [Cancer Diagnosis] | .subject | Reference(Patient) | |
| Date (A, Y) | Condition | Condition | |||
| .onsetDateTime | dateTime | Krebsdiagnose [Cancer Diagnosis] | .onsetDateTime | dateTime | |
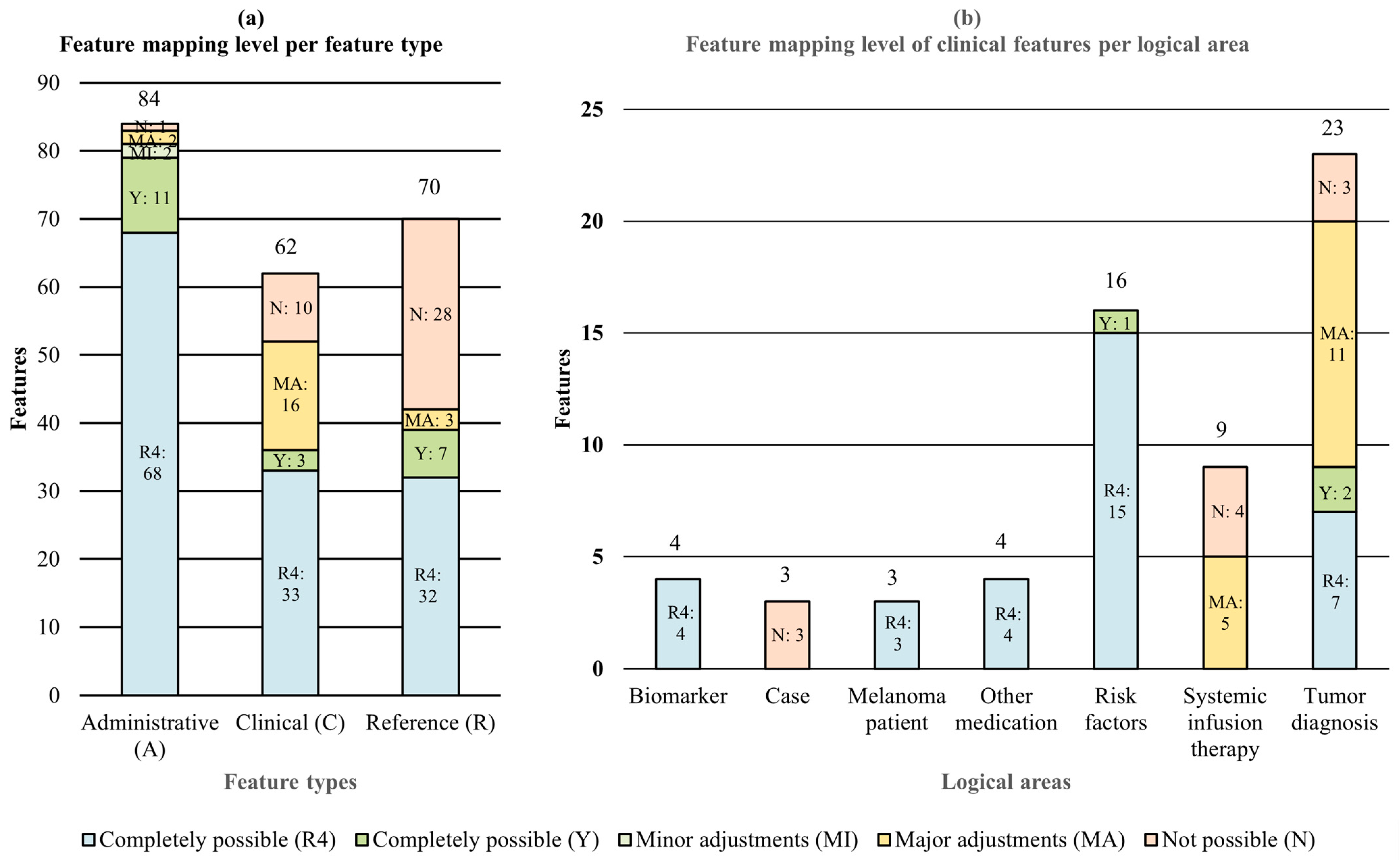
3.3. Mappability Metrics
| Feature Type | Mapping Level | Total (n = 212) | ||||
|---|---|---|---|---|---|---|
| To Basisprofil Onkologie [Basic Profile Oncology] | To Standard R4 | To Both | ||||
| Completely Possible (Y) | Minor Adjustments (MI) | Major Adjustments (MA) | Completely Possible (R4) | Not Possible (N) | ||
| Administrative (A) | 11/13.10% | 2/2.38% | 2/2.38% | 68/80.95% | 1/1.19% | 84/38.89% |
| Clinical (C) | 3/4.76% | 0/0.00% | 16/25.40% | 33/52.38% | 10/15.87% | 63/28.70% |
| Reference (R) | 7/10.00% | 0/0.00% | 3/4.29% | 32/45.71% | 28/40.00% | 70/32.41% |
| Total (n = 212) | 21/9.72% | 2/0.93% | 21/9.72% | 129/61.57% | 39/18.06% | 216/100.00% |
3.4. New Features
3.5. Mandatory Elements
4. Discussion
4.1. Data Model Creation
4.2. Granularity of Mapping Level
4.3. The Effects of the Further Development of Fast Healthcare Interoperability Resources (FHIR)
4.4. Applicability of Oncology Standard for Tumor-Specific Melanoma
4.5. Strengths
4.6. Limitations
4.7. Implications and Future Work
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ADT | Arbeitsgemeinschaft Deutscher Tumorzentren [Association of German Tumor Centers] |
| CDM | Common Data Model |
| CDS | Core Data Set |
| cTNM | Clinical TNM |
| DiGA | Digitale Gesundheitsanwendungen [Digital Health Applications] |
| EHR | Electronic Health Record |
| ePA | elektronische Patientenakte [Personal Health Record] |
| FHIR | Fast Healthcare Interoperability Resources |
| GEKID | Gesellschaft der epidemiologischen Krebsregister in Deutschland [Association of Population-Based Cancer Registries in Germany] |
| gematik | Nationale Agentur für Digitale Medizin [National Agency for Digital Medicine] |
| GOLD | German OncoLogical Data Standard |
| HL7 | Health Level 7 |
| irAE | Immune-Related Adverse Event |
| ISiK | Informationstechnische Systeme in Krankenhäusern [Information Technology in Hospital] |
| LOINC | Logical Observation Identifiers Names and Codes |
| MII | Medizininformatik Initiative [Medical Informatics Initiative] |
| MIO | Medizinische Informationsobjekte [Medical Information Object] |
| NCIm | National Cancer Institute meta thesaurus |
| nNGM | Nationales Netzwerk Genomische Medizin Lungenkrebs [German National Network Genomic Medicine Lung Cancer] |
| oBDS | Bundeseinheitlicher Onkologischer Basisdatensatz [German Uniform Basic Oncology Data Set] |
| OMOP | Observational Medical Outcomes Partnership |
| pTNM | Pathological TNM |
| SHIP | Smart Hospital Information Platform |
| SNOMED CT | SNOMED Clinical Terms |
| UML | Unified Modeling Language |
| URL | Uniform Resource Locator |
References
- Vorisek, C.N.; Lehne, M.; Klopfenstein, S.A.I.; Mayer, P.J.; Bartschke, A.; Haese, T.; Thun, S. Fast Healthcare Interoperability Resources (FHIR) for Interoperability in Health Research: Systematic Review. JMIR Med. Inform. 2022, 10, e35724. [Google Scholar] [CrossRef] [PubMed]
- Bosca, D.; Moner, D.; Maldonado, J.A.; Robles, M. Combining Archetypes with Fast Health Interoperability Resources in Future-proof Health Information Systems. In Digital Healthcare Empowering Europeans; IOS Press: Amsterdam, Netherlands, 2015; Volume 210, pp. 180–184. [Google Scholar]
- FHIR Overview. Architects. Available online: https://hl7.org/fhir/R4/overview-arch.html (accessed on 6 May 2024).
- Medizinische Informationsobjekte. Available online: https://mio.kbv.de/site/mio#tab-Rund+um+die+MIOs (accessed on 6 May 2024).
- Weber, S.; Heitmann, K.U. Interoperabilität im Gesundheitswesen: Auch für digitale Gesundheitsanwendungen (DiGA) verordnet. Bundesgesundheitsbl 2021, 64, 1262–1268. [Google Scholar] [CrossRef] [PubMed]
- Interoperabilität dank ISiK. Available online: https://fachportal.gematik.de/informationen-fuer/isik (accessed on 6 May 2024).
- Ciortuz, G.; Wiedekopf, J.; Fudickar, S. Integration von Wearables und Nutzung von digitalen Biomarkern zur Diagnostik und Therapie im Gesundheitswesen. In Health Data Management; Henke, V., Hülsken, G., Schneider, H., Varghese, J., Eds.; Springer: Wiesbaden, Germany, 2024; pp. 323–336. ISBN 978-3-658-43235-5. [Google Scholar]
- Semler, S.C.; Wissing, F.; Heyder, R. German Medical Informatics Initiative. Methods Inf. Med. 2018, 57, e50–e56. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.D.; Roda, D.; Yap, T.A. Strategies for modern biomarker and drug development in oncology. J. Hematol. Oncol. 2014, 7, 70. [Google Scholar] [CrossRef] [PubMed]
- Pflugfelder, A.; Kochs, C.; Blum, A.; Capellaro, M.; Czeschik, C.; Dettenborn, T.; Dill, D.; Dippel, E.; Eigentler, T.; Feyer, P.; et al. Malignant melanoma S3-guideline “diagnosis, therapy and follow-up of melanoma”. J. Dtsch. Dermatol. Ges. 2013, 11 (Suppl. S6), 1–116. [Google Scholar] [CrossRef] [PubMed]
- Deppenwiese, N.; Delpy, P.; Lambarki, M.; Lablans, M. ADT2FHIR—A Tool for Converting ADT/GEKID Oncology Data to HL7 FHIR Resources. In German Medical Data Sciences 2021: Digital Medicine: Recognize–Understand–Heal; IOS Press: Amsterdam, The Netherlands, 2021; Volume 283, pp. 104–110. [Google Scholar] [CrossRef]
- González-Castro, L.; Cal-González, V.M.; Del Fiol, G.; López-Nores, M. CASIDE: A data model for interoperable cancer survivorship information based on FHIR. J. Biomed. Inform. 2021, 124, 103953. [Google Scholar] [CrossRef] [PubMed]
- Oeppert, L.; Hartz, T.; Wehner, K.; Schrader, T.; Meier, J. FHIR-Datenmodell zur Übermittlung von Tumordaten zwischen Krebsregistern und IQTIG. GMS Med. Inform. Biom. Und Epidemiol. 2021, 17, Doc17. [Google Scholar] [CrossRef]
- Lambarki, M.; Kern, J.; Croft, D.; Engels, C.; Deppenwiese, N.; Kerscher, A.; Kiel, A.; Palm, S.; Lablans, M. Oncology on FHIR: A Data Model for Distributed Cancer Research. In German Medical Data Sciences: Bringing Data to Life; IOS Press: Amsterdam, The Netherlands, 2021; Volume 278, pp. 203–210. [Google Scholar] [CrossRef]
- Digitalisierung: Mit Einem Konsentierten Datenformat gegen den Krebs. Available online: https://vision-zero-oncology.de/projekte-arbeitsgruppe-digitalisierung.php (accessed on 6 May 2024).
- Project NCCN Chemotherapy Order Templates. Available online: https://simplifier.net/NCCNChemotherapyOrde (accessed on 6 May 2024).
- Peng, Y.; Henke, E.; Reinecke, I.; Zoch, M.; Sedlmayr, M.; Bathelt, F. An ETL-process design for data harmonization to participate in international research with German real-world data based on FHIR and OMOP CDM. Int. J. Med. Inform. 2023, 169, 104925. [Google Scholar] [CrossRef]
- Peng, Y.; Nassirian, A.; Ahmadi, N.; Sedlmayr, M.; Bathelt, F. Towards the Representation of Genomic Data in HL7 FHIR and OMOP CDM. In German Medical Data Sciences 2021: Digital Medicine: Recognize—Understand—Heal; IOS Press: Amsterdam, The Netherlands, 2021; Volume 283, pp. 86–94. [Google Scholar] [CrossRef]
- Stellmach, C.; Sass, J.; Auber, B.; Boeker, M.; Wienker, T.; Heidel, A.J.; Benary, M.; Schumacher, S.; Ossowski, S.; Klauschen, F.; et al. Creation of a structured molecular genomics report for Germany as a local adaption of HL7’s Genomic Reporting Implementation Guide. J. Am. Med. Inform. Assoc. 2023, 30, 1179–1189. [Google Scholar] [CrossRef] [PubMed]
- Holweg, F.; Achenbach, S.; Deppenwiese, N.; Gaede, L.; Prokosch, H.-U. Towards a FHIR-Based Data Model for Coronary Angiography Observations. In Healthcare of the Future 2022; IOS Press: Amsterdam, The Netherlands, 2022; Volume 292, pp. 96–99. [Google Scholar] [CrossRef]
- Gundler, C.; Zhu, Q.R.; Trübe, L.; Dadkhah, A.; Gutowski, T.; Rosch, M.; Langebrake, C.; Nürnberg, S.; Baehr, M.; Ückert, F. A Unified Data Architecture for Assessing Motor Symptoms in Parkinson’s Disease. In German Medical Data Sciences 2023—Science. Close to People; IOS Press: Amsterdam, The Netherlands, 2023; Volume 307, pp. 22–30. [Google Scholar] [CrossRef]
- Project of HL7 Deutschland e.V.: Basisprofil Onkologie. Available online: https://simplifier.net/BasisprofileOnkologie (accessed on 6 May 2024).
- Project GOLD—German OncoLogical Data Standard. Available online: https://simplifier.net/GOLD---German-OncoLogical-Data-Standard (accessed on 6 May 2024).
- Project of Medizininformatik Initiative: Medizininformatik Initiative—Modul Onkologie. Available online: https://simplifier.net/MedizininformatikInitiative-ModulOnkologie (accessed on 6 May 2024).
- Whiteman, D.C.; Green, A.C.; Olsen, C.M. The Growing Burden of Invasive Melanoma: Projections of Incidence Rates and Numbers of New Cases in Six Susceptible Populations through 2031. J. Investig. Dermatol. 2016, 136, 1161–1171. [Google Scholar] [CrossRef] [PubMed]
- Zimmer, L.; Goldinger, S.M.; Hofmann, L.; Loquai, C.; Ugurel, S.; Thomas, I.; Schmidgen, M.I.; Gutzmer, R.; Utikal, J.S.; Göppner, D.; et al. Neurological, respiratory, musculoskeletal, cardiac and ocular side-effects of anti-PD-1 therapy. Eur. J. Cancer 2016, 60, 210–225. [Google Scholar] [CrossRef] [PubMed]
- Kähler, K.C.; Hassel, J.C.; Heinzerling, L.; Loquai, C.; Mössner, R.; Ugurel, S.; Zimmer, L.; Gutzmer, R. Management of side effects of immune checkpoint blockade by anti-CTLA-4 and anti-PD-1 antibodies in metastatic melanoma. JDDG J. Der Dtsch. Dermatol. Ges. 2016, 14, 662–681. [Google Scholar] [CrossRef] [PubMed]
- Leitlinienprogramm Onkologie (Deutsche Krebsgesellschaft, Deutsche Krebshilfe, AWMF): Diagnostik, Therapie und Nachsorge des Melanoms, Langversion 3.3, 2020, AWMF Registernummer: 032/024OL. Available online: http://www.leitlinienprogramm-onkologie.de/leitlinien/melanom/ (accessed on 6 May 2024).
- Kähler, K.C.; Hassel, J.C.; Heinzerling, L.; Loquai, C.; Thoms, K.-M.; Ugurel, S.; Zimmer, L.; Gutzmer, R. Side effect management during immune checkpoint blockade using CTLA-4 and PD-1 antibodies for metastatic melanoma—An update. JDDG J. Der Dtsch. Dermatol. Ges. 2020, 18, 582–609. [Google Scholar] [CrossRef] [PubMed]
- Baldini, G.; Arzideh, K.; Trienes, J.; Schlötterer, J.; Seifert, C.; Nensa, F. Aufbau einer Automatisierten NLP-Pipeline zur De-Identifikation Klinischer Dokumente; German Medical Science GMS Publishing House: Düsseldorf, Germany, 2023. [Google Scholar] [CrossRef]
- Hosch, R.; Baldini, G.; Parmar, V.; Borys, K.; Koitka, S.; Engelke, M.; Arzideh, K.; Ulrich, M.; Nensa, F. FHIR-PYrate: A data science friendly Python package to query FHIR servers. BMC Health Serv. Res. 2023, 23, 734. [Google Scholar] [CrossRef] [PubMed]
- Benson, T.; Grieve, G. FHIR Resources. In Principles of Health Interoperability; Benson, T., Grieve, G., Eds.; Springer International Publishing: Cham, Switzerland, 2016; pp. 361–379. ISBN 978-3-319-30368-0. [Google Scholar]
- Ulrich, H.; Behrend, P.; Wiedekopf, J.; Drenkhahn, C.; Kock-Schoppenhauer, A.-K.; Ingenerf, J. Hands on the Medical Informatics Initiative Core Data Set—Lessons Learned from Converting the MIMIC-IV. In German Medical Data Sciences 2021: Digital Medicine: Recognize—Understand—Heal; IOS Press: Amsterdam, The Netherlands, 2021; Volume 283, pp. 119–126. [Google Scholar] [CrossRef]
- Medical Informatics Initiative Germany. Basic Modules of the MII Core Data Set. Available online: https://www.medizininformatik-initiative.de/en/basic-modules-mii-core-data-set (accessed on 6 May 2024).
- FHIR Specification. Publication (Version) History. Available online: https://hl7.org/fhir/directory.html (accessed on 6 May 2024).
- FHIR Specification DSTU 1—Resource Observation—Content. Available online: https://hl7.org/fhir/DSTU1/observation.html (accessed on 6 May 2024).
- HL7 FHIR Release 4—Resource Observation—Content. Available online: https://hl7.org/fhir/R4/observation.html (accessed on 6 May 2024).

| Characteristic | Oncological FHIR Profile for Germany | ||
|---|---|---|---|
| Organization | HL7 Deutschland [Germany] | Medizininformatik Initiative [Medical Informatics Initiative] | Vision Zero |
| Profile | Basisprofil Onkologie [Basic Profile Oncology] | Medizininformatik Initiative [Medical Informatics Initiative]—Modul Onkologie [Module Oncology] | GOLD—German OncoLogical Data Standard |
| Simplifier | https://simplifier.net/BasisprofileOnkologie (acessed on 24 June 2024) | https://simplifier.net/MedizininformatikInitiative-ModulOnkologie (acessed on 24 June 2024) | https://simplifier.net/gold---german-oncological-data-standard (acessed on 24 June 2024) |
| Start | 2020 | 2022 | 2022 |
| FHIR | R4 | R4 | R4 |
| Profiles n (status) | 16 (active) | 34 (draft) | 1 (active), 18 (draft) |
| Value sets n (status) | 33 (active) | 50 (draft) | 35 (draft) |
| Code systems n (status) | 7 (active) | 35 (draft) | 1 (draft) |
| Extension n (status) | 9 (active) | 9 (draft) | 6 (draft) |
| Connection(s) | Basis for:
| Based on:
| Combines:
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Swoboda, J.; Albert, M.; Beckmann, C.L.; Lodde, G.C.; Livingstone, E.; Nensa, F.; Schadendorf, D.; Böckmann, B. The Mappability of Clinical Real-World Data of Patients with Melanoma to Oncological Fast Healthcare Interoperability Resources (FHIR) Profiles: A Single-Center Interoperability Study. Informatics 2024, 11, 42. https://doi.org/10.3390/informatics11030042
Swoboda J, Albert M, Beckmann CL, Lodde GC, Livingstone E, Nensa F, Schadendorf D, Böckmann B. The Mappability of Clinical Real-World Data of Patients with Melanoma to Oncological Fast Healthcare Interoperability Resources (FHIR) Profiles: A Single-Center Interoperability Study. Informatics. 2024; 11(3):42. https://doi.org/10.3390/informatics11030042
Chicago/Turabian StyleSwoboda, Jessica, Moritz Albert, Catharina Lena Beckmann, Georg Christian Lodde, Elisabeth Livingstone, Felix Nensa, Dirk Schadendorf, and Britta Böckmann. 2024. "The Mappability of Clinical Real-World Data of Patients with Melanoma to Oncological Fast Healthcare Interoperability Resources (FHIR) Profiles: A Single-Center Interoperability Study" Informatics 11, no. 3: 42. https://doi.org/10.3390/informatics11030042
APA StyleSwoboda, J., Albert, M., Beckmann, C. L., Lodde, G. C., Livingstone, E., Nensa, F., Schadendorf, D., & Böckmann, B. (2024). The Mappability of Clinical Real-World Data of Patients with Melanoma to Oncological Fast Healthcare Interoperability Resources (FHIR) Profiles: A Single-Center Interoperability Study. Informatics, 11(3), 42. https://doi.org/10.3390/informatics11030042