
Executive Functions and Rapid Automatized Naming: A New Tele-Rehabilitation Approach in Children with Language and Learning Disorders

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Assessment Materials
2.3. Preschool Protocol
- −
- Digit span forward (BVN 5–11 [50]): it is a task in which the child is asked to repeat, in the same order, an increasing series of numbers.
- −
- High-frequency bisyllabic word list repetition test [51]: this is a test to be performed on the PC, which allows for assessing the auditory-visual working memory. The child is presented with audios, referring to concrete objects and after listening a series of figures are presented on the screen; the child will have to indicate the figures that s/he has heard, in order of presentation. The exercise is made up of a series of 5 audios each, in which the number of objects named in each series increases progressively, starting from 2 elements; if the child indicates correctly at least 3 out of 5 trials, s/he goes on to the next series, increasing the number of named figures. The auditory-visual memory span is given by the number of objects correctly named, within a series, in which the named figures are at least 3.
- −
- Inhibition (NEPSY-II, [52]): it is a test in which shapes are presented (squares and circles or arrows in different directions) and the child must name the shapes, first correctly (conditions A—naming) and then invert them inhibiting automatic responses (condition B—inhibition) and finally following different criteria of naming (condition C—switching). At preschool age, only conditions A-B are administered, calculating time spent and errors/self-corrections made.
- −
- Verbal fluency (NEPSY-II, [52]): the child is given a semantic category or phonological cue and is asked to produce as many words as possible in one minute.
- −
- Sustained attention (AS) test (Leiter-3, [53]): it is a “barrage” test in which there are animal figures that the child must identify and cross out in 30 s; it is divided into 4 parts and the number of targets found is measured.
- −
- Ranette (BIA, [54]): it is an activity that requires auditory sustained attention skills, selective attention and inhibition of motor response. It is a go/no-go type task, in which the child must inhibit the motor act, required in the presence of a specific go sound, when the sound presented is slightly different from the previous one (no-go sound); the number of correct answers is scored.
- −
- Test of rapid automatized naming of colours and figures (RAN, [55]): the test consists of matrices of figures and colours, two matrices for each condition and the child must name them aloud, in left-right order (such as reading), noting the time taken and errors/self-corrections made.
- −
- BRIEF-P [56]: it is a questionnaire that allows evaluating in depth the EFs through parent perception, to detect the behaviour of children between 2 and 5 years; it provides scorings for 5 clinical scales: inhibition, shift, emotion regulation, working memory and planning/organisation, besides a global composite score.
2.4. School Protocol
- −
- Digit span forward and backward (BVN 5–11 [50]): in addition to the forward test, in which the child is asked to repeat in the same order increasing series of numbers, the backward version requested the child to repeat in reverse order with respect to the presentation.
- −
- Listening span test elementary (LSTE [58]): the test consists of a series of elementary sentences, at the lexical, syntactic and meaning level, for the assessment of working memory in children aged 8–11 years. Sentences are organised in 4 blocks, each preceded by an example. The task is to judge the semantic correctness of each sentence, i.e., whether it is true or false, and to remember the last word of each sentence heard. The elements investigated in this test are the number of last words remembered, the possible intrusions, the inversions of order in remembering the words and finally errors of judgement.
- −
- Inhibition and verbal fluency (NEPSY-II, [52]): these subtests were the same proposed for pre-schoolers. For Inhibition, in addition to conditions A-B, condition C (switching) is also administered, always examining time spent and errors/self-corrections made.
- −
- Test SD4 (PRCR-2, [59]): the test required searching a sequence of letters. It is presented as matrices of sequences of letters, progressively less spaced between them, in which the child must mark on the paper all the strings “TOC” that identifies; the clinician investigates the time taken, the errors made and the number of targets found.
- −
- Test of rapid automatized naming of figures and numbers (RAN, [55]): the same as the preschool protocol, but with figures and numbers as stimuli.
- −
- Text reading and comprehension (ALCE, [60]): text reading (text 1 in the T0 assessment and text 2 in the T1 assessment), assessing reading speed in syllables per second and error rate, together with comprehension of the text read (through ten open questions) were analysed.
- −
- Words dictation (DDE-2, [61]): a word dictation test has been included, in which the number of errors made is investigated.
- −
- BRIEF-2 [56]: like the preschool protocol, a questionnaire that allows evaluating in depth the EF through parent perception.
2.5. Tele-Rehabilitation Program
- −
- the processing capacity of the system, dictated by the temporal rate at which stimuli are presented (presentation time and inter-stimuli time) and the complexity of instructions;
- −
- the integration of modalities, enhancing visual-verbal processing, going to modify the parameters of the activity, reducing or enlarging the visual and verbal load, manipulating figure size and/or word length and complexity;
- −
- the components of EF involved, thanks to the gradual progression of each exercise, which allows moving from the involvement of simpler to more complex components: first exercises work mainly on inhibition, then intervenes the working memory and finally an integration of the two EF until the introduction of cognitive flexibility.
2.6. Procedure
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- de Oliveira Rosa, V.; Rosa Franco, A.; Abrahão Salum Júnior, G.; Moreira-Maia, C.R.; Wagner, F.; Simioni, A.; de Fraga Bassotto, C.; Moritz, G.R.; Schaffer Aguzzoli, C.; Buchweitz, A.; et al. Effects of Computerized Cognitive Training as Add-on Treatment to Stimulants in ADHD: A Pilot FMRI Study. Brain Imaging Behav. 2020, 14, 1933–1944. [Google Scholar] [CrossRef] [PubMed]
- Wiest, D.J.; Wong, E.H.; Bacon, J.M.; Rosales, K.P.; Wiest, G.M. The Effectiveness of Computerized Cognitive Training on Working Memory in a School Setting. Appl. Cogn. Psychol. 2020, 34, 465–471. [Google Scholar] [CrossRef]
- Gathercole, S.E.; Dunning, D.L.; Holmes, J.; Norris, D. Corrigendum to ‘Working Memory Training Involves Learning New Skills’. J. Mem. Lang. 2019, 106, 203. [Google Scholar] [CrossRef]
- Rabiner, D.L.; Murray, D.W.; Skinner, A.T.; Malone, P.S. A Randomized Trial of Two Promising Computer-Based Interventions for Students with Attention Difficulties. J. Abnorm. Child. Psychol. 2010, 38, 131–142. [Google Scholar] [CrossRef]
- Jones, J.S.; Milton, F.; Mostazir, M.; Adlam, A.R. The Academic Outcomes of Working Memory and Metacognitive Strategy Training in Children: A Double-Blind Randomized Controlled Trial. Dev. Sci. 2020, 23, e12870. [Google Scholar] [CrossRef]
- Harder, L.; Hernandez, A.; Hague, C.; Neumann, J.; McCreary, M.; Cullum, C.M.; Greenberg, B. Home-Based Pediatric Teleneuropsychology: A Validation Study. Arch. Clin. Neuropsychol. 2020, 35, 1266–1275. [Google Scholar] [CrossRef]
- Kronenberger, W.G.; Montgomery, C.J.; Henning, S.C.; Ditmars, A.; Johnson, C.A.; Herbert, C.J.; Pisoni, D.B. Remote Assessment of Verbal Memory in Youth with Cochlear Implants during the COVID-19 Pandemic. Am. J. Speech. Lang. Pathol. 2021, 30, 740–747. [Google Scholar] [CrossRef]
- Ragbeer, S.N.; Augustine, E.F.; Mink, J.W.; Thatcher, A.R.; Vierhile, A.E.; Adams, H.R. Remote Assessment of Cognitive Function in Juvenile Neuronal Ceroid Lipofuscinosis (Batten Disease): A Pilot Study of Feasibility and Reliability. J. Child. Neurol. 2016, 31, 481–487. [Google Scholar] [CrossRef]
- Stain, H.J.; Payne, K.; Thienel, R.; Michie, P.; Carr, V.; Kelly, B. The Feasibility of Videoconferencing for Neuropsychological Assessments of Rural Youth Experiencing Early Psychosis. J. Telemed. Telecare 2011, 17, 328–331. [Google Scholar] [CrossRef]
- Werfel, K.L.; Grey, B.; Johnson, M.; Brooks, M.; Cooper, E.; Reynolds, G.; Deutchki, E.; Vachio, M.; Lund, E.A. Transitioning Speech-Language Assessment to a Virtual Environment: Lessons Learned from the ELLA Study. Lang. Speech Hear. Serv. Sch. 2021, 52, 769–775. [Google Scholar] [CrossRef]
- Maresca, G.; De Cola, M.C.; Caliri, S.; De Luca, R.; Manuli, A.; Scarcella, I.; Silvestri, G.; Bramanti, P.; Torrisi, M.; Calabrò, R.S.; et al. Sicilian Teleneurology Group. Moving towards Novel Multidisciplinary Approaches for Improving Elderly Quality of Life: The Emerging Role of Telemedicine in Sicily. J. Telemed. Telecare 2019, 25, 318–324. [Google Scholar] [CrossRef] [PubMed]
- Sarfo, F.S.; Ulasavets, U.; Opare-Sem, O.K.; Ovbiagele, B. Tele-Rehabilitation after Stroke: An Updated Systematic Review of the Literature. J. Stroke Cerebrovasc. Dis. 2018, 27, 2306–2318. [Google Scholar] [CrossRef] [PubMed]
- Corti, C.; Oldrati, V.; Oprandi, M.C.; Ferrari, E.; Poggi, G.; Borgatti, R.; Urgesi, C.; Bardoni, A. Remote Technology-Based Training Programs for Children with Acquired Brain Injury: A Systematic Review and a Meta-Analytic Exploration. Behav. Neurol. 2019, 2019, 1346987. [Google Scholar] [CrossRef] [PubMed]
- Agostini, M.; Moja, L.; Banzi, R.; Pistotti, V.; Tonin, P.; Venneri, A.; Turolla, A. Telerehabilitation and Recovery of Motor Function: A Systematic Review and Meta-Analysis. J. Telemed. Telecare 2015, 21, 202–213. [Google Scholar] [CrossRef] [PubMed]
- Cardullo, S.; Gamberini, L.; Milan, S.; Mapelli, D. Rehabilitation Tool: A Pilot Study on A New Neuropsychological Interactive Training System. Stud. Health Technol. Inform. 2015, 219, 168–173. [Google Scholar] [PubMed]
- Coleman, J.J.; Frymark, T.; Franceschini, N.M.; Theodoros, D.G. Assessment and Treatment of Cognition and Communication Skills in Adults with Acquired Brain Injury via Telepractice: A Systematic Review. Am. J. Speech. Lang. Pathol. 2015, 24, 295–315. [Google Scholar] [CrossRef] [PubMed]
- Solana, J.; Cáceres, C.; García-Molina, A.; Opisso, E.; Roig, T.; Tormos, J.M.; Gómez, E.J. Improving Brain Injury Cognitive Rehabilitation by Personalized Telerehabilitation Services: Guttmann Neuropersonal Trainer. IEEE J. Biomed. Health Inform. 2015, 19, 124–131. [Google Scholar] [CrossRef]
- Casalini, C.; Mazzotti, S. Problematiche e Prospettive Dell’intervento a Distanza Nei Disturbi Del Neurosviluppo. Psicol. Clin. Dello Svilupp. 2021, 3, 389–416. [Google Scholar] [CrossRef]
- Theodoros, D.G. Telerehabilitation for Service Delivery in Speech-Language Pathology. J. Telemed. Telecare 2008, 14, 221–224. [Google Scholar] [CrossRef]
- Caso, V.; Federico, A. No Lockdown for Neurological Diseases during COVID-19 Pandemic Infection. Neurol. Sci. Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol. 2020, 41, 999–1001. [Google Scholar]
- Dayal, D. We urgently need guidelines for managing COVID-19 in children with comorbidities. Acta Paediatr. 2020, 109, 1497–1498. [Google Scholar] [CrossRef] [PubMed]
- Sarti, D.; De Salvatore, M.; Gazzola, S.; Pantaleoni, C.; Granocchio, E. So Far so Close: An Insight into Smart Working and Telehealth Reorganization of a Language and Learning Disorders Service in Milan during COVID-19 Pandemic. Neurol. Sci. 2020, 41, 1659–1662. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association Publishing: Washington, DC, USA, 2015. [Google Scholar]
- Huc-Chabrolle, M.; Barthez, M.A.; Tripi, G.; Barth’el’emy, C.; Bonnet-Brilhault, F. Psychocognitive and Psychiatric Disorders Associated with Developmental Dyslexia: A Clinical and Scientific Issue. Encephale 2010, 36, 172–179. [Google Scholar] [CrossRef] [PubMed]
- Catts, H.W.; Adlof, S.M.; Hogan, T.P.; Weismer, S.E. Are Specific Language Impairment and Dyslexia Distinct Disorders? J. Speech Lang. Hear. Res. 2005, 48, 1378–1396. [Google Scholar] [CrossRef]
- Angelelli, P.; Marinelli, C.V.; Iaia, M.; Putzolu, A.; Gasperini, F.; Brizzolara, D.; Chilosi, A.M. Spelling Impairments in Italian Dyslexic Children with and without a History of Early Language Delay. Are There Any Differences? Front. Psychol. 2016, 7, 527. [Google Scholar] [CrossRef]
- Brizzolara, D.; Chilosi, A.; Cipriani, P.; Di Filippo, G.; Gasperini, F.; Mazzotti, S.; Pecini, C.; Zoccolotti, P. Do Phonologic and Rapid Automatized Naming Deficits Differentially Affect Dyslexic Children with and without a History of Language Delay? A Study of Italian Dyslexic Children. Cogn. Behav. Neurol. 2006, 19, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Brizzolara, D.; Gasperini, F.; Pfanner, L.; Cristofani, P.; Casalini, C.; Chilosi, A.M. Long-Term Reading and Spelling Outcome in Italian Adolescents with a History of Specific Language Impairment. Cortex 2011, 47, 955–973. [Google Scholar] [CrossRef]
- Chilosi, A.M.; Brizzolara, D.; Lami, L.; Pizzoli, C.; Gasperini, F.; Pecini, C.; Cipriani, P.; Zoccolotti, P. Reading and Spelling Disabilities in Children with and without a History of Early Language Delay: A Neuropsychological and Linguistic Study. Child. Neuropsychol. 2009, 15, 582–604. [Google Scholar] [CrossRef]
- Pecini, C.; Biagi, L.; Brizzolara, D.; Cipriani, P.; Di Lieto, M.C.; Guzzetta, A.; Tosetti, M.; Chilosi, A.M. How Many Functional Brains in Developmental Dyslexia? When the History of Language Delay Makes the Difference. Cogn. Behav. Neurol. 2011, 24, 85–92. [Google Scholar] [CrossRef]
- Tucci, R.; Savoia, V.; Bertolo, L.; Vio, C.; Tressoldi, P.E. Efficacy and Efficiency Outcomes of a Training to Ameliorate Developmental Dyslexia Using the Online Software Reading Trainer®. BPA-Appl. Psychol. Bull. 2015, 63, 53–60. [Google Scholar]
- Bonacina, S.; Cancer, A.; Lanzi, P.L.; Lorusso, M.L.; Antonietti, A. Improving Reading Skills in Students with Dyslexia: Efficacy of a Sublexical Training with Rhythmic Background. Front. Psychol. 2015, 6, 1510. [Google Scholar] [CrossRef] [PubMed]
- Gori, S.; Facoetti, A. Perceptual Learning as a Possible New Approach for Remediation and Prevention of Developmental Dyslexia. Vision Res. 2014, 99, 78–87. [Google Scholar] [CrossRef] [PubMed]
- van Bergen, E.; van der Leij, A.; de Jong, P.F. The Intergenerational Multiple Deficit Model and the Case of Dyslexia. Front. Hum. Neurosci. 2014, 8, 346. [Google Scholar] [CrossRef] [PubMed]
- Zampolini, M.; Todeschini, E.; Bernabeu Guitart, M.; Hermens, H.; Ilsbroukx, S.; Macellari, V.; Magni, R.; Rogante, M.; Scattareggia Marchese, S.; Vollenbroek, M.; et al. Tele-Rehabilitation: Present and Future. Ann. Ist. Super. Sanita 2008, 44, 125–134. [Google Scholar]
- Pecini, C.; Spoglianti, S.; Michetti, S.; Bonetti, S.; Di Lieto, M.C.; Gasperini, F.; Cristofani, P.; Bozza, M.; Brizzolara, D.; Casalini, C.; et al. Telerehabilitation in Developmental Dyslexia: Methods of Implementation and Expected Results. Minerva Pediatr. 2018, 70, 529–538. [Google Scholar] [CrossRef]
- Tressoldi, P.E.; Brembati, F.; Donini, R.; Iozzino, R.; Vio, C. Treatment of Dyslexia in a Regular Orthography: Efficacy and Efficiency (Cost-Effectiveness), Comparison between Home vs Clinic-Based Treatments. Eur. J. Psychol. 2012, 8, 375–390. [Google Scholar] [CrossRef]
- Maggio, M.G.; Foti Cuzzola, M.; Calatozzo, P.; Marchese, D.; Andaloro, A.; Calabrò, R.S. Improving Cognitive Functions in Adolescents with Learning Difficulties: A Feasibility Study on the Potential Use of Telerehabilitation during COVID-19 Pandemic in Italy. J. Adolesc. 2021, 89, 194–202. [Google Scholar] [CrossRef]
- Holmes, J.; Gathercole, S.E. Taking Working Memory Training from the Laboratory into Schools. Educ. Psychol. 2014, 34, 440–450. [Google Scholar] [CrossRef]
- Johann, V.E.; Karbach, J. Effects of Game-Based and Standard Executive Control Training on Cognitive and Academic Abilities in Elementary School Children. Dev. Sci. 2020, 23, e12866. [Google Scholar] [CrossRef]
- Dahlin, K.I.E. Working Memory Training and the Effect on Mathematical Achievement in Children with Attention Deficits and Special Needs. J. Educ. Learn. 2013, 2, 118–133. [Google Scholar] [CrossRef][Green Version]
- Schwaighofer, M.; Fischer, F.; Bühner, M. Does Working Memory Training Transfer? A Meta-Analysis Including Training Conditions as Moderators. Educ. Psychol. 2015, 50, 138–166. [Google Scholar] [CrossRef]
- Diamond, A. Executive Functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef] [PubMed]
- Holmes, J.; Gathercole, S.E.; Dunning, D.L. Adaptive Training Leads to Sustained Enhancement of Poor Working Memory in Children. Dev. Sci. 2009, 12, F9–F15. [Google Scholar] [CrossRef] [PubMed]
- Consensus Conferenfe. DSA. Documento D’intesa, PARCC. 2011. Available online: www.lineeguidadsa.it (accessed on 12 March 2022).
- Casalini, C.; Pecini, C.; Zaccaria, S.; Orsolini, L.; Brizzolara, D. Telepsychology’ and Specific Learning Disabilities in COVID-19 Time: A Critical Review. Psicol. Clin. Dello Svilupp. 2020, 24, 361–374. [Google Scholar]
- Peijnenborgh, J.C.A.W.; Hurks, P.M.; Aldenkamp, A.P.; Vles, J.S.H.; Hendriksen, J.G.M. Efficacy of Working Memory Training in Children and Adolescents with Learning Disabilities: A Review Study and Meta-Analysis. Neuropsychol. Rehabil. 2016, 26, 645–672. [Google Scholar] [CrossRef]
- MemoRAN in RIDInet Platform, Anastatis, Bologna, Italy. Available online: https://www.anastasis.it/ridinet/ (accessed on 15 April 2019).
- Wechsler, D. WPPSI-III Administration and Scoring Manual; Psychological Corporation: San Antonio, TX, USA, 2002. [Google Scholar]
- Bisiacchi, P.S.; Cendron, M.; Gugliotta, M.; Tressoldi, P.E.; Vio, C. Batteria Di Valutazione Neuropsicologica per l’Età Evolutiva. BNV 5-11; Erickson: Trento, Italy, 2005. [Google Scholar]
- IRCCS Stella Maris. High Frequency Bisyllabic Word List Repetition Test, 2017; in press.
- Korkman, M.; Kirk, U.; Kemp, S. NEPSY-II. Italian Adaptation; Giunti OS: Firenze, Italy, 2011. [Google Scholar]
- Roid, G.H.; Koch, C. Leiter-3: Nonverbal Cognitive and Neuropsychological Assessment. In Handbook of Nonverbal Assessment; Springer International Publishing: Cham, Switzerland, 2017; pp. 127–150. [Google Scholar]
- Marzocchi, G.M.; Re, A.M.; Cornoldi, C. BIA. Batteria Italiana per l’ADHID per La Valutazione Dei Bambini Con Deficit Di Attenzione-Iperattività; Edizioni Erickson: Trento, Italy, 2010. [Google Scholar]
- De Luca, M.; Di Filippo, G.; Judica, A.; Spinelli, D.; Zoccolotti, P. Test. Di Denominazione Rapida e Ricerca Visiva Di Colori, Figure e Numeri; IRCCS Fondazione Santa Lucia: Roma, Italy, 2005. [Google Scholar]
- Gioia, G.A.; Isquith, P.K.; Guy, S.C.; Kenworthy, L. BRIEF2—Behavior Rating Inventory of Executive Function; Hogrefe: Firenze, Itlay, 2009. [Google Scholar]
- Wechsler, D. Wechsler Intelligence Scale for Children—Fourth Edition Technical and Interpretive Manual; Psychological Corporation: San Antonio, TX, USA, 2003. [Google Scholar]
- Palladino, P. Uno Strumento per Esaminare La Memoria Di Lavoro Verbale in Bambini Di Scuola Elementare: Taratura e Validità. Psicol. Clin. Dello Svilupp. 2005, 9, 129–150. [Google Scholar]
- Cornoldi, C.; Miato, L.; Molin, A.; Poli, S. PRCR—2/2009 Prove Di Prerequisito per La Diagnosi Delle Difficoltà Della Lettura e Scrittura; Giunti OS: Firenze, Italy, 2009. [Google Scholar]
- Bonifacci, P.; Tobia, V.; Lami, L.; Snowling, M. ALCE. Assessment Di Lettura e Comprensione per l’Età Evolutiva; Hogrefe: Göttingen, Germany, 2014. [Google Scholar]
- Sartori, G.; Job, R.; Tressoldi, P.E. DDE-2. Batteria per La Valutazione Della Dislessia e Della Disortografia Evolutiva (Battery for the Assessment of Developmental Dyslexia and Dysorthographia); Giunti OS: Firenze, Italy, 2007. [Google Scholar]
- Diamond, A.; Lee, K. Interventions Shown to Aid Executive Function Development in Children 4 to 12 Years Old. Science 2011, 333, 959–964. [Google Scholar] [CrossRef]
- Di Lieto, M.C.; Brovedani, M.C.; Pecini, P.; Chilosi, C.; Belmonti, A.M.; Fabbro, V.; Cioni, G. Spastic Diplegia in Preterm-Born Children: Executive Function Impairment and Neuroanatomical Correlates. Res. Dev. Disabil. 2017, 61, 116–126. [Google Scholar] [CrossRef]
- Di Lieto, M.C.; Inguaggiato, M.C.; Castro, E.; Cecchi, E.; Cioni, F.; Dell’omo, G.; Dario, P. Educational Robotics Intervention on Executive Functions in Preschool Children: A Pilot Study. Comput. Hum. Behav. 2017, 71, 16–23. [Google Scholar] [CrossRef]
- Cohen, D.K. Teaching Practice: Plus Ça Change; Michigan State University: East Lansing, MI, USA, 1988. [Google Scholar]
- McCue, M.; Fairman, A.; Pramuka, M. Enhancing Quality of Life through Telerehabilitation. Phys. Med. Rehabil. Clin. N. Am. 2010, 21, 195–205. [Google Scholar] [CrossRef]
- Ghidoni, E.; Angelini, D. La Dislessia Negli Adolescenti e Negli Adulti. Ann. Della Pubblica Istr. 2011, 4, 119–127. [Google Scholar]
- Spencer-Smith, M.; Klingberg, T. Correction: Benefits of a Working Memory Training Program for Inattention in Daily Life: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0167373. [Google Scholar] [CrossRef] [PubMed]
- Flaugnacco, E.; Lopez, L.; Terribili, C.; Montico, M.; Zoia, S.; Schön, D. Music Training Increases Phonological Awareness and Reading Skills in Developmental Dyslexia: A Randomized Control Trial. PLoS ONE 2015, 10, e0138715. [Google Scholar] [CrossRef] [PubMed]
- Zoccolotti, P.; de Jong, P.F.; Spinelli, D. Editorial: Understanding Developmental Dyslexia: Linking Perceptual and Cognitive Deficits to Reading Processes. Front. Hum. Neurosci. 2016, 10, 140. [Google Scholar] [CrossRef] [PubMed]
- De Cola, M.C.; Maresca, G.; D’Aleo, G.; Carnazza, L.; Giliberto, S.; Maggio, M.G.; Bramanti, A.; Calabrò, R.S. Teleassistance for Frail Elderly People: A Usability and Customer Satisfaction Study. Geriatr. Nurs. 2020, 41, 463–467. [Google Scholar] [CrossRef]
- Manuli, A.; Maggio, M.G.; Tripoli, D.; Gullì, M.; Cannavò, A.; La Rosa, G.; Sciarrone, F.; Avena, G.; Calabrò, R.S. Patients’ Perspective and Usability of Innovation Technology in a New Rehabilitation Pathway: An Exploratory Study in Patients with Multiple Sclerosis. Mult. Scler. Relat. Disord. 2020, 44, 102312. [Google Scholar] [CrossRef]
- Norton, E.S.; Wolf, M. Rapid Automatized Naming (RAN) and Reading Fluency: Implications for Understanding and Treatment of Reading Disabilities. Annu. Rev. Psychol. 2012, 63, 427–452. [Google Scholar] [CrossRef]
- Resquín, F.; Cuesta Gómez, A.; Gonzalez-Vargas, J.; Brunetti, F.; Torricelli, D.; Molina Rueda, F.; Cano de la Cuerda, R.; Miangolarra, J.C.; Pons, J.L. Hybrid Robotic Systems for Upper Limb Rehabilitation after Stroke: A Review. Med. Eng. Phys. 2016, 38, 1279–1288. [Google Scholar] [CrossRef]
- Chacko, A.; Uderman, J.; Feirsen, N.; Bedard, A.C.; Marks, D. Learning and Cognitive Disorders: Multidisciplinary Treatment Approaches. Child. Adolesc. Psychiatr. Clin. N. Am. 2013, 22, 457–477. [Google Scholar] [CrossRef]
- Klingberg, T.; Fernell, E.; Olesen, P.J.; Johnson, M.; Gustafsson, P.; Dahlström, K. Computerized Training of Working Memory in Children with ADHD-a Randomized, Controlled Trial. J. Am. Acad. Child. Adolesc. Psychiatry 2005, 44, 177–186. [Google Scholar] [CrossRef]
- Kuusisaari, H. Teachers at the Zone of Proximal Development: Collaboration Promoting or Hindering the Development Process. Teach. Teach. Educ. 2014, 43, 46–57. [Google Scholar] [CrossRef]
- Thorell, L.B.; Lindqvist, S.; Bergman Nutley, S.; Bohlin, G.; Klingberg, T. Training and Transfer Effects of Executive Functions in Preschool Children. Dev. Sci. 2009, 12, 106–113. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| N | M (Months) | SD | MAX | MIN | |
|---|---|---|---|---|---|
| AGE | 42 | 103 | 42 | 137 | 59 |
| IRP | 38 | 99.47 | 12.81 | 132 | 78 |
| IQ | 37 | 90.43 | 10.53 | 108 | 70 |
| Exercise 1. Inversion | This is an inhibition exercise that requires reversing the naming of two stimuli, out of five that are presented; there is a preview phase, in which the child sees which stimuli have to be named correctly and which to reverse. The parent should report errors in the application, each time the child omits or misses a name and each time s/he misses the reversal task. |
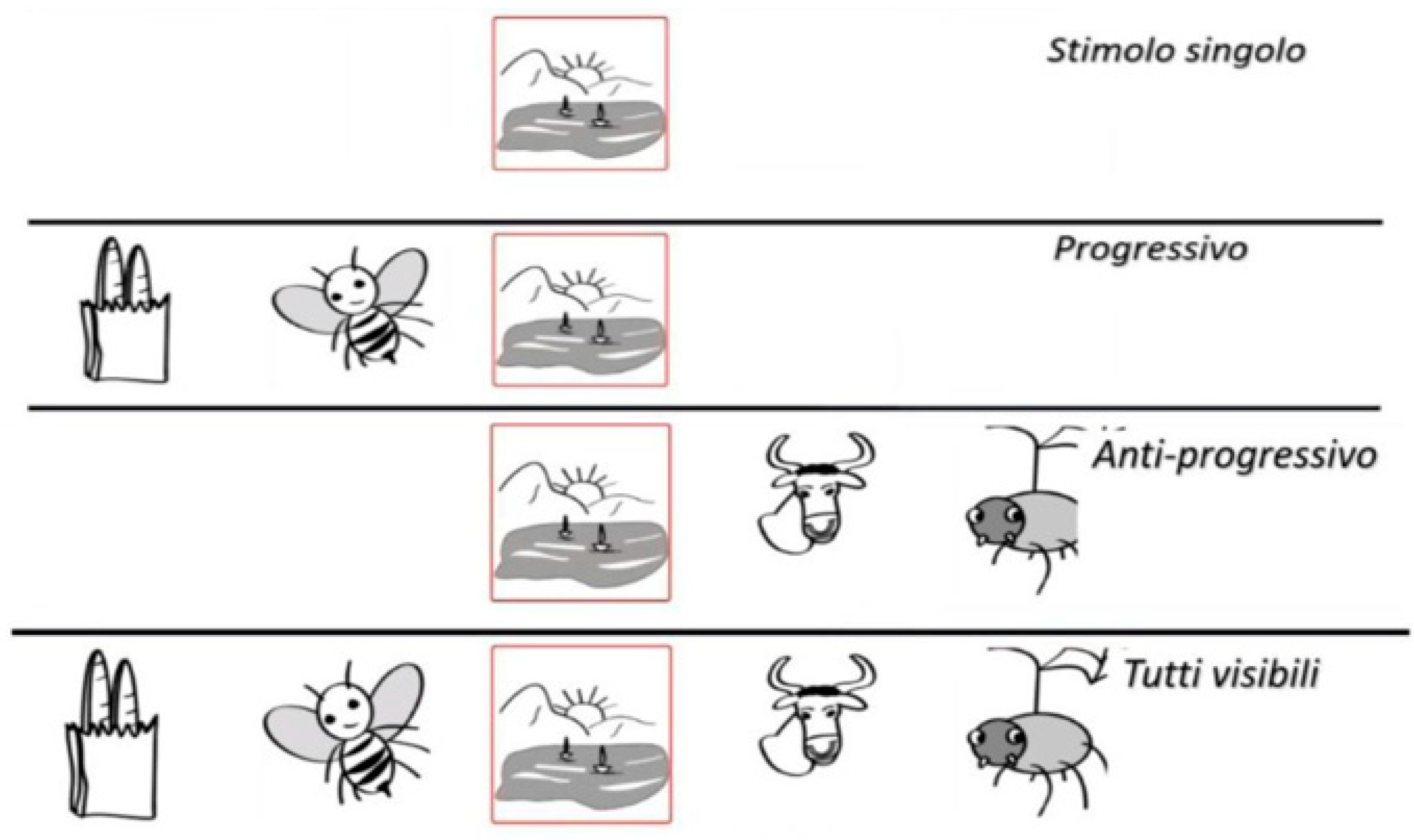
| Exercise 2. Cluster | In this exercise, several figures are presented or highlighted at the same time, within a cluster defined by a yellow rectangle; the child is asked to name only the stimuli highlighted by the red square (within the cluster). We can define this exercise as an activity of attentional focusing with shifting of visual and spatial attention. With each omission or error in naming, the parent will report the error on the application. |
| Exercise 3. Ran variable time | This task requires the child to quickly name all the stimuli s/he sees; the peculiarity is that the figures are presented with a very variable exposure and inter-stimuli time: sometimes very slow, sometimes very fast, sometimes medium. Therefore, the child will have to inhibit his own automatic rhythm and adapt to that imposed by the outside world, that is, by the advance. With each omission or error in naming, the parent will report the error on the application. |
| Exercise 4. Action | This is a dual-task activity, in which the child will have to name the figures as they are, as well as having to perform an action at the same time as the naming, for two specific marked stimuli. The aim is to encourage integration between a visual-verbal task and a motor control task, increasing the complexity of the processing/response mode. An error is marked both when a naming is omitted and the action is not performed (e.g., clapping). |
| Exercise 5. 1-back | It is a working memory exercise: the child must name the figures as they are; however, should not name the figure surrounded by the red square but the previous stimulus, that after being appeared will be replaced by a red dot; it is also important that the clinician tells the child to follow the rhythm of the visual cue. With each omission or error in 1-back naming, the parent will report the error on the application. |
| Exercise 6. Inversion and action | In this exercise, a complex dual task is proposed: among the five stimuli presented, two will have inverted naming, two others will be associated with an action, and the last stimulus will require simple naming as presented. Error may result from inaccuracies in naming or actions. |
| Exercise 7. Silence and action | This is another dual-task exercise but also includes an inhibition component: silence is required for one stimulus, silence is required for another stimulus at the same time as the tapping action on the table, and simple naming is required for the other three stimuli. The error comes from not respecting silence or respecting it for stimuli that are not required, as well as making mistakes in the execution of actions. |
| Exercise 8. 2-back | This exercise consists in naming the stimulus that precedes the highlighted one by two positions, keeping to the rhythm of the visual cue. If the child omits or makes a mistake in naming or does not name the figure two positions ahead, parents report the error. |
| TEST | N | M (DS) PRE | M (DS) POST | t/Z | p | d di Cohen |
|---|---|---|---|---|---|---|
| Word dictation (DDE-2–errors) | 27 | 16.15 (9.56) | 12.19(8.87) | −3.12 | p < 0.005 | −1.22 ** |
| Alce–comprehension (correct responses) | 17 | 6.88 (5.45) | 7.41 (4.89) | −0.39 | n.s. | −0.20 |
| Alce–reading speed (syll/s) | 26 | 1.53 (0.94) | 1.76 (1.05) | −2.43 | p < 0.05 | −0.97 ** |
| Alce–reading accuracy (errors) | 26 | 8.78 (5.86) | 6.75 (5.27) | Z = −2.172 | p < 0.05 | 1.04 ** |
| NEPSY-II–verbal fluency correct responses | 37 | 16.72 (5.52) | 17.62 (5.94) | −1.84 | p < 0.05 | −0.61 * |
| RAN–response time | 38 | 125.21 (64.80) | 117.95 (65.18) | Z = −2.110 | p < 0.05 | 0.55 * |
| RAN–accuracy (errors) | 37 | 2.36 (2.65) | 2.15 (2.57) | 0.61 | n.s. | 0.20 |
| PRCR-2–SD4 response time | 28 | 251.93 (89.89) | 239.04 (105.05) | 0.85 | n.s. | 0.33 |
| PRCR-2–SD4 errors | 29 | 8.34 (6.87) | 6.62 (7.34) | 1.64 | p = 0.06 | 0.62 * |
| PRCR-2–SD4 target found | 29 | 23.31 (6.44) | 24.21 (6.77) | −0.92 | n.s. | −0.35 |
| NEPSY-II–inhibition rapidity (s) | 37 | 59.83 (22.87) | 55.69 (27.56) | 1.34 | p = 0.09 | 0.45 |
| NEPSY-II –inhibition accuracy (errors) | 37 | 4.60 (4.15) | 2.66 (2.71) | 3.96 | p < 0.001 | 1.32 ** |
| Digit span forward | 35 | 4.46 (1.60) | 4.66 (1.49) | −0.93 | n.s. | −0.32 |
| Digit span backward | 28 | 3.57 (1.32) | 4.07 (1.49) | −1.68 | p = 0.05 | −0.65 * |
| BAF-listening span test–n. words | 28 | 10.39 (4.93) | 12.29(6.38) | −2.00 | p < 0.05 | −0.77 * |
| BRIEF | 30 | 18.18 (16.07) | 18.20 (16.25) | Z = −0.097 | n.s. | −0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Capodieci, A.; Romano, M.; Castro, E.; Di Lieto, M.C.; Bonetti, S.; Spoglianti, S.; Pecini, C. Executive Functions and Rapid Automatized Naming: A New Tele-Rehabilitation Approach in Children with Language and Learning Disorders. Children 2022, 9, 822. https://doi.org/10.3390/children9060822
Capodieci A, Romano M, Castro E, Di Lieto MC, Bonetti S, Spoglianti S, Pecini C. Executive Functions and Rapid Automatized Naming: A New Tele-Rehabilitation Approach in Children with Language and Learning Disorders. Children. 2022; 9(6):822. https://doi.org/10.3390/children9060822
Chicago/Turabian StyleCapodieci, Agnese, Marco Romano, Emanuela Castro, Maria Chiara Di Lieto, Silvia Bonetti, Silvia Spoglianti, and Chiara Pecini. 2022. "Executive Functions and Rapid Automatized Naming: A New Tele-Rehabilitation Approach in Children with Language and Learning Disorders" Children 9, no. 6: 822. https://doi.org/10.3390/children9060822
APA StyleCapodieci, A., Romano, M., Castro, E., Di Lieto, M. C., Bonetti, S., Spoglianti, S., & Pecini, C. (2022). Executive Functions and Rapid Automatized Naming: A New Tele-Rehabilitation Approach in Children with Language and Learning Disorders. Children, 9(6), 822. https://doi.org/10.3390/children9060822