
Designing, Implementing, and Evaluating a Home-Based, Multidisciplinary, Family-Centered Pediatric Obesity Intervention: The ProxOb Program

 , ,
, ,  ,
,  ,
,  , , and
, , and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Origins and Development
2.2. Implementation
2.2.1. Specific Training of the Practitioners
2.2.2. Participating Families
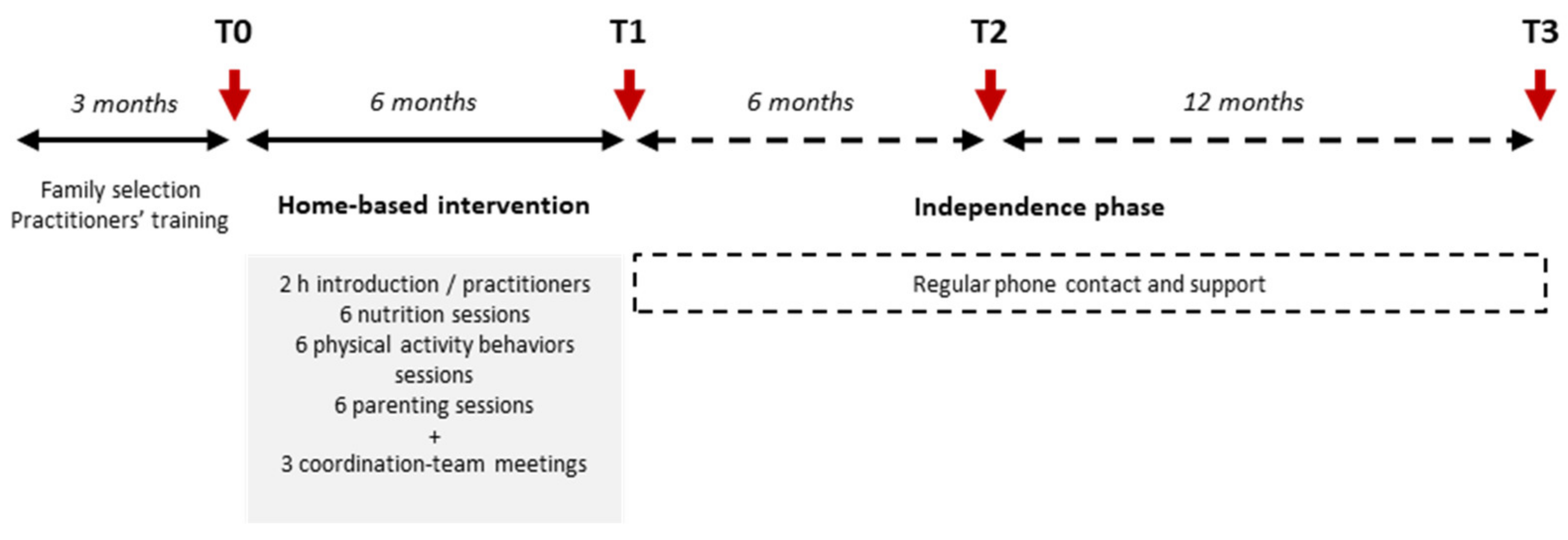
2.2.3. Intervention
2.3. Evaluations
2.4. Statistical Considerations
3. Results
3.1. Descriptive Characteristics of the Families
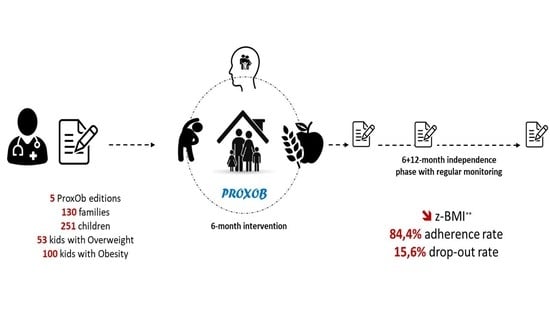
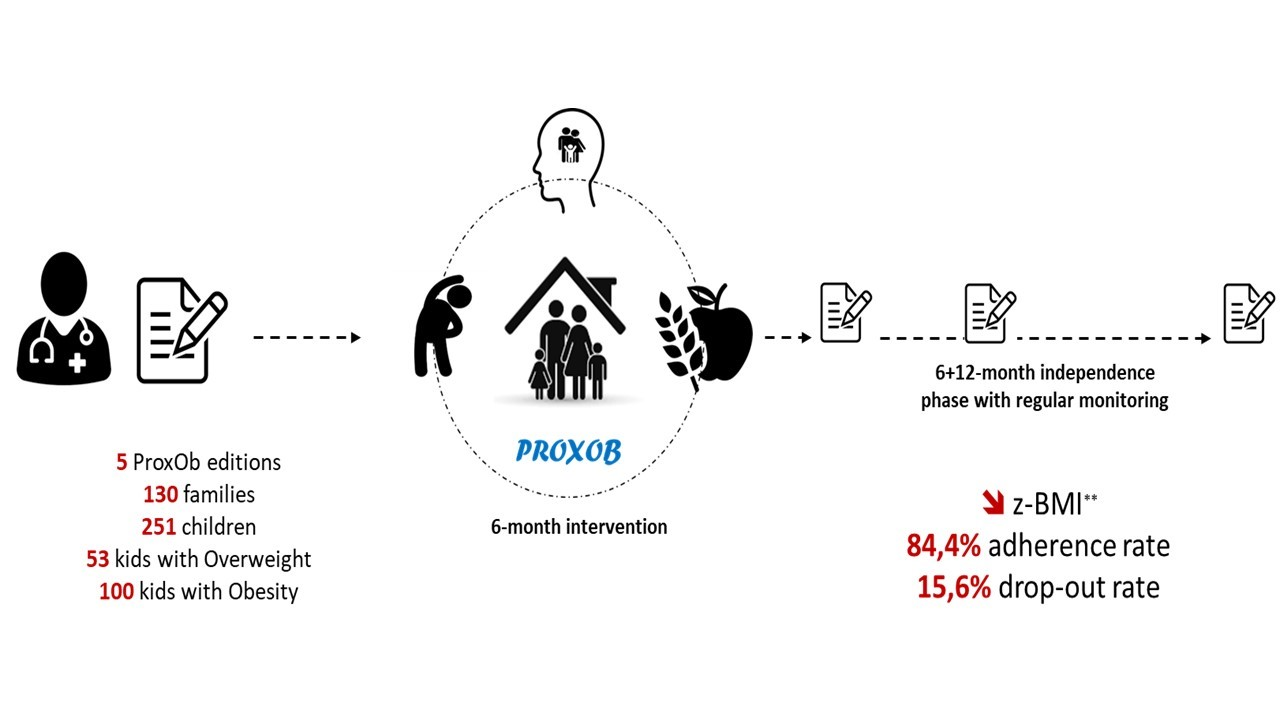
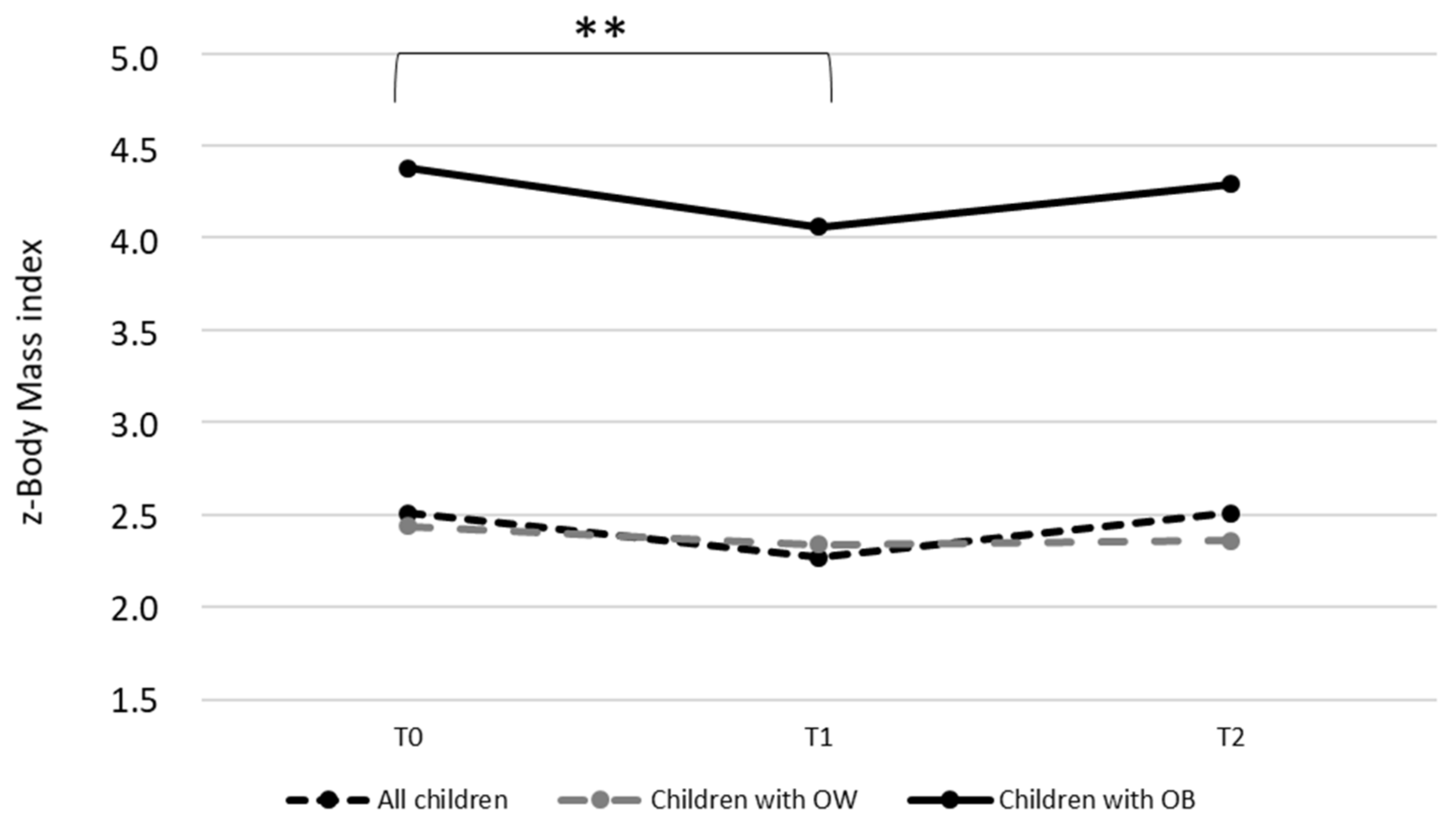
3.2. Preliminary Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Whitaker, R.C.; Wright, J.A.; Pepe, M.S.; Seidel, K.D.; Dietz, W.H. Predicting Obesity in Young Adulthood from Childhood and Parental Obesity. N. Engl. J. Med. 1997, 337, 869–873. [Google Scholar] [CrossRef] [PubMed]
- American Dietetic Association (ADA). Position of the American Dietetic Association: Individual-, Family-, School-, and Community-Based Interventions for Pediatric Overweight. J. Am. Diet. Assoc. 2006, 106, 925–945. [Google Scholar] [CrossRef] [PubMed]
- Jacob, C.M.; Hardy-Johnson, P.L.; Inskip, H.M.; Morris, T.; Parsons, C.M.; Barrett, M.; Hanson, M.; Woods-Townsend, K.; Baird, J. A systematic review and meta-analysis of school-based interventions with health education to reduce body mass index in adolescents aged 10 to 19 years. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 1. [Google Scholar] [CrossRef] [PubMed]
- Berge, J.M. A review of familial correlates of child and adolescent obesity: What has the 21st Century taught us so far? Int. J. Adolesc. Med. Health 2009, 21, 457–483. [Google Scholar] [CrossRef]
- Kitzmann, K.M.; Beech, B.M. Family-based interventions for pediatric obesity: Methodological and conceptual challenges from family psychology. J. Fam. Psychol. 2006, 20, 175–189. [Google Scholar] [CrossRef]
- Eisenmann, J.C.; Gentile, D.A.; Welk, G.J.; Callahan, R.; Strickland, S.; Walsh, M.; Walsh, D.A. SWITCH: Rationale, design, and implementation of a community, school, and family-based intervention to modify behaviors related to childhood obesity. BMC Public Health 2008, 8, 223. [Google Scholar] [CrossRef] [Green Version]
- Epstein, L.H.; Valoski, A.; Wing, R.R.; McCurley, J. Ten-year outcomes of behavioral family-based treatment for childhood obesity. Health Psychol. 1994, 13, 373–383. [Google Scholar] [CrossRef]
- Coppock, J.H.; Ridolfi, D.R.; Hayes, J.F.; Paul, M.S.; Wilfley, D.E. Current Approaches to the Management of Pediatric Overweight and Obesity. Curr. Treat. Options Cardiovasc. Med. 2014, 16, 343. [Google Scholar] [CrossRef] [Green Version]
- Robertson, W.; Friede, T.; Blissett, J.; Rudolf, M.C.J.; Wallis, M.; Stewart-Brown, S. Pilot of “Families for Health”: Community-based family intervention for obesity. Arch. Dis. Child. 2008, 93, 921–926. [Google Scholar] [CrossRef] [Green Version]
- Gerards, S.M.P.L.; Sleddens, E.F.C.; Dagnelie, P.C.; De Vries, N.K.; Kremers, S.P.J. Interventions addressing general parenting to prevent or treat childhood obesity. Pediatr. Obes. 2011, 6, e28–e45. [Google Scholar] [CrossRef]
- Arnason, A.; Langarica, N.; Dugas, L.R.; Mora, N.; Luke, A.; Markossian, T. Family-based lifestyle interventions: What makes them successful? A systematic literature review. Prev. Med. Rep. 2020, 21, 101299. [Google Scholar] [CrossRef]
- Robertson, W.; Thorogood, M.; Inglis, N.; Grainger, C.; Stewart-Brown, S. Two-year follow-up of the ‘Families for Health’ programme for the treatment of childhood obesity. Child Care Health Dev. 2011, 38, 229–236. [Google Scholar] [CrossRef]
- Varagiannis, P.; Magriplis, E.; Risvas, G.; Vamvouka, K.; Nisianaki, A.; Papageorgiou, A.; Pervanidou, P.; Chrousos, G.P.; Zampelas, A. Effects of Three Different Family-Based Interventions in Overweight and Obese Children: The “4 Your Family” Randomized Controlled Trial. Nutrients 2021, 13, 341. [Google Scholar] [CrossRef]
- Appelhans, B.M.; Thomas, A.S.; Roisman, G.I.; Booth-LaForce, C.; Bleil, M.E. Preexisting Executive Function Deficits and Change in Health Behaviors During the COVID-19 Pandemic. Int. J. Behav. Med. 2021, 28, 813–819. [Google Scholar] [CrossRef]
- Kinlin, L.M.; Oreskovich, S.M.; Dubrowski, R.; Ball, G.D.; Barwick, M.; Dettmer, E.; Haines, J.; Hamilton, J.; Kim, T.H.; Klaassen, M.; et al. Managing Obesity in Young Children: A Multiple Methods Study Assessing Feasibility, Acceptability, and Implementation of a Multicomponent, Family-Based Intervention. Child. Obes. 2022. ahead of print. [Google Scholar] [CrossRef]
- Bihan, H.; Laurent, S.; Sass, C.; Nguyen, G.; Huot, C.; Moulin, J.J.; Guegen, R.; Le Toumelin, P.; Le Clésiau, H.; La Rosa, E.; et al. Association Among Individual Deprivation, Glycemic Control, and Diabetes Complications. Diabetes Care 2005, 28, 2680–2685. [Google Scholar] [CrossRef] [Green Version]
- Janicke, D.M.; Sallinen, B.J.; Perri, M.G.; Lutes, L.D.; Huerta, M.; Silverstein, J.H.; Brumback, B. Comparison of Parent-Only vs Family-Based Interventions for Overweight Children in Underserved Rural Settings. Arch. Pediatr. Adolesc. Med. 2008, 162, 1119–1125. [Google Scholar] [CrossRef] [Green Version]
- Johnston, C.A.; Tyler, C.; McFarlin, B.K.; Poston, W.S.; Haddock, C.K.; Reeves, R.; Foreyt, J.P. Weight Loss in Overweight Mexican American Children: A Randomized, Controlled Trial. Pediatrics 2007, 120, e1450–e1457. [Google Scholar] [CrossRef]
- Endevelt, R.; Elkayam, O.; Cohen, R.; Peled, R.; Tal-Pony, L.; Grunwald, R.M.; Valinsky, L.; Porath, A.; Heymann, A.D. An Intensive Family Intervention Clinic for Reducing Childhood Obesity. J. Am. Board Fam. Med. 2014, 27, 321–328. [Google Scholar] [CrossRef] [Green Version]
- Verney, J.; Schwartz, C.; Amiche, S.; Pereira, B.; Thivel, D. Comparisons of a Multi-Frequency Bioelectrical Impedance Analysis to the Dual-Energy X-Ray Absorptiometry Scan in Healthy Young Adults Depending on their Physical Activity Level. J. Hum. Kinet. 2015, 47, 73–80. [Google Scholar] [CrossRef] [Green Version]
- Rabin, R.; De Charro, F. EQ-SD: A measure of health status from the EuroQol Group. Ann. Med. 2001, 33, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E., Jr.; Kosinski, M.; Keller, S.D. SF-36 Physical and Mental Health Summary Scales: A User’s Manual; Health Assessment Lab, New England Medical Center: Boston, MA, USA, 2002; Volume 8, pp. 23–28. [Google Scholar]
- Laureyns, F.; Séné, J.M. Questionnaire D’auto-Evaluation de L’activité Physique d’après Ricci J et Gagnon L, Modifié par F. Laureyns et JM. Séné. Available online: https://onaps.fr/outils-devaluation/ (accessed on 29 November 2021).
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stunkard, A.J.; Messick, S. The three-factor eating questionnaire to measure dietary restraint, disinhibition and hunger. J. Psychosom. Res. 1985, 29, 71–83. [Google Scholar] [CrossRef]
- Cappelleri, J.C.; Bushmakin, A.G.; Gerber, R.A.; Leidy, N.K.; Sexton, C.C.; Lowe, M.R.; Karlsson, J. Psychometric analysis of the Three-Factor Eating Questionnaire-R21: Results from a large diverse sample of obese and non-obese participants. Int. J. Obes. 2009, 33, 611–620. [Google Scholar] [CrossRef] [Green Version]
- Gibaud-Wallston, J. Self-Esteem and Situational Stress: Factors Related to Sense of Competence in New Parents. Doctoral Dissertation, Peabody College for Teachers of Vanderbilt University, Nashville, TN, USA, 1977. [Google Scholar]
- Terisse, B.; Trudelle, D. Le Questionnaire d’auto-Évaluation de La Compétence Éducative Parentale (Q.A.E.C.E.P.); Université du Québec: Montréal, BC, Canada, 1988. [Google Scholar]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240–1243. [Google Scholar] [CrossRef] [Green Version]
- Verney, J.; Metz, L.; Chaplais, E.; Cardenoux, C.; Pereira, B.; Thivel, D. Bioelectrical impedance is an accurate method to assess body composition in obese but not severely obese adolescents. Nutr. Res. 2016, 36, 663–670. [Google Scholar] [CrossRef]
- Thivel, D.; Verney, J.; Miguet, M.; Masurier, J.; Cardenoux, C.; Lambert, C.; Courteix, D.; Metz, L.; Pereira, B. The accuracy of bioelectrical impedance to track body composition changes depends on the degree of obesity in adolescents with obesity. Nutr. Res. 2018, 54, 60–68. [Google Scholar] [CrossRef]
- Kreimeier, S.; Greiner, W. EQ-5D-Y as a Health-Related Quality of Life Instrument for Children and Adolescents: The Instrument’s Characteristics, Development, Current Use, and Challenges of Developing Its Value Set. Value Heal. 2019, 22, 31–37. [Google Scholar] [CrossRef] [Green Version]
- Manificat, S.; Dazord, A.; Cochat, P.; Nicolas, J. Évaluation de la qualité de vie en pédiatrie: Comment recueillir le point de vue de l’enfant. Archives de Pédiatrie 1997, 4, 1238–1246. [Google Scholar] [CrossRef]
- Varni, J.W.; Seid, M.; Rode, C.A. The PedsQL™: Measurement Model for the Pediatric Quality of Life Inventory. Med. Care 1999, 37, 126–139. [Google Scholar] [CrossRef]
- Sapin, C.; Simeoni, M.-C.; El Khammar, M.; Antoniotti, S.; Auquier, P. Reliability and validity of the VSP-A, a health-related quality of life instrument for ill and healthy adolescents. J. Adolesc. Health 2005, 36, 327–336. [Google Scholar] [CrossRef]
- Simeoni, M.; Auquier, P.; Antoniotti, S.; Sapin, C.; Marco, J.S. Validation of a French health-related quality of life instrument for adolescents: The VSP-A. Qual. Life Res. 2000, 9, 393–403. [Google Scholar] [CrossRef]
- Fillon, A.; Masurier, J.; Boirie, Y.; Duclos, M.; Thivel, D. Development of a Adapted Questionnaire to Assess Physical Activity and Sedentary Behaviors among Young Children. In Proceedings of the ONAPS’ 2020 Annual National Workshop, Niort, France, 2–3 June 2020. [Google Scholar]
- Bryant, E.J.; Thivel, D.; Chaput, J.-P.; Drapeau, V.; E Blundell, J.; King, N.A. Development and validation of the Child Three-Factor Eating Questionnaire (CTFEQr17). Public Health Nutr. 2018, 21, 2558–2567. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Families | ProxOb II | ProxOb III | ProxOb IV | ProxOb V |
|---|---|---|---|---|
| n = 41 | n = 30 | n = 25 | n = 34 | |
| Number of people per family | 4 (3; 5) | 4 (3; 4) | 3 (2; 4) | 4 (3; 4) |
| Single-parent family | 14 (34.1) | 13 (43.3) | 13 (52.0) | 9 (26.5) |
| Number of children per family | 2 (1; 3) | 2 (1; 3) | 2 (1; 2) | 2 (1; 2) |
| At least one parent per family with overweight/obesity | 40/40 (100.0) | 29/30 (96.7) | 22/24 (91.7) | 30/33 (90.9) |
| At least one parent with a precarious economic situation | 12/22 (54.5) | 18/28 (64.3) | 14/19 (73.7) | 13/26 (50.0) |
| Children | n = 87 | n = 58 | n = 42 | n = 64 |
| Weight status | ||||
| Underweight | 1 (1.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Normal | 36 (41.4) | 14 (24.1) | 7 (16.7) | 17 (26.6) |
| Overweight | 16 (18.4) | 16 (27.6) | 5 (11.9) | 16 (25.0) |
| Obesity | 25 (28.7) | 24 (41.4) | 26 (61.9) | 25 (39.0) |
| Missing data | 9 (10.3) | 4 (6.9) | 4 (9.5) | 6 (9.4) |
| Male sex | ||||
| All children | 43 (49.4) | 37 (63.8) | 21 (50.0) | 30 (46.9) |
| Children with overweight | 10/16 (62.5) | 8/16 (50.0) | 2/5 (40.0) | 8/16 (50.0) |
| Children with obesity | 8/25 (32.0) | 18/24 (75.0) | 15/26 (57.7) | 13/25 (48.0) |
| Age (years) | ||||
| All children (n = 87/58/42/64) | 9.9 ± 5.1 | 10.1 ± 4.0 | 10.6 ± 4.5 | 10.4 ± 4.2 |
| Children with overweight (n = 16/16/5/16) | 12.2 ± 3.6 | 10.8 ± 2.7 | 11.7 ± 1.5 | 9.6 ± 2.8 |
| Girls with overweight (n = 6/8/3/8) | 10.6 ± 3.4 | 10.6 ± 2.0 | 11.0 ± 1.5 | 8.7 ± 2.1 |
| Boys with overweight (n = 10/8/2/8) | 13.1 ± 3.5 | 11.1 ± 3.4 | 12.9 ± 0.2 | 10.5 ± 3.2 |
| Children with obesity (n = 25/24/26/25) | 11.4 ± 5.1 | 10.3 ± 3.4 | 10.4 ± 4.1 | 11.4 ± 3.2 |
| Girls with obesity (n = 17/6/11/12) | 11.2 ± 5.0 | 9.0 ± 1.9 | 8.7 ± 3.9 | 10.4 ± 2.8 |
| Boys with obesity (n = 8/18/15/13) | 11.9 ± 5.5 | 10.7 ± 3.8 | 11.6 ± 3.9 | 12.3 ± 3.4 |
| Z-body mass index | ||||
| All children (n = 78/54/37/58) | 1.90 ± 2.11 | 2.80 ± 1.80 | 3.38 ± 1.97 | 3.04 ± 1.89 |
| Children with overweight (n = 16/16/5/16) | 2.48 ± 0.38 | 2.33 ± 0.42 | 2.67 ± 0.66 | 3.16 ± 1.50 |
| Girls with overweight (n = 6/8/3/8) | 2.43 ± 0.44 | 2.30 ± 0.39 | 2.32 ± 0.58 | 3.42 ± 1.86 |
| Boys with overweight (n = 10/8/2/8) | 2.51 ± 0.36 | 2.36 ± 0.48 | 3.19 ± 0.42 | 2.90 ± 1.09 |
| Children with obesity (n = 25/24/25/25) | 4.27 ± 1.03 | 4.39 ± 1.23 | 4.47 ± 0.92 | 4.24 ± 1.22 |
| Girls with obesity (n = 17/6/11/12) | 4.25 ± 0.77 | 4.71 ± 1.35 | 4.21 ± 1.02 | 4.28 ± 0.72 |
| Boys with obesity (n = 8/18/14/13) | 4.32 ± 1.52 | 4.28 ± 1.21 | 4.67 ± 0.81 | 4.21 ± 1.58 |
| Parents | n = 68 | n = 47 | n = 37 | n = 59 |
| Weight status | ||||
| Underweight | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Normal | 9 (13.2) | 5 (10.6) | 4 (10.8) | 6 (10.2) |
| Overweight | 17 (25.0) | 13 (27.7) | 10 (27.0) | 10 (16.9) |
| Obesity | 37 (54.4) | 29 (61.7) | 22 (59.5) | 40 (67.8) |
| Missing data | 5 (7.4) | 0 (0.0) | 1 (2.7) | 3 (5.1) |
| Male sex | ||||
| All parents | 28 (41.2) | 19 (40.4) | 14 (37.8) | 25 (42.4) |
| Parents with overweight | 8/17 (47.1) | 5/13 (38.5) | 4/10 (40.0) | 7/10 (70.0) |
| Parents with obesity | 8/37 (21.6) | 10/29 (34.5) | 8/22 (36.4) | 15/40 (37.5) |
| Age (years) | ||||
| All parents (n = 68/47/37/59) | 40.5 ± 7.3 | 42.6 ± 8.1 | 43.6 ± 6.1 | 42.9 ± 6.4 |
| Parents with overweight (n = 17/13/10/10) | 44.0 ± 7.2 | 43.9 ± 5.4 | 42.6 ± 7.1 | 42.1 ± 8.6 |
| Women with overweight (n = 9/8/6/3) | 42.3 ± 7.6 | 42.1 ± 5.6 | 43.4 ± 8.7 | 42.3 ± 7.2 |
| Men with overweight (n = 8/5/4/7) | 45.9 ± 6.7 | 46.9 ± 3.8 | 41.2 ± 4.9 | 41.9 ± 9.6 |
| Parents with obesity (n = 37/29/22/40) | 39.4 ± 6.9 | 42.2 ± 8.5 | 44.3 ± 5.8 | 42.9 ± 6.1 |
| Women with obesity (n = 29/19/14/25) | 39.0 ± 6.6 | 40.2 ± 7.7 | 43.9 ± 6.4 | 42.2 ± 5.7 |
| Men with obesity (n = 8/10/8/15) | 41.1 ± 8.0 | 46.0 ± 8.9 | 44.8 ± 5.0 | 44.1 ± 6.8 |
| Body mass index (kg/m2) | ||||
| All parents (n = 63/47/36/56) | 33.5 ± 8.7 | 33.0 ± 8.3 | 32.2 ± 7.1 | 35.6 ± 9.7 |
| Parents with overweight (n = 17/13/10/10) | 27.5 ± 1.5 | 27.3 ± 1.5 | 27.6 ± 1.7 | 28.5 ± 1.1 |
| Women with overweight (n = 9/8/6/3) | 27.9 ± 1.3 | 27.2 ± 1.5 | 27.6 ± 2.1 | 28.1 ± 1.6 |
| Men with overweight (n = 8/5/4/7) | 27.1 ± 1.6 | 27.3 ± 1.6 | 27.7 ± 1.2 | 28.6 ± 1.0 |
| Parents with obesity (n = 37/29/22/40) | 38.7 ± 7.5 | 37.3 ± 7.6 | 36.0 ± 6.1 | 39.2 ± 9.0 |
| Women with obesity (n = 29/19/14/25) | 38.4 ± 7.6 | 37.3 ± 6.4 | 35.9 ± 6.2 | 41.9 ± 10.2 |
| Men with obesity (n = 8/10/8/15) | 39.9 ± 7.6 | 37.5 ± 9.8 | 36.2 ± 6.3 | 34.8 ± 3.7 |
| Families | Drop-Outs | Completers | p |
|---|---|---|---|
| n = 15 | n = 81 | ||
| ProxOb | |||
| II | 10 (66.7) | 31 (38.3) | 0.11 |
| III | 2 (13.3) | 28 (34.6) | |
| IV | 3 (20.0) | 23 (27.1) | |
| Number of people per family | 3 (3; 4) | 4 (3; 4) | 0.66 |
| Single-parent family | 5 (33.3) | 51 (63.0) | 0.03 * |
| Number of children per family | 2 (1; 3) | 2 (1; 3) | 0.58 |
| At least one parent per family with overweight/obesity | 14/14 (100.0) | 77/80 (96.2) | 1.00 |
| At least one parent with a precarious economic situation | 5/7 (71.4) | 39/62 (62.9) | 1.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miolanne, M.; Lambert, C.; Masurier, J.; Cardenoux, C.; Fillion, A.; Beraud, S.; Desblés, C.; Rigal, A.; Védrine, E.; Dalmais, C.; et al. Designing, Implementing, and Evaluating a Home-Based, Multidisciplinary, Family-Centered Pediatric Obesity Intervention: The ProxOb Program. Children 2022, 9, 737. https://doi.org/10.3390/children9050737
Miolanne M, Lambert C, Masurier J, Cardenoux C, Fillion A, Beraud S, Desblés C, Rigal A, Védrine E, Dalmais C, et al. Designing, Implementing, and Evaluating a Home-Based, Multidisciplinary, Family-Centered Pediatric Obesity Intervention: The ProxOb Program. Children. 2022; 9(5):737. https://doi.org/10.3390/children9050737
Chicago/Turabian StyleMiolanne, Magalie, Céline Lambert, Julie Masurier, Charlotte Cardenoux, Alicia Fillion, Sarah Beraud, Chloé Desblés, Amélie Rigal, Elodie Védrine, Carla Dalmais, and et al. 2022. "Designing, Implementing, and Evaluating a Home-Based, Multidisciplinary, Family-Centered Pediatric Obesity Intervention: The ProxOb Program" Children 9, no. 5: 737. https://doi.org/10.3390/children9050737
APA StyleMiolanne, M., Lambert, C., Masurier, J., Cardenoux, C., Fillion, A., Beraud, S., Desblés, C., Rigal, A., Védrine, E., Dalmais, C., Da Silva, B., De L’Eprevier, E., Hazart, J., Chaput, J.-P., Drapeau, V., Pereira, B., O’Malley, G., Thivel, D., & Boirie, Y. (2022). Designing, Implementing, and Evaluating a Home-Based, Multidisciplinary, Family-Centered Pediatric Obesity Intervention: The ProxOb Program. Children, 9(5), 737. https://doi.org/10.3390/children9050737