
The Needs of Parents of Children Suffering from Cancer—Continuation of Research


Abstract
:1. Introduction
Objective of the Work
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Research Procedures
2.4. Method
Questionnaire
2.5. Procedure
2.6. Data Analysis
3. Results
3.1. Demographic
3.2. Needs
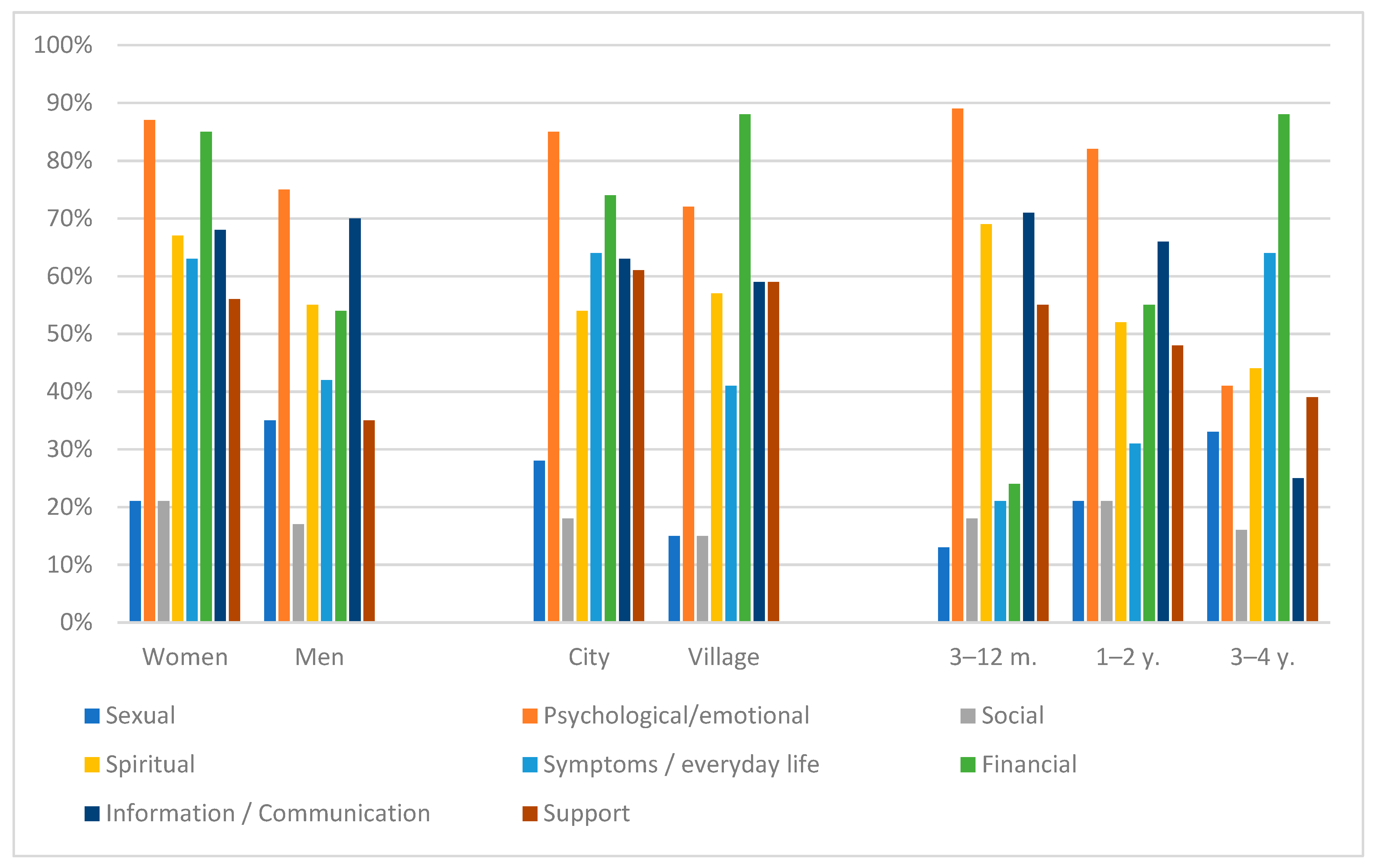
3.3. Needs by Domain
4. Discussion
5. Conclusions
- (1)
- Parents of children with cancer experience a high level of needs, especially psychological, emotional, and information. These data suggest that the existing healthcare system does not meet the needs of parents of sick children. The results show the need to investigate the mechanisms by which healthcare providers can use the healthcare system to identify and meet needs.
- (2)
- Parent-oriented care should be included in pediatric oncology departments. It is possible, thanks to the development and application of strategies, to understand the needs of parents, respond positively to needs, and provide effective care, all to reduce the needs of this vulnerable group and thus minimize the risks of not being satisfied.
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Toledano-Toledano, F.; Domínguez-Guedea, M.T. Psychosocial factors related with caregiver burden among families of children with chronic conditions. BioPsychoSocial Med. 2019, 13, 6. [Google Scholar] [CrossRef]
- Toledano-Toledano, F.; Moral de la Rubia, J.; Domínguez-Guedea, M.T.; Nabors, L.A.; Barcelata-Eguiarte, B.E.; Rocha-Pérez, E. Validity and Reliability of the Beck Anxiety Inventory (BAI) for Family Caregivers of Children with Cancer. Int. J. Environ. Res. Public Health 2020, 17, 7765. [Google Scholar] [CrossRef]
- Toledano-Toledano, F.; Contreras-Valdez, J.A. Validity and reliability of the Beck Depression Inventory II (BDI-II) in family caregivers of children with chronic diseases. PLoS ONE 2018, 13, e0206917. [Google Scholar] [CrossRef]
- Qingying, J.; Currin-McCulloch, J.A.; Zhang, A.; Streeter, C.L.; Jones, B.L.; Chen, Y. Assessing the Needs of Parents of Children Diagnosed with Cancer in China: A Psychometric Study Developing a Needs Assessment Tool. J. Pediatr. Oncol. Nurs. 2018, 35, 6–15. [Google Scholar] [CrossRef]
- Kaptacz, I. Assessment of quality of life, acceptance of illness, needs and expectations of patients under palliative home care—Preliminary pilot study. Palliat. Med. 2018, 10, 137–144. [Google Scholar] [CrossRef] [Green Version]
- Koohkan, E.; Yousofian, S.; Rajabi, G.; Zare-Farashbandi, F. Health information needs of families at childhood cancer: A qualitative study. J. Educ. Health Promot. 2019, 8, 246. [Google Scholar] [CrossRef]
- Chrapek, E. Psychological difficulties, social support and stress management in parents of children with cancer. Psychiatr. Psychol. Klin. 2016, 16, 27–32. [Google Scholar] [CrossRef]
- Toledano-Toledano, F.; Luna, D.; Moral de la Rubia, J.; Martínez Valverde, S.; Bermúdez Morón, C.A.; Salazar García, M. Psychosocial Factors Predicting Resilience in Family Caregivers of Children with Cancer: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 748. [Google Scholar] [CrossRef]
- Toledano-Toledano, F.; Moral de la Rubia, J.; Broche-Pérez, Y.; Domínguez-Guedea, M.T.; Granados-García, V. The measurement scale of resilience among family caregivers of children with cancer: A psychometric evaluation. BMC Public Health 2019, 19, 1164. [Google Scholar] [CrossRef] [Green Version]
- Toledano-Toledano, F.; Moral de la Rubia, J.; McCubbin, L.D.; Liebenberg, L.; Jiménez, J.; Rivera-Rivera, L. Validity and reliability of the Mexican resilience measurement scale in families of children with chronic conditions. Health Qual. Life Outcomes 2017, 15, 242. [Google Scholar] [CrossRef] [Green Version]
- Toledano-Toledano, F.; Moral de la Rubia, J.; Nabors, L.A.; Domínguez-Guedea, M.T.; Salinas Escudero, G.; Rocha Pérez, E.; Luna, D.; Leyva López, A. Predictors of Quality of Life among Parents of Children with Chronic Diseases: A Cross-Sectional Study. Healthcare 2020, 8, 456. [Google Scholar] [CrossRef]
- Toledano-Toledano, F.; Moral de la Rubia, J.; McCubbin, L.D.; Cauley, B.; Luna, D. Brief version of the coping health inventory for parents (CHIP) among family caregivers of children with chronic diseases. Health Qual. Life Outcomes 2020, 18, 104. [Google Scholar] [CrossRef] [Green Version]
- Toledano-Toledano, F.; Moral de la Rubia, J. Factors associated with anxiety in family caregivers of children with chronic diseases. BioPsychoSocial Med. 2018, 12, 20. [Google Scholar] [CrossRef] [Green Version]
- Toledano-Toledano, F.; Moral de la Rubia, J.; Reyes Frometa, R.; González Betanzos, F.; Villavicencio Guzmán, L.; Salazar García, M. The Social Support Networks Scale (SSNS) for Family Caregivers of Children with Cancer: A Psychometric Evaluation. Int. J. Environ. Res. Public Health 2020, 17, 7820. [Google Scholar] [CrossRef]
- Toledano-Toledano, F.; Luna, D. The psychosocial profile of family caregivers of children with chronic diseases: A cross-sectional study. BioPsychoSocial Med. 2020, 14, 29. [Google Scholar] [CrossRef]
- Rainbird, K.; Perkins, J.; Sanson-Fisher, R.; Rolfe, I.; Anseline, P. The needs of patients with advanced, incurable cancer. Br. J. Cancer 2009, 101, 759–764. [Google Scholar] [CrossRef] [Green Version]
- Kerr, L.M.J.; Harrison, M.B.; Medves, J.; Tranmer, J. Supportive care needs of parents of children with cancer: Transition from diagnosis to treatment. Oncol. Nurs. Forum. 2004, 31, E116–E126. [Google Scholar] [CrossRef]
- Shorofi, S.A.; Jannati, Y.; Moghaddam, H.R.; Yazdani-Charati, J. Psychosocial needs of families of intensive care patients: Perceptions of nurses and families. Niger. Med. J. 2016, 57, 10–18. [Google Scholar] [CrossRef]
- Borjalilu, S.; Shahidi, S.; Fath-Abadi, J.; Mazaheri, M.A. Spiritual issues and challenges of the children with cancer: Parent’s experience. J. Res. Psychol. Health 2014, 3, 37–54. [Google Scholar]
- Kahouei, M.; Najarioon, O.; Ebrahimi, N.; Ahmadi-Takhorani, F.; Haidari, S. A study on the preferences of parents of patients with thalassemia major in obtaining health information. Health Inf. Manag. 2016, 13, 78–83. [Google Scholar]
- Grochowska, A.; Bodys-Cupak, I.; Kubik, B.; Starzec, P. Assessment of parental stress and anxiety in children with acute lymphoblastic leukemia. Pol. Nurs. 2018, 2, 173–181. [Google Scholar] [CrossRef]
- Stenka, K.E.; Izdebski, P. Parents facing their child’s struggle with cancer. Psychiatr. Psychol. Klin. 2018, 18, 306–314. [Google Scholar] [CrossRef]
- Olagunju, A.T.; Sarimiye, F.O.; Olagunju, T.O.; Habeebu, M.Y.; Aina, O.F. Child’s symptom burden and depressive symptoms among caregivers of children with cancers: An argument for early integration of pediatric palliative care. Ann. Palliat. Med. 2016, 5, 157–165. [Google Scholar] [CrossRef]
- Klassen, A.F.; Raina, P.; McIntosh, C.; Sung, L.; Klaassen, R.J.; O’Donnell, M. Parents of children with cancer: Which factors explain differences in health-related quality of life. Int. J. Cancer 2011, 129, 1190–1198. [Google Scholar] [CrossRef]
- Wiener, L.; Battles, H.; Zadeh, S.; Pelletier, W.; Arruda-Colli, M.N.F.; Muriel, A.C. The perceived influence of childhood cancer on the parents’ relationship. Psychooncology 2017, 26, 2109–2117. [Google Scholar] [CrossRef]
- Santos, S.; Crespo, C.; Canavarro, M.C.; Alderfer, M.A.; Kazak, A.E. Family rituals, financial burden, and mothers’ adjustment in pediatric cancer. J. Fam. Psychol. 2016, 30, 1008–1013. [Google Scholar] [CrossRef]
- Riahi, A.; Hariri, N.; Nooshinfard, F. Health Information Needs of Immigrant Patients with Cancer in Iran. J. Mod. Med. Inf. Sci. 2016, 2, 21–30. [Google Scholar]
- Borjalilu, S.; Sharif, Z.; Azad, M.S.; Afzali, M.; Koochakzadeh, L.; Afzali, M. The information needs of parents of children with cancer: A qualitative study. J. Qual. Res. Health Sci. 2017, 6, 228–237. [Google Scholar]
- Adams, E.; Boulton, M.; Watson, E. The information needs of partners and family members of cancer patients: A systematic literature review. Patient Educ. Couns. 2009, 77, 179–186. [Google Scholar] [CrossRef] [Green Version]
- Inman, K. Examining Parent Information Needs in Pediatric Cancer. Senior Honors Theses & Projects. Department Psychology Eastern Michigan University Digital Commons EMU. 2017. Available online: https://commons.emich.edu/honors/556 (accessed on 25 November 2021).
- Mitchell, W.; Clarke, S.; Sloper, P. Care and support needs of children and young people with cancer and their parents. Psycho-Oncol. J. Psychol. Soc. Behav. Dimens. Cancer 2006, 15, 805–816. [Google Scholar] [CrossRef]
- Maree, J.E.; Parker, S.; Kaplan, L.; Oosthuizen, J. The information needs of South African parents of children with cancer. J. Pediatr. Oncol. Nurs. 2016, 33, 9–17. [Google Scholar] [CrossRef]
- Yeh, C.H. Gender differences of parental distress in children with cancer. J. Adv. Nurs. 2002, 38, 598–606. [Google Scholar] [CrossRef]
- Santacroce, S. Uncertainty, anxiety, and symptoms of posttraumatic stress in parents of children recently diagnosed with cancer. J. Pediatr. Oncol. Nurs. 2002, 19, 104–111. [Google Scholar] [CrossRef]
- Sawyer, M.G.; Antoniou, G.; Toogood, I.; Rice, M.; Baghurst, P.A. A prospective study of the psychological adjustment of parents and families of children with cancer. J. Paediatr. Child Health 1993, 29, 352–356. [Google Scholar] [CrossRef]
- Bruce, M. A systematic and conceptual review of posttraumatic stress in childhood cancer survivors and their parents. Clin. Psychol. Rev. 2006, 26, 233–256. [Google Scholar] [CrossRef]
- Pinquart, M.; Sörensen, S. Spouses, adult children, and children-in-law as caregivers of older adults: A meta-analytic comparison. Psychol. Aging. 2011, 26, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Buckley, M. Childhood cancer: Meeting the information needs of families. Paediatr. Nurs. 2000, 12, 22–23. [Google Scholar] [CrossRef]
- Tremolada, M.; Taverna, L.; Bonichini, S.; Putti, M.C.; Pillon, M.; Biffi, A. Health Locus of Control in Parents of Children with Leukemia and Associations with Their Life Perceptions and Depression Symptomatology. Children 2020, 7, 40. [Google Scholar] [CrossRef]
- Tarr, J.; Pickler, R.H. Becoming a cancer patient: A study of families of children with acute lymphocytic leukemia. J. Pediatr. Oncol. Nurs. 1999, 16, 44–50. [Google Scholar] [CrossRef]
- Loghmani, L.; Borhani, F.; Abbaszadeh, A. Determination of the content of communication between the care team and family members of patients in the intensive care unit: The experience of nurses and patients’ families. J. Qual. Res. Health Sci. 2014, 3, 257–268. [Google Scholar]
- Tomlinson, P.S.; Mitchell, K.E. On the nature of social support for families of critically ill children. J. Pediatr. Nurs. 1992, 7, 386–394. [Google Scholar] [PubMed]
- Jurbergs, N.; Long, A.; Ticona, L.; Phipps, S. Symptoms of posttraumatic stress in parents of children with cancer: Are they elevated relative to parents of healthy children? J. Pediatr. Psychol. 2009, 34, 4–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Institute of Medicine (US) Committee on Psychosocial Services to Cancer Patients/Families in a Community Setting. Cancer Care for the Whole Patient: Meeting Psychosocial Health Needs; Adler, N.E., Page, A.E.K., Eds.; National Academies Press: Washington, DC, USA, 2008.
- Shamsaei, F.; Kermanshahi, S.M.; Vanaki, Z. Survey of family caregiver needs of patients with bipolar disorder. Avicenna J. Clin. Med. 2010, 17, 57–63. [Google Scholar] [CrossRef]
- Aitken, T.J.; Hathaway, G. Long distance related stressors and coping behaviors in parents of children with cancer. J. Pediatr. Oncol. Nurs. 1993, 10, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.A.; Barbarin, O.A. Gender differences in parenting a child with cancer. Soc. Work Health Care 1996, 22, 53–71. [Google Scholar] [CrossRef]
- Cayse, L.N. Fathers of children with cancer: A descriptive study of their stressors and coping strategies. J. Pediatr. Oncol. Nurs. 1994, 11, 102–108. [Google Scholar] [CrossRef]
- Enskar, K.; Carlsson, M.; Golsater, M.; Hamrin, E.; Kreuger, A. Life situation and problems as reported by children with cancer and their parents. J. Pediatr. Oncol. Nurs. 1997, 14, 18–26. [Google Scholar] [CrossRef]
- Martinson, I.M.; Leavitt, M.; Liu, C.Y.; Armstrong, V.; Hornberger, L.; Zhang, J.Q. Comparison of Chinese and Caucasian families caregiving to children with cancer at home: Part I. J. Pediatr. Nurs. 1999, 14, 99–109. [Google Scholar] [CrossRef]
- Yiu, J.M.; Twinn, S. Determining the needs of chinese parents during the hospitalization of Their child diagnosed with cancer: An exploratory study. Cancer Nurs. 2001, 24, 483–489. [Google Scholar] [CrossRef]
- Cornman, B.J. Childhood cancer: Differential effects on the family members. Oncol. Nurs. Forum 1993, 20, 1559–1566. [Google Scholar]
- Manne, S.; Miller, D.; Meyers, P.; Wollner, N.; Steinherz, P.; Redd, W.H. Depressive symptoms among parents of newly diagnosed children with cancer: A 6-month follow-up study. Child. Health Care 2009, 25, 191–209. [Google Scholar] [CrossRef]
- McGrath, P. Findings on the impact of treatment for childhood acute lymphoblastic leukemia on family relationships. Child Fam. Soc. Work 2001, 6, 229–237. [Google Scholar] [CrossRef]
- McGrath, P. Identifying support issues of parents of children with leukemia. Cancer Pract. 2001, 9, 198–205. [Google Scholar] [CrossRef] [PubMed]
- Skolin, I.; Hursti, U.K.; Wahlin, Y.B. Parents’ perception of their child’s food intake after the start of chemotherapy. J. Pediatr. Oncol. Nurs. 2001, 18, 124–136. [Google Scholar] [CrossRef]
- Clarke-Steffen, L. Reconstructing reality: Family strategies for managing childhood cancer. J. Pediatr. Nurs. 1997, 12, 278–287. [Google Scholar] [CrossRef]
- Ferrell, B.R.; Rhiner, M.; Shapiro, B.; Dierkes, M. The experience of pediatric cancer pain, Part I: Impact of pain on the family. J. Pediatr. Nurs. 1994, 9, 368–379. [Google Scholar]
- Chesler, M.A.; Parry, C. Gender roles and/or styles in crisis: An integrative analysis of the experiences of fathers of children with cancer. Qual. Health Res. 2001, 11, 363–384. [Google Scholar] [CrossRef]


{kind=link}
| Demographic Information | Total n = 800 | p |
|---|---|---|
| Characteristics % (n) | ||
| Sex | ||
| women | 85% (680) | 0.01 |
| men | 15% (120) | |
| The age of the study group | ||
| SD | 44.1 (7.76) | 0.12 |
| 95% CI | [26; 57] | |
| The age of women | ||
| ± standard deviation | 38.2 ± 7.25 | 0.21 |
| scope | [26; 57] | |
| median | 38 | |
| 95% CI | [39.8; 41.8] | |
| The age of men | ||
| ± standard deviation | 41.1 ± 7.03 | 0.19 |
| scope | [26; 57] | |
| median | 41 | |
| 95% CI | [39.8; 41.8] | |
| Place of residence | ||
| city | 68% (544) | 0.21 |
| village | 32% (256) | |
| Financial situation | ||
| very good | 1% (8) | 0.01 |
| good | 8% (64) | |
| average | 68% (544) | |
| bad | 10% (80) | |
| very bad | 13% (104) | |
| Age groups | ||
| 20–29 | 3% (24) | 0.01 |
| 30–40 | 35% (280) | |
| 41–50 | 37% (296) | |
| 51–60 | 25% (200) | |
| Education of the study group | ||
| higher education | 47% (378) | 0.01 |
| secondary education | 35% (276) | |
| vocational education | 18% (146) | |
| primary education | 0% (0) | |
| Marital status | ||
| married | 74% (592) | 0.62 |
| widowed | 3% (24) | |
| unmarried | 23% (184) | |
| Source of income | ||
| professionally active | 76% (608) | 0.59 |
| annuity | 15% (120) | |
| benefit | 9% (72) | |
| Type of cancer in the family | ||
| leukemia | 54% (432) | 0.07 |
| brain tumors | 19% (152) | |
| solid tumors | 27% (216) | |
| Age of children with cancer | ||
| up to 5 years | 22% (176) | 0.19 |
| 5–10 years | 51% (408) | |
| 11–18 years | 27% (216) | |
| Number of children | ||
| one child | 45% (360) | 0.71 |
| two children | 41% (328) | |
| three children | 10% (80) | |
| four children | 4% (32) | |
| Times of illness | ||
| 3–12 m | 43% (344) | 0.01 |
| 1–2 y | 37% (296) | |
| 3–4 y | 20% (160) | |
| Needs | Moderate/High Needs % (n) | Moderate/High Needs % (n) | Moderate/High Needs % (n) | p | ||||
|---|---|---|---|---|---|---|---|---|
| Sex | Place of Residence | Times of Illness | ||||||
| Women | Men | City | Village | 3–12 Months | 1–2 Years | 3–4 Years | ||
| Support | ||||||||
| support in dealing with depression | 31% (211) | 35% (42) | 37% (201) | 24% (61) | 38% (131) | 24% (71) | 21% (34) | 0.91 |
| support in dealing with frustration | 56% (381) | 31% (37) | 61% (332) | 59% (151) | 55% (189) | 48% (142) | 39% (62) | 0.55 |
| emotional support from loved ones | 29% (197) | 18% (22) | 22% (120) | 31% (79) | 33% (113) | 27% (80) | 24% (38) | 0.44 |
| psychological support from support groups | 20% (136) | 15% (18) | 18% (98) | 17% (43) | 18% (62) | 7% (21) | 11% (18) | 0.55 |
| psychological support from medical staff | 45% (306) | 30% (36) | 41% (223) | 28% (72) | 44% (151) | 35% (104) | 25% (40) | 0.91 |
| Information/Communication | ||||||||
| need information about health status | 66% (449) | 70% (84) | 58% (315) | 54% (138) | 71% (244) | 55% (163) | 19% (30) | 0.01 |
| need information about treatment | 58% (394) | 69% (83) | 61% (332) | 52% (133) | 56% (193) | 30% (89) | 14% (22) | 0.01 |
| the need for education about illness from medical staff | 68% (462) | 59% (71) | 63% (343) | 59% (151) | 70% (241) | 66% (195) | 25% (40) | 0.01 |
| the need for information about the factors that may influence the course of the neoplastic disease | 51% (347) | 48% (58) | 53% (288) | 42% (107) | 46% (158) | 26% (77) | 7% (11) | 0.41 |
| need information about health opportunities | 44% (299) | 53% (64) | 45% (245) | 55% (141) | 34% (117) | 15% (44) | 18% (29) | 0.01 |
| the need for complete information on the results of medical examinations | 52% (354) | 61% (73) | 45% (245) | 55% (141) | 50% (172) | 48% (142) | 22% (35) | 0.01 |
| Financial | ||||||||
| support in everyday life finances | 85% (578) | 54% (65) | 74% (402) | 88% (225) | 22% (76) | 55% (163) | 88% (141) | 0.01 |
| support in treatment costs | 25% (170) | 20% (24) | 21% (114) | 25% (64) | 24%( 82) | 48% (142) | 74% (118) | 0.01 |
| Symptoms/everyday life | ||||||||
| help in dealing with symptoms | 63% (428) | 42% (50) | 64% (348) | 41% (105) | 15% (52) | 29% (86) | 64% (102) | 0.01 |
| help in everyday functioning | 32% (218) | 21% (25) | 30% (163) | 25% (64) | 21% (72) | 31% (92) | 35% (56) | 0.01 |
| Spiritual | ||||||||
| changing priorities | 39% (265) | 21% (25) | 40% (218) | 25% (64) | 33% (113) | 34% (101) | 29% (46) | 0.91 |
| help in dealing with the problem of dying | 67% (456) | 55% (66) | 54% (294) | 57% (146) | 69% (237) | 52% (154) | 44% (70) | 0.71 |
| Social | ||||||||
| ability to express feelings | 21% (143) | 17% (20) | 12% (65) | 15% (38) | 15% (52) | 10% (30) | 13% (21) | 0.74 |
| planning the future | 19% (129) | 12% (14) | 18% (98) | 11% (28) | 18% (62) | 21% (62) | 16% (25) | 0.91 |
| support in the functioning of the family | 14% (95) | 10% (12) | 14% (76) | 8% (20) | 15% (52) | 7% (21) | 8% (13) | 0.55 |
| Psychological/emotional | ||||||||
| help in dealing with worries about prognosis | 84% (571) | 75% (90) | 81% (441) | 72% (184) | 88% (303) | 74% (219) | 31% (50) | 0.01 |
| help in dealing with frustration | 87% (592) | 61% (73) | 85% (462) | 71% (182) | 89% (306) | 82% (243) | 41% (66) | 0.01 |
| help in dealing with fears for the family | 58% (394) | 46% (55) | 55% (299) | 60% (154) | 55% (189) | 41% (121) | 20% (32) | 0.01 |
| Sexual | ||||||||
| support in intimate life | 21% (143) | 35% (42) | 28% (152) | 15% (38) | 13% (45) | 21% (62) | 33% (53) | 0.19 |
| Needs | Level % | ||
|---|---|---|---|
| Low | Moderate | High | |
| support in dealing with depression | 34% | 30% | 36% |
| support in dealing with frustration | 14% | 58% | 28% |
| emotional support from loved ones | 0% | 9% | 91% |
| psychological support from support groups | 69% | 20% | 11% |
| psychological support from medical staff | 26% | 41% | 33% |
| psychologist support | 28% | 41% | 31% |
| emotional support of the clergyman | 74% | 11% | 15% |
| talks about passing and death | 34% | 28% | 38% |
| the need for information about the state of health | 0% | 17% | 83% |
| need information about treatment | 2% | 28% | 70% |
| the need for education about the disease on the part of medical personnel | 13% | 38% | 49% |
| the need for information on prognosis | 31% | 41% | 28% |
| the need for information about health opportunities | 11% | 38% | 51% |
| support in the finances of everyday life | 0% | 83% | 17% |
| support in treatment costs | 58% | 25% | 17% |
| help in dealing with symptoms | 20% | 65% | 15% |
| help in everyday functioning | 07% | 23% | 77% |
| changing priorities in life | 40% | 42% | 18% |
| help in dealing with the problem of dying | 9% | 40% | 51% |
| the ability to express feelings | 60% | 25% | 15% |
| planning for the future | 73% | 17% | 10% |
| support in the functioning of the family | 74% | 14% | 12% |
| support in intimate life | 43% | 39% | 18% |
| striving to achieve life goals and desires | 75% | 15% | 10% |
| learning and personal development | 82% | 10% | 8% |
| recognition from other people | 68% | 21% | 11% |
| maintaining social contacts | 66% | 19% | 15% |
| need for faith and religious needs | 64% | 21% | 15% |
| understanding and love | 21% | 31% | 48% |
| being able to be independent and self-sufficient | 32% | 29% | 39% |
| care/medical visits | 9% | 32% | 59% |
| nursing care/visits | 6% | 33% | 61% |
| respect and subjective treatment | 0% | 28% | 72% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lewandowska, A. The Needs of Parents of Children Suffering from Cancer—Continuation of Research. Children 2022, 9, 144. https://doi.org/10.3390/children9020144
Lewandowska A. The Needs of Parents of Children Suffering from Cancer—Continuation of Research. Children. 2022; 9(2):144. https://doi.org/10.3390/children9020144
Chicago/Turabian StyleLewandowska, Anna. 2022. "The Needs of Parents of Children Suffering from Cancer—Continuation of Research" Children 9, no. 2: 144. https://doi.org/10.3390/children9020144
APA StyleLewandowska, A. (2022). The Needs of Parents of Children Suffering from Cancer—Continuation of Research. Children, 9(2), 144. https://doi.org/10.3390/children9020144