


Development of a German Physical Literacy Assessment for Children in the Context of Health Promotion—An Explorative Approach
 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
Socioconomic Status Variable: School-Based Social Index
- Child and youth poverty—measured by the proportion of children living near their primary school and whose parents receive state support for job-seekers (SGB II rate);
- The proportion of children in families whose mother tongue is not German;
- The proportion of children who have immigrated from abroad;
- The proportion of children with special needs in the areas of learning, emotional and social development, and language.
2.2. Anthropometric Data, Age, and Sex
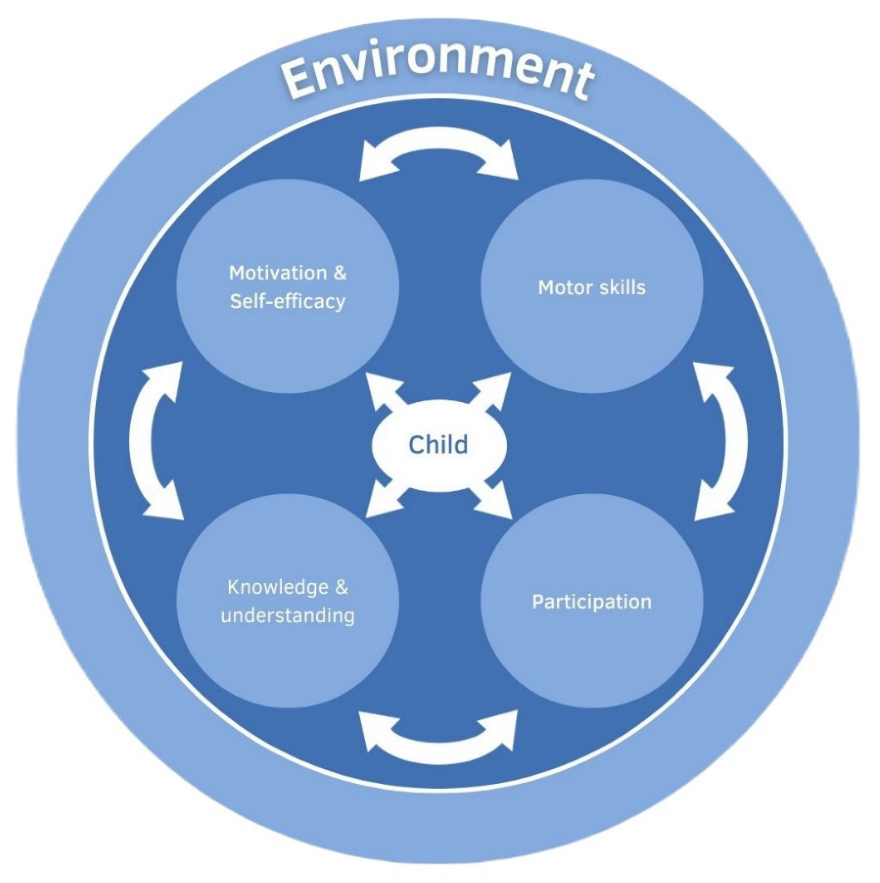
2.3. Operationalisation of the PL Model and Assessment
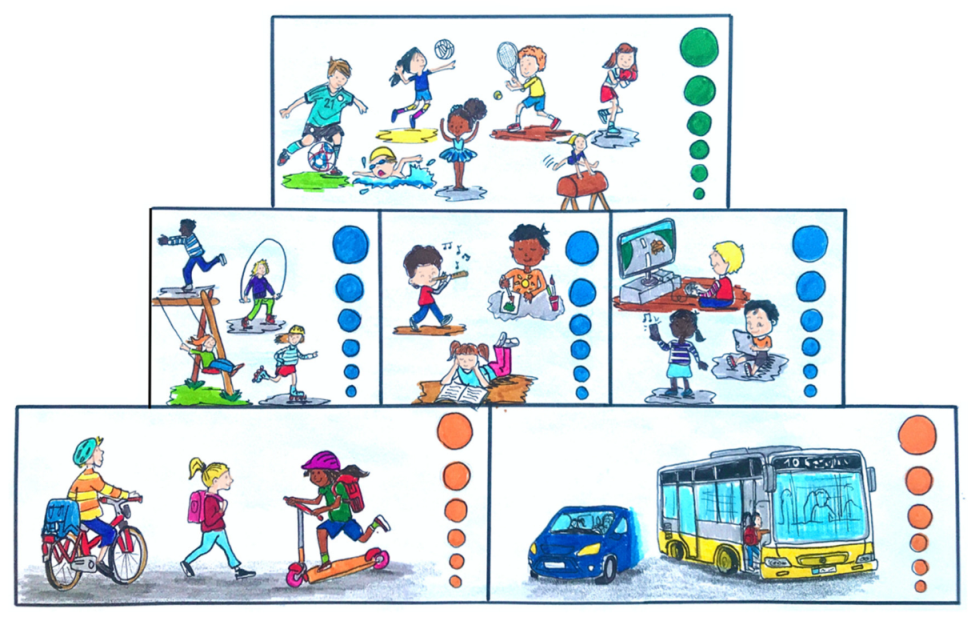
2.3.1. Participation: Physical Activity in Everyday Life and Leisure, Sport, and Sedentary Behaviour
2.3.2. Motivation and Self-Efficacy
2.3.3. Knowledge and Understanding
2.3.4. Motor Skills
2.3.5. Total Scoring
2.4. Statistical Analysis
3. Results
3.1. Anthropometric and Socio-Demographic Data
3.2. Exploratory Factor Analysis
- Scale 1: Knowledge of body and time span (E1, E2);
- Scale 2: Motor skills (A1, A2, A3);
- Scale 3: Self-efficacy (D1, D2);
- Scale 4: Knowledge about feelings (E3);
- Scale 5: Participation and motivation (B2, B3, C2).
3.3. SES and Anthropometric Data
3.4. SES and PL Subdomains
4. Discussion
4.1. Content Validity
4.2. Exploratory Factor Analysis
4.3. Impact of SES
4.4. Strengths und Weaknesses
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Motivation | ||
|---|---|---|
| Autonomous | Controlled | Amotivated |
| become faster | parents want that | just like that |
| become famous | no fun | |
| fun | no answer | |
| keep fit | ||
| is cool | ||
| against boredom | ||
| other kids | ||
| like sports | ||
| meeting friends | ||
| important | ||
| endurance | ||
| career aspiration | ||
| learning something | ||
| exciting | ||
| parents as role models | ||
| getting muscles | ||
| feeling better | ||
| getting thinner/lose weight | ||
| winning | ||
| being good at something | ||
| power | ||
| teamwork | ||
| balance | ||
| simple | ||
| desire | ||
| happy | ||
| try it out | ||
| recognition | ||
| good for health | ||
| role model | ||
| exercise | ||
| play | ||
| getting stronger | ||
| relax | ||
| Feelings | Body | |
|---|---|---|
| Short-Term Effects | Long-Term Effects | |
| Relaxation relaxed freedom stress relief clear your head let out anger self-confidence pride self-confidence fun fun joy good better mood happy cheerful joy strength strong courage courageous | physical strain tired no more power exhausted frazzled lungs/breathing out of breath hurting lungs breathing faster cardiovascular system sweating heart beats faster thirst warm turning red side stitches side stitches muscle ache sore muscles | endurance more endurance flexibility more flexible coordination know how to move speed faster health healthy learning to move learning new things weight loss thin lose weight fitness fit sportier more energy gaining muscles stronger muscles |
| Dimension | Item | n | Min | Max | Mean ± SD | Item Diff. | Factor Loadings | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | |||||||
| Motor Skills | A1 lateral jumping | 563 | 1.00 | 6.00 | 3.38 ± 1.30 | 47.6 | 0.633 | ||||
| A2 standing long jump | 564 | 1.00 | 6.00 | 2.88 ± 1.25 | 37.6 | 0.607 | |||||
| A3 6 min run | 564 | 1.00 | 6.00 | 2.56 ± 1.06 | 31.2 | 0.580 | |||||
| Participation | B1 active everyday life | 559 | 1.00 | 6.00 | 4.66 ± 1.67 | 73.2 | |||||
| B2 active leisure time | 560 | 1.00 | 6.00 | 4.83 ± 1.37 | 76.6 | 0.501 | |||||
| B3 sport | 561 | 1.00 | 6.00 | 5.08 ± 1.36 | 81.6 | 0.462 | |||||
| B4 leisure time non-medial | 558 | 1.00 | 6.00 | 4.51 ± 1.64 | 70.2 | ||||||
| B5 leisure time digital | 561 | 1.00 | 6.00 | 4.48 ± 1.67 | 69.6 | ||||||
| Motivation | C1 motives | 563 | 1.00 | 6.00 | 5.40 ± 1.60 | 88.0 | |||||
| C2 enjoyment | 562 | 1.00 | 6.00 | 5.64 ± 0.77 | 92.8 | 0.420 | |||||
| Sef-Efficacy | D1 confidence | 559 | 1.00 | 6.00 | 4.59 ± 1.77 | 71.8 | 0.593 | ||||
| D2 practice and try again | 556 | 1.00 | 6.00 | 4.67 ± 1.96 | 73.4 | 0.775 | |||||
| Knowledge and Understanding | E1 body | 567 | 1.00 | 4.00 | 1.83 ± 0.82 | 27.7 | 0.958 | ||||
| E2 time span | 567 | 1.00 | 4.00 | 2.11 ± 1.09 | 37.0 | 0.889 | |||||
| E3 feelings | 566 | 1.00 | 4.00 | 1.80 ± 0.62 | 26.6 | 0.992 | |||||
References
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child Adolesc. Health 2020, 4, 23–35. [Google Scholar] [CrossRef] [PubMed]
- Krug, S.; Finger, J.D.; Lange, C.; Richter, A.; Mensink, G. Sport-und Ernährungsverhalten bei Kindern und Jugendlichen in Deutschland–Querschnittergebnisse aus KiGGS Welle 2 und Trends; Robert Koch-Institut: Berlin, Germany, 2018. [Google Scholar]
- Lindqvist, A.K.; Rutberg, S. One Step Forward: Development of a Program Promoting Active School Transportation. JMIR Res. Protoc. 2018, 7, e123. [Google Scholar] [CrossRef] [PubMed]
- Rossi, L.; Behme, N.; Breuer, C. Physical activity of children and adolescents during the COVID-19 pandemic—A scoping review. Int. J. Environ. Res. Public Health 2021, 18, 11440. [Google Scholar] [CrossRef] [PubMed]
- Finger, J.D.; Varnaccia, G.; Borrmann, A.; Lange, C.; Mensink, G. Körperliche Aktivität von Kindern und Jugendlichen in Deutschland—Querschnittergebnisse aus KiGGS Welle 2 und Trends; Epidemiologie und Gesundheitsberichterstattung; Robert Koch-Institut: Berlin, Germany, 2018. [Google Scholar]
- Rauner, A.; Jekauc, D.; Mess, F.; Schmidt, S.; Woll, A. Tracking physical activity in different settings from late childhood to early adulthood in Germany: The MoMo longitudinal study. BMC Public Health 2015, 15, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Kuntz, B.; Waldhauer, J.; Zeiher, J.; Finger, J.D.; Lampert, T. Soziale Unterschiede im Gesundheitsverhalten von Kindern und Jugendlichen in Deutschland–Querschnittergebnisse aus KiGGS Welle 2; Robert Koch-Institut: Berlin, Germany, 2018. [Google Scholar]
- Barriuso, L.; Miqueleiz, E.; Albaladejo, R.; Villanueva, R.; Santos, J.M.; Regidor, E. Socioeconomic position and childhood-adolescent weight status in rich countries: A systematic review, 1990–2013. BMC Pediatr. 2015, 15, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Love, R.; Adams, J.; van Sluijs, E.M.F. Are school-based physical activity interventions effective and equitable? A meta-analysis of cluster randomized controlled trials with accelerometer-assessed activity. Obes. Rev. 2019, 20, 859–870. [Google Scholar] [CrossRef]
- Simonds, S.K. Health education: Facing issues of policy, ethics, and social justice. Health Educ. Monogr. 1978, 6 (Suppl. S1), 18–27. [Google Scholar] [PubMed]
- Batterham, R.; Beauchamp, A.; Osborne, R. Health Literacy, in the International Encyclopedia of Public Health; Academic Press: Cambridge, MA, USA, 2017; pp. 428–437. [Google Scholar]
- Berkman, N.D.; Sheridan, S.L.; Donahue, K.E.; Halpern, D.J.; Crotty, K. Low health literacy and health outcomes: An updated systematic review. Ann. Intern. Med. 2011, 155, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Protheroe, J.; Whittle, R.; Bartlam, B.; Estacio, E.V.; Clark, L.; Kurth, J. Health literacy, associated lifestyle and demographic factors in adult population of an English city: A cross-sectional survey. Health Expect. 2017, 20, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Schaeffer, D.; Berens, E.M.; Gille, S.; Griese, L.; Klinger, J.; de Sombre, S.; Vogt, D.; Hurrelmann, K. Gesundheitskompetenz der Bevölkerung in Deutschland vor und während der Corona Pandemie: Ergebnisse des HLS-GER 2; Bielefeld University, Interdisciplinary Center for Health Competence Research: Bielefeld, Germany, 2021. [Google Scholar]
- Hills, A.P.; Dengel, D.R.; Lubans, D.R. Supporting public health priorities: Recommendations for physical education and physical activity promotion in schools. Prog. Cardiovasc. Dis. 2015, 57, 368–774. [Google Scholar] [CrossRef]
- Whitehead, M. The History and Development of Physical Literacy; International Council of Sport Science and Physical Education: Berlin, Germany, 2013; Volume 65, pp. 21–27. [Google Scholar]
- IPLA. IPLA Definition; International Physical Literacy Association: Wigan, UK, 2017; Available online: https://www.physical-literacy.org.uk/ (accessed on 10 November 2022).
- Carl, J.; Barrett, J.; Wanner, P.; Töpfer, C.; Cairney, J.; Pfeifer, K. The Effectiveness of Physical Literacy Interventions: A Systematic Review with Meta-Analysis. Sport. Med. 2022, 52, 2965–2999. [Google Scholar] [CrossRef] [PubMed]
- Whitehead, M. The concept of physical literacy. Eur. J. Phys. Educ. 2001, 6, 127–138. [Google Scholar] [CrossRef]
- Cairney, J.; Dudley, D.; Kwan, M.; Bulten, R.; Kriellaars, D. Physical Literacy, Physical Activity and Health: Toward an Evidence-Informed Conceptual Model. Sport. Med. 2019, 49, 371–383. [Google Scholar] [CrossRef] [PubMed]
- Hedman-Robertson, A.S.; Allison, K.G.; Kerr, D.L.; Lysoby, L. Historical and contemporary aspects of health literacy in certified health education practice. Am. J. Health Educ. 2021, 52, 323–332. [Google Scholar] [CrossRef]
- Shearer, C.; Goss, H.R.; Edwards, L.C.; Keegan, R.J.; Knowles, Z.R.; Boddy, L.M.; Durden-Myers, E.J.; Foweather, L. How is physical literacy defined? A contemporary update. J. Teach. Phys. Educ. 2018, 37, 237–245. [Google Scholar] [CrossRef]
- Tremblay, M.S.; Longmuir, P.E.; Barnes, J.D.; Belanger, K.; Anderson, K.D.; Bruner, B.; Copeland, J.L.; Nyström, C.D.; Gregg, M.J.; Hall, N.; et al. Physical literacy levels of Canadian children aged 8–12 years: Descriptive and normative results from the RBC Learn to Play–CAPL project. BMC Public Health 2018, 18, 1036. [Google Scholar] [CrossRef]
- Longmuir, P.E.; Boyer, C.; Lloyd, M.; Yang, Y.; Boiarskaia, E.; Zhu, W.; Tremblay, M.S. The Canadian Assessment of Physical Literacy: Methods for children in grades 4 to 6 (8 to 12 years). BMC Public Health 2015, 15, 767. [Google Scholar] [CrossRef]
- Edwards, L.C.; Bryant, A.S.; Keegan, R.; Morgan, K.; Jones, A.M. Definitions, Foundations and Associations of Physical Literacy: A Systematic Review. Sport. Med. 2017, 47, 113–126. [Google Scholar] [CrossRef]
- Cairney, J.; Clark, H.J.; James, M.E.; Mitchell, D.; Dudley, D.A.; Kriellaars, D. The Preschool Physical Literacy Assessment Tool: Testing a New Physical Literacy Tool for the Early Years. Front. Pediatr. 2018, 6, 138. [Google Scholar] [CrossRef] [PubMed]
- Sum, R.K.; Ha, A.S.C.; Cheng, C.F.; Chung, P.K.; Yiu, K.T.C.; Kuo, C.C.; Yu, C.K.; Wang, F.J. Construction and Validation of a Perceived Physical Literacy Instrument for Physical Education Teachers. PLoS ONE 2016, 11, e0155610. [Google Scholar] [CrossRef]
- Liu, Y.; Chen, S. Physical literacy in children and adolescents: Definitions, assessments, and interventions. Eur. Phys. Educ. Rev. 2021, 27, 96–112. [Google Scholar] [CrossRef]
- Naylor, P.-J.; A McKay, H. Prevention in the first place: Schools a setting for action on physical inactivity. Br. J. Sport. Med. 2009, 43, 10–13. [Google Scholar] [CrossRef]
- Wessely, S.; Klaudius, M.; Grauduszus, M.; Hahne, H.; Joisten, C. StuPs—A School- and Community-Based Approach for Participatory Physical Literacy Promotion of Children and their Families—A Study Design and Definition of Physical Literacy. In Proceedings of the 25th Annual Congress of the European College of Sport Science, Virtual, 28–30 October 2020; p. 427. [Google Scholar]
- Wessely, S.; Starke, D.; Weyers, S.; Joisten, C. Closing the gap between practice and science in school- and community-based participatory physical literacy promotion: Study protocol of the StuPs project. BMC Public Health 2021, 21, 642. [Google Scholar] [CrossRef]
- Schräpler, J.; Jeworutzki, S. Konstruktion des Sozialindex für Schulen in Nordrhein-Westfalen; Zentrum für Interdisziplinäre Regionalforschung (ZEFIR), Fakultät für Sozialwissenschaft, Ruhr-Universität Bochum, LOTA: Bochum, Germany, 2021; Volume 38, p. 4 4780.
- Köln, S. Kölner Lebenslagenbericht (1st Cologne Life Situation Report); Institut für Sozialforschung und Gesellschaftspolitik: Cologne, Germany, 2020. [Google Scholar]
- Stolzenberg, H.; Kahl, H.; Bergmann, K.E. Körpermaße bei Kindern und Jugendlichen in Deutschland. Bundesgesundheitsblatt Gesundh. Gesundh. 2007, 50, 659–669. [Google Scholar] [CrossRef]
- WHO. Waist Circumference and Waist-Hip Ratio: Report of a WHO Expert Consultation, Geneva, 8–11 December 2008; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- Kromeyer-Hauschild, K.; Moss, A.; Wabitsch, M. Referenzwerte für den Body-Mass-Index für Kinder, Jugendliche und Erwachsene in Deutschland. Adipositas-Ursachen Folgeerkrankungen Ther. 2015, 9, 123–127. [Google Scholar]
- Wabitsch, M.; Kunze, D. Konsensbasierte (S2) Leitlinie zur Diagnostik, Therapie und Prävention von Übergewicht und Adipositas im Kindes-und Jugendalter. Version der Konsensuskonferenz der AGA am 15.10.2015 in Berlin, Germany. Available online: www.a-g-a.de (accessed on 10 November 2020).
- Jouck, S. Dordel-Koch-Test (DKT): Ein Test zur Erfassung der Motorischen Leistungsfähigkeit im Kindes und Jugendalter; Deutsche Sporthochschule: Köln, Germany, 2009. [Google Scholar]
- Graf, C.; Koch, B.; Dordel, S.; Schindler-Marlow, S.; Icks, A.; Schüller, A.; Bjarnason-Wehrens, B.; Tokarski, W.; Predel, H.-G. Predel, Physical activity, leisure habits and obesity in first-grade children. Eur. J. Cardiovasc. Prev. Rehabil. 2004, 11, 284–290. [Google Scholar] [CrossRef]
- Reynolds, L.; Johnson, R. Is a picture is worth a thousand words? Creating effective questionnaires with pictures. Pract. Assess. Res. Eval. 2011, 16, 8. [Google Scholar]
- Bucksch, J.; Schlicht, W. Sitzende Lebensweise als ein gesundheitlich riskantes Verhalten. Ger. J. Sport. Med. /Dtsch. Z. Sportmed. 2014, 65, 15–21. [Google Scholar] [CrossRef]
- Ainsworth, B.E.; Haskell, W.L.; Whitt, M.C.; Irwin, M.L.; Swartz, A.M.; Strath, S.J.; O’Brien, W.L.; Bassett, D.R., Jr.; Schmitz, K.H.; Emplaincourt, P.O.; et al. Compendium of physical activities: An update of activity codes and MET intensities. Med. Sci. Sport. Exerc. 2000, 32 (Suppl. S1), S498–S504. [Google Scholar] [CrossRef]
- Pate, R.R.; Pratt, M.; Blair, S.N.; Haskell, W.L.; Macera, C.A.; Bouchard, C.; Buchner, D.; Ettinger, W.; Heath, G.W.; King, A.C.; et al. Physical activity and public health. A recommendation from the Centers for Disease Control and Prevention and the American College of Sports Medicine. JAMA 1995, 273, 402–407. [Google Scholar] [CrossRef]
- Deci, E.L.; Ryan, R.M. Self-determination theory. In Handbook of theories of social psychology; van Lange, P.A.M., Kruglanski, A.W., Higgins, E.T., Eds.; Sage Publications Ltd: Thousand Oaks, CA, USA, 2012; pp. 416–436. [Google Scholar] [CrossRef]
- Vallerand, R.J. Deci and Ryan’s self-determination theory: A view from the hierarchical model of intrinsic and extrinsic motivation. Psychol. Inq. 2000, 11, 312–318. [Google Scholar]
- Krapp, A.; Ryan, R.M. Selbstwirksamkeit und Lernmotivation. In Zeitschrift für Pädagogik; Selbstwirksamkeit und Motivationsprozesse in Bildungsinstitutionen; BELTZ: Weinheim, Germany, 2002; Volume 44, pp. 54–82. [Google Scholar]
- Schwarzer, R.; Jerusalem, M. The general self-efficacy scale (GSE). Anxiety Stress Coping 2010, 12, 329–345. [Google Scholar]
- Bandura, A. Social cognitive theory: An agentic perspective. Annu. Rev. Psychol. 2001, 52, 1–26. [Google Scholar] [CrossRef]
- Bandura, A.; Freeman, W.H.; Lightsey, R. Self-Efficacy: The Exercise of Control; Springer: Berlin, Germany, 1999. [Google Scholar]
- Weineck, J. Optimales Training: Leistungsphysiologische Trainingslehre: Unter besonder Berücksichtigung des Kinder-und Jugendtrainings; Perimed Fachbuch: Fürth, Germany, 1980. [Google Scholar]
- van Mechelen, W.; Hlobil, H.; Kemper, H.C. Validation of two running tests as estimates of maximal aerobic power in children. Eur. J. Appl. Physiol. Occup. Physiol. 1986, 55, 503–506. [Google Scholar] [CrossRef]
- Schlag, E.; Ferrari, N.; Koch, B.; Dordel, S.; Joisten, C. Secular trends in motor performance of children and adolescents between 2010 and 2020. Transl. Sport. Med. 2021, 4, 882–891. [Google Scholar] [CrossRef]
- Francis, C.E.; Longmuir, P.E.; Boyer, C.; Andersen, L.B.; Barnes, J.D.; Boiarskaia, E.; Cairney, J.; Faigenbaum, A.D.; Faulkner, G.; Hands, B.P.; et al. The Canadian Assessment of Physical Literacy: Development of a Model of Children’s Capacity for a Healthy, Active Lifestyle Through a Delphi Process. J. Phys. Act. Health 2016, 13, 214–222. [Google Scholar] [CrossRef]
- Cattell, R.B. The Scree Test For The Number Of Factors. Multivar. Behav. Res. 1966, 1, 245–276. [Google Scholar] [CrossRef]
- Gorsuch, R.L. Exploratory factor analysis: Its role in item analysis. J. Personal. Assess. 1997, 68, 532–560. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: London, UK, 2013. [Google Scholar]
- Young, L.; O’Connor, J.; Alfrey, L. Physical literacy: A concept analysis. Sport Educ. Soc. 2020, 25, 946–959. [Google Scholar] [CrossRef]
- Whitehead, M. Definition of physical literacy and clarification of related issues. ICSSPE Bull. 2013, 65, 28. [Google Scholar]
- George, A.M.; Rohr, L.E.; Byrne, J. Impact of Nintendo Wii Games on Physical Literacy in Children: Motor Skills, Physical Fitness, Activity Behaviors, and Knowledge. Sports 2016, 4, 3. [Google Scholar] [CrossRef]
- Rudd, J.R.; Crotti, M.; Fitton-Davies, K.; O’Callaghan, L.; Bardid, F.; Utesch, T.; Roberts, S.; Boddy, L.M.; Cronin, C.J.; Knowles, Z.; et al. Skill Acquisition Methods Fostering Physical Literacy in Early-Physical Education (SAMPLE-PE): Rationale and Study Protocol for a Cluster Randomized Controlled Trial in 5-6-Year-Old Children From Deprived Areas of North West England. Front. Psychol. 2020, 11, 1228. [Google Scholar] [CrossRef]
- Longmuir, P.E.; Gunnell, K.E.; Barnes, J.D.; Belanger, K.; LeDuc, G.; Woodruff, S.J.; Tremblay, M.S. Canadian Assessment of Physical Literacy Second Edition: A streamlined assessment of the capacity for physical activity among children 8 to 12 years of age. BMC Public Health 2018, 18 (Suppl. S2), 1047. [Google Scholar] [CrossRef] [PubMed]
- Starker, A.; Lampert, T.; Worth, A.; Oberger, J.; Kahl, H.; Bös, K. Motorische Leistungsfähigkeit. Bundesgesundheitsblatt Gesundh. Gesundh. 2007, 50, 775–783. [Google Scholar] [CrossRef] [PubMed]
- Pastor-Cisneros, R.; Carlos-Vivas, J.; Muñoz-Bermejo, L.; Adsuar-Sala, J.C.; Merellano-Navarro, E.; Mendoza-Muñoz, M. Association between physical literacy and self-perceived fitness level in children and adolescents. Biology 2021, 10, 1358. [Google Scholar] [CrossRef]
- Sylvia, L.G.; Bernstein, E.E.; Hubbard, J.L.; Keating, L.; Anderson, E.J. Practical guide to measuring physical activity. J. Acad. Nutr. Diet. 2014, 114, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F. Self-report measures of children’s physical activity. J. Sch. Health 1991, 61, 215–219. [Google Scholar] [CrossRef] [PubMed]
- Weston, A.T.; Petosa, R.; Pate, R.R. Validation of an instrument for measurement of physical activity in youth. Med. Sci. Sport. Exerc. 1997, 29, 138–143. [Google Scholar] [CrossRef]
- Anderssen, N.; Jacobs, D.R., Jr.; Aas, H.; Jakobsen, R. Do adolescents and parents report each other’s physical activity accurately? Scand. J. Med. Sci. Sport. 1995, 5, 302–307. [Google Scholar] [CrossRef] [PubMed]
- Pate, R.R.; Almeida, M.J.; McIver, K.L.; Pfeiffer, K.A.; Dowda, M. Validation and calibration of an accelerometer in preschool children. Obesity 2006, 14, 2000–2006. [Google Scholar] [CrossRef]
- Nyström, C.D.; Traversy, G.; Barnes, J.D.; Chaput, J.-P.; Longmuir, P.E.; Tremblay, M.S. Associations between domains of physical literacy by weight status in 8-to 12-year-old Canadian children. BMC Public Health 2018, 18, 1–8. [Google Scholar]
- Comeau, M.E.; Bouchard, D.R.; Levesque, C.; Jonhson, M.J.; Rioux, B.V.; Mayo, A.; Sénéchal, M. Association between functional movements skills and health indicators in children aged between 9 and 12 years old. Int. J. Environ. Res. Public Health 2017, 14, 1010. [Google Scholar] [CrossRef]
- Drewnowski, A. The economics of food choice behavior: Why poverty and obesity are linked. Nestle Nutr. Inst. Workshop Ser. 2012, 73, 95–112. [Google Scholar] [PubMed]
- Morley, D.; Till, K.; Ogilvie, P.; Turner, G. Influences of gender and socioeconomic status on the motor proficiency of children in the UK. Hum. Mov. Sci. 2015, 44, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Krug, S.; Worth, A.; Finger, J.D.; Damerow, S.; Manz, K. Motorische Leistungsfähigkeit 4-bis 10-jähriger Kinder in Deutschland. Bundesgesundheitsblatt Gesundh. Gesundh. 2019, 62, 1242–1252. [Google Scholar] [CrossRef]
- Bühner, M. Einführung in die Test- und Fragebogenkonstruktion; Pearson Deutschland GmbH: Munich, Germany, 2011. [Google Scholar]
- Wessely, S.; Ferrari, N.; Friesen, D.; Grauduszus, M.; Klaudius, M.; Joisten, C. Changes in Motor Performance and BMI of Primary School Children over Time-Influence of the COVID-19 Confinement and Social Burden. Int. J. Environ. Res. Public Health 2022, 19, 4565. [Google Scholar] [CrossRef]
- Currie, C.; Molcho, M.; Boyce, W.; Holstein, B.; Torsheim, T.; Richter, M. Researching health inequalities in adolescents: The development of the Health Behaviour in School-Aged Children (HBSC) family affluence scale. Soc. Sci. Med. 2008, 66, 1429–1436. [Google Scholar] [CrossRef]
- Hilpert, M.; Brockmeier, K.; Dordel, S.; Koch, B.; Weiß, V.; Ferrari, N.; Tokarski, W.; Graf, C. Sociocultural Influence on Obesity and Lifestyle in Children: A Study of Daily Activities, Leisure Time Behavior, Motor Skills, and Weight Status. Obes. Facts 2017, 10, 168–178. [Google Scholar] [CrossRef]
- Kelso, A.; Reimers, A.K.; Abu-Omar, K.; Wunsch, K.; Niessner, C.; Wäsche, H.; Demetriou, Y. Locations of Physical Activity: Where Are Children, Adolescents, and Adults Physically Active? A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 1240. [Google Scholar] [CrossRef] [PubMed]





| Feelings | Body | |
|---|---|---|
| Short-Term Effects | Long-Term Effects | |
| relaxation | physical strain | endurance |
| stress relief | lungs/breathing | flexibility |
| self-confidence | cardiovascular system | coordination |
| fun | side stitches | speed |
| joy | muscle ache | health |
| strength | learning to move | |
| courage | weight loss | |
| fitness | ||
| gaining muscles | ||
| Parameter | Total | Girls | Boys | p-Value | |||
|---|---|---|---|---|---|---|---|
| n | Mean ± SD | n | Mean ± SD | n | Mean ± SD | ||
| age (years) | 567 | 8.0 ± 1.3 | 274 | 8.0 ± 1.2 | 293 | 8.0 ± 1.3 | 0.780 + |
| height (cm) | 567 | 129.7 ± 9.3 | 274 | 129.2 ± 9.0 | 293 | 130.1 ± 9.5 | 0.286 + |
| weight (kg) | 567 | 30.5 ± 8.6 | 274 | 29.9 ± 8.6 | 293 | 31.0 ± 8.7 | 0.110 + |
| waist (cm) | 567 | 61.8 ± 9.5 | 274 | 60.9 ± 9.3 | 293 | 62.7 ± 9.5 | 0.021 + |
| BMI (kg/m2) | 567 | 17.9 ± 3.4 | 274 | 17.6 ± 3.3 | 293 | 18.1 ± 3.4 | 0.093 + |
| BMI-SDS | 567 | 0.64 ± 1.14 | 274 | 0.53 ± 1.14 | 293 | 0.74 ± 1.13 | 0.032 + |
| percentile % | 567 | 274 | 293 | 0.037 ++ | |||
| underweight | 25 | 4.4% | 18 | 6.6% | 7 | 2.4% | |
| normal weight | 370 | 65.3% | 177 | 64.6% | 193 | 65.9% | |
| overweight | 89 | 15.7% | 46 | 16.8% | 43 | 14.7% | |
| obese | 83 | 14.6% | 33 | 12.0% | 50 | 17.1% | |
| Item | Factor | Item Difficulty | ||||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | ||
| A1 lateral jumping | 0.633 | 47.6 | ||||
| A2 standing long jump | 0.607 | 37.6 | ||||
| A3 6 min run | 0.580 | 31.2 | ||||
| B1 active everyday life | 73.2 | |||||
| B2 active leisure time | 0.501 | 76.6 | ||||
| B3 sport | 0.462 | 81.6 | ||||
| B4 leisure time non-medial | 70.2 | |||||
| B5 leisure time digital | 69.6 | |||||
| C1 motives | 88.0 | |||||
| C2 enjoyment | 0.420 | 92.8 | ||||
| D1 confidence | 0.593 | 71.8 | ||||
| D2 practice and try again | 0.775 | 73.4 | ||||
| E1 body | 0.958 | 27.7 | ||||
| E2 time span | 0.889 | 37.0 | ||||
| E3 feelings | 0.992 | 26.6 | ||||
| Parameter | Low SES | High SES | p-Value | ||
|---|---|---|---|---|---|
| n | Mean ± SD | n | Mean ± SD | ||
| female sex % | 215 | 49.2% | 59 | 45.4% | |
| male sex % | 222 | 50.8% | 71 | 44.6% | 0.445 ++ |
| age (years) | 437 | 8.0 ± 1.3 | 130 | 8.3 ± 1.3 | 0.005 + |
| height (cm) | 437 | 128.9 ± 9.3 | 130 | 132.2 ± 8.9 | <0.001 + |
| weight (kg) | 437 | 30.7 ± 9.1 | 130 | 29.7 ± 6.6 | 0.094 + |
| waist (cm) | 437 | 62.4 ± 9.9 | 130 | 59.7 ± 7.5 | 0.002 + |
| BMI (kg/m2) | 437 | 18.2 ± 3.6 | 130 | 16.9 ± 2.3 | <0.001 + |
| BMI-SDS | 437 | 0.75 ± 1.17 | 130 | 0.28 ± 0.93 | <0.001 + |
| percentile % | 437 | 130 | <0.001 ++ | ||
| underweight | 17 | 3.9% | 8 | 6.2% | |
| normal weight | 270 | 61.8% | 100 | 76.9% | |
| overweight | 74 | 16.9% | 15 | 11.5% | |
| obese | 76 | 17.4% | 7 | 5.4% | |
| Parameter | Low SES | High SES | p-Value | r-Value | ||
|---|---|---|---|---|---|---|
| n | Median (IQR) | n | Median (IQR) | |||
| Motor skills | 432 | 8 (3) | 128 | 10 (4) | <0.001 | 0.28 |
| Participation | 429 | 15 (4) | 129 | 13 (4) | <0.001 | 0.22 |
| Motivation and self-efficacy | 424 | 16.5 (4.44) | 130 | 17 (2.5) | 0.012 | 0.11 |
| Knowledge and understanding | 436 | 2.7 (1.2) | 130 | 3.3 (0.9) | <0.001 | 0.20 |
| Overall physical literacy | 416 | 42.5 (7.4) | 127 | 43.2 (8) | 0.025 | 0.10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krenz, L.; Grauduszus, M.; Klaudius, M.; Stolz, I.; Wessely, S.; Joisten, C. Development of a German Physical Literacy Assessment for Children in the Context of Health Promotion—An Explorative Approach. Children 2022, 9, 1908. https://doi.org/10.3390/children9121908
Krenz L, Grauduszus M, Klaudius M, Stolz I, Wessely S, Joisten C. Development of a German Physical Literacy Assessment for Children in the Context of Health Promotion—An Explorative Approach. Children. 2022; 9(12):1908. https://doi.org/10.3390/children9121908
Chicago/Turabian StyleKrenz, Leonie, Martin Grauduszus, Marlen Klaudius, Isabel Stolz, Stefanie Wessely, and Christine Joisten. 2022. "Development of a German Physical Literacy Assessment for Children in the Context of Health Promotion—An Explorative Approach" Children 9, no. 12: 1908. https://doi.org/10.3390/children9121908
APA StyleKrenz, L., Grauduszus, M., Klaudius, M., Stolz, I., Wessely, S., & Joisten, C. (2022). Development of a German Physical Literacy Assessment for Children in the Context of Health Promotion—An Explorative Approach. Children, 9(12), 1908. https://doi.org/10.3390/children9121908