
Are Health Literacy and Physical Literacy Independent Concepts? A Gender-Stratified Analysis in Medical School Students from Croatia


 ,
,  ,
,  ,
,  and
and Highlights
- Health and physical literacy are independent concepts in high school adolescents.
- Body composition was associated with physical literacy and not health literacy.
- Health and physical literacy should be evaluated separately in older adolescents
- Health and physical literacy development should be carried out independently.
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Design of the Study
2.2. Variables and Measurement
2.3. Statistical Analysis
3. Results
4. Discussion
4.1. Gender Differences in Health Literacy and Physical Literacy
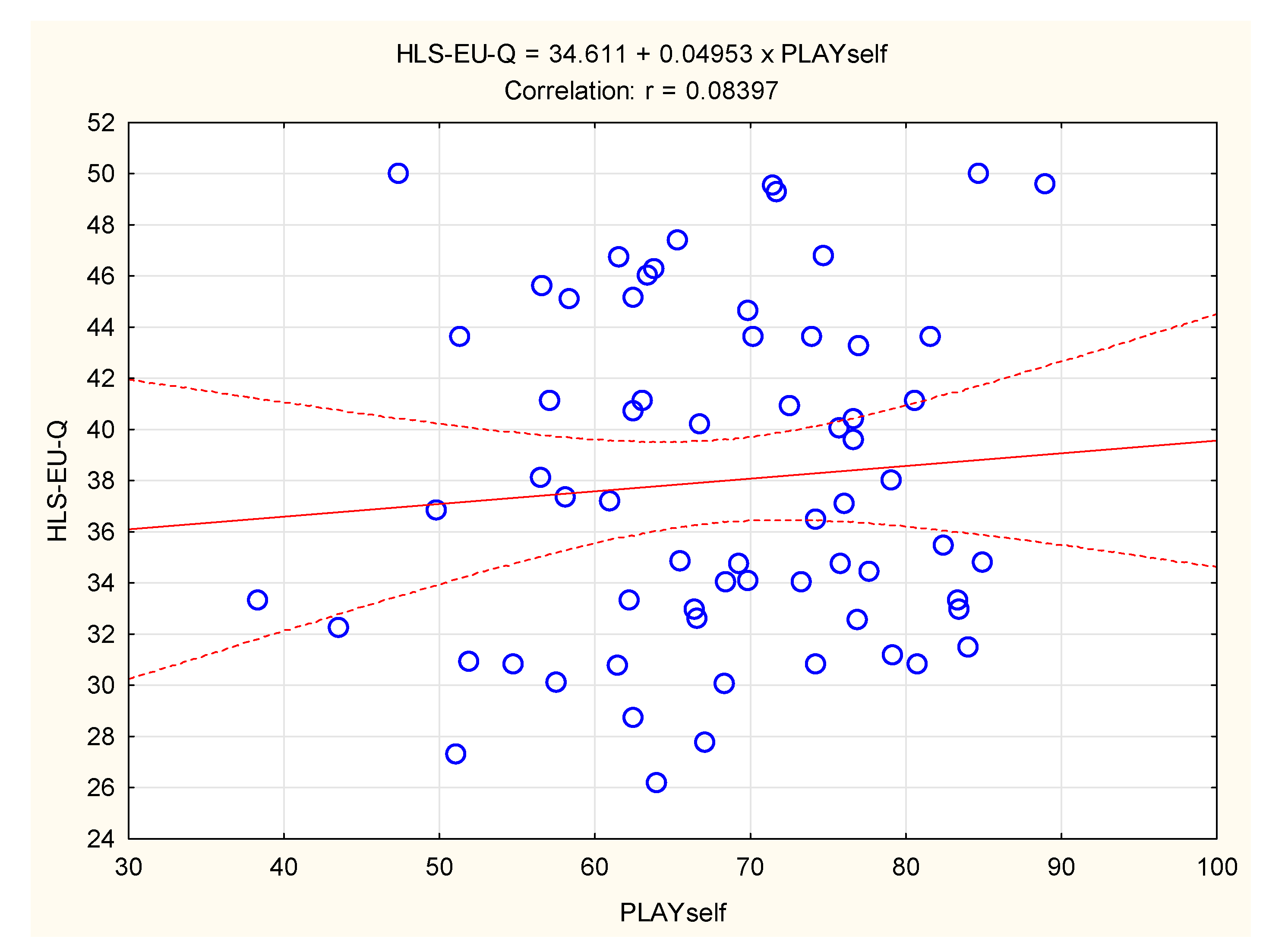
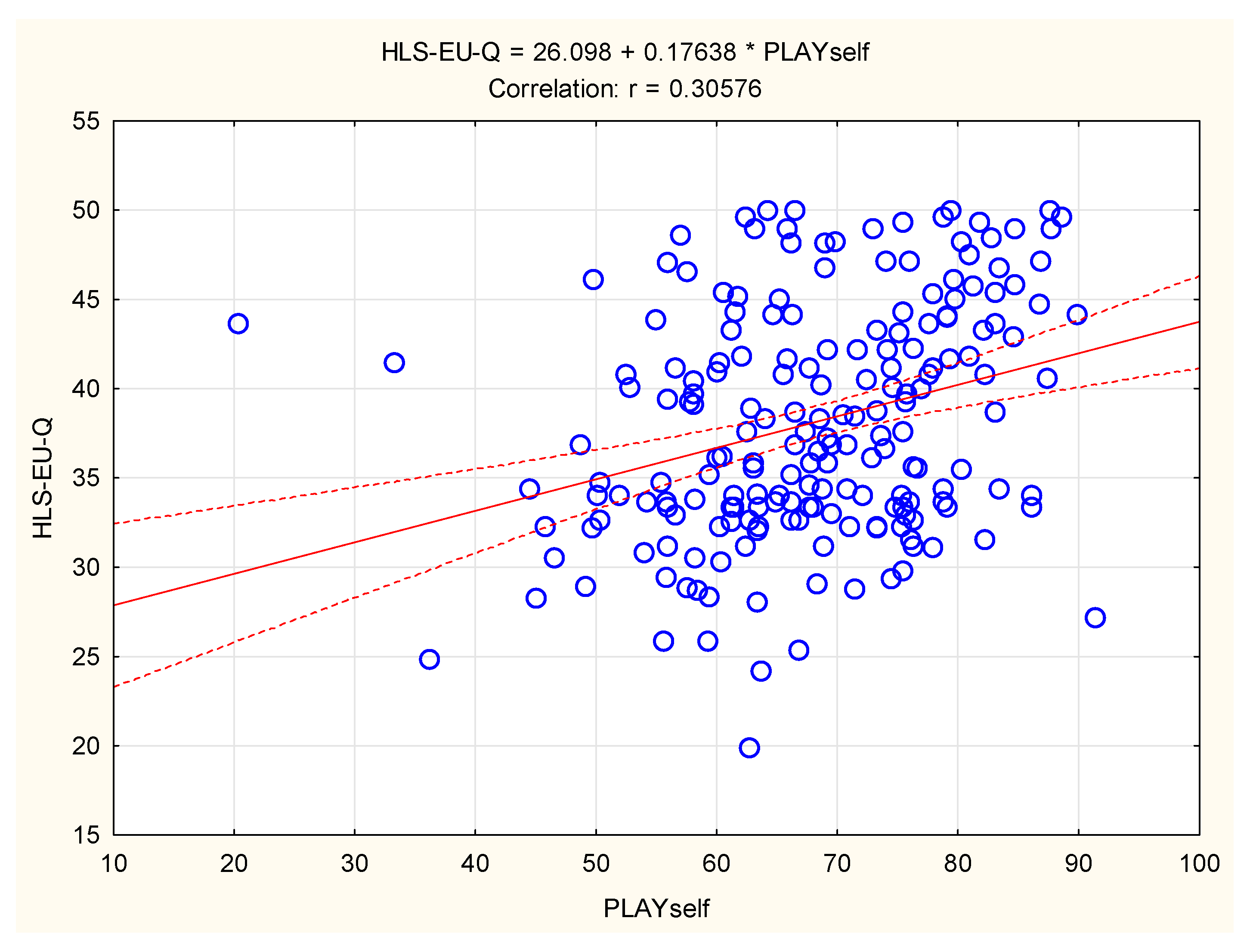
4.2. Associations between Health Literacy and Physical Literacy
4.3. Associations among Body Composition, Health Literacy, and Physical Literacy
4.4. Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- De Bruin, W.B. Judgment and decision making in adolescents. In Judgment and Decision Making As a Skill: Learning, Development and Evolution; Cambridge University Press: New York, NY, USA, 2012; pp. 85–111. [Google Scholar]
- La Torre, G.; Mannocci, A.; Saulle, R.; Sinopoli, A.; D’Egidio, V.; Sestili, C.; Manfuso, R.; Masala, D. GiochiAMO! The protocol of a school based intervention for the promotion of physical activity and nutrition among children. Clin. Ter. 2016, 167, 152–155. [Google Scholar] [CrossRef]
- Neil-Sztramko, S.E.; Caldwell, H.; Dobbins, M. School-based physical activity programs for promoting physical activity and fitness in children and adolescents aged 6 to 18. Cochrane Database Syst. Rev. 2021, 9, Cd007651. [Google Scholar] [CrossRef]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef]
- Cross, S.J.; Lotfipour, S.; Leslie, F.M. Mechanisms and genetic factors underlying co-use of nicotine and alcohol or other drugs of abuse. Am. J. Drug Alcohol Abus. 2017, 43, 171–185. [Google Scholar] [CrossRef]
- Das, J.K.; Lassi, Z.S.; Hoodbhoy, Z.; Salam, R.A. Nutrition for the Next Generation: Older Children and Adolescents. Ann. Nutr. Metab. 2018, 72, 56–64. [Google Scholar] [CrossRef]
- Bauer, U.E.; Briss, P.A.; Goodman, R.A.; Bowman, B.A. Prevention of chronic disease in the 21st century: Elimination of the leading preventable causes of premature death and disability in the USA. Lancet 2014, 384, 45–52. [Google Scholar] [CrossRef]
- Berkman, N.D.; Sheridan, S.L.; Donahue, K.E.; Halpern, D.J.; Crotty, K. Low health literacy and health outcomes: An updated systematic review. Ann. Intern. Med. 2011, 155, 97–107. [Google Scholar] [CrossRef]
- Cornish, K.; Fox, G.; Fyfe, T.; Koopmans, E.; Pousette, A.; Pelletier, C.A. Understanding physical literacy in the context of health: A rapid scoping review. BMC Public Health 2020, 20, 1569. [Google Scholar] [CrossRef]
- World Health Organization. Regional Office for South-East Asia. In Health Literacy Toolkit for Low- and Middle-Income Countries: A Series of Information Sheets to Empower Communities and Strengthen Health Systems; WHO Regional Office for South-East Asia: Geneva, Switzerland, 2015. [Google Scholar]
- Smith, C.; Goss, H.R.; Issartel, J.; Belton, S. Health Literacy in Schools? A Systematic Review of Health-Related Interventions Aimed at Disadvantaged Adolescents. Children 2021, 8, 176. [Google Scholar] [CrossRef]
- Prihanto, J.B.; Nurhayati, F.; Wahjuni, E.S.; Matsuyama, R.; Tsunematsu, M.; Kakehashi, M. Health Literacy and Health Behavior: Associated Factors in Surabaya High School Students, Indonesia. Int. J. Environ. Res. Public Health 2021, 18, 8111. [Google Scholar] [CrossRef]
- Qiao, H.; Wang, X.; Qin, Z.; Wang, N.; Zhang, N.; Xu, F. The relationship between health literacy and health-related quality of life among school-aged children in regional China. Health Qual. Life Outcomes 2021, 19, 262. [Google Scholar] [CrossRef] [PubMed]
- Ozturk Haney, M. Health Literacy and Predictors of Body Weight in Turkish Children. J. Pediatr. Nurs. 2020, 55, e257–e262. [Google Scholar] [CrossRef] [PubMed]
- Lam, L.T.; Yang, L. Is low health literacy associated with overweight and obesity in adolescents: An epidemiology study in a 12–16 years old population, Nanning, China, 2012. Arch. Public Health 2014, 72, 11. [Google Scholar] [CrossRef] [PubMed]
- Buja, A.; Grotto, G.; Montecchio, L.; De Battisti, E.; Sperotto, M.; Bertoncello, C.; Cocchio, S.; Baldovin, T.; Baldo, V. Association between health literacy and dietary intake of sugar, fat and salt: A systematic review. Public Health Nutr. 2021, 24, 2085–2097. [Google Scholar] [CrossRef] [PubMed]
- Martins, J.; Onofre, M.; Mota, J.; Murphy, C.; Repond, R.-M.; Vost, H.; Cremosini, B.; Svrdlim, A.; Markovic, M.; Dudley, D. International approaches to the definition, philosophical tenets, and core elements of physical literacy: A scoping review. Prospects 2021, 50, 13–30. [Google Scholar] [CrossRef]
- Cairney, J.; Dudley, D.; Kwan, M.; Bulten, R.; Kriellaars, D. Physical Literacy, Physical Activity and Health: Toward an Evidence-Informed Conceptual Model. Sports Med. 2019, 49, 371–383. [Google Scholar] [CrossRef]
- Mendoza-Munoz, M.; Barrios-Fernandez, S.; Adsuar, J.C.; Pastor-Cisneros, R.; Risco-Gil, M.; Garcia-Gordillo, M.A.; Carlos-Vivas, J. Influence of Body Composition on Physical Literacy in Spanish Children. Biology 2021, 10, 482. [Google Scholar] [CrossRef]
- Caldwell, H.A.T.; Di Cristofaro, N.A.; Cairney, J.; Bray, S.R.; MacDonald, M.J.; Timmons, B.W. Physical Literacy, Physical Activity, and Health Indicators in School-Age Children. Int. J. Environ. Res. Public Health 2020, 17, 5367. [Google Scholar] [CrossRef]
- Bagherniya, M.; Taghipour, A.; Sharma, M.; Sahebkar, A.; Contento, I.R.; Keshavarz, S.A.; Mostafavi Darani, F.; Safarian, M. Obesity intervention programs among adolescents using social cognitive theory: A systematic literature review. Health Educ. Res. 2018, 33, 26–39. [Google Scholar] [CrossRef]
- Tsang, S.K.; Hui, E.K.; Law, B.C. Self-efficacy as a positive youth development construct: A conceptual review. Sci. World J. 2012, 2012, 452327. [Google Scholar] [CrossRef]
- Hassan, S.; Masoud, O. Online health information seeking and health literacy among non-medical college students: Gender differences. J. Public Health 2020, 29, 1267–1273. [Google Scholar] [CrossRef]
- Lee, H.Y.; Lee, J.; Kim, N.K. Gender Differences in Health Literacy Among Korean Adults: Do Women Have a Higher Level of Health Literacy Than Men? Am. J. Mens. Health 2015, 9, 370–379. [Google Scholar] [CrossRef] [PubMed]
- Kirchengast, S. Gender Differences in Body Composition from Childhood to Old Age: An Evolutionary Point of View. J. Life Sci. 2010, 2, 1–10. [Google Scholar] [CrossRef]
- Caldwell, H.A.T.; Proudfoot, N.A.; DiCristofaro, N.A.; Cairney, J.; Bray, S.R.; Timmons, B.W. Preschool to School-Age Physical Activity Trajectories and School-Age Physical Literacy: A Longitudinal Analysis. J. Phys. Act. Health 2022, 19, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Geets Kesic, M.; Penjak, A.; Sekulic, D. Reliability and validity of the croatian version of the european health literacy survey questionnaire. In Proceedings of the Montenegrin Journal of Sports Science and Medicine, Abstracts from the 19th Annual Scientific Conference of Montenegrin Sports Academy “Sport, Physical Activity and Health: Contemporary Perspectives”, Dubrovnik, Croatia, 7–10 April 2022. [Google Scholar]
- Hulley, S.B.; Cummings, S.R.; Browner, W.S.; Grady, D.; Hearst, N.; Newman, T.B. Designing clinical research: An epidemiologic approach. In Designing Clinical Research: An Epidemiologic Approach; Lippincott Williams: Philadelphia, PA, USA, 2001; p. 336. [Google Scholar]
- Sørensen, K.; Van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, K.; Van den Broucke, S.; Pelikan, J.M.; Fullam, J.; Doyle, G.; Slonska, Z.; Kondilis, B.; Stoffels, V.; Osborne, R.H.; Brand, H. Measuring health literacy in populations: Illuminating the design and development process of the European Health Literacy Survey Questionnaire (HLS-EU-Q). BMC Public Health 2013, 13, 948. [Google Scholar] [CrossRef]
- Jefferies, P.; Bremer, E.; Kozera, T.; Cairney, J.; Kriellaars, D. Psychometric properties and construct validity of PLAYself: A self-reported measure of physical literacy for children and youth. Appl. Physiol. Nutr. Metab. 2021, 46, 579–588. [Google Scholar] [CrossRef]
- Gilic, B.; Malovic, P.; Sunda, M.; Maras, N.; Zenic, N. Adolescents with Higher Cognitive and Affective Domains of Physical Literacy Possess Better Physical Fitness: The Importance of Developing the Concept of Physical Literacy in High Schools. Children 2022, 9, 796. [Google Scholar] [CrossRef]
- Sunda, M.; Gilic, B.; Sekulic, D.; Matic, R.; Drid, P.; Alexe, D.I.; Cucui, G.G.; Lupu, G.S. Out-of-School Sports Participation Is Positively Associated with Physical Literacy, but What about Physical Education? A Cross-Sectional Gender-Stratified Analysis during the COVID-19 Pandemic among High-School Adolescents. Children 2022, 9, 753. [Google Scholar] [CrossRef]
- Caldwell, H.A.; Di Cristofaro, N.A.; Cairney, J.; Bray, S.R.; Timmons, B.W. Measurement properties of the Physical Literacy Assessment for Youth (PLAY) Tools. Appl. Physiol. Nutr. Metab. 2021, 46, 571–578. [Google Scholar] [CrossRef]
- Tremblay, M.S.; Longmuir, P.E.; Barnes, J.D.; Belanger, K.; Anderson, K.D.; Bruner, B.; Copeland, J.L.; Delisle Nystrom, C.; Gregg, M.J.; Hall, N.; et al. Physical literacy levels of Canadian children aged 8–12 years: Descriptive and normative results from the RBC Learn to Play-CAPL project. BMC Public Health 2018, 18, 1036. [Google Scholar] [CrossRef] [PubMed]
- Stodden, D.F.; Goodway, J.D.; Langendorfer, S.J.; Roberton, M.A.; Rudisill, M.E.; Garcia, C.; Garcia, L.E. A Developmental Perspective on the Role of Motor Skill Competence in Physical Activity: An Emergent Relationship. Quest 2008, 60, 290–306. [Google Scholar] [CrossRef]
- Wong, K. Gender differences in mental health literacy of university students. West. Undergrad. Psychol. J. 2016, 4. [Google Scholar]
- Riiser, K.; Helseth, S.; Haraldstad, K.; Torbjornsen, A.; Richardsen, K.R. Adolescents’ health literacy, health protective measures, and health-related quality of life during the COVID-19 pandemic. PLoS ONE 2020, 15, e0238161. [Google Scholar] [CrossRef]
- Nutbeam, D. The evolving concept of health literacy. Soc. Sci. Med. 2008, 67, 2072–2078. [Google Scholar] [CrossRef]
- Geets Kesic, M.; Gilic, B.; Cerkez Zovko, I.; Drid, P.; Korovljev, D.; Sekulic, D. Differential impact of COVID-19 lockdown on physical activity in younger and older adolescents—Prospective study. Med. Pr. 2021, 72, 633–643. [Google Scholar] [CrossRef]
- Lynch, T.; Soukup, G.J. “Physical education”, “health and physical education”, “physical literacy” and “health literacy”: Global nomenclature confusion. Cogent Educ. 2016, 3, 1217820. [Google Scholar] [CrossRef]
- Freedman, D.S.; Perry, G. Body composition and health status among children and adolescents. Prev. Med. 2000, 31, S34–S53. [Google Scholar] [CrossRef]
- Sharif, I.; Blank, A.E. Relationship between child health literacy and body mass index in overweight children. Patient Educ. Couns. 2010, 79, 43–48. [Google Scholar] [CrossRef]
- Chari, R.; Warsh, J.; Ketterer, T.; Hossain, J.; Sharif, I. Association between health literacy and child and adolescent obesity. Patient Educ. Couns. 2014, 94, 61–66. [Google Scholar] [CrossRef]
- Klinker, C.D.; Aaby, A.; Ringgaard, L.W.; Hjort, A.V.; Hawkins, M.; Maindal, H.T. Health Literacy is Associated with Health Behaviors in Students from Vocational Education and Training Schools: A Danish Population-Based Survey. Int. J. Environ. Res. Public Health 2020, 17, 671. [Google Scholar] [CrossRef]
- Rademakers, J.; Hahnraths, M.T.H.; van Schayck, O.C.P.; Heijmans, M. Children’s Health Literacy in Relation to Their BMI z-Score, Food Intake, and Physical Activity: A Cross-Sectional Study among 8–11-Year-Old Children in The Netherlands. Children 2022, 9, 925. [Google Scholar] [CrossRef] [PubMed]
- Flegal, K.M.; Kit, B.K.; Orpana, H.; Graubard, B.I. Association of all-cause mortality with overweight and obesity using standard body mass index categories: A systematic review and meta-analysis. JAMA 2013, 309, 71–82. [Google Scholar] [CrossRef] [PubMed]
- Huck, W. Reading Statistics and Research; Pearson Education: Boston, MA, USA; University of Tennessee: Knoxville, TN, USA, 2012; p. 593. [Google Scholar]
- Rizzo, N.S.; Ruiz, J.R.; Hurtig-Wennlöf, A.; Ortega, F.B.; Sjöström, M. Relationship of physical activity, fitness, and fatness with clustered metabolic risk in children and adolescents: The European youth heart study. J. Pediatr. 2007, 150, 388–394. [Google Scholar] [CrossRef]
- Golob Jančič, S.; Močnik, M.; Švigelj, M.; Marčun Varda, N. Body Composition and Cardiovascular Risk Factors in a Paediatric Population. Children 2022, 9, 603. [Google Scholar] [CrossRef]
- Delisle Nyström, C.; Traversy, G.; Barnes, J.D.; Chaput, J.P.; Longmuir, P.E.; Tremblay, M.S. Associations between domains of physical literacy by weight status in 8- to 12-year-old Canadian children. BMC Public Health 2018, 18, 1043. [Google Scholar] [CrossRef] [PubMed]
- Comeau, M.E.; Bouchard, D.R.; Levesque, C.; Jonhson, M.J.; Rioux, B.V.; Mayo, A.; Sénéchal, M. Association between Functional Movements Skills and Health Indicators in Children Aged between 9 and 12 Years Old. Int. J. Environ. Res. Public Health 2017, 14, 1010. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Boys (n = 68) | Girls (n = 198) | t-Test | ||||
|---|---|---|---|---|---|---|
| Mean | Std. Dev. | Mean | Std. Dev. | t-Value | p-Value | |
| Age (years) | 17.08 | 1.31 | 16.96 | 1.41 | 0.62 | 0.53 |
| Body height (cm) | 180.97 | 14.30 | 169.27 | 6.53 | 9.10 | 0.001 |
| Body mass (kg) | 74.40 | 12.49 | 64.48 | 11.15 | 6.13 | 0.001 |
| BMI (kg/m2) | 24.06 | 15.30 | 22.44 | 3.29 | 1.40 | 0.16 |
| Fat mass (kg) | 12.73 | 5.59 | 18.30 | 7.36 | −5.70 | 0.001 |
| Fat mass (%) | 16.61 | 4.98 | 27.42 | 6.39 | −12.69 | 0.001 |
| Free fat mass (kg) | 61.68 | 8.55 | 46.36 | 5.32 | 17.31 | 0.001 |
| Muscle mass (kg) | 58.90 | 8.11 | 43.89 | 4.45 | 19.04 | 0.001 |
| Visceral fat (kg) | 2.14 | 1.51 | 1.81 | 1.21 | 1.18 | 0.24 |
| PLAYself environment (sub-score) | 50.86 | 15.23 | 51.16 | 15.43 | −0.13 | 0.89 |
| PLAYself self-description (sub-score) | 73.68 | 14.51 | 70.24 | 15.06 | 1.63 | 0.10 |
| PLAYself literacy (sub-score) | 72.51 | 16.25 | 83.11 | 17.31 | −4.39 | 0.001 |
| PLAYself numeracy (sub-score) | 60.06 | 21.28 | 61.07 | 22.70 | −0.32 | 0.75 |
| PLAYself physical literacy (sub-score) | 82.59 | 18.04 | 86.60 | 19.45 | −1.48 | 0.14 |
| PLAYself total (score) | 68.05 | 11.04 | 68.03 | 11.36 | 0.01 | 0.99 |
| HLS- EU-Q (score) | 37.87 | 6.53 | 38.06 | 6.54 | −0.21 | 0.83 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age (1) | - | |||||||||||||
| Body height (2) | 0.10 | |||||||||||||
| Body mass (3) | 0.25 * | 0.28 | ||||||||||||
| BMI (4) | 0.03 | −0.13 | 0.91 * | |||||||||||
| Fat mass kg (5) | 0.03 | 0.03 | 0.85 * | 0.87 * | ||||||||||
| Fat mass % (6) | 0.09 | −0.08 | 0.65 * | 0.71 * | 0.95 * | |||||||||
| Free fat mass (7) | 0.35 * | 0.40 * | 0.95 * | 0.81 * | 0.64 * | 0.37 | ||||||||
| Muscle mass (8) | 0.35 | 0.40 * | 0.95 * | 0.81 * | 0.63 * | 0.37 | 0.99 * | |||||||
| Visceral fat (9) | 0.30 | −0.19 | 0.73 * | 0.83 * | 0.84 * | 0.76 * | 0.55 * | 0.56 * | ||||||
| PLAYself environment (10) | 0.02 | −0.03 | 0.30 | 0.30 | 0.39 * | 0.40 * | 0.20 | 0.20 | 0.24 | |||||
| PLAYself self-description (11) | 0.04 | −0.04 | 0.52 * | 0.54 * | 0.59 * | 0.55 * | 0.40 * | 0.41 * | 0.57 * | 0.62 * | ||||
| PLAYself literacy (12) | 0.21 | −0.07 | 0.03 | 0.06 | 0.09 | 0.10 | −0.01 | −0.01 | 0.13 | 0.09 | 0.30 | |||
| PLAYself numeracy (13) | 0.03 | 0.21 | 0.14 | 0.05 | −0.03 | −0.12 | 0.23 | 0.23 | 0.00 | 0.06 | 0.27 | 0.64 * | ||
| PLAYself physical literacy (14) | 0.14 | −0.34 | −0.08 | 0.05 | 0.03 | 0.08 | −0.14 | −0.14 | 0.15 | 0.09 | 0.38 | 0.34 | 0.31 | |
| PLAYself total (15) | 0.05 | −0.06 | −0.40 * | −0.43 * | −0.47 * | −0.44 * | 0.31 | 0.31 | 0.45 * | 0.67 * | 0.92 * | 0.55 * | 0.52 * | 0.53 * |
| HLS-EU-Q (16) | 0.04 | 0.19 | 0.08 | −0.02 | 0.12 | 0.15 | 0.05 | 0.04 | 0.01 | 0.29 | 0.34 | −0.15 | 0.09 | 0.28 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age (1) | - | |||||||||||||
| Body height (2) | 0.04 | |||||||||||||
| Body mass (3) | 0.03 | 0.66 * | ||||||||||||
| BMI (4) | 0.01 | 0.28 * | 0.90 * | |||||||||||
| Fat mass kg (5) | 0.01 | 0.56 * | 0.97 * | 0.92 * | ||||||||||
| Fat mass % (6) | 0.03 | 0.48 * | 0.89 * | 0.87 * | 0.97 * | |||||||||
| Free fat mass (7) | 0.09 | 0.59 * | 0.73 * | 0.59 * | 0.61 * | 0.49 * | ||||||||
| Muscle mass (8) | 0.09 | 0.73 * | 0.89 * | 0.71 * | 0.74 * | 0.59 * | 0.81 * | |||||||
| Visceral fat (9) | −0.17 | 0.31 * | 0.86 * | 0.92 * | 0.91 * | 0.85 * | 0.52* | 0.62 * | ||||||
| PLAYself environment (10) | −0.21 * | −0.04 | −0.07 | −0.06 | −0.09 | −0.08 | 0.11 | −0.02 | −0.14 | |||||
| PLAYself self-description (11) | 0.07 | 0.00 | −0.11 | −0.14 | −0.16 | −0.19 | −0.01 | −0.03 | −0.16 | 0.41 * | ||||
| PLAYself literacy (12) | 0.13 | 0.05 | 0.15 | 0.17 | 0.19 | 0.21 | 0.07 | 0.07 | 0.16 | 0.12 | 0.05 | |||
| PLAYself numeracy (13) | 0.11 | −0.01 | −0.01 | −0.02 | −0.04 | −0.07 | 0.13 | 0.04 | −0.02 | −0.05 | 0.11 | 0.20 | ||
| PLAYself physical literacy (14) | 0.03 | 0.16 | 0.07 | −0.02 | 0.05 | 0.02 | 0.11 | 0.10 | −0.01 | 0.25 * | 0.39 * | 0.19 | 0.43 * | |
| PLAYself total (15) | −0.04 | 0.03 | −0.05 | −0.09 | −0.09 | −0.12 | 0.10 | 0.02 | −0.12 | 0.61 * | 0.85 * | 0.32 * | 0.42 * | 0.66 * |
| HLS- EU-Q (16) | 0.19 * | −0.08 | −0.01 | 0.04 | 0.00 | 0.05 | 0.03 | −0.06 | −0.03 | 0.05 | 0.26 * | 0.27 * | 0.38 * | 0.04 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kesic, M.G.; Peric, M.; Gilic, B.; Manojlovic, M.; Drid, P.; Modric, T.; Znidaric, Z.; Zenic, N.; Pajtler, A. Are Health Literacy and Physical Literacy Independent Concepts? A Gender-Stratified Analysis in Medical School Students from Croatia. Children 2022, 9, 1231. https://doi.org/10.3390/children9081231
Kesic MG, Peric M, Gilic B, Manojlovic M, Drid P, Modric T, Znidaric Z, Zenic N, Pajtler A. Are Health Literacy and Physical Literacy Independent Concepts? A Gender-Stratified Analysis in Medical School Students from Croatia. Children. 2022; 9(8):1231. https://doi.org/10.3390/children9081231
Chicago/Turabian StyleKesic, Marijana Geets, Mia Peric, Barbara Gilic, Marko Manojlovic, Patrik Drid, Toni Modric, Zeljka Znidaric, Natasa Zenic, and Aleksander Pajtler. 2022. "Are Health Literacy and Physical Literacy Independent Concepts? A Gender-Stratified Analysis in Medical School Students from Croatia" Children 9, no. 8: 1231. https://doi.org/10.3390/children9081231
APA StyleKesic, M. G., Peric, M., Gilic, B., Manojlovic, M., Drid, P., Modric, T., Znidaric, Z., Zenic, N., & Pajtler, A. (2022). Are Health Literacy and Physical Literacy Independent Concepts? A Gender-Stratified Analysis in Medical School Students from Croatia. Children, 9(8), 1231. https://doi.org/10.3390/children9081231