
Burden of Traumatic Brain Injuries in Children and Adolescents in Europe: Hospital Discharges, Deaths and Years of Life Lost

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Study Design, Population, and Setting
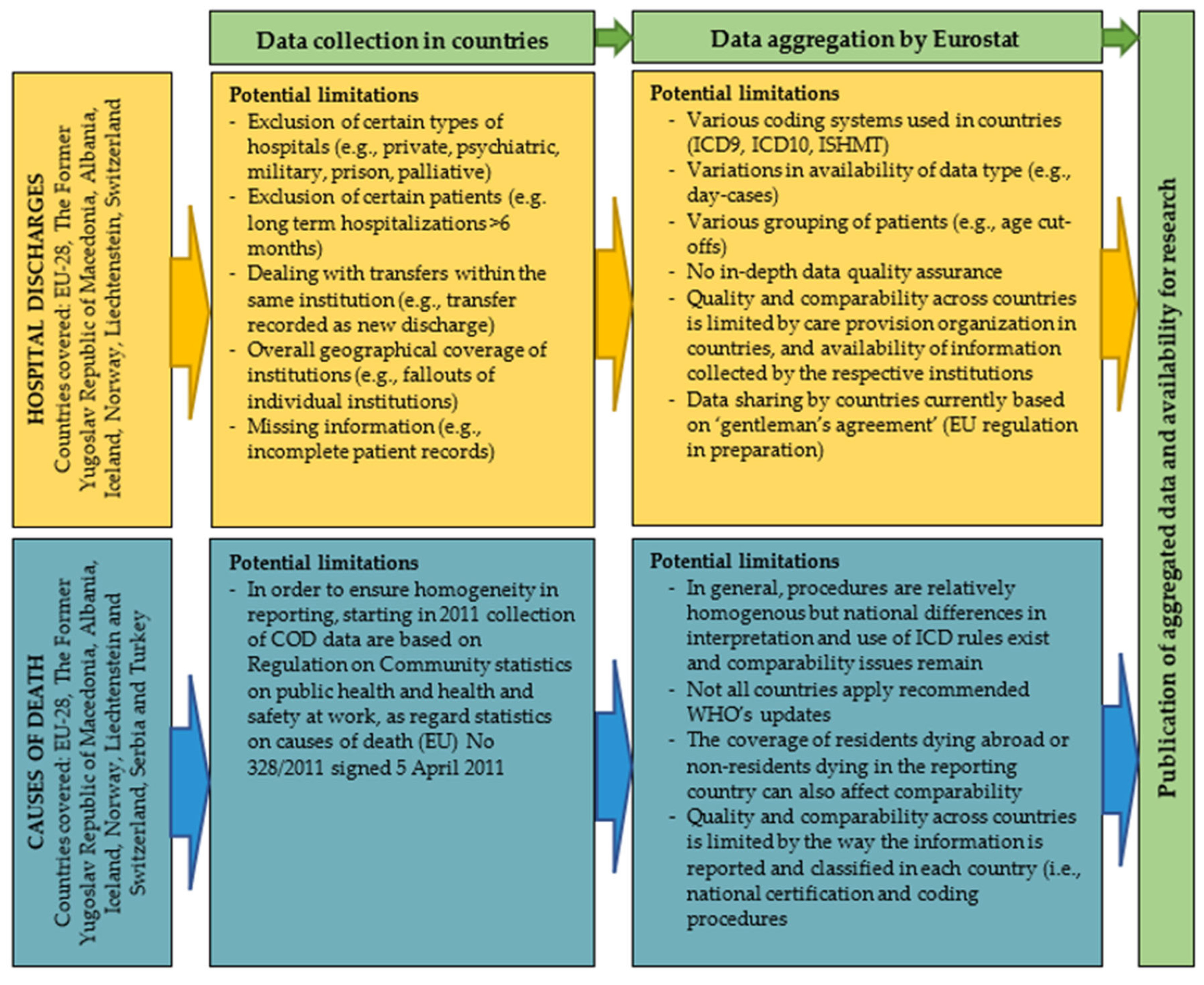
2.2. Data Sources

2.3. Case Definition
2.4. Variable Definitions and Calculations
3. Results
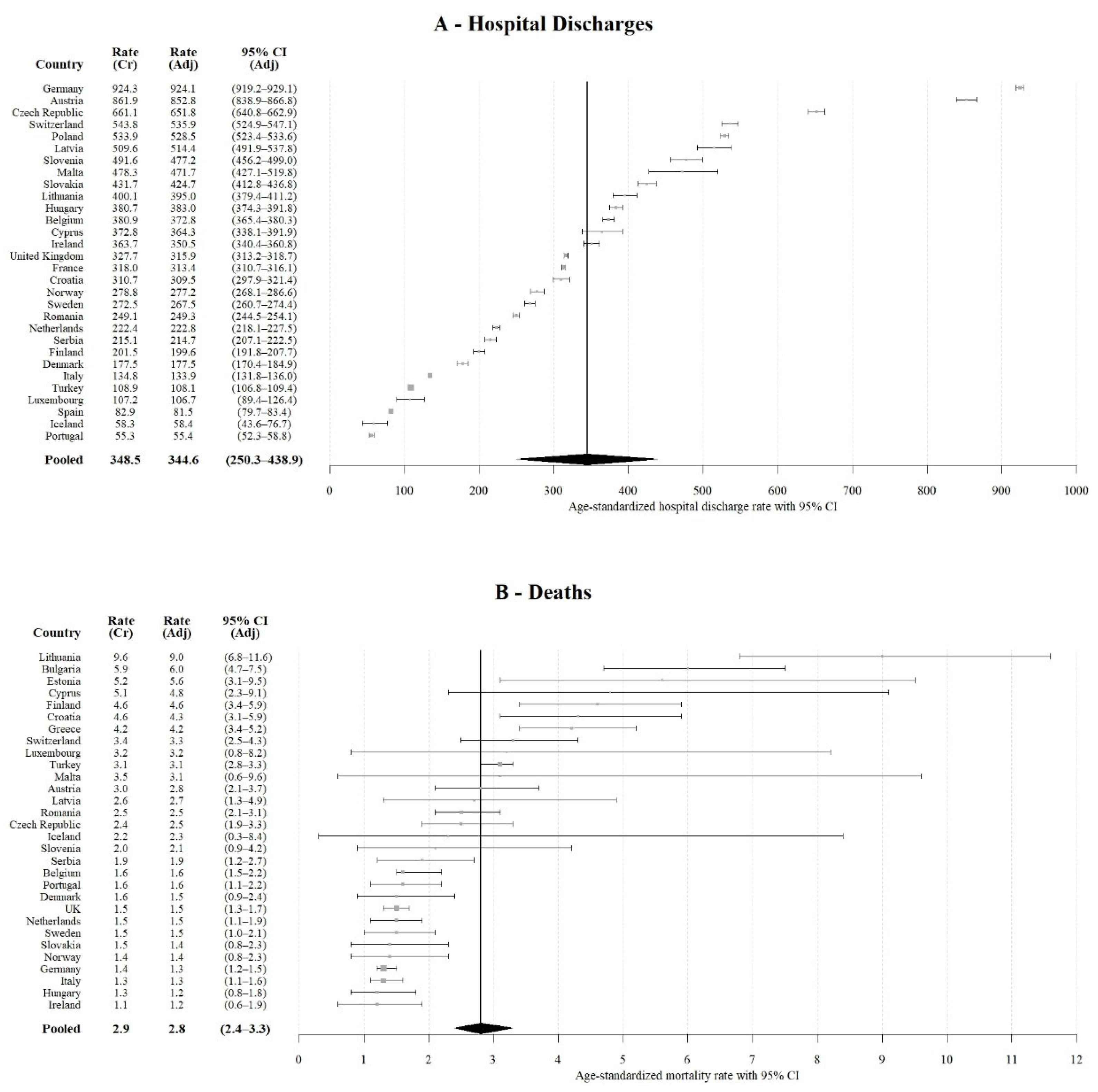
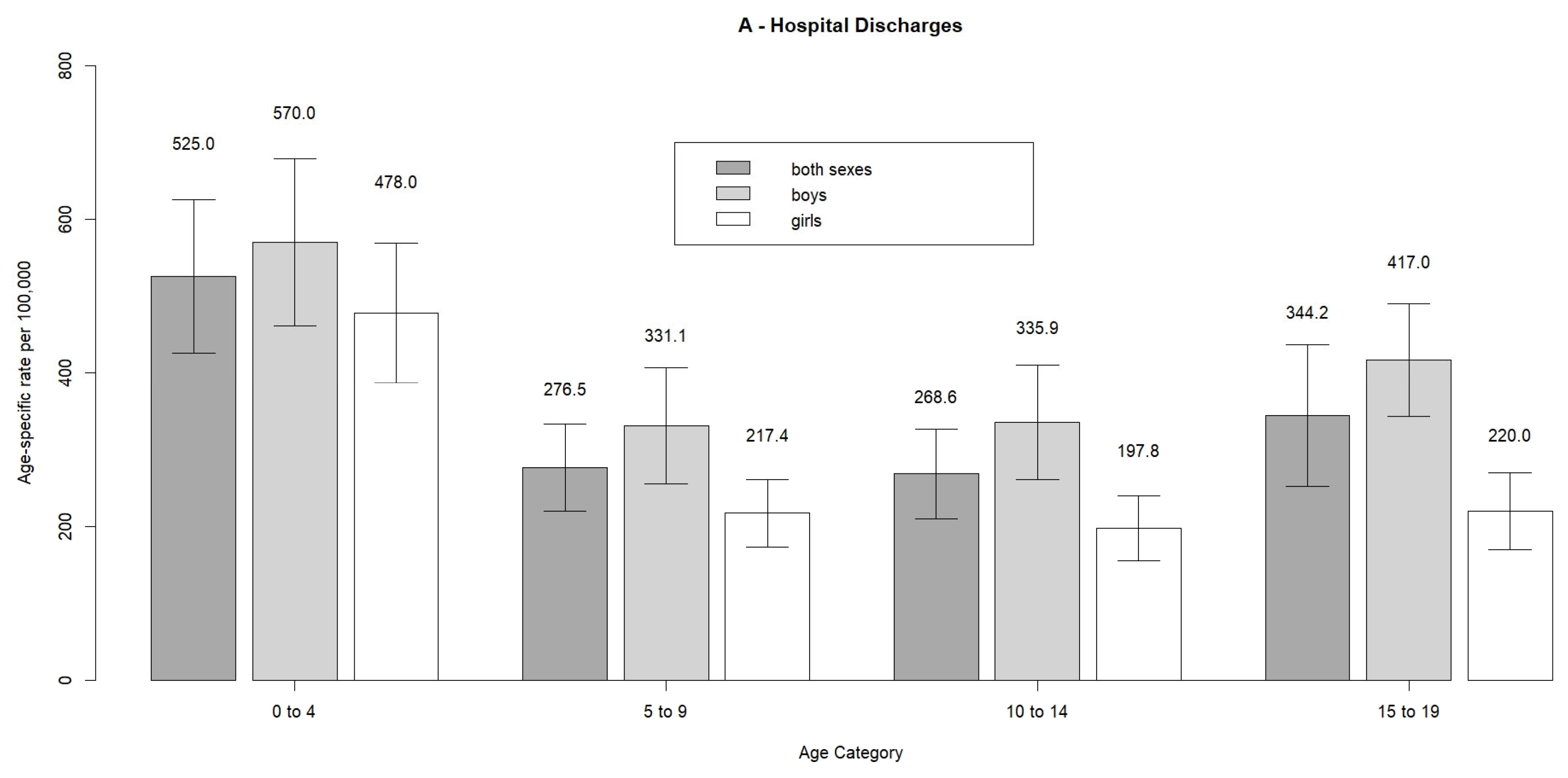
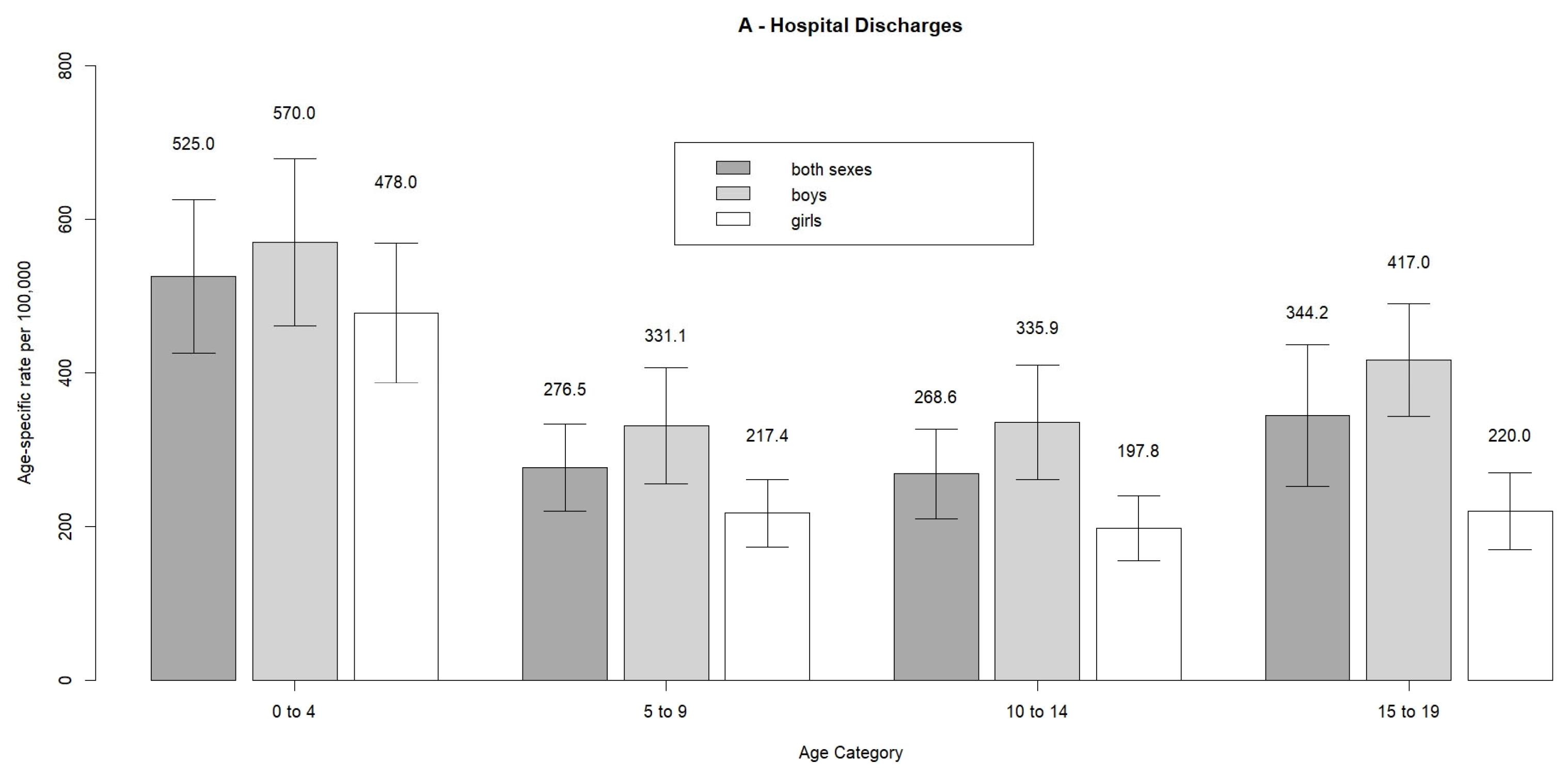
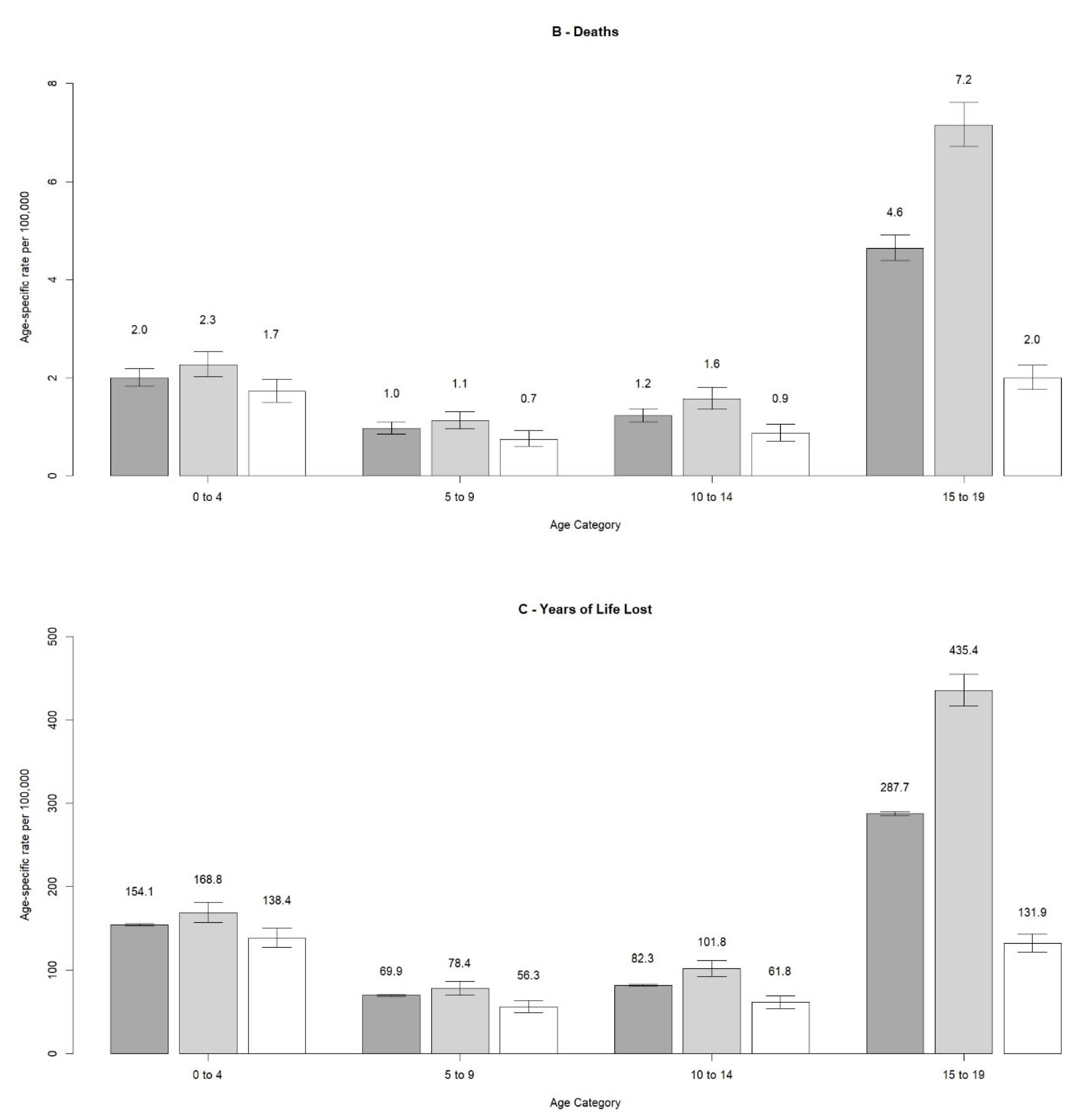
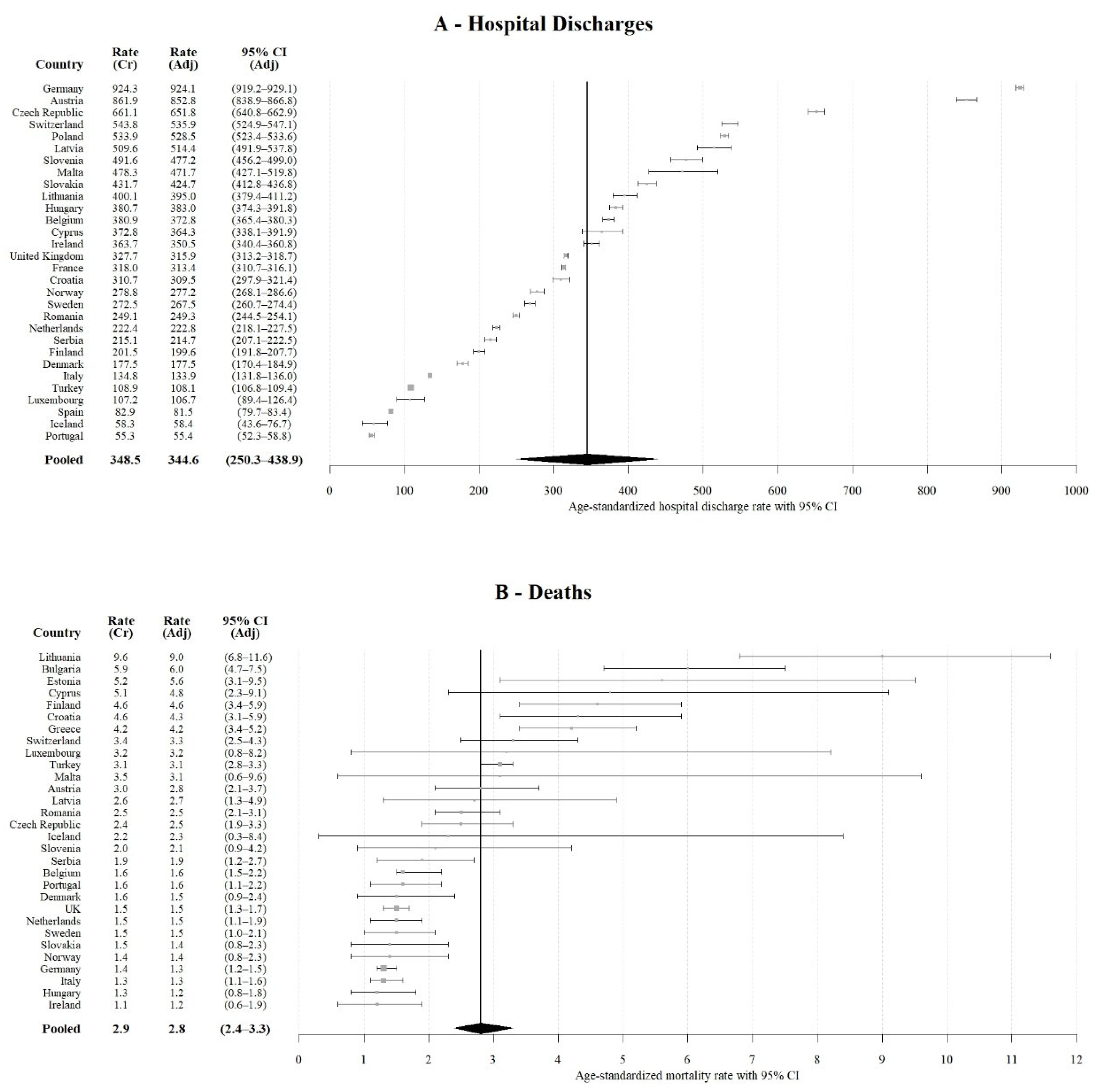
3.1. Hospital Discharges Due to TBI
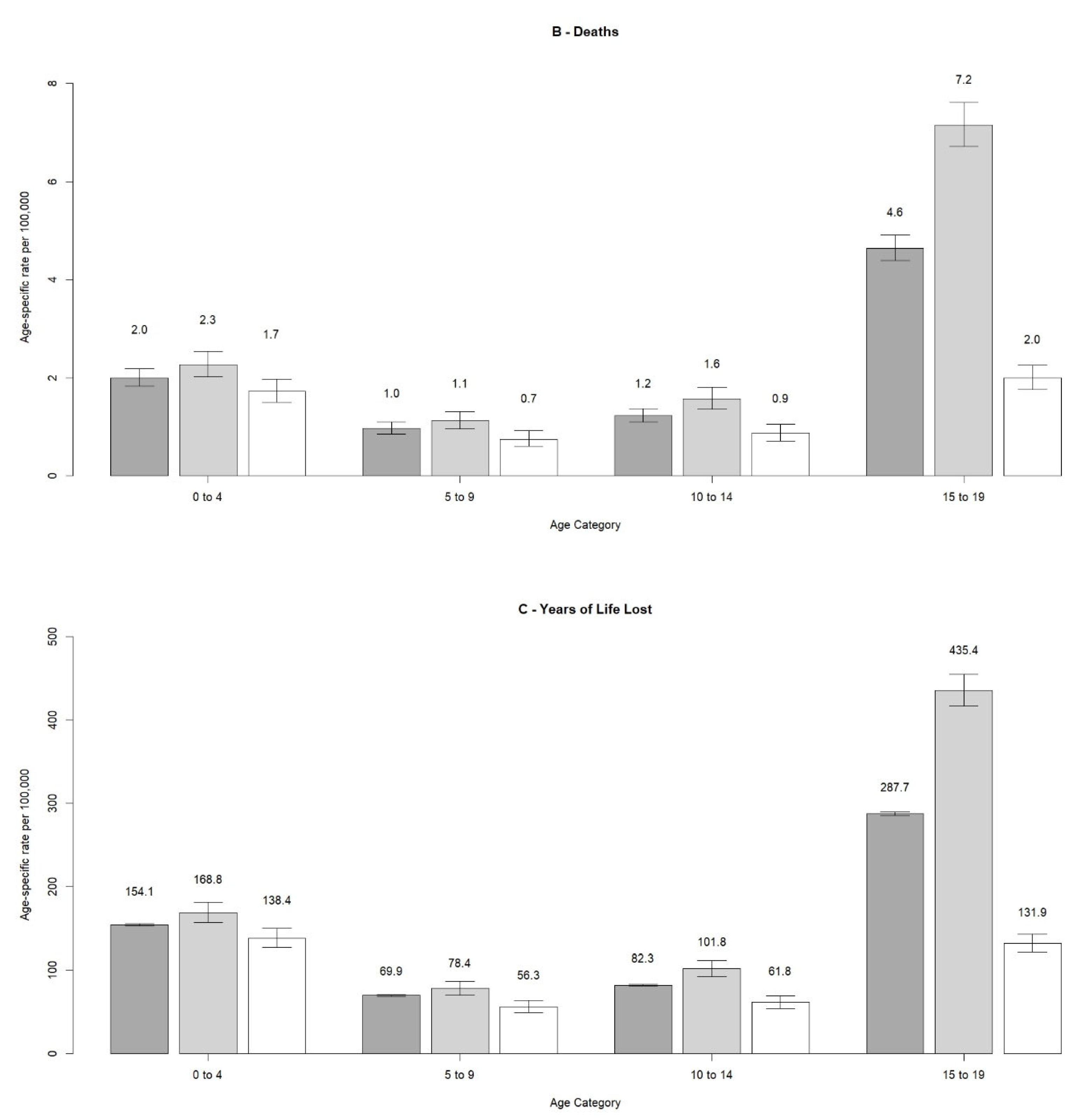
3.2. Deaths Due to TBI
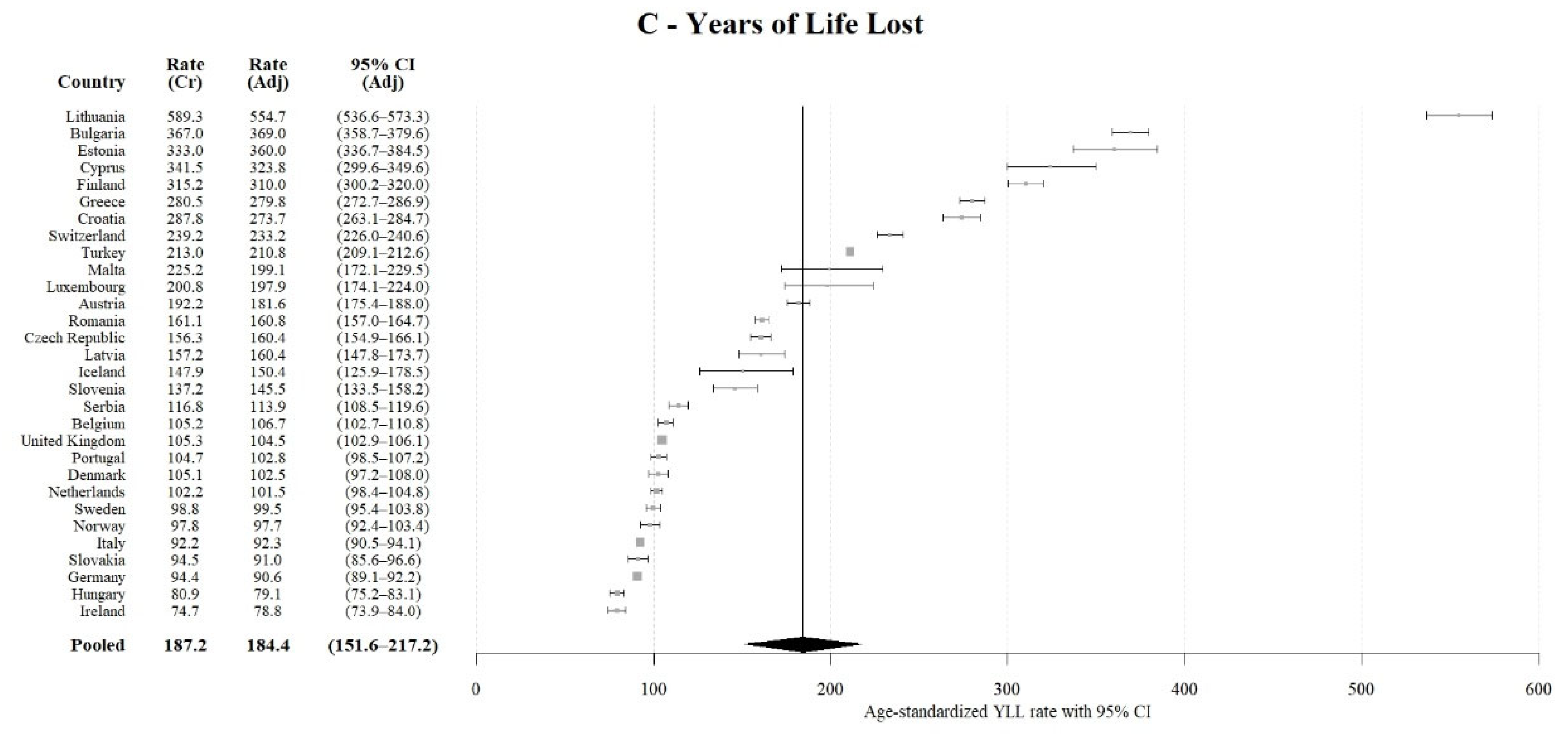
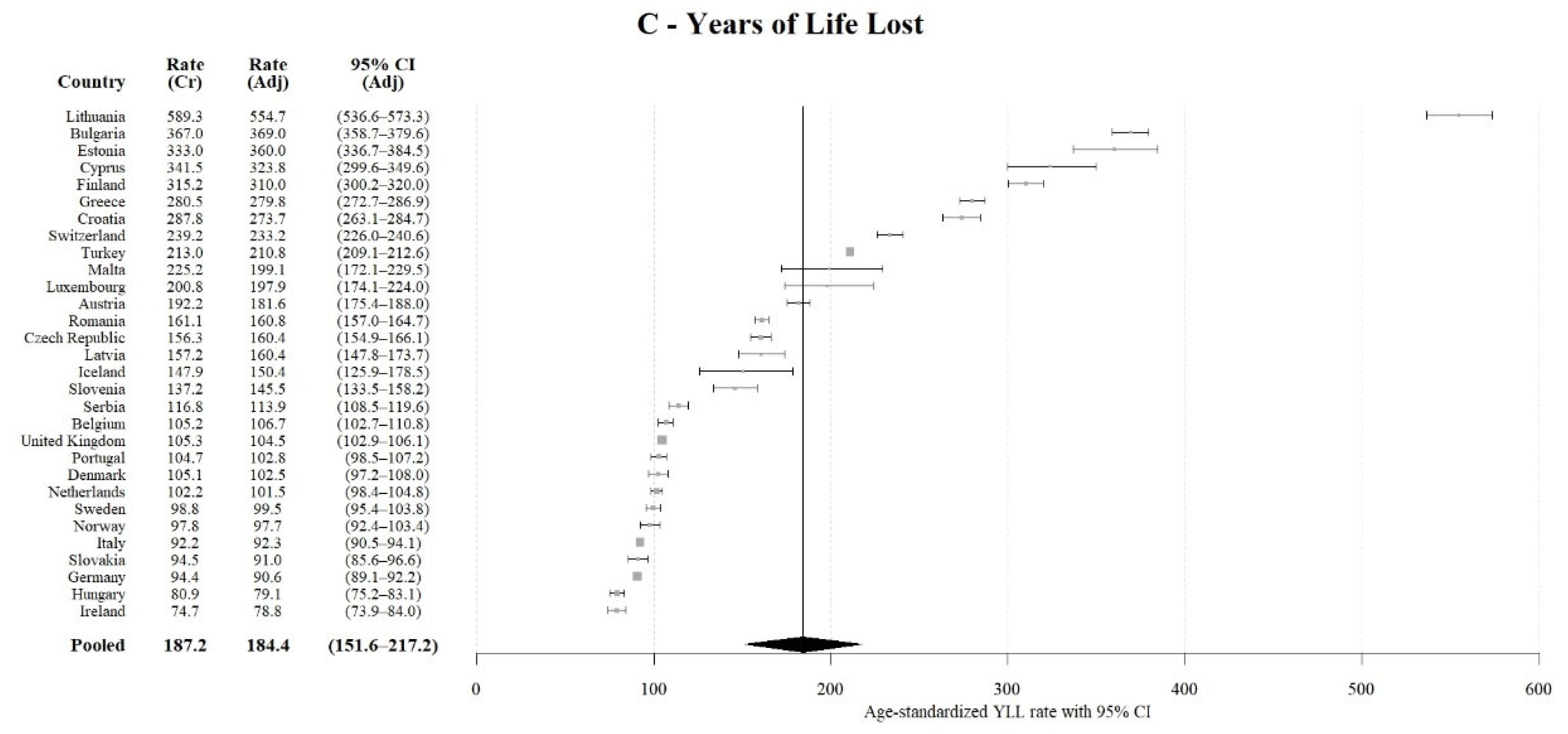
3.3. Years of Life Lost Due to TBI
3.4. Extrapolations
4. Discussion
4.1. Authors’ Main Findings
4.2. Comparison with Literature
4.3. Implications for Research and Practice
4.4. Generalizability, Limitations and Bias
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Maas, A.I.; Stocchetti, N.; Bullock, R. Moderate and severe traumatic brain injury in adults. Lancet Neurol. 2008, 7, 728–741. [Google Scholar] [CrossRef]
- Feigin, V.L.; Theadom, A.; Barker-Collo, S.; Starkey, N.; McPherson, K.; Kahan, M.; Dowell, A.; Brown, P.; Parag, V.; Kydd, R.; et al. Incidence of traumatic brain injury in New Zealand: A population-based study. Lancet Neurol. 2013, 12, 53–64. [Google Scholar] [CrossRef]
- Majdan, M.; Plancikova, D.; Brazinova, A.; Rusnak, M.; Nieboer, D.; Feigin, V.L.; Maas, A. Epidemiology of traumatic brain injuries in Europe: A cross-sectional analysis. Lancet Public Health 2016, 1, e76–e83. [Google Scholar] [CrossRef]
- Majdan, M.; Plancikova, D.; Maas, A.I.; Polinder, S.; Feigin, V.L.; Theadom, A.; Rusnak, M.; Brazinova, A.; Haagsma, J. Years of life lost due to traumatic brain injury in Europe: A cross-sectional analysis of 16 countries. PLoS Med. 2017, 14, e1002331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jager, T.E.; Weiss, H.B.; Coben, J.H.; Pepe, P.E. Traumatic Brain Injuries Evaluated in U.S. Emergency Departments, 1992–1994. Acad. Emerg. Med. 2000, 7, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.A.; Bell, J.M.; Breiding, M.J.; Xu, L. Traumatic brain injury–related emergency department visits, hospitalizations, and deaths—United States, 2007 and 2013. MMWR Surveill Summ. 2017, 66, 1. [Google Scholar] [CrossRef] [PubMed]
- Barker-Collo, S.L.; Wilde, N.J.; Feigin, V.L. Trends in head injury incidence in New Zealand: A hospital-based study from 1997/1998 to 2003/2004. Neuroepidemiology 2009, 32, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Te Ao, B.; Tobias, M.; Ameratunga, S.; McPherson, K.; Theadom, A.; Dowell, A.; Starkey, N.; Jones, K.; Barker-Collo, S.; Brown, P.; et al. Burden of Traumatic Brain Injury in New Zealand: Incidence, Prevalence and Disability-Adjusted Life Years. Neuroepidemiology 2015, 44, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Dewan, M.C.; Mummareddy, N.; Wellons III, J.C.; Bonfield, C.M. Epidemiology of global pediatric traumatic brain injury: Qualitative review. World Neurosurg. 2016, 91, 497–509. [Google Scholar] [CrossRef] [PubMed]
- Thurman, D.J. The epidemiology of traumatic brain injury in children and youths: A review of research since 1990. J. Child Neurol. 2016, 31, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Eurostat. Hospital Discharges and Length of Stay for Inpatient and Curative Care Dataset; Eurostat: Luxembourg, 2019; Available online: https://ec.europa.eu/eurostat/web/health/data/database (accessed on 15 October 2019).
- Eurostat. Your Key to European Statistics; Eurostat: Luxembourg, 2020; Available online: https://ec.europa.eu/eurostat/home (accessed on 20 February 2020).
- European Commission. Commission Regulation (EU) No 328/2011 on Community Statistics on Public Health and Health and Safety at Work, as Regards Statistics on Causes of Death; European Commission: Brussels, Belgium, 2011; Available online: https://eur-lex.europa.eu/legal-content/EN/ALL/?uri=CELEX%3A32011R0328 (accessed on 10 February 2020).
- Eurostat. Population Database; Eurostat: Luxembourg, 2019; Available online: https://ec.europa.eu/eurostat/web/population-demography-migration-projections/data/database (accessed on 10 October 2019).
- Eurostat. Life Expectancy by Age and Sex Dataset; Eurostat: Luxembourg, 2019; Available online: https://appsso.eurostat.ec.europa.eu/nui/show.do?dataset=demo_mlexpec&lang=en (accessed on 10 October 2019).
- Eurostat. Eurostat Hospital Discharge Dataset Metadata; Eurostat: Luxembourg, 2020; Available online: https://ec.europa.eu/eurostat/cache/metadata/Annexes/hlth_act_esms_an4.pdf (accessed on 15 February 2020).
- Eurostat. Eurostat Causes of Deaths Dataset Metadata; Eurostat: Luxembourg, 2020; Available online: https://ec.europa.eu/eurostat/cache/metadata/en/hlth_cdeath_sims.htm (accessed on 15 February 2020).
- World Health Organization. International Shortlist for Hospital Morbidity Tabulation (ISHMT); World Health Organizationn: Geneva, Switzerland, 2020; Available online: https://www.who.int/classifications/icd/implementation/morbidity/ishmt/en/ (accessed on 20 February 2020).
- Eurostat. Revision of the European Standard Population—Report of Eurostat’s Task Force. Eurostat Methodologies and Working Papers Website. 2013. Available online: https://ec.europa.eu/eurostat/documents/3859598/5926869/KS-RA-13-028-EN.PDF/e713fa79-1add-44e8-b23d-5e8fa09b3f8f (accessed on 10 October 2019).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age Group | Hospital Discharges | Deaths | YLLs | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Boys | Girls | Total | Boys | Girls | Total | Boys | Girls | Total | |
| 0 to 4 | 100,142 (56%) | 79,239 (44%) | 179,381 | 294 (58%) | 212 (42%) | 506 | 21,913 (56%) | 17,039 (44%) | 38,952 |
| 5 to 9 | 52,781 (62%) | 32,330 (38%) | 85,111 | 155 (63%) | 93 (37%) | 248 | 10,820 (61%) | 6999 (39%) | 17,819 |
| 10 to 14 | 49,678 (64%) | 27,654 (36%) | 77,332 | 205 (65%) | 108 (35%) | 313 | 13,297 (63%) | 7644 (37%) | 20,941 |
| 15 to 19 | 66,917 (67%) | 32,627 (33%) | 99,544 | 978 (79%) | 258 (21%) | 1236 | 59,512 (78%) | 17,058 (22%) | 76,570 |
| Total | 269,518 (61%) | 171,850 (39%) | 441,368 | 1632 (71%) | 671 (29%) | 2303 | 105,542 (68%) | 48,740 (32%) | 154,282 |
| Variables | Pooled Crude Rate (95% CI) | Estimated Annual Number of Cases (95% CI) |
|---|---|---|
| Hospital discharges due to TBI–overall | 348.5 (253.1–443.9) | 370,951 (269,405–472,497) |
| Hospital discharges–intracranial injuries | 156.3 (123.3–189.3) | 166,369 (131,243–201,495) |
| Hospital discharges–other head injuries | 192.2 (152.9–231.5) | 204,582 (162,750–246,414) |
| Deaths due to TBI | 2.9 (1.9–3.8) | 3087 (2022–4045) |
| YLLs due to TBI | 187.2 (153.1–221.4) | 199,260 (162,963–235,663) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Majdan, M.; Melichova, J.; Plancikova, D.; Sivco, P.; Maas, A.I.R.; Feigin, V.L.; Polinder, S.; Haagsma, J.A. Burden of Traumatic Brain Injuries in Children and Adolescents in Europe: Hospital Discharges, Deaths and Years of Life Lost. Children 2022, 9, 105. https://doi.org/10.3390/children9010105
Majdan M, Melichova J, Plancikova D, Sivco P, Maas AIR, Feigin VL, Polinder S, Haagsma JA. Burden of Traumatic Brain Injuries in Children and Adolescents in Europe: Hospital Discharges, Deaths and Years of Life Lost. Children. 2022; 9(1):105. https://doi.org/10.3390/children9010105
Chicago/Turabian StyleMajdan, Marek, Juliana Melichova, Dominika Plancikova, Patrik Sivco, Andrew I. R. Maas, Valery L. Feigin, Suzanne Polinder, and Juanita A. Haagsma. 2022. "Burden of Traumatic Brain Injuries in Children and Adolescents in Europe: Hospital Discharges, Deaths and Years of Life Lost" Children 9, no. 1: 105. https://doi.org/10.3390/children9010105
APA StyleMajdan, M., Melichova, J., Plancikova, D., Sivco, P., Maas, A. I. R., Feigin, V. L., Polinder, S., & Haagsma, J. A. (2022). Burden of Traumatic Brain Injuries in Children and Adolescents in Europe: Hospital Discharges, Deaths and Years of Life Lost. Children, 9(1), 105. https://doi.org/10.3390/children9010105