
Multi-Validity Process and Factor-Invariance. Perceived Self-Efficacy-Scale for the Prevention of Obesity in Preteens

 , ,
, ,  ,
,
Abstract
1. Introduction
2. Methods
2.1. Design
2.2. Participants
2.3. Instrument
2.4. Procedure
2.5. Statistical Analysis
3. Results
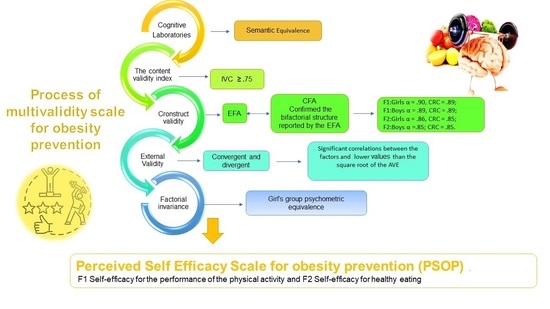
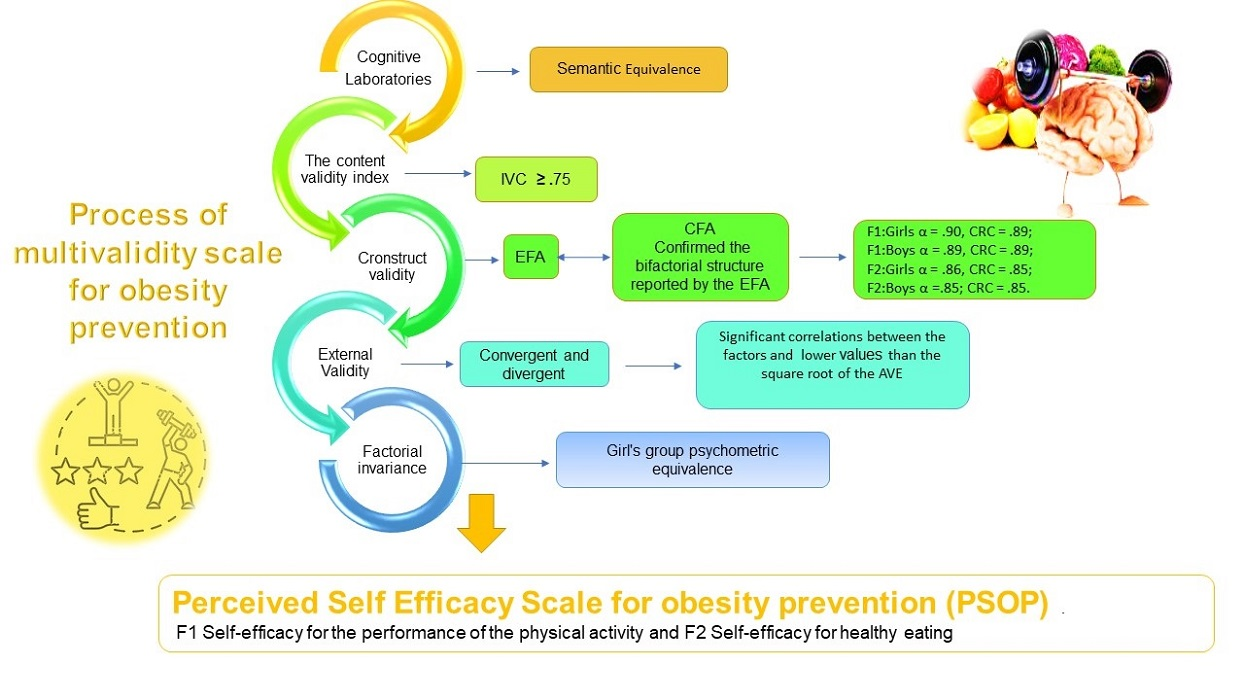
3.1. Exploratory Factor Analysis EFA
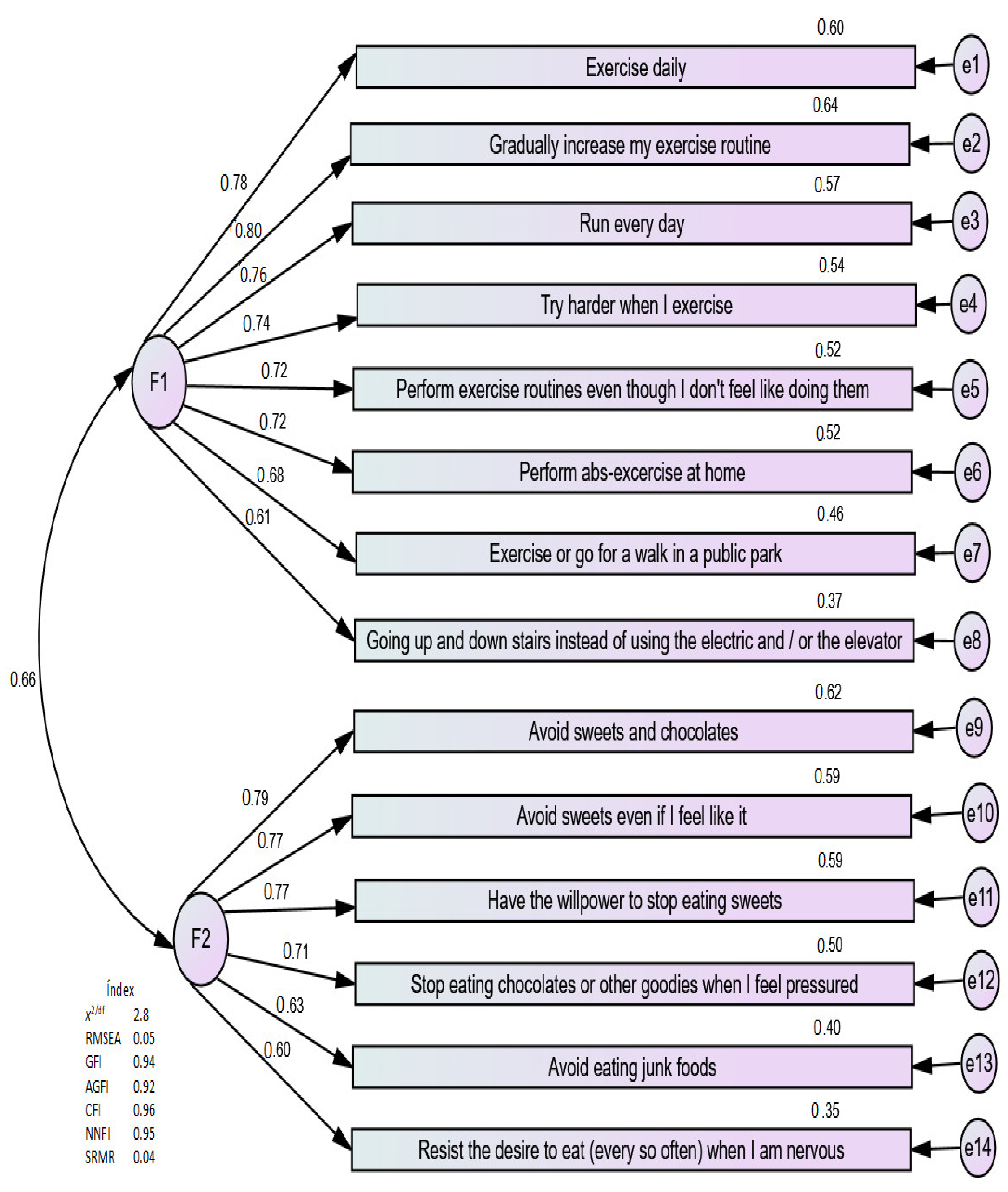
3.2. Confirmatory Factor Analysis (CFA) and the Factorial Model (FM)
3.3. External Validity and Convergent and Discriminant Validities
4. Discussion
4.1. Content and Construct Validity
4.2. External Validity
4.3. Factorial Invariance (FI)
5. Conclusions
Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Residence | EFA | ||
|---|---|---|---|
| Girls | Boys | Total | |
| CMX | 241 | 199 | 440 |
| CsMR | 373 | 387 | 760 |
| CFA | |||
| CMX | 224 | 200 | 424 |
| CsMR | 359 | 388 | 747 |
| Total | 1197 (Mage = 12.68, SD = 0.79) | 1174 (Mage = 12.82, SD = 0.84) | 2371 (Mage = 12.75, SD = 0.81) |


| ITEMS | λ Boys | λ Girls | CRC (Composite Reliability) Boys/Girls | AVE (Average Variance Extracted) | |
|---|---|---|---|---|---|
| SPA | Exercise daily | 0.72 | 0.77 | 0.88 Boys 0.90 Girls | 0.53 Boys 0.52 Girls |
| Run every day | 0.76 | 0.75 | |||
| Try harder when I exercise | 0.75 | 0.73 | |||
| Gradually increase my exercise routine | 0.75 | 0.79 | |||
| Perform exercise routines even though I don’t feel like doing them | 0.73 | 0.72 | |||
| Perform abs exercise at home | 0.67 | 0.72 | |||
| Exercise or go for a walk in a public park | 0.72 | 0.67 | |||
| Going up and down stairs instead of using the electric and/or the elevator | 0.61 | ||||
| SHE | Avoid eating junk foods | 0.57 | 0.62 | 0.86 Boys 0.85 Girls | 0.51 Boys 0.50 Girls |
| Resist the desire to eat (every so often) when I am nervous. | 0.58 | 0.59 | |||
| Stop eating chocolates or other goodies when I feel pressured | 0.67 | 0.70 | |||
| Have the willpower to stop eating sweets | 0.78 | 0.77 | |||
| Avoid sweets even if I feel like them | 0.80 | 0.76 | |||
| Avoid sweets and chocolates | 0.84 | 0.78 |
| Boys | ||
|---|---|---|
| SPA | SHE | |
| F1 SPA | 0.72 | |
| F2 SHE | 0.55 ** | 0.71 |
| Girls | ||
| F1 SPA | 0.72 | |
| F2 SHE | 0.59 ** | 0.70 |
| Model | χ2(df) | χ2/df | CFI | RMSEA | Δχ2 | ΔCFI | ΔRMSEA | |
|---|---|---|---|---|---|---|---|---|
| (IC 90%) | p > 0.05 | ≤0.01 | ≤0.015 | |||||
| M1. Configuration invariance (Base line) | 319.83 (152) p = 0.001 | 2.10 | 0.95 | 0.044 (0.037–0.050) | ||||
| M2. Metric or weak invariance (λ restricted) | 333.88 (164) p = 0.001 | 2.03 | 0.95 | 0.042 (0.036–0.049) | 14.05 (12), p = 0.301 | 0.001 | 0.002 | |
| M3. Scalar or strong invariance (λ and τ restricted) | 348.02 (178) p = 0.001 | 1.95 | 0.95 | 0.041 (0.034–0.047) | 14.14 (14), p = 0.378 | 0.001 | 0.001 | |
| M4. Strict invariance (λ, τ and θ restricted) | 377.75 (195) p = 0.001 | 1.93 | 0.95 | 0.040 (0.034–0.046) | 43.87 (31), p = 0.061 | 0.001 | 0.002 | |
| M5. Structural Invariance (Factor variances and covariances) | 348.19 (181) p = 0.001 | 1.92 | 0.95 | 0.040 (0.034–0.046) | 14.31 (17), p = 0.595 | 0.001 | 0.002 | |
| Model | χ2(df) | χ2/df | CFI | RMSEA | Δχ2 | ΔCFI | ΔRMSEA |
|---|---|---|---|---|---|---|---|
| (IC 90%) | p > 0.05 | ≤0.01 | ≤0.015 | ||||
| M1. Configuration invariance (Base line) | 257.16(128) p = 0.001 | 2 | 0.96 | 0.041(0.034–0.049) | |||
| M2. Metric or weak invariance (λ restricted) | 284.52(139) p = 0.001 | 2.04 | 0.96 | 0.042(0.035–0.049) | 27.35 (11), p = 0.005 | 0.001 | −0.001 |
| M3. Scalar or strong invariance (λ and τ restricted) | 303.17(152) p = 0.001 | 1.99 | 0.95 | 0.041(0.034–0.048) | 18.65(13), p = 0.123 | 0.001 | 0.001 |
| M4. Strict invariance (λ, τ and θ restricted) | 326.92(168) p = 0.001 | 1.94 | 0.95 | 0.040(0.034–0.047) | 42.40 (29), p = 0.056 | 0.001 | 0.001 |
| M5. Structural Invariance (Factor variances and covariances) | 308.71(155) p = 0.001 | 1.99 | 0.95 | 0.041(0.034–0.048) | 24.19 (16), p = 0.090 | 0.001 | 0.001 |
References
- WHO. Obesity and Overweight: Fact Sheet; 2018. Available online: http://www.who.int/mediacentre/factsheets/fs311/en (accessed on 12 January 2021).
- Bhutta, Z.A.; Ahmed, T.; Black, R.E.; Cousens, S.; Dewey, K.; Giugliani, E.; Haider, B.A.; Kirkwood, B.; Morris, S.S.; Sachdev, H.P.; et al. Maternal and Child Undernutrition Study Group. What works? Interventions for maternal and child undernutrition and survival. Lancet 2008, 371, 417–440. [Google Scholar] [CrossRef]
- Rivera-Dommarco, J.A.; Cuevas-Nasu, L.; de Cosío, T.G.; Shamah-Levy, T.; García-Feregrino, R. Desnutrición crónica en México en el último cuarto de siglo: Análisis de cuatro encuestas nacionales. Salud Pública de México 2013, 55 (Suppl. S2), S161–S169. [Google Scholar] [CrossRef][Green Version]
- Rivera, J.A.; Irizarry, L.M.; González-Cossío, T. Overview of the nutritional status of the Mexican population in the last two decades. Salud Pública Mex. 2009, 51 (Suppl. S4), S645–S656. [Google Scholar] [CrossRef]
- Licona, H.G. Nutrición y pobreza. Política pública basada en evidencia. Salud Pública Mex. 2009, 51 (Suppl. S4), S677–S678. [Google Scholar] [CrossRef]
- WHO. Malnutrición; 2020. Available online: https://www.who.int/dietphysicalactivity/childhood/es/ (accessed on 12 January 2021).
- Levy, T.S.; Nasu, L.C.; Pineda, E.B.G.; Acosta, L.M.G.; Rúan, M.D.C.M.; Ávila, M.H. Sobrepeso y obesidad en niños y adolescentes en México, actualización de la Encuesta Nacional de Salud y Nutrición de Medio Camino 2016. Salud Pública Mex. 2018, 60, 244–253. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez, J.P.; Dommarco, J.R.; Shamah-Levy, T.; Hernández, S.V.; Franco, A.; Cuevas-Nasu, L. Encuesta Nacional de Salud y Nutrición 2012; Centro de Investigación en Evaluación y Encuestas: Cuernavaca, Mexico, 2012. [Google Scholar]
- Shamsalinia, A.; Ghadimi, R.; Chafjiri, R.T.; Chafjiri, R.T.; Norouzinejad, F.; Pourhabib, A.; Ghaffari, F. Nutrition self-efficacy assessment: Designing and psychometric evaluation in a community-dwelling elderly population. J. Health Popul. Nutr. 2019, 38. [Google Scholar] [CrossRef]
- Wilson, K.E.; Harden, S.M.; Almeida, F.A.; You, W.; Hill, J.L.; Goessl, C.; Estabrooks, P.A. Brief self-efficacy scales for use in weight-loss trials: Preliminary evidence of validity. Psychol Assess. 2016, 28, 1255–1264. [Google Scholar] [CrossRef]
- González, L.M.; Cortés, M.I.O. Psychosocial and behavioral factors in the regulation of weight: Self-regulation, self-efficacy and locus control. Enferm. Clin. 2018, 28, 154–161. [Google Scholar]
- Román, Y.; Díaz, B.; Cárdenas, M.; Lugli, Z. Construcción y validación del Inventario Autoeficacia Percibida para el Control de Peso. Clinica y Salud 2007, 18, 45–56. [Google Scholar]
- Gómez-Peresmitré, G.; Acevedo, S.P.; Pineda-García, G.; Saldaña, R.G.; Hernández, R.L. Validación de un instrumento de autoeficacia para la prevención de obesidad en niños escolares. Rev. Mex. de Trastor. Aliment 2017, 8, 21–30. [Google Scholar] [CrossRef]
- Rutten, L.J.F.; Hesse, B.W.; St Sauver, J.L.; Wilson, P.; Chawla, N.; Hartigan, D.B.; Moser, R.P.; Taplin, S.; Glasgow, R.; Arora, N.K. Health self-efficacy among populations with multiple chronic conditions: The value of patient-centered communication. Adv. Ther. 2016, 33, 1440–1451. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.H.; Chae, S.J.; Chang, K.H. The relationship among self-efficacy, perfectionism and academic burnout in medical school students. Korean J. Med. Educ. 2016, 28, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Hays, L.M.; Finch, E.A.; Saha, C.; Marrero, D.G.; Ackermann, R.T. Effect of self-efficacy on weight loss: A psychosocial analysis of a community-based adaptation of the diabetes prevention program lifestyle intervention. Diabetes Spectr. 2014, 27, 270–275. [Google Scholar] [CrossRef]
- Henry, H.; Reimer, K.; Smith, C.; Reicks, M. Associations of decisional balance, processes of change and self-efficacy with stages of change for increased fruit and vegetable intake among low-income, African-American mothers. Am. Diet. Assoc. 2006, 106, 841–849. [Google Scholar] [CrossRef]
- Linde, J.A.; Rothman, A.J.; Baldwin, A.S.; Jeffery, R.W. The impact of self-efficacy on behavior change and weight change among overweight participants in a weight loss trial. Health Psychol. 2006, 25, 282–291. [Google Scholar] [CrossRef] [PubMed]
- McCabe, P. Enhancing self-efficacy for high-stakes reading tests. Read. Teach. 2003, 57, 12–20. [Google Scholar]
- Baker, E.K. Caring for Ourselves: A Therapist’s Guide to Personal and Professional Well-Being; American Psychological Association: Washington, DC, USA, 2003. [Google Scholar]
- Reigal, R.; Videra, A.; Gil, J. Physical exercise, general self-efficacy and life satisfaction in adolescence. Rev. Int Med. Cienc. Act. Fís. Deporte 2014, 14, 561–576. [Google Scholar]
- Sánchez, G.F.L.; Víllora, S.G.; Suárez, A.D. Level of habitual physical activity in children and adolescents from the Region of Murcia (Spain). SpringerPlus 2016, 5, 1–6. [Google Scholar] [CrossRef]
- Steele, M.M.; Burns, L.G.; Whitaker, B.N. Reliability and Validity of the SE-HEPA. Health Educ. Behav. 2012, 40, 355–361. [Google Scholar] [CrossRef]
- Bandura, A. Self-Efficacy: The Exercise of Control; Freeman: New York, NY, USA, 1997. [Google Scholar]
- Guzmán, S.; Gómez, G. Análisis discriminante del Inventario de Autoeficacia para Control de Peso en adolescentes mexicanos. Psicol. Salud 2011, 21, 157–164. [Google Scholar]
- Youssefzadeh, M. Cognitive laboratory approach to instrument design. In Proceedings of the Personal Travel: The Long and Short of it, Washington, DC, USA, 28 June–1 July 1999; Transportation Research Board: Washington, DC, USA, 1999; pp. 431–447. [Google Scholar]
- Tristán, L.A. Modificación al modelo de Lawshe para el dictamen cuantitativo de la validez de contenido de un instrumento objetivo. Avances en Medición 2008, 6, 37–48. [Google Scholar]
- Potthat, M.J. Confirmatory factor analysis of ordered categorical variables with large models. Br. J. Math. Stat. Psychol. 1993, 46, 273–286. [Google Scholar] [CrossRef]
- Rodríguez, M.N.; Ruiz, M.A. Atenuación de la asimetría y de la curtosis de las puntuaciones observadas mediante transformaciones de variables: Incidencia sobre la estructura factorial. Psicológica 2008, 29, 205–227. [Google Scholar]
- Kaiser, H.F. An index of factorial simplicity. Psychometrika 1974, 39, 31–36. [Google Scholar] [CrossRef]
- Arbuckle, J.R. AMOS Users Guide, version 21.0; Marketing Department, SPSS Incorporated: Chicago, IL, USA, 2012. [Google Scholar]
- Brown, T.A. Confirmatory Factor Analysis for Applied Research; Guilford Publications: New York, NY, USA, 2015; p. 462. [Google Scholar]
- Kline, R. Principles and Practices of Structural Equation Modeling, 2nd ed.; Guilford Press: New York, NY, USA, 2016. [Google Scholar]
- Nunnally, J.C. Psychometric Theory; McGraw-Hill: New York, NY, USA, 1978. [Google Scholar]
- Dimitrov, D.M. Statistical Methods for Validation of Assessment Scale Data in Counseling and Related Fields, 1st ed.; J. ACA: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Roesch, S.C.; Norman, G.J.; Merz, E.L.; Sallis, J.F.; Patrick, K. Longitudinal measurement invariance of psychosocial measures in physical activity research: An application to adolescent data: Longitudinal measurement invariance. J. Appl Soc. Psychol. 2013, 43, 721–729. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gómez-Peresmitré, G.; Platas Acevedo, R.S.; Pineda-García, G.; Guzmán-Saldaña, R.; León-Hernández, R.C.; Calleja, N. Multi-Validity Process and Factor-Invariance. Perceived Self-Efficacy-Scale for the Prevention of Obesity in Preteens. Children 2021, 8, 504. https://doi.org/10.3390/children8060504
Gómez-Peresmitré G, Platas Acevedo RS, Pineda-García G, Guzmán-Saldaña R, León-Hernández RC, Calleja N. Multi-Validity Process and Factor-Invariance. Perceived Self-Efficacy-Scale for the Prevention of Obesity in Preteens. Children. 2021; 8(6):504. https://doi.org/10.3390/children8060504
Chicago/Turabian StyleGómez-Peresmitré, Gilda, Romana Silvia Platas Acevedo, Gisela Pineda-García, Rebeca Guzmán-Saldaña, Rodrigo Cesar León-Hernández, and Nazira Calleja. 2021. "Multi-Validity Process and Factor-Invariance. Perceived Self-Efficacy-Scale for the Prevention of Obesity in Preteens" Children 8, no. 6: 504. https://doi.org/10.3390/children8060504
APA StyleGómez-Peresmitré, G., Platas Acevedo, R. S., Pineda-García, G., Guzmán-Saldaña, R., León-Hernández, R. C., & Calleja, N. (2021). Multi-Validity Process and Factor-Invariance. Perceived Self-Efficacy-Scale for the Prevention of Obesity in Preteens. Children, 8(6), 504. https://doi.org/10.3390/children8060504