
Efficacy of Intact Cord Resuscitation Compared to Immediate Cord Clamping on Cardiorespiratory Adaptation at Birth in Infants with Isolated Congenital Diaphragmatic Hernia (CHIC)

 , , ,
, , , {kind=link}
{kind=link}
Abstract
1. Introduction
Preliminary Data Obtained
2. Materials and Methods
2.1. Objectives
2.1.1. Primary Endpoints
2.1.2. Secondary Endpoints
- To ensure maternal safety of the procedure, blood loss will be carefully monitored after birth. A graduated collector bag for blood, placed under the woman’s buttocks just after delivery of the child, will be used systematically to measure the blood lost through the vagina in the immediate postpartum period. This bag will be left in place at least for 15 min. The following maternal safety endpoints will be assessed:
- -
- Frequency of postpartum hemorrhage (PPH) defined by blood loss ≥ 500 mL;
- -
- Frequency of severe PPH, defined by measured blood loss ≥ 1000 mL;
- -
- Blood loss volume at 15 min after birth;
- -
- Total postpartum blood loss volume (at bag removal);
- To assess the effect of intact cord resuscitation compared to immediate cord clamping on cardiorespiratory adaptation of infants after birth, the following secondary endpoints will be assessed:
- -
- Frequency of infants with the need for epinephrine administration and/or fluid resuscitation;
- -
- Frequency of infants with the need for chest compressions;
- -
- Pre-ductal SpO2, and heart rate at 1, 5, and 10 min after birth: a pulse oxymeter sensor will be placed at the right hand as soon as possible (within the first minute after birth), which then will be connected to a pulse oxymeter;
- -
- Blood gases and plasma lactate concentration at one hour after birth (H1): these quantitative variables can be considered as objective markers of early cardiorespiratory adaptation at birth.
- -
- Blood gases, pre- and postductal SpO2, lactate, FiO2 set to obtain preductal SpO2 90–94%, ventilatory parameters (peak inspiratory pressure, respiratory rate), heart rate, blood pressure, and urine output at H1, H24, H48, H72, D7, D28;
- -
- Volume of fluid resuscitation during the first 24 h;
- -
- Frequency of infants with the need for vasoactive drugs during the first 24 h;
- -
- Frequency of infants with the need for pulmonary vasodilator during the first 24 h;
- -
- Hemoglobin concentration at H24;
- -
- Echocardiographic parameters (left and right mean blood flow velocities, pulmonary artery pressure) at H6, H24, H48, D7, D28;
- To assess the effect of intact cord resuscitation compared to immediate cord clamping on infants’ mortality and morbidity, we choose to assess the number of free-days from medical support in order to address the effect of mortality on the assessment of morbidity. Because of the randomization process, we can assume that the two groups will be similar in term of severity. In the hypothesis that intact cord resuscitation decreases the mortality, it means that more severe CDH infant may survive, which may in turn increase the apparent morbidity. In case of death, the number of free-days from medical support is zero, which will not modify the number of free-days from medical support in the surviving population. Therefore, the following secondary end-points will be assessed:
- -
- Infant mortality rate at 90-day after birth;
- -
- Infant morbidity outcomes assessed within the first 90 days after birth:
- ○
- mechanical ventilation free-days (defined as days alive and free of mechanical ventilation from birth to 90 days),
- ○
- extracorporeal membranous oxygenation free-days (defined as days alive and free of extracorporeal membranous oxygenation from birth to 90 days)
- ○
- pulmonary vasodilator treatment free-days (defined as days alive and free of pulmonary vasodilator treatment including inhaled NO, sildenafil, prostacyclin analog, bosentan from birth to 90 days),
- ○
- O2 supplementation free-days (defined as days alive and free of O2 supplementation including non-invasive respiratory support from birth to 90 days),
- ○
- parenteral nutrition free-days (defined as days alive and free of parenteral nutrition from birth to 90 days)
- ○
- Total duration of hospitalization,
- To assess parental acceptability and psychological impact of starting resuscitation while the cord is intact as compared to the immediate cord clamping group:
- -
- Number of refusals to participating with the protocol: the reasons for refusal will be recorded (do not want to participate to a research protocol, to not want to be randomized in the immediate cord clamping group, to not want to be randomized in the intact cord resuscitation group);
- -
- Anxiety and depression level assessed by Hospital Anxiety and Depression Scale, HADS. HADS is an auto-questionnaire translated in French, including seven questions to assess anxiety and seven questions to assess depression. HADS questionnaire lasts 3 to 6 min, and is mostly well accepted. Both parents will be requested to answer the questionnaire within the first 3 days after birth, in a calm and neutral room at the maternity ward. Psychologist in charge of the parents will be informed of the results of the test to adapt family support if required;
- -
- Semi-structured interviews will be proposed by a psychologist to the parents whatever the issue, at the end of the study period (90 ± 7 days after birth) to assess their personal experience of the resuscitating period at birth, including both early/delayed cord clamping and close/remote resuscitation maneuvers. The interviews tape recordings will be transcribed and then analyzed using thematic coding. The anonymized data will be independently coded by three researchers and compared for consistency of interpretation. The themes that emerged following the final coding will be used for a qualitative analysis of the parental verbatim;
2.2. Trial Design
2.3. Inclusion Criteria
- Antenatal diagnosis of CDH
- No severe additional malformation or chromosomal diseases
- Full term (>36 weeks gestational age)
- No inclusion in another antenatal trial
- Written informed consents from the parents
- The fetuses which required Fetoscopic Endoluminal Tracheal Occlusion (FETO procedure) will also be included in the study.
2.4. Exclusion Criteria
- Preterm birth before 37 weeks gestational age
- Other severe malformation(s) or chromosomal diseases
- Need for emergency cesarean section (“red code”)
- Twin pregnancy
- Postnatal diagnosis of additional severe malformation(s) or chromosomal diseases
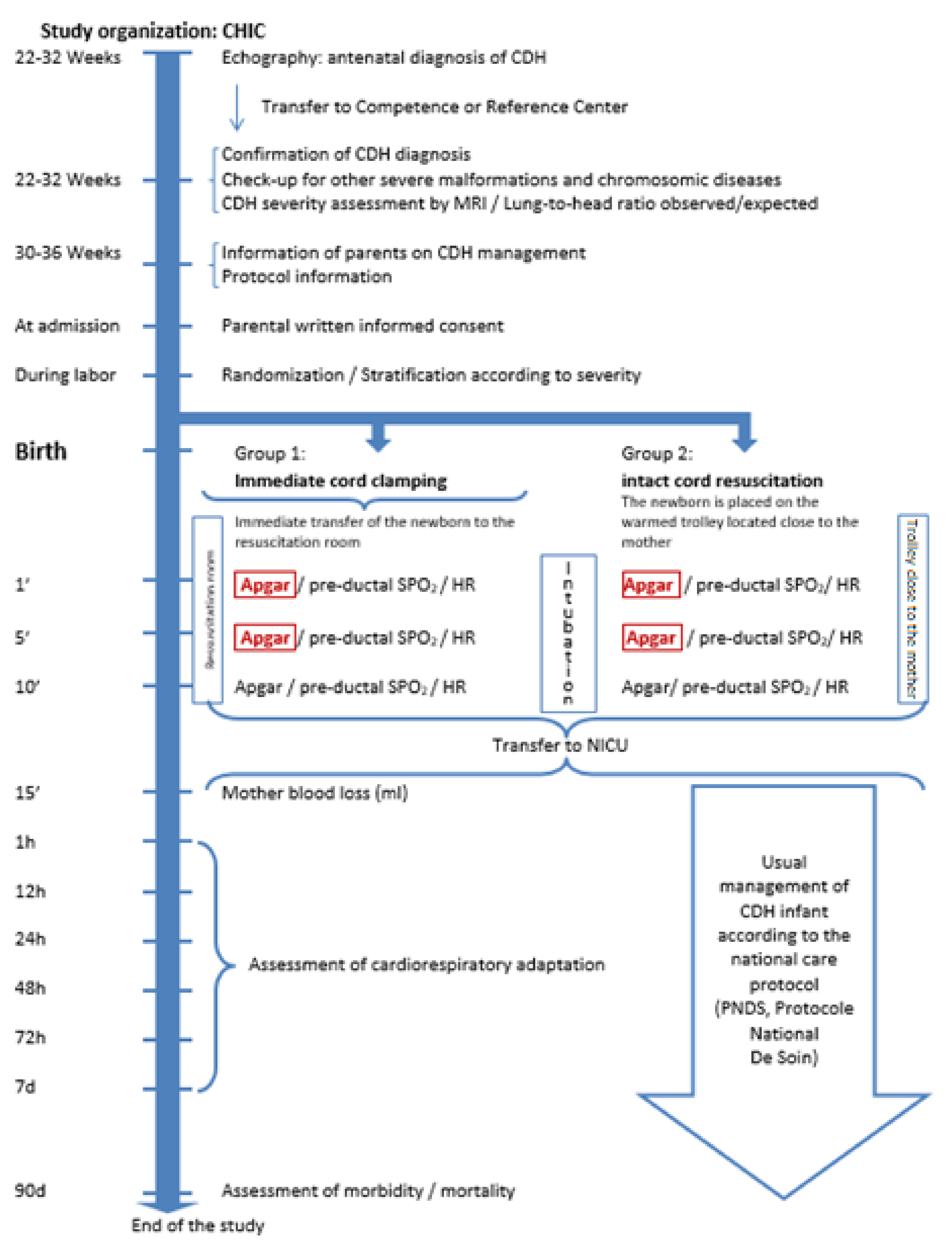
2.5. Study Organization
- The newborn infant should be intubated routinely without bag and mask ventilation, with an endotracheal tube 3.5 mm;
- Ventilation in the delivery room should be done with a peak pressure below 25 cmH2O, and an initial FiO2 = 1;
- The goal of treatment in the delivery room is achieving heart rate > 120 beats/min and increasing preductal SpO2 or achieving acceptable preductal SpO2 targets between 80 and 95%;
- An oro- or nasogastric tube with continuous or intermittent suction should be placed;
- Group 1: Immediate cord clamping with transfer to the resuscitation room
- Group 2: Intact cord resuscitation with resuscitation maneuvers performed on a dedicated trolley placed close to the mother
2.6. Interventions
- Here is a photograph of the trolley (LifeStart, Inspiration Healthcare, Great Britain) (Figure 2):
- In both groups, although APGAR score is routinely assessed in every baby at 1 and 5 mn, special care will be taken to optimize scoring taken into account the fact that most infants with CDH are intubated at 5 min. APGAR score can be assessed during resuscitation maneuvers, including intubation. Slight inter-observer variation may exist in intubated baby mainly due to lack of standardization of scoring respiratory effort states [22]. In order to limit inter-observer variability, we will standardize respiratory effort scoring as previously reported [22]:
- an infant who is apneic and requires intubation and ventilation should receive the minimum value of 0 for respiratory effort;
- an infant who requires artificial ventilation at birth due to irregular or shallow ventilation should score 1;
- To assess whether an artificially ventilated infant is apnoeic or not, ventilation should be stopped briefly, when possible, to check for the presence of spontaneous respiratory movements (apneic, score = 0; irregular or shallow ventilation, score 1; spontaneous effective ventilation, score 2).
- Preductal SpO2 and heart rate are routinely assessed in every baby with CDH. They will be recorded at 1, 5 and 10 min after birth in both groups.
- Blood gases and lactate concentration are routinely assessed in every baby with CDH. These parameters will be recorded at H1, H12, H24, H48, H72, D7, D28, in both groups. Compared with usual care, no additional blood samples are required for the protocol;
- In both groups, although noninvasive echocardiography is routinely assessed in every baby with CDH, left and right mean blood flow velocities, pulmonary artery pressure will be recorded at H6, H24, H48, D7, D28. Compared with usual care, no additional echocardiography is required for the protocol;
- Acceptability by the parents and psychological impact of intact cord resuscitation will be assessed using a questionnaire and a semi-directive interview.
2.7. Criteria for Discontinuation of the Procedure
2.8. Sample Size Calculation
2.9. Statistical Analysis Plan
2.10. Data Safety Monitoring Board
- -
- If the number of Serious Adverse Event (SAE) within the first 24 h after birth is twice higher in the “intact cord resuscitation” group after the inclusion of 30 patients,
- -
- If the DSMB judges that a reported SAE caused by the procedure requires to stop the study,
- -
- If inclusion rate is less than 25% of the total inclusion objectives, 24 months after starting the inclusion in the study. The board will meet after the inclusion of 30, 90 and 150 patients, to address those points, but it could be summoned on other circumstances:
- -
- If a mother’s death occurs within three months after she gave birth to her child,
- -
- At the request of any PI involved in the study.
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Skari, H.; Bjornland, K.; Haugen, G.; Egeland, T.; Emblem, R. Congenital Diaphragmatic Hernia: A Meta-Analysis of Mortality Factors. J. Pediatric Surg. 2000, 35, 1187–1197. [Google Scholar] [CrossRef] [PubMed]
- Congenital Diaphragmatic Hernia Study Group; Morini, F.; Valfrè, L.; Capolupo, I.; Lally, K.P.; Lally, P.A.; Bagolan, P. Congenital Diaphragmatic Hernia: Defect Size Correlates with Developmental Defect. J. Pediatric Surg. 2013, 48, 1177–1182. [Google Scholar] [CrossRef] [PubMed]
- Storme, L.; Aubry, E.; Rakza, T.; Houeijeh, A.; Debarge, V.; Tourneux, P.; Deruelle, P.; Pennaforte, T. Pathophysiology of Persistent Pulmonary Hypertension of the Newborn: Impact of the Perinatal Environment. Arch. Cardiovasc. Dis. 2013, 106, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Bohn, D. Congenital Diaphragmatic Hernia. Am. J. Respir. Crit. Care Med. 2002, 166, 911–915. [Google Scholar] [CrossRef]
- Snoek, K.G.; Reiss, I.K.M.; Greenough, A.; Capolupo, I.; Urlesberger, B.; Wessel, L.; Storme, L.; Deprest, J.; Schaible, T.; van Heijst, A.; et al. Standardized Postnatal Management of Infants with Congenital Diaphragmatic Hernia in Europe: The CDH EURO Consortium Consensus—2015 Update. Neonatology 2016, 110, 66–74. [Google Scholar] [CrossRef]
- Usui, N.; Nagata, K.; Hayakawa, M.; Okuyama, H.; Kanamori, Y.; Takahashi, S.; Inamura, N.; Taguchi, T. Pneumothoraces As a Fatal Complication of Congenital Diaphragmatic Hernia in the Era of Gentle Ventilation. Eur. J. Pediatric Surg. 2013, 24, 031–038. [Google Scholar] [CrossRef]
- Sakurai, Y.; Azarow, K.; Cutz, E.; Messineo, A.; Pearl, R.; Bohn, D. Pulmonary Barotrauma in Congenital Diaphragmatic Hernia: A Clinicopathological Correlation. J. Pediatric Surg. 1999, 34, 1813–1817. [Google Scholar] [CrossRef]
- Crossley, K.J.; Allison, B.J.; Polglase, G.R.; Morley, C.J.; Davis, P.G.; Hooper, S.B. Dynamic Changes in the Direction of Blood Flow through the Ductus Arteriosus at Birth: Blood Flow through the Ductus Arteriosus at Birth. J. Physiol. 2009, 587, 4695–4704. [Google Scholar] [CrossRef]
- Wyckoff, M.H.; Aziz, K.; Escobedo, M.B.; Kapadia, V.S.; Kattwinkel, J.; Perlman, J.M.; Simon, W.M.; Weiner, G.M.; Zaichkin, J.G. Part 13: Neonatal Resuscitation: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2015, 132, S543–S560. [Google Scholar] [CrossRef]
- Rabe, H.; Gyte, G.M.; Díaz-Rossello, J.L.; Duley, L. Effect of Timing of Umbilical Cord Clamping and Other Strategies to Influence Placental Transfusion at Preterm Birth on Maternal and Infant Outcomes. Cochrane Database Syst. Rev. 2019. [Google Scholar] [CrossRef]
- Fogarty, M.; Osborn, D.A.; Askie, L.; Seidler, A.L.; Hunter, K.; Lui, K.; Simes, J.; Tarnow-Mordi, W. Delayed vs Early Umbilical Cord Clamping for Preterm Infants: A Systematic Review and Meta-Analysis. Am. J. Obstet. Gynecol. 2018, 218, 1–18. [Google Scholar] [CrossRef]
- Cass, D.L.; Olutoye, O.O.; Cassady, C.I.; Zamora, I.J.; Ivey, R.T.; Ayres, N.A.; Olutoye, O.A.; Lee, T.C. EXIT-to-Resection for Fetuses with Large Lung Masses and Persistent Mediastinal Compression near Birth. J. Pediatric Surg. 2013, 48, 138–144. [Google Scholar] [CrossRef]
- Houeijeh, A.; Tourneux, P.; Mur, S.; Aubry, E.; Viard, R.; Sharma, D.; Storme, L. Lung Liquid Clearance in Preterm Lambs Assessed by Magnetic Resonance Imaging. Pediatric Res. 2017, 82, 114–121. [Google Scholar] [CrossRef]
- Viard, R.; Tourneux, P.; Storme, L.; Girard, J.-M.; Betrouni, N.; Rousseau, J. Magnetic Resonance Imaging Spatial and Time Study of Lung Water Content in Newborn Lamb: Methods and Preliminary Results. Investig. Radiol. 2008, 43, 470–480. [Google Scholar] [CrossRef]
- Jaillard, S.; Elbaz, F.; Bresson-Just, S.; Riou, Y.; Houfflin-Debarge, V.; Rakza, T.; Larrue, B.; Storme, L. Pulmonary Vasodilator Effects of Norepinephrine during the Development of Chronic Pulmonary Hypertension in Neonatal Lambs. Br. J. Anaesth. 2004, 93, 818–824. [Google Scholar] [CrossRef]
- Lefebvre, C.; Rakza, T.; Weslinck, N.; Vaast, P.; Houfflin-debarge, V.; Mur, S.; Storme, L. Feasibility and Safety of Intact Cord Resuscitation in Newborn Infants with Congenital Diaphragmatic Hernia (CDH). Resuscitation 2017, 120, 20–25. [Google Scholar] [CrossRef]
- Lopriore, E.; van Burk, G.F.; Walther, F.J.; de Beaufort, A.J. Correct Use of the Apgar Score for Resuscitated and Intubated Newborn Babies: Questionnaire Study. BMJ 2004, 329, 143–144. [Google Scholar] [CrossRef]
- Natarajan, G.; Pappas, A.; Shankaran, S. Outcomes in Childhood Following Therapeutic Hypothermia for Neonatal Hypoxic-Ischemic Encephalopathy (HIE). Semin. Perinatol. 2016, 40, 549–555. [Google Scholar] [CrossRef]
- Bent, D.P.; Nelson, J.; Kent, D.M.; Jen, H.C. Population-Based Validation of a Clinical Prediction Model for Congenital Diaphragmatic Hernias. J. Pediatrics 2018, 201, 160–165. [Google Scholar] [CrossRef]
- Jani, J.C.; Benachi, A.; Nicolaides, K.H.; Allegaert, K.; Gratacós, E.; Mazkereth, R.; Matis, J.; Tibboel, D.; Van Heijst, A.; Storme, L.; et al. Prenatal Prediction of Neonatal Morbidity in Survivors with Congenital Diaphragmatic Hernia: A Multicenter Study. Ultrasound Obs. Gynecol. 2009, 33, 64–69. [Google Scholar] [CrossRef]
- Dütemeyer, V.; Cordier, A.-G.; Cannie, M.M.; Bevilacqua, E.; Huynh, V.; Houfflin-Debarge, V.; Verpillat, P.; Olivier, C.; Benachi, A.; Jani, J.C. Prenatal Prediction of Postnatal Survival in Fetuses with Congenital Diaphragmatic Hernia Using MRI: Lung Volume Measurement, Signal Intensity Ratio, and Effect of Experience. J. Matern. Fetal Neonatal Med. 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Pocock, S.J.; Simon, R. Sequential Treatment Assignment with Balancing for Prognostic Factors in the Controlled Clinical Trial. Biometrics 1975, 31, 103–115. [Google Scholar] [CrossRef] [PubMed]
- Storme, L.; Boubnova, J.; Mur, S.; Pognon, L.; Sharma, D.; Aubry, E.; Sfeir, R.; Vaast, P.; Rakza, T.; Benachi, A.; et al. Review Shows That Implementing a Nationwide Protocol for Congenital Diaphragmatic Hernia Was a Key Factor in Reducing Mortality and Morbidity. Acta Paediatr. 2018, 107, 1131–1139. [Google Scholar] [CrossRef] [PubMed]
- Hernie de Coupole Diaphragmatique; Haute Autorité de Santé: Saint-Denis, France, 2020.
- Bhatt, S.; Alison, B.J.; Wallace, E.M.; Crossley, K.J.; Gill, A.W.; Kluckow, M.; Pas, A.B.T.; Morley, C.J.; Polglase, G.R.; Hooper, S.B. Delaying cord clamping until ventilation onset improves cardiovascular function at birth in preterm lambs. J. Physiol. 2013, 591, 2113–2126. [Google Scholar] [CrossRef] [PubMed]
- Hooper, S.B.; Binder-Heschl, C.; Polglase, G.R.; Gill, A.W.; Kluckow, M.; Wallace, E.M.; Blank, D.; Pas, A.B.T. The timing of umbilical cord clamping at birth: physiological considerations. Matern. Health Neonatol. Perinatol. 2016, 2, 4. [Google Scholar] [CrossRef] [PubMed]
- Foglia, E.; Ades, A.; Hedrick, H.L.; Rintoul, N.; Munson, D.A.; Moldenhauer, J.; Gebb, J.; Serletti, B.; Chaudhary, A.; Weinberg, D.D.; et al. Initiating resuscitation before umbilical cord clamping in infants with congenital diaphragmatic hernia: a pilot feasibility trial. Arch. Dis. Child. Fetal Neonatal Ed. 2020, 105, 322–326. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Le Duc, K.; Mur, S.; Rakza, T.; Boukhris, M.R.; Rousset, C.; Vaast, P.; Westlynk, N.; Aubry, E.; Sharma, D.; Storme, L. Efficacy of Intact Cord Resuscitation Compared to Immediate Cord Clamping on Cardiorespiratory Adaptation at Birth in Infants with Isolated Congenital Diaphragmatic Hernia (CHIC). Children 2021, 8, 339. https://doi.org/10.3390/children8050339
Le Duc K, Mur S, Rakza T, Boukhris MR, Rousset C, Vaast P, Westlynk N, Aubry E, Sharma D, Storme L. Efficacy of Intact Cord Resuscitation Compared to Immediate Cord Clamping on Cardiorespiratory Adaptation at Birth in Infants with Isolated Congenital Diaphragmatic Hernia (CHIC). Children. 2021; 8(5):339. https://doi.org/10.3390/children8050339
Chicago/Turabian StyleLe Duc, Kévin, Sébastien Mur, Thameur Rakza, Mohamed Riadh Boukhris, Céline Rousset, Pascal Vaast, Nathalie Westlynk, Estelle Aubry, Dyuti Sharma, and Laurent Storme. 2021. "Efficacy of Intact Cord Resuscitation Compared to Immediate Cord Clamping on Cardiorespiratory Adaptation at Birth in Infants with Isolated Congenital Diaphragmatic Hernia (CHIC)" Children 8, no. 5: 339. https://doi.org/10.3390/children8050339
APA StyleLe Duc, K., Mur, S., Rakza, T., Boukhris, M. R., Rousset, C., Vaast, P., Westlynk, N., Aubry, E., Sharma, D., & Storme, L. (2021). Efficacy of Intact Cord Resuscitation Compared to Immediate Cord Clamping on Cardiorespiratory Adaptation at Birth in Infants with Isolated Congenital Diaphragmatic Hernia (CHIC). Children, 8(5), 339. https://doi.org/10.3390/children8050339