
Validity of Appendicitis Inflammatory Response Score in Distinguishing Perforated from Non-Perforated Appendicitis in Children

 ,
,  ,
,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Study Protocol
2.3. Clinical Diagnosis and Indication for Surgery
2.4. Operative Technique
2.5. Outcome Measures
2.6. Follow-Up
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lounis, Y.; Hugo, J.; Demarche, M.; Seghaye, M.C. Influence of age on clinical presentation, diagnosis delay and outcome in pre-school children with acute appendicitis. BMC Pediatr. 2020, 20, 151. [Google Scholar] [CrossRef]
- Pogorelić, Z.; Jukić, D.; Jukić, M.; Mrklić, I. Factors associated with ovarian preservation in children and adolescents with primary tumors of ovary. Indian Pediatr. 2020, 57, 515–518. [Google Scholar] [CrossRef] [PubMed]
- Pogorelić, Z.; Katić, J.; Gudelj, K.; Mrklić, I.; Vilović, K.; Perko, Z. Unusual cause of acute abdomen in a child-torsion of greater omentum: Report of two cases. Scott. Med. J. 2015, 60, e1–e4. [Google Scholar] [CrossRef]
- Snyder, M.J.; Guthrie, M.; Cagle, S. Acute appendicitis: Efficient diagnosis and management. Am. Fam. Phys. 2018, 98, 25–33. [Google Scholar] [PubMed]
- Pogorelić, Z.; Domjanović, J.; Jukić, M.; Peričić, T.P. Acute appendicitis in children younger than five years of age: Diagnostic challenge for pediatric surgeons. Surg. Infect. (Larchmt.) 2020, 21, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Tamini, N.; Santurro, L.; Chiappetta, M.F.; Gattuso, I.; Barbieri, C.; Fattori, L.; Gianotti, L. Morbidity after negative appendectomy: A single-centre experience on 627 cases. Eur. J. Trauma Emerg. Surg. 2020, 46, 859–864. [Google Scholar] [CrossRef] [PubMed]
- Zouari, M.; Abid, I.; Ben Dhaou, M.; Louati, H.; Jallouli, M.; Mhiri, R. Predictive factors of negative appendectomy in children. Am. J. Emerg. Med. 2018, 36, 335–336. [Google Scholar] [CrossRef] [PubMed]
- Augustin, G.; Čižmešija, Z.; Žedelj, J.; Petrović, I.; Ivković, V.; Antabak, A.; Mijatović, D.; Škegro, M. Laparoscopic appendectomy does not increase the rate of negative appendectomy along with a lower rate of perforated appendicitis—Results in 1899 patients at Zagreb UHC. Acta Clin. Croat. 2018, 57, 503–509. [Google Scholar] [CrossRef]
- Pogorelić, Z.; Rak, S.; Mrklić, I.; Jurić, I. Prospective validation of Alvarado score and Pediatric Appendicitis Score for the diagnosis of acute appendicitis in children. Pediatr. Emerg. Care 2015, 31, 164–168. [Google Scholar] [CrossRef]
- De Castro, S.M.M.; Geerdink, T.H.; Macco, S.; van Veen, R.N.; Jensch, S.; Vrouenraets, B.C. Mandatory imaging in the work-up of children suspected of having appendicitis reduces the rate of unnecessary surgeries. J. Pediatr. Surg. 2018, 53, 2028–2031. [Google Scholar] [CrossRef]
- Alvarado, A. A practical score for the early diagnosis of acute appendicitis. Ann. Emerg. Med. 1986, 15, 557–564. [Google Scholar] [CrossRef]
- Samuel, M. Pediatric appendicitis score. J. Pediatr. Surg. 2002, 37, 872–881. [Google Scholar] [CrossRef] [PubMed]
- Macco, S.; Vrouenraets, B.C.; de Castro, S.M. Evaluation of scoring systems in predicting acute appendicitis in children. Surgery 2016, 160, 1599–1604. [Google Scholar] [CrossRef] [PubMed]
- Ebell, M.H.; Shinholser, J. What are the most clinically useful cutoffs for the Alvarado and Pediatric Appendicitis Scores? A systematic review. Ann. Emerg. Med. 2014, 64, 365–372.e2. [Google Scholar] [CrossRef] [PubMed]
- Andersson, M.; Andersson, R.E. The appendicitis inflammatory response score: A tool for the diagnosis of acute appendicitis that outperforms the Alvarado score. World J. Surg. 2008, 32, 1843–1849. [Google Scholar] [CrossRef]
- De Castro, S.M.; Ünlü, C.; Steller, E.P.; van Wagensveld, B.A.; Vrouenraets, B.C. Evaluation of the Appendicitis Inflammatory Response score for patients with acute appendicitis. World J. Surg. 2012, 36, 1540–1545. [Google Scholar] [CrossRef]
- Scott, A.J.; Mason, S.E.; Arunakirinathan, M.; Reissis, Y.; Kinross, J.M.; Smith, J.J. Risk stratification by the Appendicitis Inflammatory Response score to guide decision-making in patients with suspected appendicitis. Br. J. Surg. 2015, 102, 563–572. [Google Scholar] [CrossRef]
- Pogorelić, Z.; Buljubašić, M.; Šušnjar, T.; Jukić, M.; Poklepović Peričić, T.; Jurić, I. Comparison of open and laparoscopic appendectomy in children: A 5-year single center experience. Indian Pediatr. 2019, 56, 299–303. [Google Scholar] [CrossRef]
- Pogorelić, Z.; Katić, J.; Mrklić, I.; Jerončić, A.; Šušnjar, T.; Jukić, M.; Vilović, K.; Perko, Z. Lateral thermal damage of mesoappendix and appendiceal base during laparoscopic appendectomy in children: Comparison of the harmonic scalpel (Ultracision), bipolar coagulation (LigaSure), and thermal fusion technology (MiSeal). J. Surg. Res. 2017, 212, 101–107. [Google Scholar] [CrossRef]
- Mihanović, J.; Šikić, N.L.; Mrklić, I.; Katušić, Z.; Karlo, R.; Jukić, M.; Jerončić, A.; Pogorelić, Z. Comparison of new versus reused Harmonic scalpel performance in laparoscopic appendectomy in patients with acute appendicitis-a randomized clinical trial. Langenbecks Arch. Surg. 2021, 406, 153–162. [Google Scholar] [CrossRef]
- Pogorelić, Z.; Kostovski, B.; Jerončić, A.; Šušnjar, T.; Mrklić, I.; Jukić, M.; Jurić, I. A Comparison of endoloop ligatures and nonabsorbable polymeric clips for the closure of the appendicular stump during laparoscopic appendectomy in children. J Laparoendosc. Adv. Surg. Tech. A 2017, 27, 645–650. [Google Scholar] [CrossRef] [PubMed]
- Rakić, M.; Jukić, M.; Pogorelić, Z.; Mrklić, I.; Kliček, R.; Družijanić, N.; Perko, Z.; Patrlj, L. Analysis of endoloops and endostaplers for closing the appendiceal stump during laparoscopic appendectomy. Surg. Today 2014, 44, 1716–1722. [Google Scholar] [CrossRef] [PubMed]
- Kollár, D.; McCartan, D.P.; Bourke, M.; Cross, K.S.; Dowdall, J. Predicting acute appendicitis? A comparison of the Alvarado score, the appendicitis inflammatory response score and clinical assessment. World J. Surg. 2015, 39, 104–109. [Google Scholar] [CrossRef]
- Bansal, S.; Banever, G.T.; Karrer, F.M.; Partrick, D.A. Appendicitis in children less than 5 years old: Influence of age on presentation and outcome. Am. J. Surg. 2012, 204, 1031–1035. [Google Scholar] [CrossRef]
- Pogorelić, Z.; Silov, N.; Jukić, M.; Elezović Baloević, S.; Poklepović Peričić, T.; Jerončić, A. Ertapenem monotherapy versus gentamicin plus metronidazole for perforated appendicitis in pediatric patients. Surg. Infect. (Larchmt.) 2019, 20, 625–630. [Google Scholar] [CrossRef]
- Von-Mühlen, B.; Franzon, O.; Beduschi, M.G.; Kruel, N.; Lupselo, D. AIR score assessment for acute appendicitis. Arq. Bras. Cir. Dig. 2015, 28, 171–173. [Google Scholar] [CrossRef]
- Pogorelić, Z.; Lukšić, B.; Ninčević, S.; Lukšić, B.; Polašek, O. Hyponatremia as a predictor of perforated acute appendicitis in pediatric population: A prospective study. J. Pediatr. Surg. 2020. [Google Scholar] [CrossRef]
- Karki, O.B.; Hazra, N.K. Evaluation of the appendicitis inflammatory response score against Alvarado score in diagnosis of acute appendicitis. Kathmandu Univ. Med. J. (KUMJ) 2020, 18, 171–175. [Google Scholar]
- Chisthi, M.M.; Surendran, A.; Narayanan, J.T. RIPASA and air scoring systems are superior to Alvarado scoring in acute appendicitis: Diagnostic accuracy study. Ann. Med. Surg. (Lond.) 2020, 59, 138–142. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Predictive Factor | ||
|---|---|---|
| Vomiting | 1 | |
| Pain in the RIF of abdomen | 1 | |
| Rebound tenderness/abdominal guarding | Light | 1 |
| Medium | 2 | |
| Strong | 3 | |
| Body temperature ≥38.5 °C | 1 | |
| Polymorphonuclear leukocytes | <70% | 0 |
| 70–84% | 1 | |
| ≥85% | 2 | |
| CRP level | <10 mg/L | 0 |
| 10–49 mg/L | 1 | |
| ≥50 mg/L | 2 | |
| WBC count | <10 × 109/L | 0 |
| 10–14.9 × 109/L | 1 | |
| ≥15 × 109/L | 2 |
| Group I | Group II | p | |
|---|---|---|---|
| Perforated Appendicitis (n = 38) | Non-Perforated Appendicitis (n = 146) | ||
| Demographic characteristics of patients | |||
| Age (years) median (IQR) | 10 (8, 12.5) | 11 (9, 14) | 0.098 ‡ |
| Gender n (%) Male Female | 0.355 † | ||
| 27 (71) | 92 (63) | ||
| 11 (29) | 54 (37) | ||
| Weight (kg) mean ± SD | 0.342 * | ||
| 44.2 ± 19.1 | 47.4 ± 17.4 | ||
| Height (cm) mean ± SD | 0.230 * | ||
| 150.1 ± 22.3 | 154.9 ± 19.7 | ||
| BMI (kg/m2) median (IQR) | 18.9 (16.7, 22.3) | 19.1 (16.2, 24.5) | 0.679 ‡ |
| Clinical data of patients | |||
| Duration of symptoms (h) median (IQR) | 50 (36, 84) | 24 (16, 30) | <0.001 ‡ |
| Body temperature (°C) mean ± SD | <0.001 * | ||
| 38.2 ± 0.8 | 37.4 ± 0.6 | ||
| Vomiting n (%) | 28 (73.7) | 83 (56.8) | 0.059 † |
| Pain in RIF n (%) | 38 (100) | 146 (100) | >0.999 † |
| Rebound tenderness n (%) | 38 (100) | 146 (100) | >0.999 † |
| Laboratory data of patients | |||
| WBC count (×109/L) mean ± SD | <0.001 * | ||
| 17.5 ± 5.3 | 14.2 ± 4.1 | ||
| CRP level (mg/L) mean ± SD | <0.001 * | ||
| 111.6 ± 81.3 | 33.6 ± 40.2 | ||
| Polymorphonuclear leukocytes (%) mean ± SD | 0.003 * | ||
| 83.9 ± 6.9 | 80.1 ± 7.0 | ||
| Group I | Group II | p | |
|---|---|---|---|
| Perforated Appendicitis (n = 38) | Non-Perforated Appendicitis (n = 146) | ||
| Surgical approach, n (%) | |||
| Open appendectomy | 14 (36.8) | 24 (16.4) | |
| Laparoscopic appendectomy | 24 (63.2) | 122 (83.6) | 0.006 * |
| Treatment outcomes | |||
| Complications | |||
| Intraoperative, n (%) | 0 | 0 | - |
| Postoperative, n (%) | 1 (2.6) | 2 (1.4) | 0.584 ‡ |
| Reoperations, n (%) | 0 | 0 | - |
| Operative time (min), median (IQR) | 50 (30, 65) | 30 (20, 40) | <0.001 § |
| LOS (days), median (IQR) | 7 (6; 8) | 3 (2; 3) | <0.001 § |
| Pathohistological analysis, n (%) | |||
| Catarrhal appendicitis | 0 | 1 (0.7) | |
| Phlegmonous appendicitis | 0 | 88 (60.3) | |
| Gangrenous appendicitis | 38 (100) | 57 (39) | |
| Predictive Factor, n (%) | Group I | Group II | p * | |
|---|---|---|---|---|
| Perforated Appendicitis (n = 38) | Non-Perforated Appendicitis (n = 146) | |||
| Vomiting | 28 (73.7) | 83 (56.8) | 0.059 | |
| Pain in RIF | 38 (100) | 146 (100) | >0.999 | |
| Axillary temperature ≥38.5 °C | 18 (47.4) | 16 (11) | <0.001 | |
| Polymorphonuclear leukocytes | <70% | 2 (5.3) | 10 (6.8) | <0.001 |
| 70–84% | 10 (26.3) | 92 (63) | ||
| ≥85% | 26 (68.4) | 44 (30.2) | ||
| CRP level | <10 mg/L | 1 (2.6) | 45 (30.8) | <0.001 |
| 10–49 mg/L | 9 (23.7) | 68 (46.6) | ||
| ≥50 mg/L | 28 (73.7) | 33 (22.6) | ||
| WBC count | <10 × 109/L | 2 (5.3) | 23 (15.8) | <0.001 |
| 10–14.9 × 109/L | 12 (31.6) | 71 (48.6) | ||
| ≥15 × 109/L | 24 (63.2) | 52 (35.6) | ||
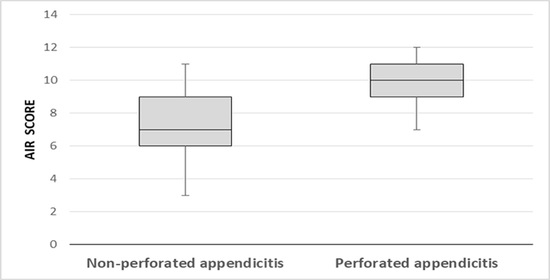
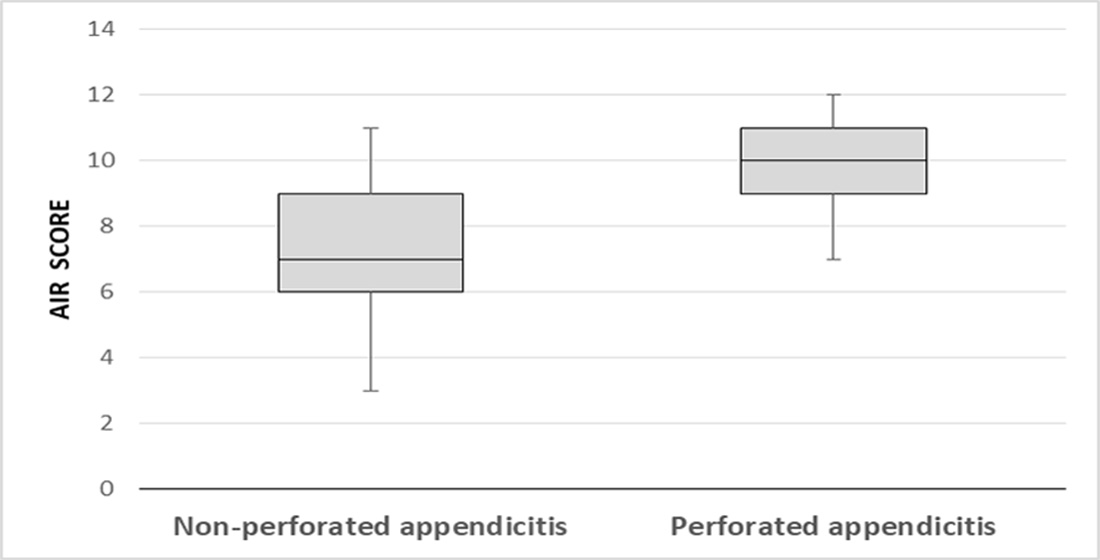
| AIR score median (IQR) | 10 (9, 11) | 7 (6, 9) | <0.001 † | |
| n (%) | High Risk (Score ≥ 9) | Indeterminate Risk (Score 5–8) | Low Risk (Score < 5) |
|---|---|---|---|
| Non-perforated appendicitis | 40 (27.4) | 98 (67.1) | 8 (5.5) |
| Perforated appendicitis | 33 (86.8) | 5 (13.2) | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pogorelić, Z.; Mihanović, J.; Ninčević, S.; Lukšić, B.; Elezović Baloević, S.; Polašek, O. Validity of Appendicitis Inflammatory Response Score in Distinguishing Perforated from Non-Perforated Appendicitis in Children. Children 2021, 8, 309. https://doi.org/10.3390/children8040309
Pogorelić Z, Mihanović J, Ninčević S, Lukšić B, Elezović Baloević S, Polašek O. Validity of Appendicitis Inflammatory Response Score in Distinguishing Perforated from Non-Perforated Appendicitis in Children. Children. 2021; 8(4):309. https://doi.org/10.3390/children8040309
Chicago/Turabian StylePogorelić, Zenon, Jakov Mihanović, Stipe Ninčević, Bruna Lukšić, Sara Elezović Baloević, and Ozren Polašek. 2021. "Validity of Appendicitis Inflammatory Response Score in Distinguishing Perforated from Non-Perforated Appendicitis in Children" Children 8, no. 4: 309. https://doi.org/10.3390/children8040309
APA StylePogorelić, Z., Mihanović, J., Ninčević, S., Lukšić, B., Elezović Baloević, S., & Polašek, O. (2021). Validity of Appendicitis Inflammatory Response Score in Distinguishing Perforated from Non-Perforated Appendicitis in Children. Children, 8(4), 309. https://doi.org/10.3390/children8040309