
Association of Dental Caries and Anthropometric Measures among Primary School Children

 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Statement
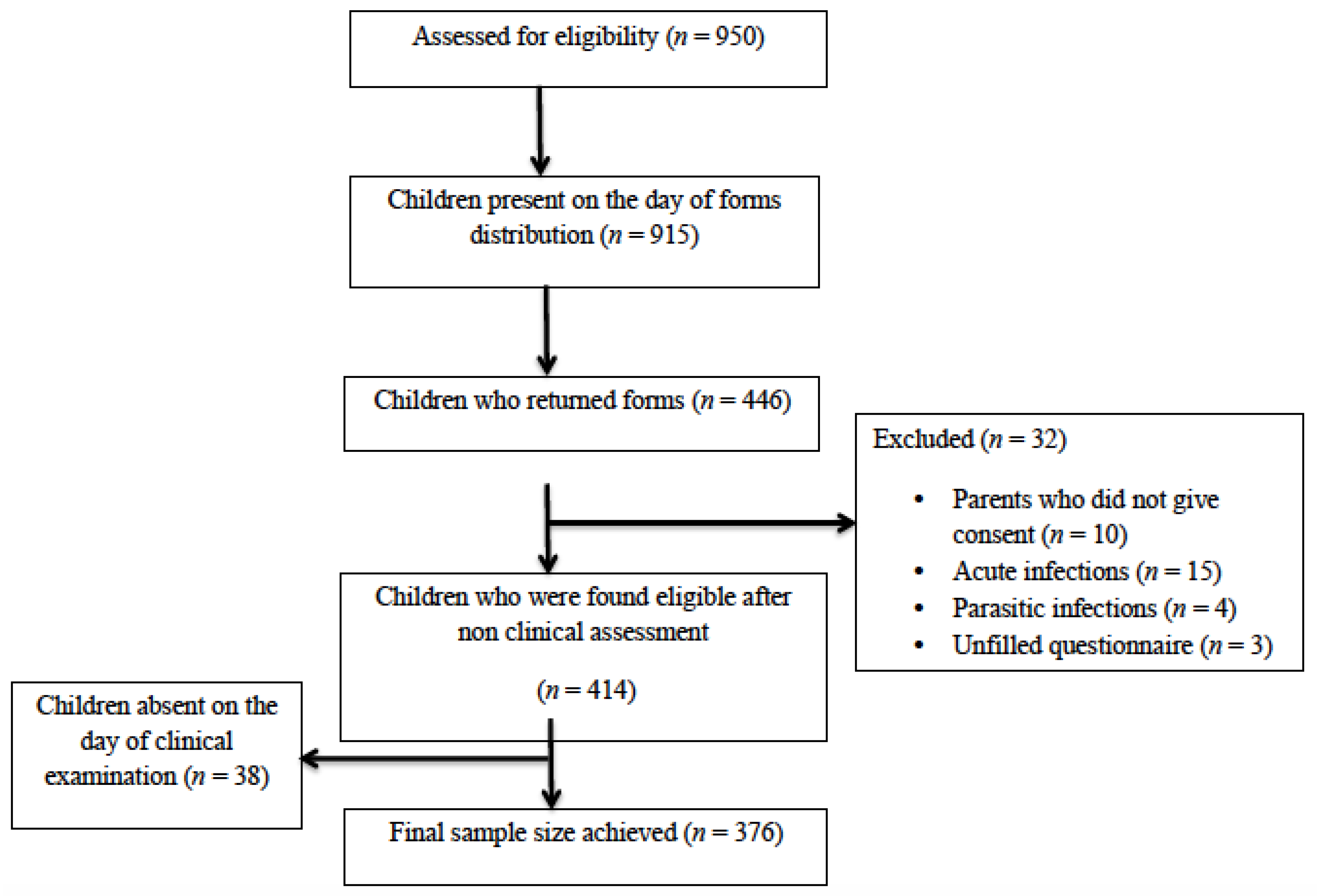
2.2. Study Setting and Participants
2.3. Questionnaire for Parents
2.4. Dental Caries Examination
2.5. Anthropometric Measurements
2.6. Confounders
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rouxel, P.; Chandola, T. Socioeconomic and ethnic inequalities in oral health among children and adolescents living in England, Wales and Northern Ireland. Community Dent. Oral Epidemiol. 2018, 46, 426–434. [Google Scholar] [CrossRef] [PubMed]
- CDC. Prevalence of Total and Untreated Dental Caries Among Youth: United States, 2015–2016. Available online: https://www.cdc.gov/nchs/data/databriefs/db307.pdf (accessed on 1 February 2021).
- Schmidt, A.L.; Strack, M.H.; Conde, S.R. Relationship between food consumption, nutritional status and school performance. J. Hum. Growth Dev. 2018, 28, 240–251. [Google Scholar] [CrossRef]
- Paisi, M.; Kay, E.; Bennett, C.; Kaimi, I.; Witton, R.; Nelder, R.; Lapthorne, D. Body mass index and dental caries in young people: A systematic review. BMC pediatrics. 2019, 19, 1–9. [Google Scholar] [CrossRef]
- Shen, A.; Bernabé, E.; Sabbah, W. Severe dental caries is associated with incidence of thinness and overweight among preschool Chinese children. Acta Odontol. Scand. 2020, 78, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Tosi, F. The Anthropometric Reference Data. Design for Ergonomics; Springer: Berlin/Heidelberg, Germany, 2020; pp. 217–231. [Google Scholar]
- World Health Organization (WHO). Nutrition Landscape Information System (NLIS) Country Profile Indicators: Interpretation Guide; 2019; Available online: https://apps.who.int/iris/handle/10665/44397 (accessed on 1 February 2021).
- Fernández, L.; Rubini, A.; Soriano, J.M.; Aldás-Manzano, J.; Blesa, J. Anthropometric assessment of Nepali children institutionalized in orphanages. Children 2020, 7, 217. [Google Scholar] [CrossRef]
- Li, L.W.; Wong, H.M.; Peng, S.M.; McGrath, C.P. Anthropometric measurements and dental caries in children: A systematic review of longitudinal studies. Adv. Nutr. 2015, 6, 52–63. [Google Scholar] [CrossRef] [PubMed]
- Carson, S.J. No consistent association found between dental caries and body mass index in children. Evid. Based Dent. 2018, 19, 38–39. [Google Scholar] [CrossRef] [PubMed]
- Mishu, M.P.; Tsakos, G.; Heilmann, A.; Watt, R.G. Dental caries and anthropometric measures in a sample of 5- to 9-year-old children in Dhaka, Bangladesh. Community Dent. Oral Epidemiol. 2018, 46, 449–456. [Google Scholar] [CrossRef]
- Oyapero, A.; Adenaike, A.; Edomwonyi, A.; Adeniyi, A.; Olatosi, O. Association between dental caries, odontogenic infections, oral hygiene status and anthropometric measurements of children in Lagos, Nigeria. Braz. J. Oral Sci. 2020, 19, e201431. [Google Scholar] [CrossRef]
- Duijster, D.; Sheiham, A.; Hobdell, M.H.; Itchon, G.; Monse, B. Associations between oral health-related impacts and rate of weight gain after extraction of pulpally involved teeth in underweight preschool Filipino children. BMC Public Health 2013, 13, 1–9. [Google Scholar] [CrossRef]
- Mishu, M.P.; Watt, R.; Tsakos, G.; Heilmann, A. Associations between dental caries and BMI among 5–9 year old Bangladeshi childrenMasuma Pervin Mishu. European J. Public Health 2016, 26 (Suppl. 1). [Google Scholar] [CrossRef]
- Alkarimi, H.A.; Watt, R.G.; Pikhart, H.; Sheiham, A.; Tsakos, G.J.P. Dental caries and growth in school-age children. Pediatrics 2014, 133, e616–e623. [Google Scholar] [CrossRef] [PubMed]
- Petersen; Erik, P.; Baez; Ramon, J.; World Health Organization. Oral Health Surveys: Basic Methods, 5th ed.; World Health Organization, 2013; Available online: https://apps.who.int/iris/handle/10665/97035 (accessed on 1 February 2021).
- Cogill, B. Anthropometric Indicators Measurement Guide. Food and Nutrition Technical Assistance Project; Academy for Educational Development: Washington, DC, USA, 2003. [Google Scholar]
- Freire, M.D.; Corrêa-Faria, P.; Costa, L.R. Effect of dental pain and caries on the quality of life of Brazilian preschool children. Revista de Saude Publica 2018, 52, 30. [Google Scholar] [CrossRef]
- Chala, S.; El Aidouni, M.; Abouqal, R.; Abdallaoui, F. U-shaped association between untreated caries and body mass index in adults at Rabat dental University hospital, Morocco: Cross sectional study. BMC Res. Notes 2017, 10, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Umer, M.F.; Farooq, U.; Shabbir, A.; Zofeen, S.; Mujtaba, H.; Tahir, M. Prevalence and associated factors of dental caries, gingivitis, and calculus deposits in school children of sargodha district, pakistan. J. Ayub Med. Coll. Abbottabad 2016, 28, 152–156. [Google Scholar]
- Hunter, M. Oral Health 2020: Recommendations to Help Ohio Meet Healthy People 2020 Goals Based on States’ Oral Health Plans. Master’s Thesis, Wright State University, Dayton, OH, USA, 2018. Available online: https://corescholar.libraries.wright.edu/mph/214/ (accessed on 1 February 2021).
- De Onis, M.; Garza, C.; Onyango, A.; Rolland-Cachera, M. WHO growth standards for infants and young children. Archives de Pediatrie Organe Officiel Societe Francaise Pediatrie 2009, 16, 47–53. [Google Scholar]
- Dimaisip-Nabuab, J.; Duijster, D.; Benzian, H.; Heinrich-Weltzien, R.; Homsavath, A.; Monse, B.; Sithan, H.; Stauf, N.; Susilawati, S.; Kromeyer-Hauschild, K. Nutritional status, dental caries and tooth eruption in children: A longitudinal study in Cambodia, Indonesia and Lao PDR. BMC Pediatrics 2018, 18, 1–11. [Google Scholar] [CrossRef]
- Davidson, K.; Schroth, R.J.; Levi, J.A.; Yaffe, A.B.; Mittermuller, B.A.; Sellers, E.A. Higher body mass index associated with severe early childhood caries. BMC Pediatrics 2016, 16, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Koksal, E.; Tekçiçek, M.; Yalcın, S.S.; Tuğrul, B.; Yalçın, S.; Pekcan, G. Association between anthropometric measurements and dental caries in Turkish school children. Cent. Eur. J. Public Health. 2011, 19, 147–151. [Google Scholar] [CrossRef]
- Hooley, M.; Skouteris, H.; Millar, L. The relationship between childhood weight, dental caries and eating practices in children aged 4–8 years in Australia, 2004–2008. Pediatric Obes. 2012, 7, 461–470. [Google Scholar] [CrossRef]
- Shim, S.H.; Han, D.H.; Khang, Y.H. Association between dental caries and delayed growth in Korean children. Caries Res. 2018, 52, 71–77. [Google Scholar] [CrossRef]
- Oliveira, L.B.; Sheiham, A.; Bönecker, M. Exploring the association of dental caries with social factors and nutritional status in Brazilian preschool children. Eur. J. Oral Sci. 2008, 116, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Hayden, C.; Bowler, J.O.; Chambers, S.; Freeman, R.; Humphris, G.; Richards, D.; Cecil, J.E. Obesity and dental caries in children: A systematic review and meta-analysis. Community Dent. Oral Epidemiol. 2013, 41, 289–308. [Google Scholar] [CrossRef] [PubMed]
- Alkarimi, H.A.; Watt, R.G.; Pikhart, H.; Jawadi, A.H.; Sheiham, A.; Tsakos, G. Impact of treating dental caries on schoolchildren’s anthropometric, dental, satisfaction and appetite outcomes: A randomized controlled trial. BMC Public Health 2012, 12, 706. [Google Scholar] [CrossRef] [PubMed]
- Neves, É.T.; Firmino, R.T.; de França Perazzo, M.; Gomes, M.C.; Martins, C.C.; Paiva, S.M.; Granville-Garcia, A.F. Absenteeism among preschool children due to oral problems. J. Public Health 2016, 24, 65–72. [Google Scholar] [CrossRef]
- Bhutta, Z.A.; Soofi, S.B.; Zaidi, S.S.H.; Habib, A. Pakistan National Nutrition Survey; 2011; Available online: https://ecommons.aku.edu/pakistan_fhs_mc_women_childhealth_paediatr/262 (accessed on 9 January 2021).


{kind=link}
| Variables | n | % | |
|---|---|---|---|
| Gender | |||
| Male | 187 | 49.7% | |
| Female | 189 | 50.3% | |
| Father’s occupation | |||
| Government officer | 66 | 17.6% | |
| Private Job | 250 | 66.5% | |
| Retired | 11 | 2.9% | |
| Unemployed | 7 | 1.9% | |
| Others | 42 | 11.2% | |
| Mother’s occupation | |||
| Working | 63 | 16.8% | |
| House wife | 313 | 83.2% | |
| Father’s education | |||
| No formal primary schooling | 6 | 1.6% | |
| Primary schooling | 16 | 4.3% | |
| Secondary schooling | 45 | 12.0% | |
| Higher school level | 51 | 13.6% | |
| University degree | 189 | 50.3% | |
| Above bachelor degree | 69 | 18.4% | |
| Mother’s education | |||
| No formal primary schooling | 16 | 4.3% | |
| Primary schooling | 21 | 5.6% | |
| Secondary schooling | 55 | 14.6% | |
| Higher school level | 90 | 23.9% | |
| University degree | 161 | 42.8% | |
| Above bachelor degree | 33 | 8.8% | |
| Mean ± SD | Median | Min-Max | ||
|---|---|---|---|---|
| Primary teeth | ||||
| decayed teeth (dt) | 1.89 ± 1.92 | 1.0 | 0–9 | |
| Missing teeth (mt) | 0.01 ± 0.11 | 0.0 | 0–1 | |
| Filled teeth (ft) | 0.03 ± 0.18 | 0.0 | 0–1 | |
| Total dmft score | 1.93 ± 1.97 | 1.0 | 0–9 | |
| Permanent teeth | ||||
| Decayed teeth (DT) | 0.09 ± 0.32 | 0.0 | 0–3 | |
| Missing teeth (MT) | 0.0 ± 0.0 | 0.0 | 0 | |
| Filled teeth (FT) | 0.0 ± 0.0 | 0.0 | 0 | |
| Total DMFT score | 0.09 ± 0.32 | 0.0 | 0–3 | |
| HAZ | WAZ | BAZ | |||||
|---|---|---|---|---|---|---|---|
| Dental Caries | Z-Score (WHO) | Z-Score (WHO) | Z-Score (WHO) | ||||
| n (%) | Mean ± SD | p-Value * | Mean ± SD | p-Value * | Mean ± SD | p-Value * | |
| Tertile classification | |||||||
| dmft = 0–1 caries | 194 (51.6%) | 0.37 ± 1.05 | <0.001 | 0.34 ± 1.16 | <0.001 | 0.18 ± 1.12 | <0.001 |
| dmft = 2–3 caries | 99 (26.3%) | −0.49 ± 0.76 | −0.79 ± 0.83 | −0.79 ± 0.97 | |||
| dmft = ≥4 caries | 83 (22.1%) | −1.05 ± 0.83 | −1.76 ± 0.85 | −1.61 ± 0.92 | |||
| Caries free and tertile classification | |||||||
| dmft = 0 (no caries) | 122 (32.4%) | 0.62 ± 1.05 | <0.001 | 0.64 ± 1.17 | <0.001 | 0.38± 1.15 | <0.001 |
| dmft = 1–2 caries | 126 (33.5%) | −0.10 ± 0.81 | −0.31 ± 0.88 | −0.38 ± 1.00 | |||
| dmft = 3 caries | 45 (12.0%) | −0.85 ± 0.72 | −1.11 ± 0.84 | −0.92 ± 0.98 | |||
| dmft = ≥4 caries | 83 (22.1%) | −1.05 ± 0.83 | −1.7 ± 0.85 | −1.6 ± 0.92 | |||
| HAZ | WAZ | BAZ | ||
|---|---|---|---|---|
| dmft | r | −0.649 | −0.766 | −0.641 |
| p-value | <0.001 | <0.001 | <0.001 | |
| DMFT | r | −0.081 | −0.085 | −0.06 |
| p-value | 0.111 | 0.099 | 0.244 | |
| Univariate Analysis (p-Value) | Multivariate Analysis (p-Value) | |||||
|---|---|---|---|---|---|---|
| Variables | WAZ | HAZ | BAZ | WAZ | HAZ | BAZ |
| Dental caries | ||||||
| Caries free group dmft =0 (ref) | ||||||
| dmft = 1–2 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| dmft = 3 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| dmft >= 4 | <0.001 | <0.001 | <0.001 | <0.001 | <0.00 | <0.001 |
| Age | 0.983 | 0.091 * | 0.266 | ----- | 0.149 | ----- |
| Gender of child | 0.331 | 0.247 * | 0.499 | ----- | 0.326 | ------ |
| Father’s occupation | 0.412 | 0.980 | 0.237 * | ----- | 0.047 * | 0.505 |
| Mother’s occupation | 0.447 | 0.223 * | 0.547 | ----- | 0.134 | ----- |
| Father’s education | 0.007 * | 0.004 * | 0.039 * | 0.016 * | <0.001 * | 0.293 |
| Mother’s education | 0.881 | 0.688 | 0.793 | ------ | ---- | ---- |
| Income | 0.90 | 0.68 | 0.272 | ----- | ---- | ---- |
| Family members | 0.131 * | 0.531 | 0.023 * | 0.807 | ---- | 0.423 |
| Gestational weeks at birth | 0.519 | 0.568 | 0.380 | ----- | ----- | ----- |
| Birth weight | 0.125 * | 0.115 * | 0.161 * | 0.090 * | 0.763 | 0.357 |
| Past major hospitalization | 0.693 | 0.284 | 0.786 | 0.146 | 0.253 | 0.536 |
| Chronic illness | 0.857 | 0.886 | 0.930 | ---- | ---- | ---- |
| Infection in past 6 months | 0.969 | 0.857 | 0.572 | ---- | ---- | ---- |
| Previous advice by the doctor for a blood test | 0.050 * | 0.137 * | 0.153 * | 0.146 | 0.253 | 0.536 |
| Clinical examination of anemia | <0.001 * | 0.002 * | 0.002 * | 0.009 * | 0.010 * | 0.100 |
| History of medication | 0.221 * | 0.094 * | 0.187 * | 0.104 | 0.011 * | 0.273 |
| History of dental pain | 0.488 | 0.275 | 0.329 | ---- | ----- | ----- |
| Food supplements intake | 0.020 * | 0.137 * | 0.203 * | 0.469 | 0.704 | 0.829 |
| Average hours of sleep | 0.818 | 0.268 | 0.880 | ---- | ---- | ---- |
| Recent changes in child’s appetite | 0.614 | 0.892 | 0.295 | ---- | ---- | ---- |
| Difficulty in eating/sleeping/speaking learning | 0.007 * | 0.072 * | 0.002 * | 0.469 | 0.704 | 0.829 |
| Absent from school due to toothache | 0.068 * | 0.957 | 0.577 | 0.071 | --- | --- |
| Sweets and snack consumption | 0.009 * | 0.021 * | 0.018 * | 0.018 * | 0.383 | 0.051 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anzar, W.; Qureshi, A.; Afaq, A.; Kattan, H.F.; Almutairi, B.; Alzahrani, K.M.; Naseem, M.; Vohra, F.; Abduljabbar, T. Association of Dental Caries and Anthropometric Measures among Primary School Children. Children 2021, 8, 223. https://doi.org/10.3390/children8030223
Anzar W, Qureshi A, Afaq A, Kattan HF, Almutairi B, Alzahrani KM, Naseem M, Vohra F, Abduljabbar T. Association of Dental Caries and Anthropometric Measures among Primary School Children. Children. 2021; 8(3):223. https://doi.org/10.3390/children8030223
Chicago/Turabian StyleAnzar, Wajiha, Ambrina Qureshi, Ashar Afaq, Hiba F. Kattan, Basil Almutairi, Khaled M. Alzahrani, Mustafa Naseem, Fahim Vohra, and Tariq Abduljabbar. 2021. "Association of Dental Caries and Anthropometric Measures among Primary School Children" Children 8, no. 3: 223. https://doi.org/10.3390/children8030223
APA StyleAnzar, W., Qureshi, A., Afaq, A., Kattan, H. F., Almutairi, B., Alzahrani, K. M., Naseem, M., Vohra, F., & Abduljabbar, T. (2021). Association of Dental Caries and Anthropometric Measures among Primary School Children. Children, 8(3), 223. https://doi.org/10.3390/children8030223