
Pharmacometric Evaluation of Umbilical Cord Blood Concentration-Based Early Initiation of Treatment in Methadone-Exposed Preterm Neonates

 ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Assessment of Variability in Dosing Regimens
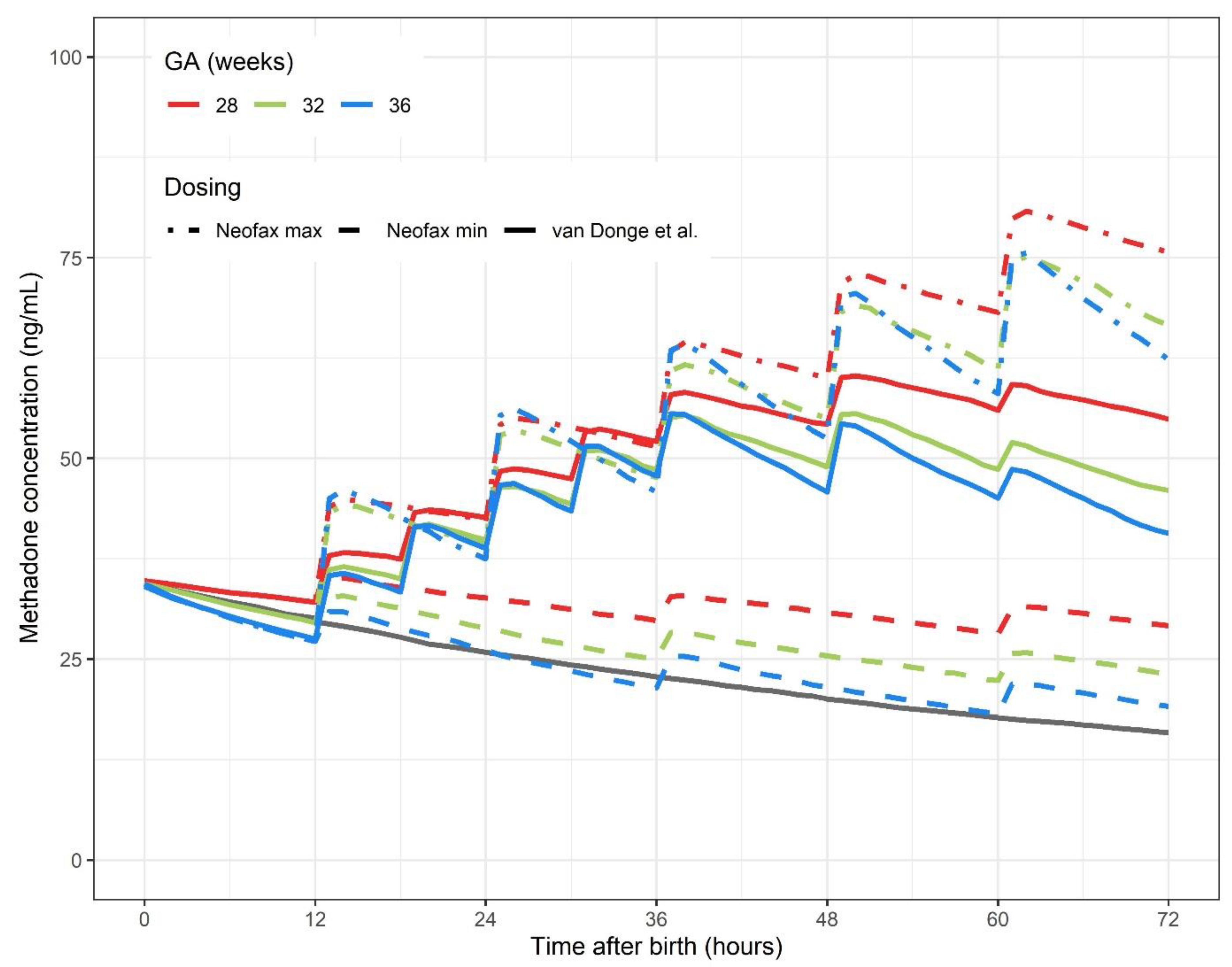
2.2. Simulation of Methadone Exposure in Three Selected Dosing Regimens
3. Results
3.1. Variability in Neonatal Methadone Dosing Guidelines
3.2. Methadone Exposure
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rudd, R.A.; Seth, P.; David, F.; Scholl, L. Increases in Drug and Opioid-Involved Overdose Deaths—United States, 2010–2015. Mmwr. Morb. Mortal. Wkly. Rep. 2016, 65, 1445–1452. [Google Scholar] [CrossRef]
- Haight, S.C.; Ko, J.Y.; Tong, V.T.; Bohm, M.K.; Callaghan, W.M. Opioid Use Disorder Documented at Delivery Hospitalization—United States, 1999–2014. Mmwr. Morb. Mortal. Wkly. Rep. 2018, 67, 845–849. [Google Scholar] [CrossRef]
- Tobon, A.L.; Habecker, E.; Forray, A. Opioid Use in Pregnancy. Curr. Psychiatry Rep. 2019, 21, 118. [Google Scholar] [CrossRef] [PubMed]
- Salsitz, E.; Wiegand, T.J. Pharmacotherapy of Opioid Addiction: “Putting a Real Face on a False Demon.”. J. Med. Toxicol. 2016, 12, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Jones, H.E.; Kaltenbach, K.; Heil, S.H.; Stine, S.M.; Coyle, M.G.; Arria, A.M.; O’Grady, K.E.; Selby, P.; Martin, P.R.; Fischer, G. Neonatal Abstinence Syndrome after Methadone or Buprenorphine Exposure. N. Engl. J. Med. 2010, 363, 2320–2331. [Google Scholar] [CrossRef]
- Stockman, J. Neonatal Abstinence Syndrome after Methadone or Buprenorphine Exposure. Yearb. Pediatr. 2012, 2012, 415–416. [Google Scholar] [CrossRef]
- Bhavsar, R.; Kushnir, A.; Kemble, N. Incidence and Severity of Neonatal Abstinence Syndrome in Infants with Prenatal Exposure to Methadone versus Buprenorphine. Available online: https://doi.org/10.1542/peds.142.1_MeetingAbstract.145 (accessed on 12 January 2021).
- Ko, J.Y.; Wolicki, S.; Barfield, W.D.; Patrick, S.W.; Broussard, C.S.; Yonkers, K.A.; Iskander, J. CDC Grand Rounds: Public Health Strategies to Prevent Neonatal Abstinence Syndrome. Mmwr Morb. Mortal. Wkly. Rep. 2017, 66, 242–245. [Google Scholar] [CrossRef]
- Kocherlakota, P. Neonatal Abstinence Syndrome. Pediatrics 2014, 134, e547–e561. [Google Scholar] [CrossRef] [PubMed]
- Van Donge, T.; Samiee-Zafarghandy, S.; Pfister, M.; Koch, G.; Kalani, M.; Bordbar, A.; Anker, J.V.D. Methadone dosing strategies in preterm neonates can be simplified. Br. J. Clin. Pharm. 2019, 85, 1348–1356. [Google Scholar] [CrossRef]
- Balevic, S.J.; Cohen-Wolkowiez, M. Innovative Study Designs Optimizing Clinical Pharmacology Research in Infants and Children. J. Clin. Pharm. 2018, 58, S58–S72. [Google Scholar] [CrossRef]
- Finnegan, L.P.; Connaughton, J.F.; E Kron, R.; Emich, J.P. Neonatal abstinence syndrome: Assessment and management. Addict. Dis. 1975, 2, 141–158. [Google Scholar] [PubMed]
- Ruwanpathirana, R.; Abdel-Latif, M.E.; Burns, L.; Chen, J.; Craig, F.; Lui, K.; Oei, J.L. Prematurity reduces the severity and need for treatment of neonatal abstinence syndrome. Acta Paediatr. 2015, 104, e188–e194. [Google Scholar] [CrossRef]
- Schiff, D.M.; Grossman, M.R. Beyond the Finnegan scoring system: Novel assessment and diagnostic techniques for the opioid-exposed infant. Semin. Fetal Neonatal Med. 2019, 24, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Rosen, T.S.; Pippenger, C.E. Pharmacologic observations on the neonatal withdrawal syndrome. J. Pediatr. 1976, 88, 1044–1048. [Google Scholar] [CrossRef]
- Kuschel, C.A.; Austerberry, L.; Cornwell, M.; Couch, R.; Rowley, R.S. HCan methadone concentrations predict the severity of withdrawal in infants at risk of neonatal abstinence syndrome? Arch. Dis. Child. Fetal Neonatal Ed. 2004, 89, F390–F393. [Google Scholar] [CrossRef] [PubMed]
- De Castro, A.; Jones, H.E.; Johnson, R.E.; Gray, T.R.; Shakleya, D.M.; Huestis, M.A. Methadone, Cocaine, Opiates, and Metabolite Disposition in Umbilical Cord and Correlations to Maternal Methadone Dose and Neonatal Outcomes. Drug Monit. 2011, 33, 443–452. [Google Scholar] [CrossRef]
- Wiles, J.R.; Isemann, B.; Mizuno, T.; Tabangin, M.E.; Ward, L.P.; Akinbi, H.; Vinks, A.A. Pharmacokinetics of Oral Methadone in the Treatment of Neonatal Abstinence Syndrome: A Pilot Study. J. Pediatr. 2015, 167, 1214–1220.e3. [Google Scholar] [CrossRef] [PubMed]
- Committee, P.F. BNF for Children 2011–2012; BMJ Publishing Group: London, UK; RPS Pub.: London, UK; RCPCH Pub.: London, UK, 2011. [Google Scholar]
- Kliegman, R.; Nelson, W. Nelson Textbook of Pediatrics; Elsevier Saunders: Philadelphia, PA, USA, 2016. [Google Scholar]
- Shann, F. Drug Doses, 17th ed.; Collective Pty, Limited: Parkville, Australia, 2017. [Google Scholar]
- Young, T.; Mangum, B.N. A Manual of Drugs used in neonatal care. Antimicrob. Ed. 23rd Thomson Reuters Montvale 2010, 7645, 42–43. [Google Scholar]
- Neonatal Formulary, 6th ed.; John Wiley & Sons: West Sussex, UK, 2011; pp. 344–345.
- Johnston, A.; Metayer, J.; Robinson, E. Management of Neonatal Opioid Withdrawal. Section 4 of Treatment of Opioid Dependence in Pregnancy: Vermont Guidelines. Vermont Children’s Hospital at Fletcher Allen Health Care. 2010. Available online: http://contentmanager.med.uvm.edu/docs/default-source/vchip-documents/vchip_5neonatal_guidelines.pdf?sfvrsn=2 (accessed on 3 January 2021).
- Consortium OCsHNR. Enteral Morphine or Methadone for Neonatal Abstinence Syndrome (NAS) from Maternal Exposure; Ohio Children’s Hospitals Neonatal Research Consortium: Columbus, OH, USA, 2013. [Google Scholar]
- McQueen, K.; Murphy-Oikonen, J. Neonatal Abstinence Syndrome. N. Engl. J. Med. 2016, 375, 2468–2479. [Google Scholar] [CrossRef]
- Brown, M.S.; Hayes, M.J.; Thornton, L.M. Methadone versus morphine for treatment of neonatal abstinence syndrome: A prospective randomized clinical trial. J. Perinatol. 2014, 35, 278–283. [Google Scholar] [CrossRef]
- Lai, A.; Do, P.P.; Boucher, J.; Meyer, A. An Outpatient Methadone Weaning Program by a Neonatal Intensive Care Unit for Neonatal Abstinence Syndrome. Popul. Health Manag. 2017, 20, 397–401. [Google Scholar] [CrossRef] [PubMed]
- Napolitano, A.; Theophilopoulos, D.; Seng, S.K.; Calhoun, D.A. Pharmacologic Management of Neonatal Abstinence Syndrome in a Community Hospital. Clin. Obs. Gynecol. 2013, 56, 193–201. [Google Scholar] [CrossRef]
- Raffaeli, G.; Cavallaro, G.; Allegaert, K.; Wildschut, E.D.; Fumagalli, M.; Agosti, M.; Tibboel, D.; Mosca, F. Neonatal Abstinence Syndrome: Update on Diagnostic and Therapeutic Strategies. Pharm. J. Hum. Pharm. Drug. 2017, 37, 814–823. [Google Scholar] [CrossRef]
- Siu, A.; Robinson, C.A. Neonatal Abstinence Syndrome: Essentials for the Practitioner. J. Pediatr. Pharm. 2014, 19, 147–155. [Google Scholar] [CrossRef]
- Davis, J.M.; Shenberger, J.; Terrin, N.; Breeze, J.L.; Hudak, M.; Wachman, E.M.; Marro, P.; Oliveira Érica, L.; Harvey-Wilkes, K.; Czynski, A.; et al. Comparison of Safety and Efficacy of Methadone vs. Morphine for Treatment of Neonatal Abstinence Syndrome: A Randomized Clinical Trial. JAMA Pediatr. 2018, 172, 741–748. [Google Scholar] [CrossRef]
- Hall, E.S.; Meinzen-Derr, J.; Wexelblatt, S.L. Cohort Analysis of a Pharmacokinetic-Modeled Methadone Weaning Optimization for Neonatal Abstinence Syndrome. J. Pediatr. 2015, 167, 1221–1225.e1. [Google Scholar] [CrossRef]
- Van Der Graaf, P.H. Introduction to Population Pharmacokinetic/Pharmacodynamic Analysis with Nonlinear Mixed Effects Models. Cpt Pharm. Syst. Pharm. 2014, 3, e153. [Google Scholar] [CrossRef]
- Committee on Obstetric Practice Committee Opinion No. 711: Opioid Use and Opioid Use Disorder in Pregnancy. Obs. Gynecol. 2017, 130, e81–e94. [CrossRef] [PubMed]
- Cleary, B.J.; Donnelly, J.M.; Strawbridge, J.D.; Gallagher, P.J.; Fahey, T.; White, M.J.; Murphy, D.J. Methadone and perinatal outcomes: A retrospective cohort study. Am. J. Obs. Gynecol. 2011, 204, 139.e1–139.e9. [Google Scholar] [CrossRef] [PubMed]
- Thigpen, J.; Melton, S.T. Neonatal Abstinence Syndrome: A Challenge for Medical Providers, Mothers, and Society. J. Pediatr. Pharm. 2014, 19, 144–146. [Google Scholar] [CrossRef]
- Allocco, E.; Melker, M.; Rojas-Miguez, F.; Bradley, C.; Hahn, K.A.; Wachman, E.M. Comparison of Neonatal Abstinence Syndrome Manifestations in Preterm Versus Term Opioid-Exposed Infants. Adv. Neonatal Care 2016, 16, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Anker, J.N.V.D.; McCune, S.; Annaert, P.; Baer, G.R.; Mulugeta, Y.; Abdelrahman, R.; Wu, K.; Krudys, K.M.; Fisher, J.; Slikker, W.; et al. Approaches to Dose Finding in Neonates, Illustrating the Variability between Neonatal Drug Development Programs. Pharmaceutics 2020, 12, 685. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Initial Phase * | Escalation Phase | Maintenance/Stabilization Phase | Weaning Phase | NAS Score | Total Daily Dose $ | |
|---|---|---|---|---|---|---|
| Dosing Recommendations International Guidelines | ||||||
| BNFc 2011–2012 [19] | 0.1 q6 h | ↑ by 0.05 q6 h until symptoms are under control | Total daily dose that controls symptoms divided over 2 doses | Reduce over 7–10 days | Yes | 0.4 |
| Nelson Textbook of Pediatrics 2015 [20] | 0.1 q12 h | ↑ by 0.025 q4 h (score > 8) maximum of 0.5 | Total daily dose that controls symptoms divided over 2 doses | Decrease dose by 10% every 1–2 weeks, discontinue when dose is 0.05 | Yes | 0.2 |
| Frank Shann’s Drug Doses 2017 [21] | 0.1–0.2 q6 h/q12 h | - | - | - | Yes | 0.2–0.8 |
| Neofax 2010 [22] | 0.05–0.2 q12 h/q24 h | - | - | 10–20% decrease every week, over 4–6 weeks | No | 0.05–0.4 |
| Neonatal formulary 7 2011 [23] | 0.1 q6 h | ↑ by 0.05 q6 h until symptoms are under control | Total daily dose that controls symptoms divided over 2 doses (q12 h) | Sustained control for 48 h -> reduce dose by 10–20% every day | Yes | 0.4 |
| VCHIP Neonatal Guideline [24] | 0.3–0.6 mg q12 h | ↑ by 0.05–0.2 mg (scores ≥ 9 after 4 doses) | - | If a dose of 0.02–0.05 mg twice a day is tolerated for 3–7 days, that dose is administered daily for 3–7 days and then discontinued. | Yes | 0.6–1.2 mg |
| Ohio Children`s Hospital Neonatal Research Consortium 2013 [25] | 0.05 q6 h | ↑ to 0.1 q6 h (score > 8 after 3 doses) -> to 0.15 q6 h (score >8 after 3 doses) | Dose that keeps scores <8 for minimum of 48 h. | Decrease dose by 10% q24 h and discontinue when dose is <0.02 | Yes | 0.2 |
| Dosing Regimens and Current Practice From Literature | ||||||
| van Donge et al., 2019 [10] | Day 1: 0.1 q6 h | - | - | Day 2: 0.1 q12 h, Day 3: 0.05 q12 h, Day 4–7: 0.01 q24 h | No | 0.4 |
| McQueen et al., 2016 [26] | 0.05 (score > 8 on 2 occasions or 1 score of ≥12) | ↑ by 0.02 (score ≥12) | Dose that keeps scores < 8 for minimum 48 h | Decrease dose by 10% q24 h and discontinue 72 h after withdrawal | Yes | 0.05 |
| Brown et al., 2015 [27] | 0.05 q4 h (score ≤ 12) 0.1 q4 h (score > 12) | - | 0.05 q12 h with maximum of 0.2 | Decrease dose by 10% if score ≤8 for q24 h | Yes | 0.3–0.6 |
| Lai et al., 2017 [28] | 0.1 q6 h (score > 8) | - | When score < 8 for 1–2 days, 0.1 q12 h | 0.1 q24 h | Yes | 0.4 |
| Napolitano et al., 2013 [29] | 0.1 q12 h | ↑ by 0.05 mg/kg q48 h with maximum of 1 mg/kg/day | - | Decrease dose by 10% at 1–2 week intervals | Yes | 0.2 |
| Raffaeli et al., 2017 [30] | 0.05–0.1 q12 h | ↑ dose by 10% q24 h-48 (score ≥ 12) maximum dose of 1 mg/kg/day | Dose that maintains score 9–11 | Decrease dose by 10% q24 h if score ≤ 8 | Yes | 0.1–0.2 |
| Siu et al., 2014 [31] | 0.05–0.1 q6 h-q24 h | - | - | Decrease dose by 10–20% every week | No | 0.05–0.4 |
| Davis et al., 2018 [32] | Score 8–10 0.3 q8 h Score 11–13 0.5 q8 h Score 14–16 0.7 q8 h Score ≥ 17 0.8 q8 h | - | - | Decrease maintenance dose by 10% q12 h-q48 h and discontinue when dose is 20% of initial dose | Yes | 0.9–2.4 |
| Wiles et al., 2015 [18] | 8 taper steps: 0.05 q6 h, 0.04 q6 h, 0.03 q6 h, 0.02 q6 h, 0.02 q8 h, 0.02 q12 h, 0.01 q12 h, 0.0.1 q24 h | If infant fails step 1 (score ≥ 12) consider 0.1 q6 h, 0.075 q6 h and 0.05 q6 h. | If average score is 8–12 do not wean. | Wean to the next step if average score is <8 for the past 24 h and discontinue after observations for 72 h from the last dose of step 8. | Yes | 0.2 |
| Hall et al., 2015 [33] | 8 taper steps: 0.1 q6 h, 0.07 q12 h, 0.05 q12 h, 0.04 q12 h, mg/kg q12 h, 0.02 q12 h, 0.01 q12 h, 0.01 q24 h | If infant fails step 1 (score ≥ 12) consider 0.1 mg/kg q4 h, 0.1 mg/kg q8 h, 0.1 mg/kg q12 h. | If average score is 8–12 do not wean. | Wean to the next step if average score is <8 for past 24 h and discontinue after observations for 72 h from the last dose of step 8. | Yes | 0.4 |
| 12 h after Birth | 24 h after Birth | 48 h after Birth | 72 h after Birth | ||
|---|---|---|---|---|---|
| Gestational age 28 weeks | |||||
| Start at 12 h | AUC | 399 [285–538] | 883 [633–1187] | 2167 [1566–2900] | 3557 [2609–4718] |
| Cmin | 31.1 [23.2–42.7] | 42.6 [30.8–56.9] | 54.3 [40.0–71.9] | 54.9 [40.9–71.7] | |
| Start at 36 h | AUC | 399 [285–538] | 766 [553–1047] | 1539 [1137–2067] | 2729 [2032–3673] |
| Cmin | 31.1 [23.2–42.7] | 29.6 [22.0–39.7] | 38.3 [28.7–51.5] | 50.9 [38.6–68.1] | |
| Gestational age 32 weeks | |||||
| Start at 12 h | AUC | 380 [282–505] | 838 [621–1112] | 2037 [1520–2688] | 3269 [2442–4253] |
| Cmin | 29.5 [21.9–38.8] | 39.8 [29.9–52.5] | 49.0 [36.8–63.4] | 46.0 [34.7–59.7] | |
| Start at 36 h | AUC | 380 [282–505] | 716 [548–948] | 1393 [1074–1836] | 2498 [1913–3244] |
| Cmin | 29.5 [21.9–38.8] | 25.9 [19.7–33.7] | 34.4 [26.5–44.7] | 45.0 [34.7–58.8] | |
| Gestational age 36 weeks | |||||
| Start at 12 h | AUC | 361 [274–478] | 811 [630–1054] | 1993 [1559–2585] | 3141 [2472–4077] |
| Cmin | 27.5 [21.0–35.7] | 38.8 [30.3–50.1] | 45.9 [36.0–60.0] | 40.7 [31.2–52.7] | |
| Start at 36 h | AUC | 361 [274–478] | 671 [505–864] | 1283 [961–1654] | 2361 [1818–3017] |
| Cmin | 27.5 [21.0–35.7] | 22.5 [16.9–29.8] | 32.7 [25.3–41.6] | 43.0 [33.0–54.4] | |
| Cumulative AUC (ng·h/mL) | 12 h after Birth | 24 h after Birth | 48 h after Birth | 72 h after Birth |
|---|---|---|---|---|
| Gestational age 28 weeks | ||||
| Neofax min | 399 [285–538] | 809 [583–1083] | 1563 [1155–2080] | 2281 [1694–3030] |
| Neofax max | 399 [285–538] | 920 [659–1241] | 2312 [1663–3107] | 4092 [2996–5471] |
| Gestational age 32 weeks | ||||
| Neofax min | 380 [282–505] | 756 [561–991] | 1401 [1061–1833] | 1965 [1501–2601] |
| Neofax max | 380 [282–505] | 880 [657–1168] | 2188 [1631–2886] | 3826 [2873–5028] |
| Gestational age 36 weeks | ||||
| Neofax min | 361 [274–478] | 704 [526–926] | 1279 [958–1675] | 1755 [1322–2299] |
| Neofax max | 361 [274–478] | 863 [654–1132] | 2194 [1666–2845] | 3786 [2895–4928] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Samiee-Zafarghandy, S.; van Donge, T.; Allegaert, K.; van den Anker, J. Pharmacometric Evaluation of Umbilical Cord Blood Concentration-Based Early Initiation of Treatment in Methadone-Exposed Preterm Neonates. Children 2021, 8, 174. https://doi.org/10.3390/children8030174
Samiee-Zafarghandy S, van Donge T, Allegaert K, van den Anker J. Pharmacometric Evaluation of Umbilical Cord Blood Concentration-Based Early Initiation of Treatment in Methadone-Exposed Preterm Neonates. Children. 2021; 8(3):174. https://doi.org/10.3390/children8030174
Chicago/Turabian StyleSamiee-Zafarghandy, Samira, Tamara van Donge, Karel Allegaert, and John van den Anker. 2021. "Pharmacometric Evaluation of Umbilical Cord Blood Concentration-Based Early Initiation of Treatment in Methadone-Exposed Preterm Neonates" Children 8, no. 3: 174. https://doi.org/10.3390/children8030174
APA StyleSamiee-Zafarghandy, S., van Donge, T., Allegaert, K., & van den Anker, J. (2021). Pharmacometric Evaluation of Umbilical Cord Blood Concentration-Based Early Initiation of Treatment in Methadone-Exposed Preterm Neonates. Children, 8(3), 174. https://doi.org/10.3390/children8030174