A Non-Invasive Investigation into the Prevalence of Higher than Normal Blood Pressure, Hypertension and the Association between Blood Pressure and Body Weight in Male and Female Adolescents in the Polokwane Local Municipality, Limpopo-South Africa: A Cross-Sectional Study

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Sampling Procedure
2.2. Exclusion and Inclusion Criteria
- Adolescents with cardiovascular conditions.
- Females who are pregnant or breastfeeding.
- Adolescents taking acute or chronic medication.
- Adolescents with orthopedic injuries.
- Adolescents who are using supplements (e.g., steroids).
2.3. Blood Pressure
2.4. Anthropometric Data (Weight and Height)
2.5. Statistical Analysis
2.6. Reliability and Validity
3. Results
3.1. Characteristics of the Population
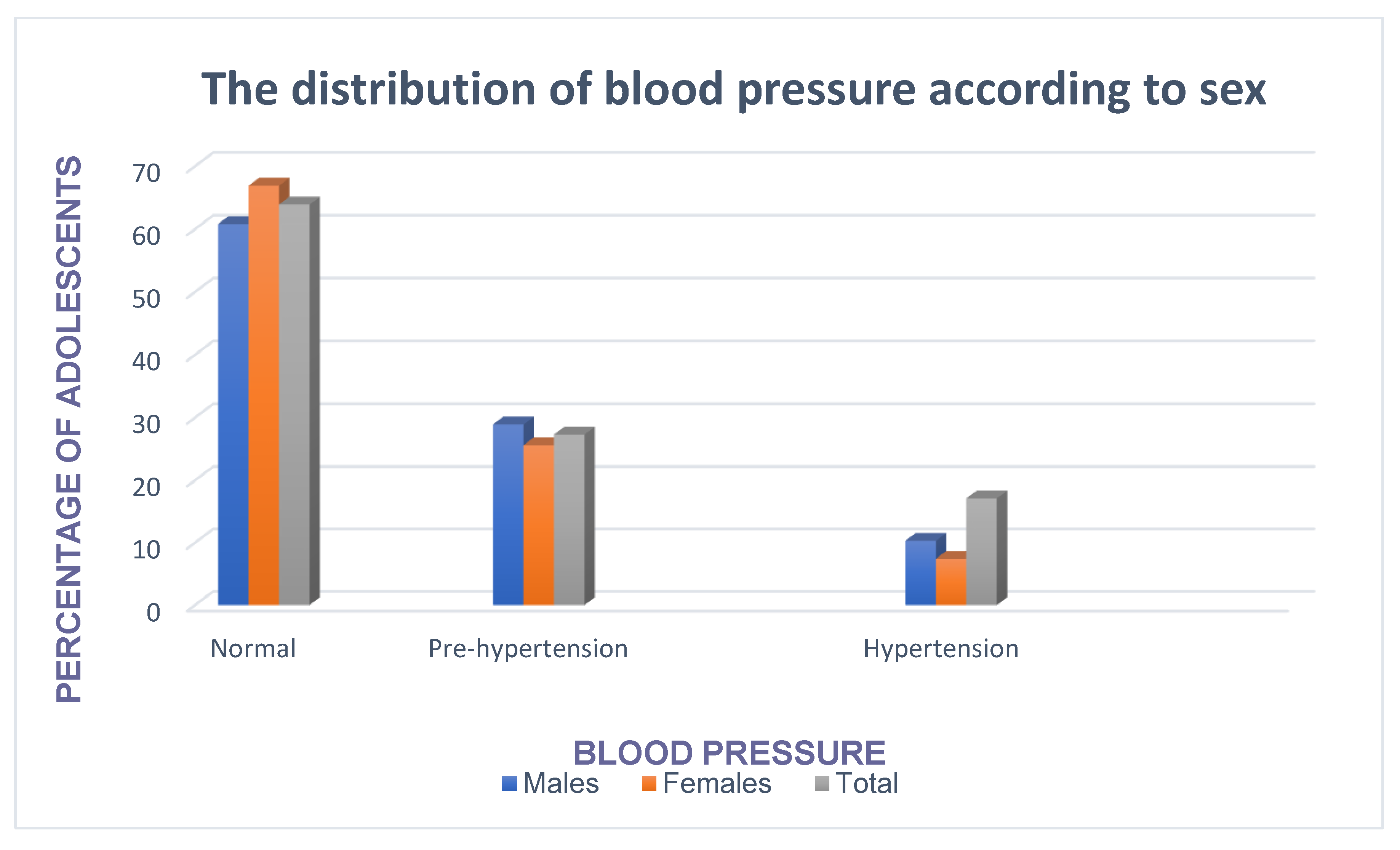
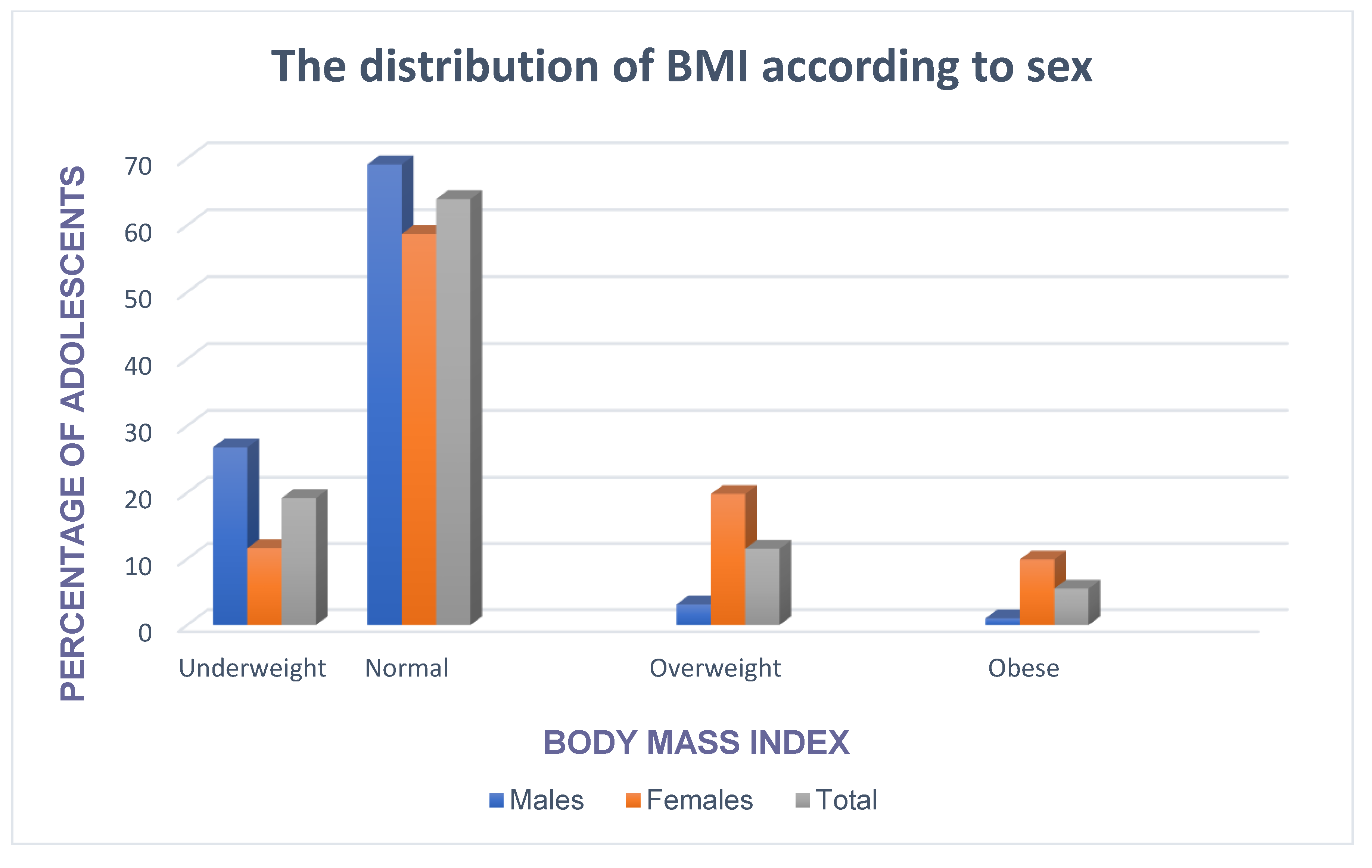
3.2. Prevalence of Prehypertension, Hypertension, Overweight and Obesity
3.3. Prevalence of Pre-Hypertension and Hypertension in Adolescents Who Were Overweight/Obesity
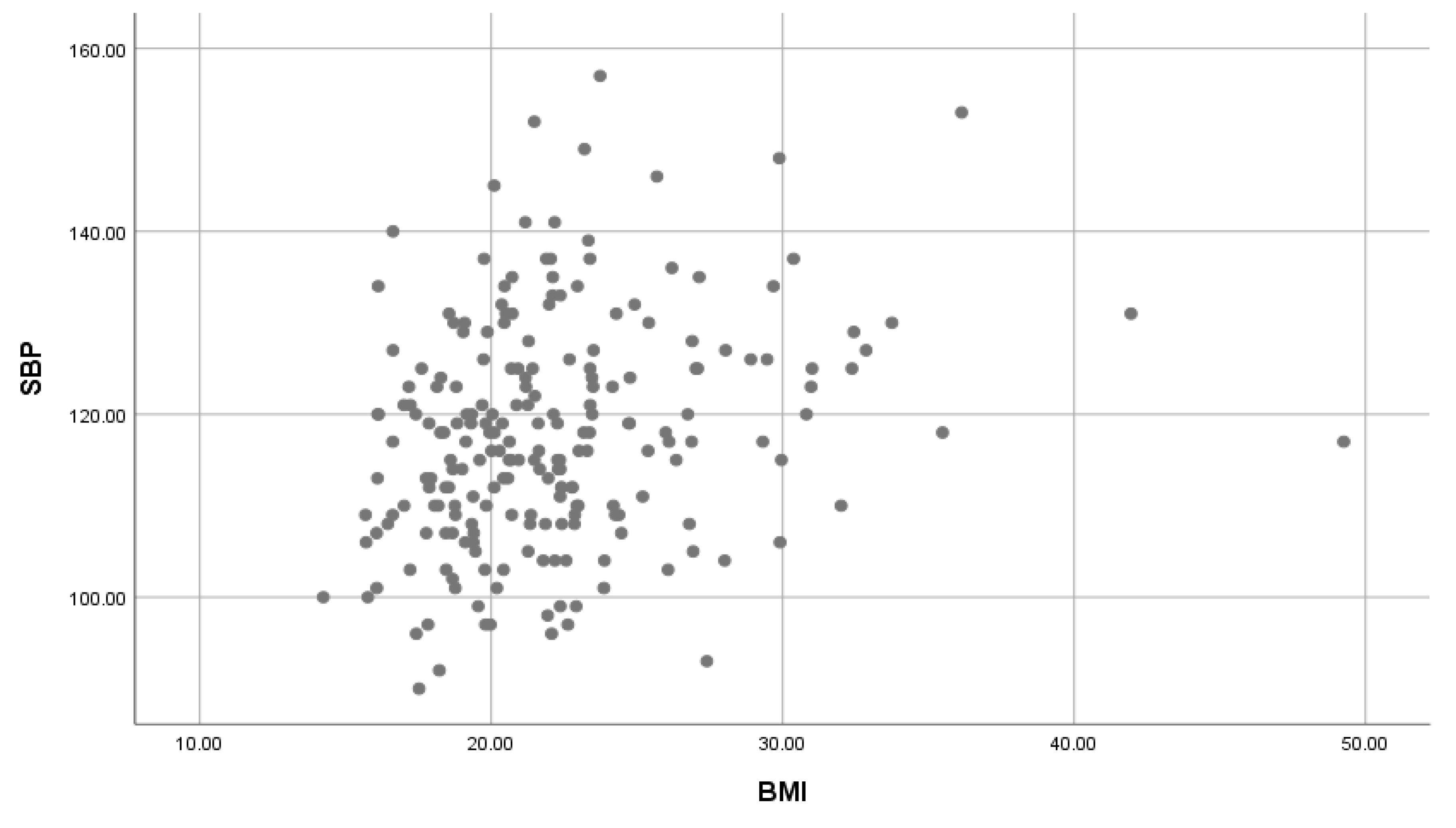
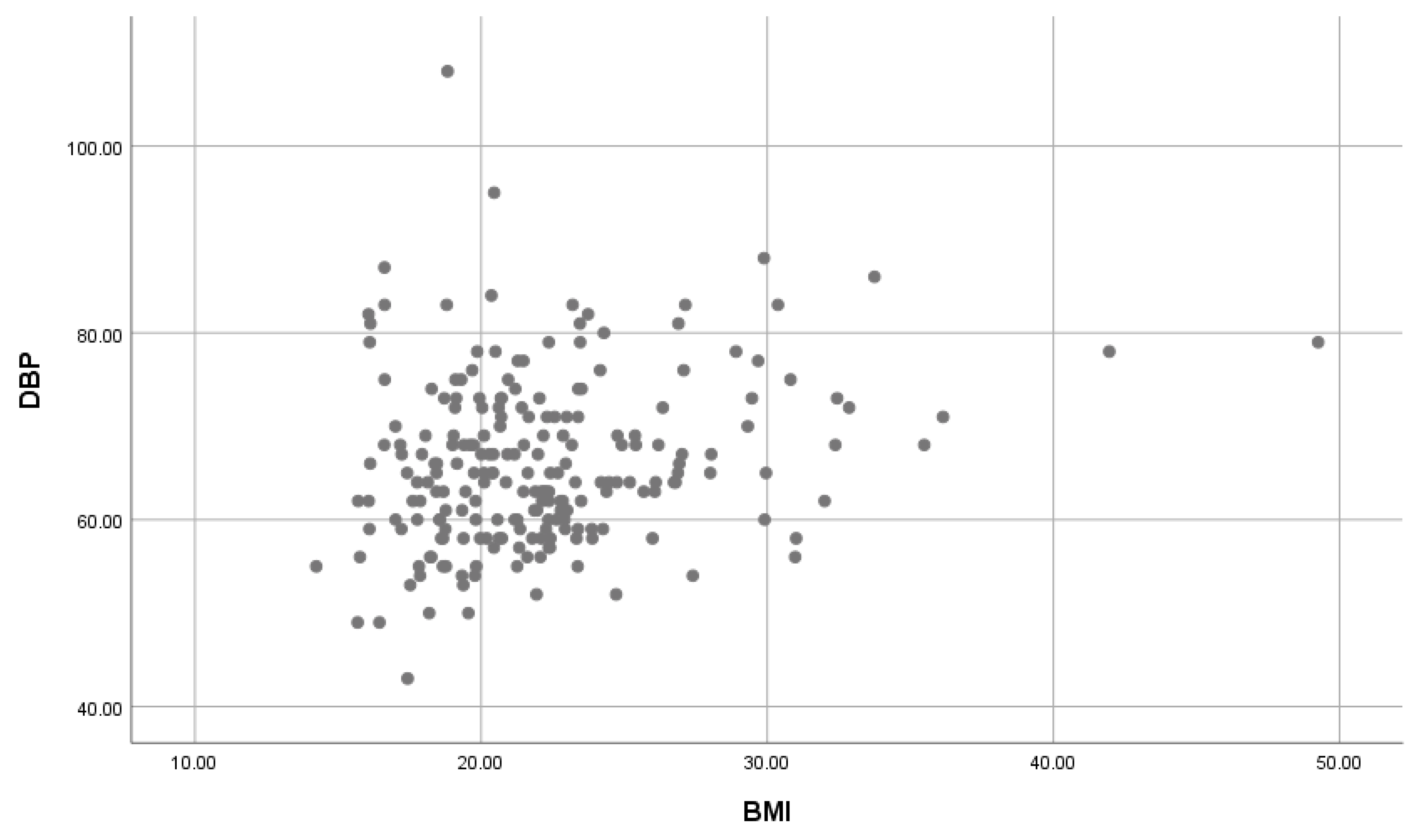
3.4. The Effect of BMI on SBP and DBP
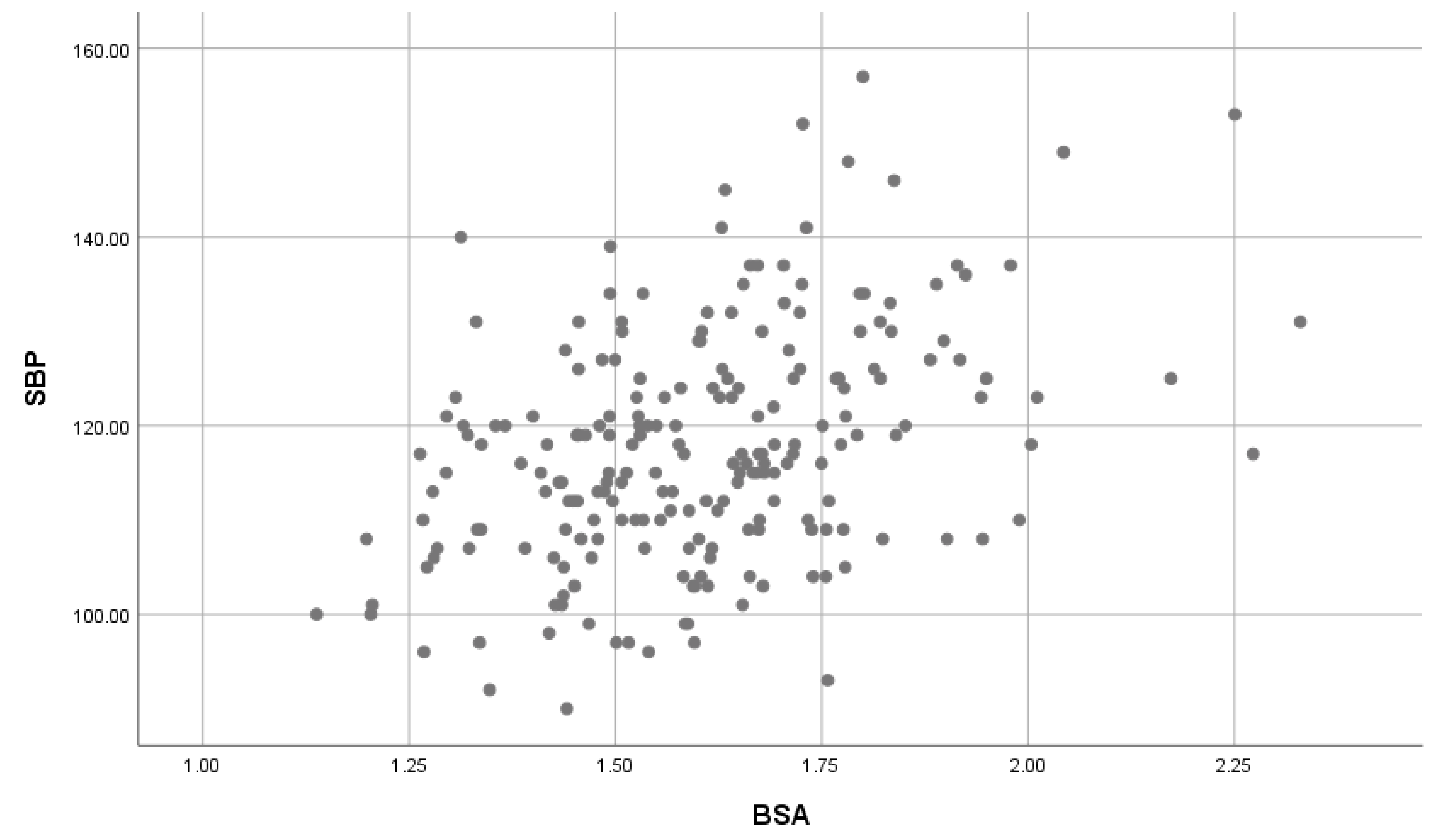
3.5. The Effect of BSA on SBP and DBP
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Prevention of Cardiovascular Disease: Guidelines for Assessment and Management of Cardiovascular Risk; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- World Health Organization. Global Status Report on Non-Communicable Diseases; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Parsekar, S.S.; Singh, M.M.; Venkatesh, B.T. High blood pressure and its association with obesity among preuniversity college students of Udupi taluk. Int. J. Public Health 2015, 4, 1. [Google Scholar] [CrossRef]
- Ewald, D.R.; Haldeman, L.A. Risk Factors in Adolescents Hypertension. GPH 2015, 3, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Kelly, R.K.; Magnussen, C.G.; Sabin, M.A.; Cheung, M.; Juonala, M. Development of hypertension in overweight adolescents: A review. Dove Press Med. J. 2015, 6, 171–187. [Google Scholar]
- Mamabolo, R.L.; Alberts, M.; Steyn, N.P.; Delemarre-van de wall, H.A.; Levitt, N. The prevalence and determinants of stunting and overweight in 3-years old black south African children residing in central regions of Limpopo province, South Africa. Public Health Nutr. 2005, 8, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Moselakgomo, V.K.; Van Staden, M. Predictors of obesity and cardiometabolic disease risk in South African children. Sajch 2017, 11, 187–192. [Google Scholar]
- Pickering, T.G.; Hall, J.E.; Appel, L.J.; Falkner, B.E.; Graves, J.W.; Hill, M.N.; Jones, D.W.; Kurtz, T.; Sheps, S.G.; Roccella, E.J. Recommendations for Blood Pressure Measurement in Humans: An AHA Scientific Statement from the Council on High Blood Pressure Research Professional and Public Education Subcommittee. Circulation 2005, 5, 697–716. [Google Scholar] [CrossRef] [PubMed]
- Aounallah-Skhiri, H.; El Ati, J.; Traissac, P.; Romdhane, H.B.; Eymard-Duvernay, S.; Delpeuch, F.; Achour, N.; Maire, B. Blood pressure and associated factors in a North Africa adolescent population. A national cross-sectional study in Tunisia. BMC Public Health 2012, 12, 98. [Google Scholar]
- National Heart, Lung and Blood Institute. The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents; National Heart, Lung and Blood Institute: Bethesda, MD, USA, 2005.
- Stewart, A.; Marefell-Jones, M.; Olds, T.; De Ridder, H. International Standards for Anthropometric Assessment; International Society for Advancement of Kinathropometry: Glasgow, Scotland, UK, 2011. [Google Scholar]
- World Health Organization. Obesity and Overweight, 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 14 March 2019).
- Vaccaro, C.A.; Vaccarezza, H.; Rossi, G.L.; Mentz, R.; Im, V.M.; Quintana, G.O.; Peralta, N.; Soriano, E.R. Body Surface Area: A new predictor factor for conversion and prolonged operative time in laparoscopic colorectal surgery. Dis. Colon Rectum J. 2012, 55, 1153–1159. [Google Scholar] [CrossRef] [PubMed]
- Papathanasiou, G.; Zerva, E.; Zacharis, I.; Papandreou, M.; Papageorgiou, E.; Tzima, C.; Georgakopoulos, D.; Evangelou, A. Association of high blood pressure with body mass index, smoking and physical activity in healthy young adults. Open Cardiovasc. Med. J. 2015, 55, 5–17. [Google Scholar] [CrossRef] [PubMed]
- Pate, R.R.; Stevens, J.; Webber, L.S.; Dowda, M.; Murray, D.M.; Young, D.R.; Going, S. Age-related change in physical activity in adolescents’ girls. J. Adolesc. Health 2009, 44, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Nkeh-Chungag, B.N.; Sekokotla, A.M.; Sewani-Rusike, C.; Namugowa, A.; Iputo, J.E. Prevalence of hypertension and pre-hypertension in 13–17 year old adolescents living in Mthatha- South Africa: A cross-sectional study. CEJPH 2015, 23, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Dubey, R.K.; Oparil, S.; Imthurn, B.; Jackson, E.K. Sex hormones and hypertension. Cardiovasc. Res. 2002, 53, 688–708. [Google Scholar] [CrossRef]
- Kolovou, G.; Giannakopoulou, V.; Vasiliadis, Y.; Bilianou, H. Effects of estrogens on atherogenesis. Curr. Vasc. 2011, 9, 244–257. [Google Scholar] [CrossRef] [PubMed]
- Palmieri, D.; Perego, P.; Palombo, D. Estrogen receptor activation protects against TNF-α- induced endothelial dysfunction. Angiol. J. 2014, 65, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Erlingsdottir, A.; Indridason, O.S.; Thorvaldsson, O.; Edvardsson, V.O. Blood pressure in children and target-organ damage later in life. Pediatr. Nephrol. 2010, 25, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Ejike, E.C.C.C. Blood pressure to height ratios as simple, sensitive and specific diagnostic tools for adolescent (pre)hypertension in Nigeria. Ital. J. Pediatr. 2011, 37, 30. [Google Scholar] [CrossRef] [PubMed]
- Abdulle, A.; Al-Junaibi, A.; Nagelkerke, N. High blood pressure and its association with body weight among children and adolescents in the United Arab Emirates. PLoS ONE 2014, 9, e85129. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Classification | Systolic and/or Diastolic Blood Pressure (mmHg) |
|---|---|
| Normal BP | <90th percentile |
| Prehypertension | 90th to <95th percentile or≥ 120 mmHg |
| Hypertension | >95th percentile |
| Males (n = 97) | Females (n = 121) | |
|---|---|---|
| Mean ± SD | Mean ± SD | |
| Age (years) | 17.3 ± 1.7 * | 16.8 ± 1.7 |
| SBP (mmHg) | 120.3 ± 13.7 * | 115.7 ± 10.7 |
| DBP (mmHg) | 64.8 ± 8.8 | 67.0 ± 9.0 * |
| Weight (kg) | 56.1 ± 11.6 | 59.4 ± 14.4 * |
| Height (m) | 1.7 ± 0.9 | 1.6 ± 0.7 |
| BMI (kg/m2) | 20.4 ± 3.0 | 23.6 ± 5.2 * |
| BSA (m2) | 1.6 ± 0.2 * | 1.6 ± 0.2 * |
| BP | Normal | Pre-Hypertension | Hypertension | Total |
|---|---|---|---|---|
| BMI | n (%) | n (%) | n (%) | n (%) |
| Underweight | 35 (16.1) | 4 (1.8) | 1 (0.4) | 40 (18.3) |
| Normal | 87 (39.9) | 39 (17.9) | 12 (5.5) | 138 (63.3) |
| Overweight | 15 (6.9) | 7 (3.2) | 5 (2.3) | 27 (12.4) |
| Obese | 3 (1.4) | 9 (4.1) | 1 (0.4) | 13 (6.0) |
| Total | 140 (64.3) | 59 (27) | 19 (8.6) | 218 (100.0) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raphadu, T.T.; Staden, M.V.; Dibakwane, W.M.; Monyeki, K.D. A Non-Invasive Investigation into the Prevalence of Higher than Normal Blood Pressure, Hypertension and the Association between Blood Pressure and Body Weight in Male and Female Adolescents in the Polokwane Local Municipality, Limpopo-South Africa: A Cross-Sectional Study. Children 2020, 7, 18. https://doi.org/10.3390/children7030018
Raphadu TT, Staden MV, Dibakwane WM, Monyeki KD. A Non-Invasive Investigation into the Prevalence of Higher than Normal Blood Pressure, Hypertension and the Association between Blood Pressure and Body Weight in Male and Female Adolescents in the Polokwane Local Municipality, Limpopo-South Africa: A Cross-Sectional Study. Children. 2020; 7(3):18. https://doi.org/10.3390/children7030018
Chicago/Turabian StyleRaphadu, Thato Tshepo, Marlise Van Staden, Winnie Maletladi Dibakwane, and Kotsedi Daniel Monyeki. 2020. "A Non-Invasive Investigation into the Prevalence of Higher than Normal Blood Pressure, Hypertension and the Association between Blood Pressure and Body Weight in Male and Female Adolescents in the Polokwane Local Municipality, Limpopo-South Africa: A Cross-Sectional Study" Children 7, no. 3: 18. https://doi.org/10.3390/children7030018
APA StyleRaphadu, T. T., Staden, M. V., Dibakwane, W. M., & Monyeki, K. D. (2020). A Non-Invasive Investigation into the Prevalence of Higher than Normal Blood Pressure, Hypertension and the Association between Blood Pressure and Body Weight in Male and Female Adolescents in the Polokwane Local Municipality, Limpopo-South Africa: A Cross-Sectional Study. Children, 7(3), 18. https://doi.org/10.3390/children7030018