
Chronic Disease in Pediatric Population—A Narrative Review of Psychosocial Dimensions and Strategies for Management

 ,
, 
Abstract
1. Introduction
Methods
2. Burden of Non-Communicable Diseases Among Children
3. Psychological Effects on Quality of Life in Children with a Chronic Disease
4. Coping with Chronic Disease in Daily Functioning
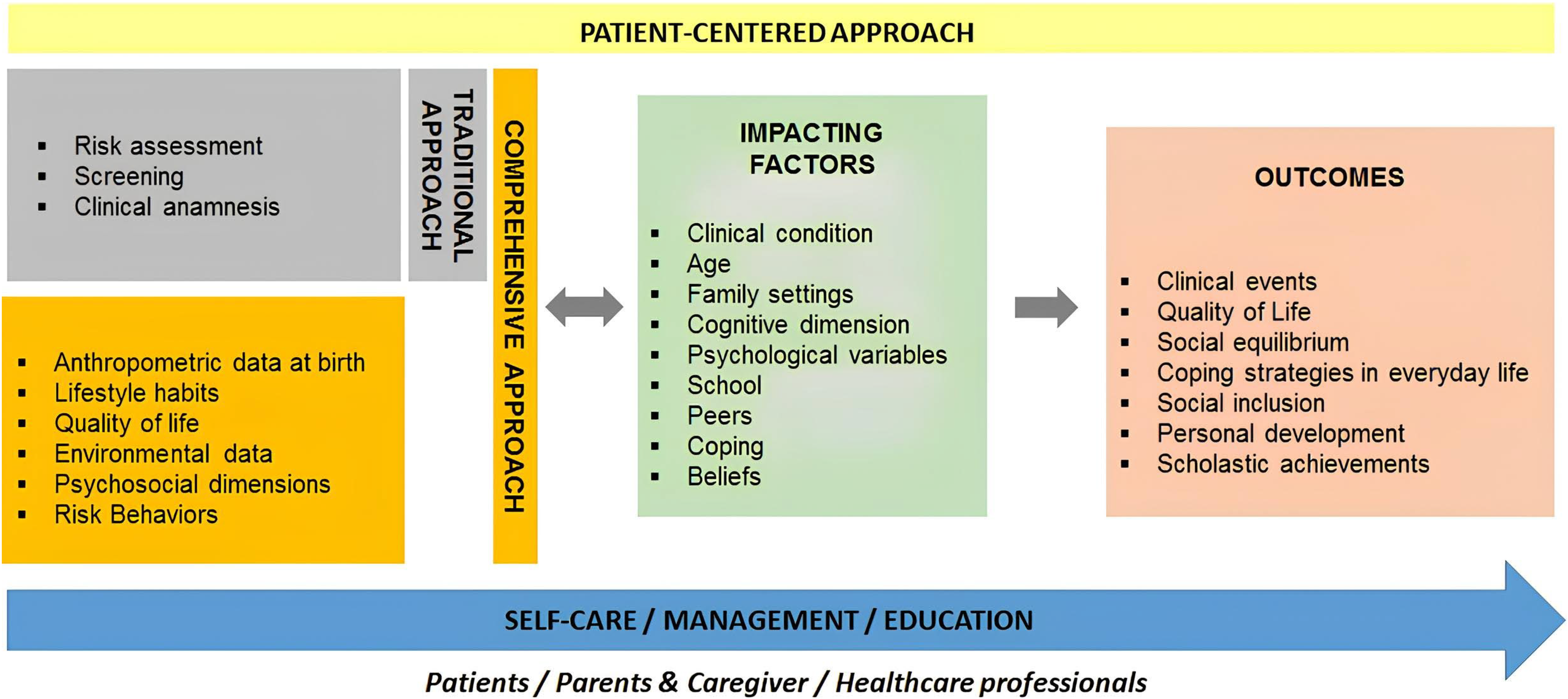
5. A Comprehensive Model for Health Management in Children with Chronic Disease
6. Limitations and Future Perspectives
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ishizaki, Y.; Ochiai, R.; Maru, M. Editorial: Advances of health care transition for patients with childhood-onset chronic diseases: International perspectives, volume II. Front. Pediatr. 2023, 11, 1147397. [Google Scholar] [CrossRef]
- National Center for Chronic Disease Prevention and Health Promotion. About Chronic Diseases. Available online: https://www.cdc.gov/chronic-disease/about/index.html (accessed on 13 June 2025).
- American Academy of Pediatrics. Chronic Conditions. HealthyChildren.Org. Available online: https://www.healthychildren.org/English/health-issues/conditions/chronic/Pages/default.aspx (accessed on 13 June 2022).
- Wagner, G.; Karwautz, A.; Philipp, J.; Truttmann, S.; Dür, W.; Waldherr, K.; Berger, G.; Zeiler, M. Mental Health and Health-Related Quality of Life in Austrian Adolescents with Chronic Physical Health Conditions: Results from the MHAT Study. J. Clin. Med. 2023, 12, 1927. [Google Scholar] [CrossRef]
- Petersson, C.; Simeonsson, R.J.; Enskar, K.; Huus, K. Comparing children’s self-report instruments for health-related quality of life using the International Classification of Functioning, Disability and Health for Children and Youth (ICF-CY). Health Qual. Life Outcomes 2013, 11, 75. [Google Scholar] [CrossRef]
- Paterson, G.A.; Nayda, R.J.; Paterson, J.A. Chronic condition self-management: Working in partnership toward appropriate models for age and culturally diverse clients. Contemp. Nurse 2012, 40, 169–178. [Google Scholar] [CrossRef]
- Berglund, M.M. Learning turning points—In life with long-term illness—Visualized with the help of the life-world philosophy. Int. J. Qual. Stud. Health Well-Being 2014, 9, 22842. [Google Scholar] [CrossRef]
- Queen Mary University of London. Chronic Illness in Childhood Linked to Higher Rates of Mental Illness. 2020. Available online: https://www.sciencedaily.com/releases/2020/05/200504114117.htm (accessed on 15 June 2022).
- Kelo, M.; Eriksson, E.; Eriksson, I. Pilot educational program to enhance empowering patient education of school-age children with diabetes. J. Diabetes Metab. Disord. 2013, 12, 16. [Google Scholar] [CrossRef]
- Kelo, A.; Anandarajah, G. Spirituality and coping with chronic disease in pediatrics. R. I. Med. J. 2013, 97, 26–30. [Google Scholar]
- Fayed, N.; Davis, A.M.; Streiner, D.L.; Rosenbaum, P.L.; Cunningham, C.E.; Lach, L.M.; Boyle, M.H.; Ronen, G.M.; Connolly, M.; Bello-Espinosa, L.; et al. Children’s perspective of quality of life in epilepsy. Neurology 2015, 84, 1830–1837. [Google Scholar] [CrossRef] [PubMed]
- Brady, A.M.; Deighton, J.; Stansfeld, S. Psychiatric outcomes associated with chronic illness in adolescence: A systematic review. J. Adolesc. 2017, 59, 112–123. [Google Scholar] [CrossRef] [PubMed]
- Wallander, J.L.; Varni, J.W. Effects of pediatric chronic physical disorders on child and family adjustment. J. Child. Psychol. Psychiatry 1998, 39, 29–46. [Google Scholar] [CrossRef]
- Varni, J.W.; Limbers, C.A.; Burwinkle, T.M. Impaired health-related quality of life in children and adolescents with chronic conditions: A comparative analysis of 10 disease clusters and 33 disease categories/severities utilizing the PedsQL 4.0 Generic Core Scales. Health Qual. Life Outcomes 2007, 5, 43. [Google Scholar] [CrossRef]
- Engel, G.L. The need for a new medical model: A challenge for biomedicine. Science 1977, 196, 129–136. [Google Scholar] [CrossRef] [PubMed]
- West, S.L.; Banks, L.; Schneiderman, J.E.; Caterini, J.E.; Stephens, S.; White, G.; Dogra, S.; Wells, G.D. Physical activity for children with chronic disease; a narrative review and practical applications. BMC Pediatr. 2019, 19, 12. [Google Scholar] [CrossRef]
- Jin, M.; An, Q.; Wang, L. Chronic conditions in adolescents. Exp. Ther. Med. 2017, 14, 478–482. [Google Scholar] [CrossRef] [PubMed]
- Sabatino, L.; Iervasi, G.; Pingitore, A. Thyroid hormone and heart failure: From myocardial protection to systemic regulation. Expert. Rev. Cardiovasc. Ther. 2014, 12, 1227–1236. [Google Scholar] [CrossRef] [PubMed]
- Bernell, S.; Howard, S.W. Use Your Words Carefully: What Is a Chronic Disease? Front. Public Health 2016, 4, 159. [Google Scholar] [CrossRef]
- GBD 2019 Child and Adolescent Communicable Disease Collaborators. The unfinished agenda of communicable diseases among children and adolescents before the COVID-19 pandemic, 1990–2019: A systematic analysis of the Global Burden of Disease Study 2019. Lancet 2023, 402, 313–335. [Google Scholar] [CrossRef]
- Compas, B.E.; Jaser, S.S.; Dunn, M.J.; Rodriguez, E.M. Coping with chronic illness in childhood and adolescence. Annu. Rev. Clin. Psychol. 2012, 8, 455–480. [Google Scholar] [CrossRef]
- Akseer, N.; Mehta, S.; Wigle, J.; Chera, R.; Brickman, Z.J.; Al-Gashm, S.; Sorichetti, B.; Vandermorris, A.; Hipgrave, D.B.; Schwalbe, N.; et al. Non-communicable diseases among adolescents: Current status, determinants, interventions and policies. BMC Public Health 2020, 20, 1908. [Google Scholar] [CrossRef]
- Denny, S.; de Silva, M.; Fleming, T.; Clark, T.; Merry, S.; Ameratunga, S.; Milfont, T.; Farrant, B.; Fortune, S.A. The prevalence of chronic health conditions impacting on daily functioning and the association with emotional well-being among a national sample of high school students. J. Adolesc. Health 2014, 54, 410–415. [Google Scholar] [CrossRef]
- Delaney, L.; Smith, J.P. Childhood health: Trends and consequences over the life course. Future Child. 2012, 22, 43–63. [Google Scholar] [CrossRef] [PubMed]
- The Global Asthma Report. Global Asthma Network, Auckland, New Zealand. 2018. Available online: https://globalasthmareport.org/2018/resources/Global_Asthma_Report_2018.pdf (accessed on 10 April 2024).
- Candelino, M.; Tagi, V.M.; Chiarelli, F. Cardiovascular risk in children: A burden for future generations. Ital. J. Pediatr. 2022, 48, 57. [Google Scholar] [CrossRef] [PubMed]
- The World Health Organization. Children: Improving Survival and Well-Being. Report. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/children-reducing-mortality (accessed on 3 May 2024).
- Meeting Report: Redesigning Child and Adolescent Health Programmes; WHO: Geneva, Switzerland, 2019.
- The World Health Organization Quality of Life assessment (WHOQOL): Position paper from the World Health Organization. Soc. Sci. Med. 1995, 41, 1403–1409. [CrossRef] [PubMed]
- Eiser, C.; Morse, R. A review of measures of quality of life for children with chronic illness. Arch. Dis. Child. 2001, 84, 205–211. [Google Scholar] [CrossRef]
- Hill, P.C.; Pargament, K.I. Advances in the conceptualization and measurement of religion and spirituality: Implications for physical and mental health research. Am. Psychol. 2008, 58, 64–74. [Google Scholar] [CrossRef]
- Reynolds, N.; Mrug, S.; Wolfe, K.; Schwebel, D.; Wallander, J. Spiritual coping, psychosocial adjustment, and physical health in youth with chronic illness: A meta-analytic review. Health Psychol. Rev. 2016, 10, 226–243. [Google Scholar] [CrossRef]
- Rohan, J.M.; Verma, T. Psychological Considerations in Pediatric Chronic Illness: Case Examples. Int. J. Environ. Res. Public Health 2020, 17, 1644. [Google Scholar] [CrossRef]
- Pinquart, M.; Teubert, D. Academic, physical, and social functioning of children and adolescents with chronic physical illness: A meta-analysis. J. Pediatr. Psychol. 2012, 37, 376–389. [Google Scholar] [CrossRef]
- Cottrell, D. Prevention and treatment of psychiatric disorders in children with chronic physical illness. Arch. Dis. Child. 2015, 100, 303–304. [Google Scholar] [CrossRef]
- Cobham, V.E.; Hickling, A.; Kimball, H.; Thomas, H.J.; Scott, J.G.; Middeldorp, C.M. Systematic Review: Anxiety in children and adolescents with chronic medical conditions. J. Am. Acad. Child. Adolesc. Psychiatry 2020, 59, 595–618. [Google Scholar] [CrossRef]
- Forrest, C.B.; Bevans, K.B.; Riley, A.W.; Crespo, R. School outcomes of children with special health care needs. Pediatrics 2011, 128, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Van Cleave, J.; Davis, M.M. Bullying and peer victimization among children with special health care needs. Pediatrics 2006, 118, e1212–e1219. [Google Scholar] [CrossRef] [PubMed]
- Hajek, C.A.; Yeates, K.O.; Anderson, V.; Mackay, M.; Greenham, M.; Gomes, A.; Lo, W. Cognitive outcomes following arterial ischemic stroke in infants and children. J. Child. Neurol. 2014, 29, 887–894. [Google Scholar] [CrossRef]
- Pop-Jordanova, N. Chronic Diseases in Children as a Challenge for Parenting. Prilozi 2023, 44, 27–36. [Google Scholar] [CrossRef]
- Lawoko, S.; Soares, J.J.F. Psychosocial morbidity among parents of children with congenital heart disease: A prospective longitudinal study. Heart Lung 2006, 35, 301–314. [Google Scholar] [CrossRef]
- Jackson, A.C.; Frydenberg, E.; Liang, R.P.T.; Higgins, R.O.; Murphy, B.M. Familial impact and coping with child heart disease: A systematic review. Pediatr. Cardiol. 2015, 36, 695–712. [Google Scholar] [CrossRef]
- Mutti, G.; Ait Ali, L.; Marotta, M.; Nunno, S.; Consigli, V.; Baratta, S.; Foffa, I. Psychological Impact of a Prenatal Diagnosis of Congenital Heart Disease on Parents: Is It Time for Tailored Psychological Support? J. Cardiovasc. Dev. Dis. 2024, 11, 31. [Google Scholar] [CrossRef]
- Mattson, G.; Kuo, D.Z. Committee on psychosocial aspects of child and family health; council on children with disabilities. Psychosocial factors in children and youth with special health care needs and their families. Pediatrics 2018, 143, e20183171. [Google Scholar] [CrossRef]
- Spencer, M. Impacts of caring for a child with chronic health problems on parental work status and security: A longitudinal cohort study. Fam. Matters 2014, 95, 24–29. [Google Scholar]
- Shojaee, S.; Alizadeh, H. Comparing behavioral-emotional difficulties in siblings of children with and without sensory impairments. Iran. J. Public. Health 2019, 48, 516–524. [Google Scholar] [CrossRef]
- Caliendo, M.; Lanzara, V.; Vetri, L.; Roccella, M.; Marotta, R.; Carotenuto, M.; Russo, D.; Cerroni, F.; Precenzano, F. Emotional-behavioral disorders in healthy siblings of children with neurodevelopmental disorders. Medicina 2020, 56, 491. [Google Scholar] [CrossRef]
- Quintana Mariñez, M.G.; Chakkera, M.; Ravi, N.; Ramaraju, R.; Vats, A.; Nair, A.R.; Khan, S. The Other Sibling: A Systematic Review of the Mental Health Effects on a Healthy Sibling of a Child with a Chronic Disease. Cureus 2022, 14, e29042. [Google Scholar] [CrossRef]
- Van Cleave, J.; Gortmaker, S.L.; Perrin, J.M. Dynamics of obesity and chronic health conditions among children and youth. JAMA 2010, 303, 623–630. [Google Scholar] [CrossRef]
- Marin, T.J.; Chen, E.; Munch, T.; Miller, G. Double exposure to acute stress and chronic family stress is associated with immune changes in children with asthma. Psychosom. Med. 2009, 71, 378–384. [Google Scholar] [CrossRef]
- Juster, R.P.; McEwen, B.S.; Lupien, S.J. Allostatic load biomarkers of chronic stress and impact on health and cognition. Neurosci. Biobehav. Rev. 2010, 35, 2–16. [Google Scholar] [CrossRef] [PubMed]
- Colizzi, M.; Lasalvia, A.; Ruggeri, M. Prevention and early intervention in youth mental health: Is it time for a multidisciplinary and trans-diagnostic model for care? Int. J. Ment. Health Syst. 2020, 14, 23. [Google Scholar] [CrossRef] [PubMed]
- Harjutsalo, V.; Sjoberg, L.; Tuomilehto, J. Time trends in the incidence of type 1 diabetes in Finnish in children: A cohort study. Lancet 2008, 371, 1777–1782. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Standards of medical care in diabetes–2011. Diab. Care 2011, 34, S11–S61. [Google Scholar] [CrossRef]
- Davidson, M.; Penney, E.A.; Muller, B.; Grey, M. Stressors and self-care challenges faced by adolescents living with type 1 diabetes. Appl. Nurs. Res. 2004, 17, 72–80. [Google Scholar] [CrossRef]
- Thompson, R.D.; Delaney, P.; Flores, I.; Szigethy, E. Cognitive-behavioral therapy for children with comorbid physical illness. Child Adolesc. Psychiatr. Clin. N. Am. 2011, 20, 329–348. [Google Scholar] [CrossRef]
- Yonker, J.E.; Schnabelrauch, C.A.; DeHaan, L.G. The relationship between spirituality and religiosity on psychological outcomes in adolescents and emerging adults: A meta-analytic review. J. Adolesc. 2012, 35, 299–314. [Google Scholar] [CrossRef]
- Modi, A.C.; Pai, A.L.; Hommel, K.A.; Hood, K.K.; Cortina, S.; Hilliard, M.E.; Guilfoyle, S.M.; Gray, W.N.; Drotar, D. Pediatric self-management: A framework for research, practice, and policy. Pediatrics 2012, 129, e473–e485. [Google Scholar] [CrossRef]
- Saxby, N.; Ford, K.; Beggs, S.; Battersby, M.; Lawn, S. Developmentally appropriate supported self-management for children and young people with chronic conditions: A consensus. Patient Educ. Couns. 2020, 103, 571–581. [Google Scholar] [CrossRef]
- Mastorci, F.; Ait-Ali, L.; Festa, P.; Martini, M.; Gagliardi, L.; Calabri, G.; La Marca, G.; Trivellini, G.; Casu, A.; Dalmiani, S.; et al. A New Web Score to Predict Health Status in Paediatric Patients with Chronic Diseases: Design and Development of the PENSAMI Study. Children 2021, 8, 1094. [Google Scholar] [CrossRef]

{kind=link}
| Main Author | Type of Article | Study Population | Materials and Methods | Main Results |
|---|---|---|---|---|
| Wagner [4] | Research Article | Children with CD | In a representative sample of Austrian adolescents aged 10–18 years, internalizing, externalizing, and behavioral problems were assessed cross-sectionally using the Youth Self-Report and health-related quality of life (HrQoL) using the KIDSCREEN questionnaire. | Of 3469 adolescents, 9.4% of girls and 7.1% of boys suffered from a chronic pediatric illness. Of these individuals, 31.7% and 11.9% had clinically relevant levels of internalizing and externalizing mental health problems, respectively, compared to 16.3% and 7.1% healthy adolescents. Anxiety, depression, and social problems were twice as high in this population. |
| Quintana [48] | Systematic Review | Siblings | / | The siblings of those with chronic illnesses have higher reported emotional, behavioral, and social problems than those with healthy siblings. |
| Queen Mary University of London [8] | Research Article | Children with CD | The results involved 7000 children. The measure of chronic illness was based on mothers assessing their child’s health at 10 and 13. | Children with CD were approximately twice as likely at 10 and at 13 to present with a mental health disorder than the control group (children reported by their mothers to be ‘healthy, no problems’). At age 15, children with chronic health problems were 60% more likely to present with such disorders. |
| Cohbam [36] | Systematic Review | Children with CD | / | Given the burden of disease of anxiety disorders, regardless of the impact on the disease outcomes, screening for and treatment of anxiety is recommended in youths with chronic medical conditions. |
| Caliendo [47] | Research Article | Parents | The results involve 153 children from the region of Campania and their caregivers through the administration of the Strength and Difficulties Questionnaire. | From the data, it emerged that siblings of children with autism spectrum disorder and siblings of children with Down syndrome have a greater emotional fragility, especially among male subjects. |
| Shojaee and Alizadeh [46] | Research Article | Siblings | The sample included all siblings of children with and without sensory impairment (SI). The sample consisted of 91 subjects: 38 siblings of children with SI and 53 without SI. | Siblings of children with SI are significantly at a higher risk of psychological diseases and need support and services. |
| Fayed [11] | Research Article | Children with CD | QUALITÉ cohort study includes 6 Canadian child epilepsy ambulatory programs with a total sample of 3481 children. | QOL is strongly related to mental health and social support in children with CD, but not to their seizures. |
| Jackson [42] | Systematic Review | Parents | / | A holistic approach should aim at improving adaptive capacities and productive parenting practices. This should lay a solid basis for these families to successfully deal with future challenges and uncertainties at various stages in the trajectory of the child’s status. |
| Denny [23] | Research Article | Children with CD | A sample of 9107 students (Years 9–13) from 96 New Zealand high schools. Students were asked about any chronic illnesses or disabilities. | One in five students reported having a chronic health condition; of these, 28% reported a negative impact of the disease on their daily activities, and 8% reported an impact on their ability to socialize. |
| Hajek [39] | Research Article | Children with CD | Participants included 36 children with perinatal or childhood arterial ischemic stroke and a comparison group of 15 children with asthma. Outcomes included cognitive ability, executive functions, and neurological function (Pediatric Stroke Outcome Measure). Magnetic resonance imaging measured lesion location and volume. | Following arterial ischemic stroke, children performed at the low end of the average range on measures of cognitive functioning. Cognitive outcomes depend on a variety of factors. |
| Spencer [45] | A cohort study | Parents | The study commenced in 2004 with two cohorts: families with 0–1-year-old infants (the B cohort) and families with 4–5-year-old children (the K cohort). Interviews took place in the family home with the main respondent, usually the mother (99%). | This study is consistent with published literature in that it finds there is an impact on parental work status of caring for a child with chronic health problems in the early years of life. The work status of both parents was adversely affected, although in different ways. |
| Kelo [9] | Research Article | Children with CD | Education protocols for school-age children with diabetes by nurses. | The education of patient management process was successfully described. |
| Forrest [37] | Research Article | Children with CD | A total of 1457 children in the fourth through sixth grades from 34 schools in 3 school districts and their parents provided survey data; parents completed the Children With Special Health Care Needs Screener. | In total, 33% of children screened positive for special health care needs. They experienced significantly lower academic achievement, as measured by grades, standardized testing, and parental-assessed academic performance. |
| Van Cleave [50] | A cohort study | Children with CD | Cohort is represented by National Longitudinal Survey of Youth-Child Cohort (1988–2006). Children were aged 2 through 8 years at the beginning of each study period, and cohorts were followed up for 6 years. | Prevalence of CD increased from 1988 to 2006. However, presence of these conditions was dynamic over each 6-year cohort. |
| Marin [51] | Research Article | Children with CD | A total of 71 children with asthma and 76 medically healthy children completed interviews regarding life stress, and peripheral blood samples were collected. After mononuclear cells had been mitogenically stimulated, production of the cytokines IL-4, IL-5, IL-13, and IFN-γ was measured. All measurements were repeated every 6 months for two years. | Children with asthma who had higher levels of chronic family stress showed increased production of IL-4, IL-5, and IFN-γ at times when they had experienced an acute event compared to times when they had not. These stress-related changes did not occur in asthmatic children with lower levels of chronic family stress or in healthy controls. |
| Harjutsalo [55] | A cohort study | Children with CD | Cohort study is represented by children with type 1 diabetes listed on the National Public Health Institute diabetes register, Central Drug Register, and Hospital Discharge Register in 1980–2005. | The incidence of type 1 diabetes is increasing even faster than before. The number of new cases diagnosed at or before 14 years of age will double in the next 15 years, and the age of onset will be younger (0–4 years). |
| Varni [14] | Research Article | Children with CD | The analyses were based on over 2500 pediatric patients from 10 physician-diagnosed disease clusters. | Pediatric patients with CD reported progressively more impaired overall HRQOL than healthy children with medium-to-large effect sizes. |
| Van Cleave and Davis [38] | Research Article | Children with CD | A secondary data analysis using the National Survey of Children’s Health of >102,000 US households, measuring the association between having a special health care need and being a victim of bullying. | Overall, 21% of children with CD reported being bullied, resulting in chronic behavioral, emotional, or developmental problems. |
| Lawoko and Soares [41] | Prospective longitudinal study | Parents | / | A significant proportion of parents of children with congenital heart disease are at risk of long-term psychosocial morbidity, with a need to implement psychosocial interventions. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mastorci, F.; Lazzeri, M.F.L.; Ait-Ali, L.; Festa, P.; Pingitore, A. Chronic Disease in Pediatric Population—A Narrative Review of Psychosocial Dimensions and Strategies for Management. Children 2025, 12, 967. https://doi.org/10.3390/children12080967
Mastorci F, Lazzeri MFL, Ait-Ali L, Festa P, Pingitore A. Chronic Disease in Pediatric Population—A Narrative Review of Psychosocial Dimensions and Strategies for Management. Children. 2025; 12(8):967. https://doi.org/10.3390/children12080967
Chicago/Turabian StyleMastorci, Francesca, Maria Francesca Lodovica Lazzeri, Lamia Ait-Ali, Pierluigi Festa, and Alessandro Pingitore. 2025. "Chronic Disease in Pediatric Population—A Narrative Review of Psychosocial Dimensions and Strategies for Management" Children 12, no. 8: 967. https://doi.org/10.3390/children12080967
APA StyleMastorci, F., Lazzeri, M. F. L., Ait-Ali, L., Festa, P., & Pingitore, A. (2025). Chronic Disease in Pediatric Population—A Narrative Review of Psychosocial Dimensions and Strategies for Management. Children, 12(8), 967. https://doi.org/10.3390/children12080967