
Cerebral Palsy Link to Sensorimotor System, Cognition, Emotion and Nociplastic Pain


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
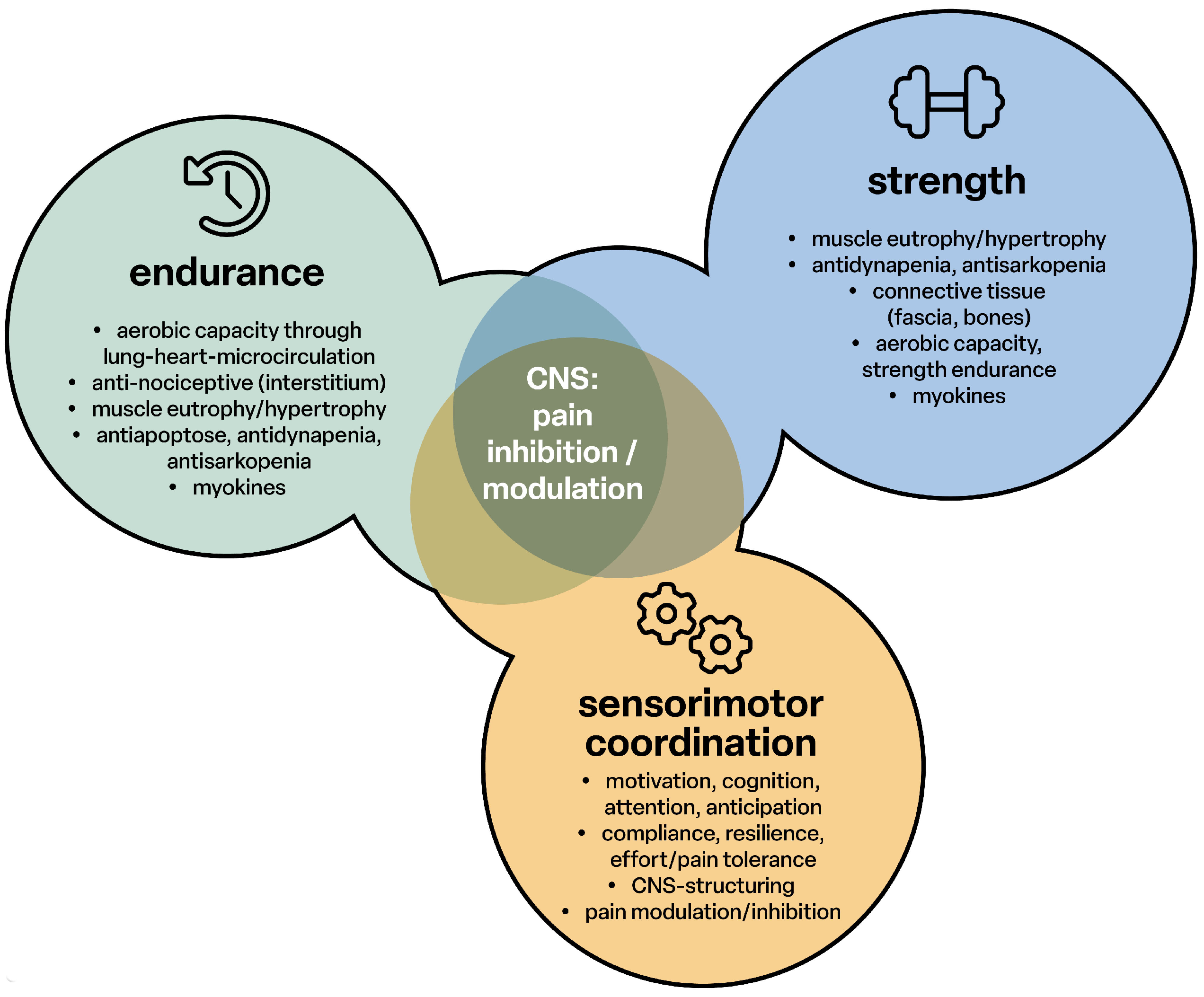
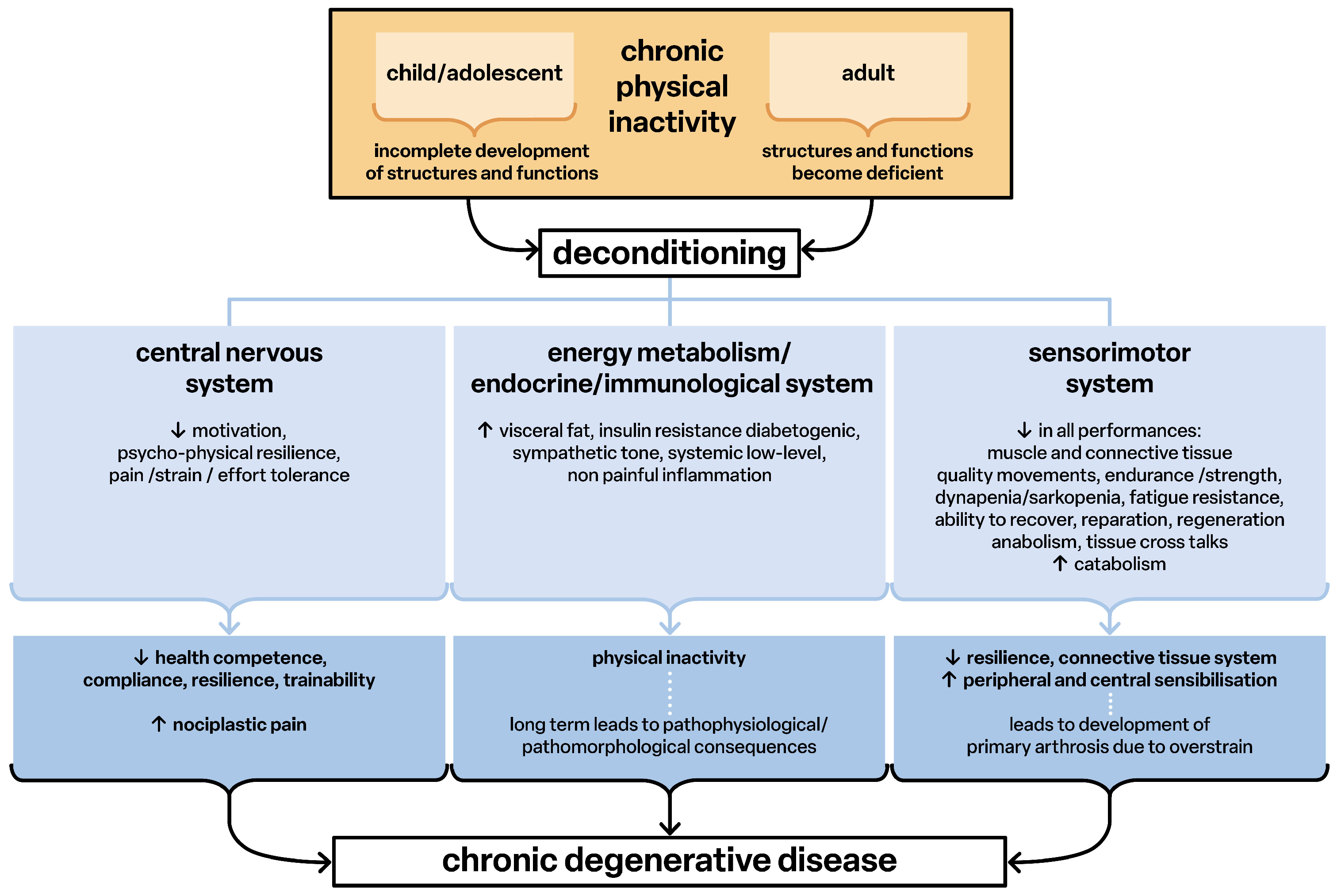
2. Link Between Impaired Sensorimotor Function Due to Deconditioning and Pain
- -
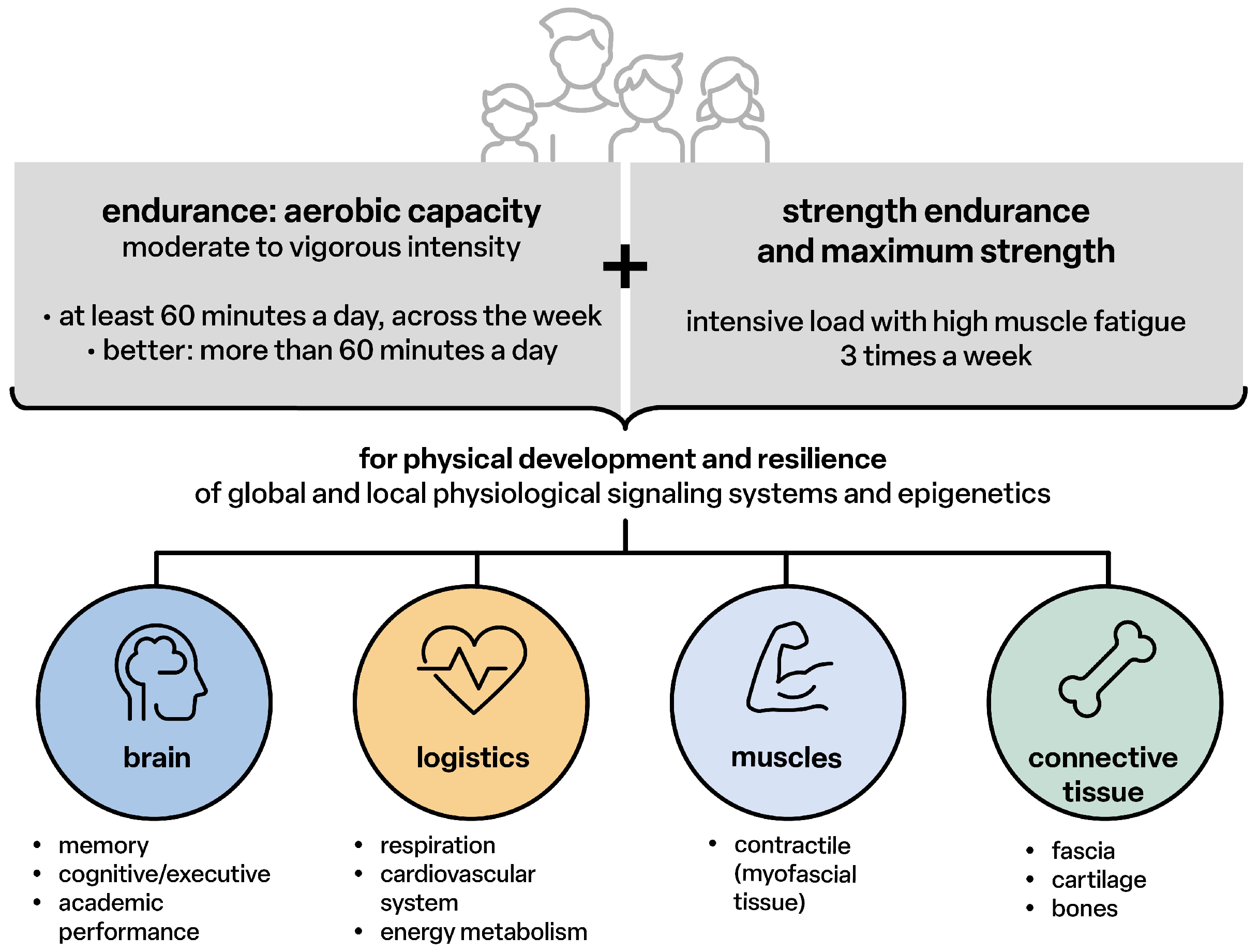
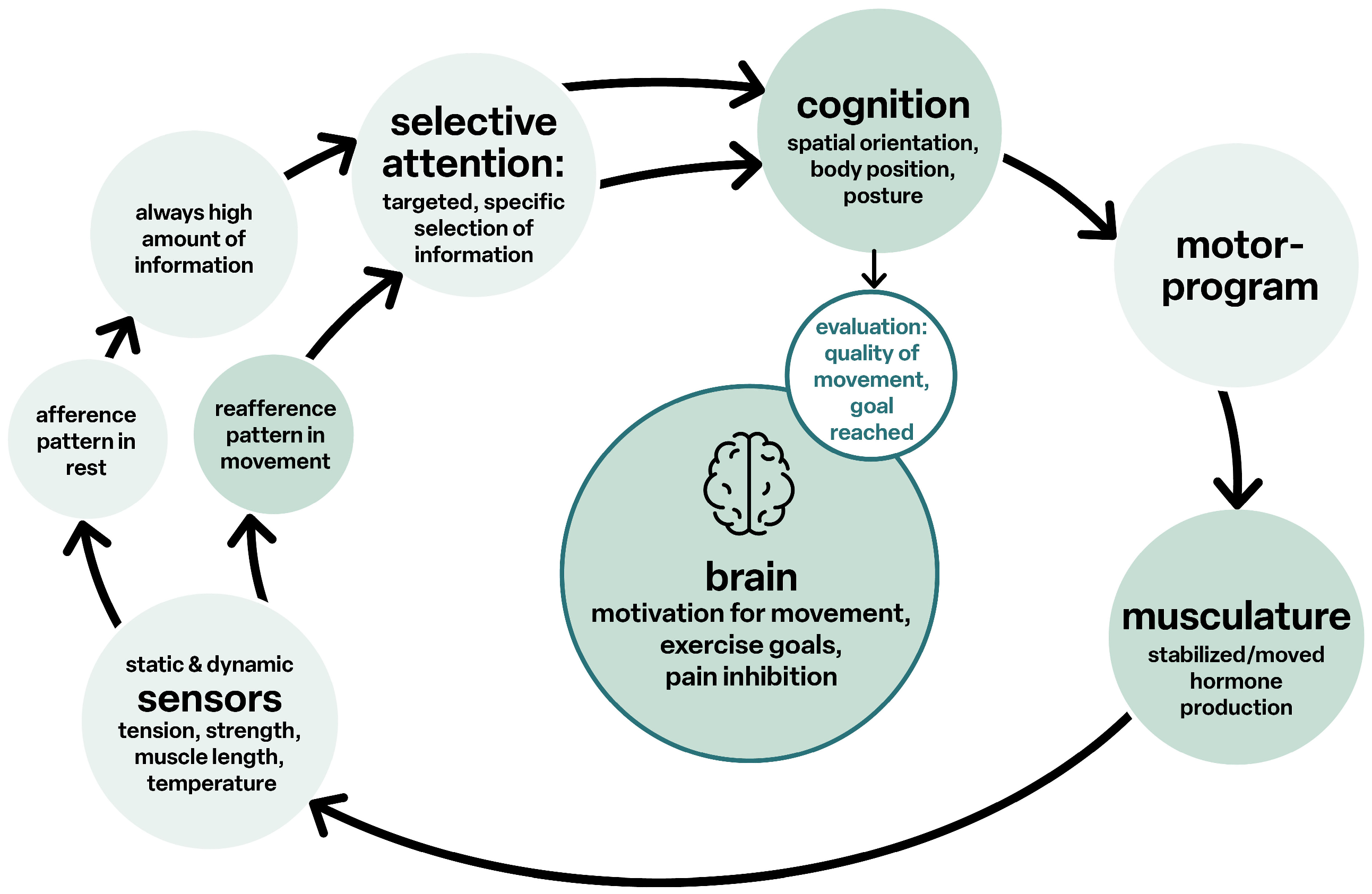
- Allow the genetic potential of physical development to become “fully” effective;
- -
- Enable all peripheral body structures and the nervous system with the brain as the highest level of behavior, communication and the integral cooperation of all structural and functional levels into a healthy, resilient, powerful and resistant functional state;
- -
- Maintain the structures and functions throughout the entire lifespan or delay the ageing process by continuing physical activities for at least 1.5 to 3.0 h per week (Figure 1).
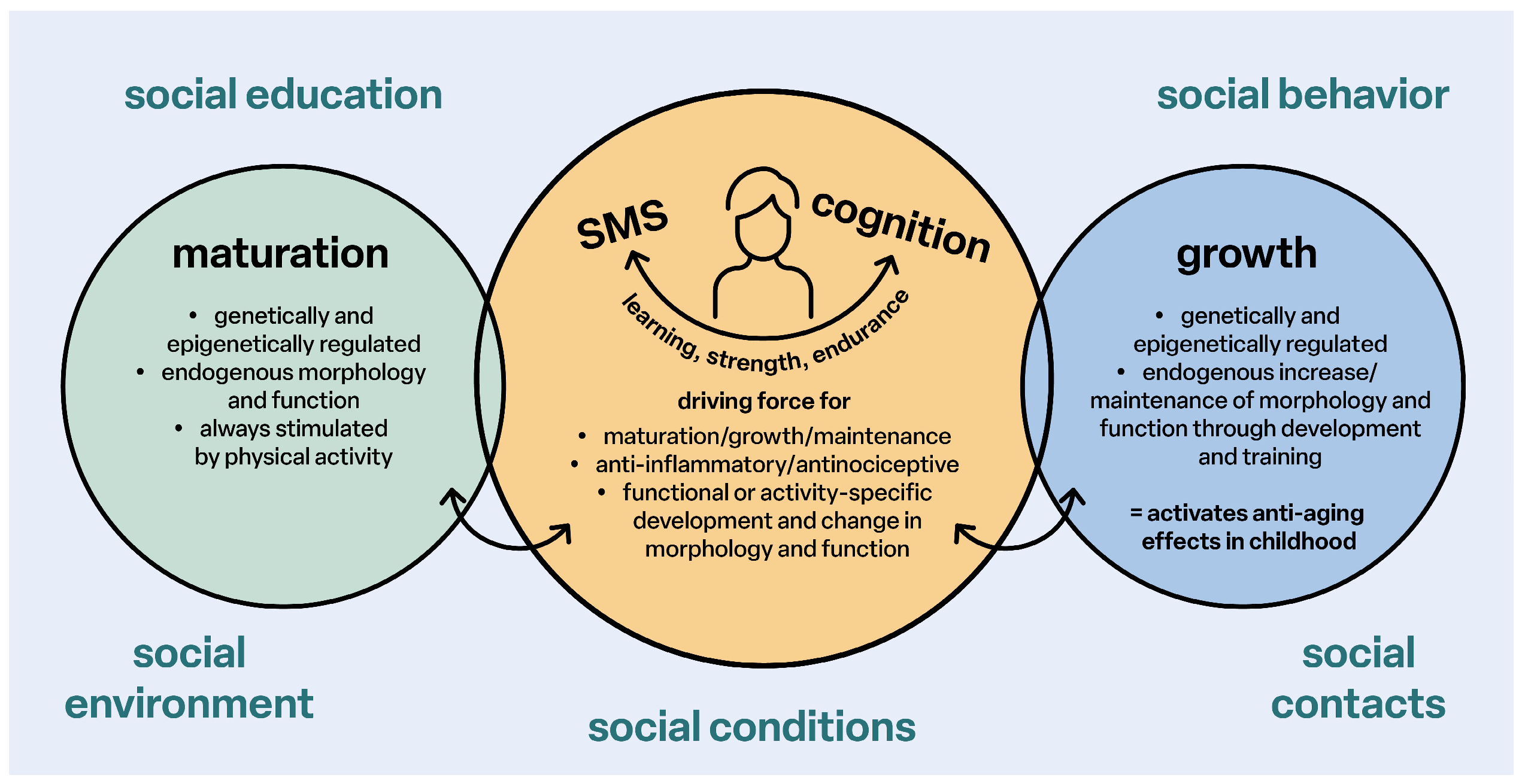
3. Link Between Delayed Sensorimotor Development and Cognition, Emotion
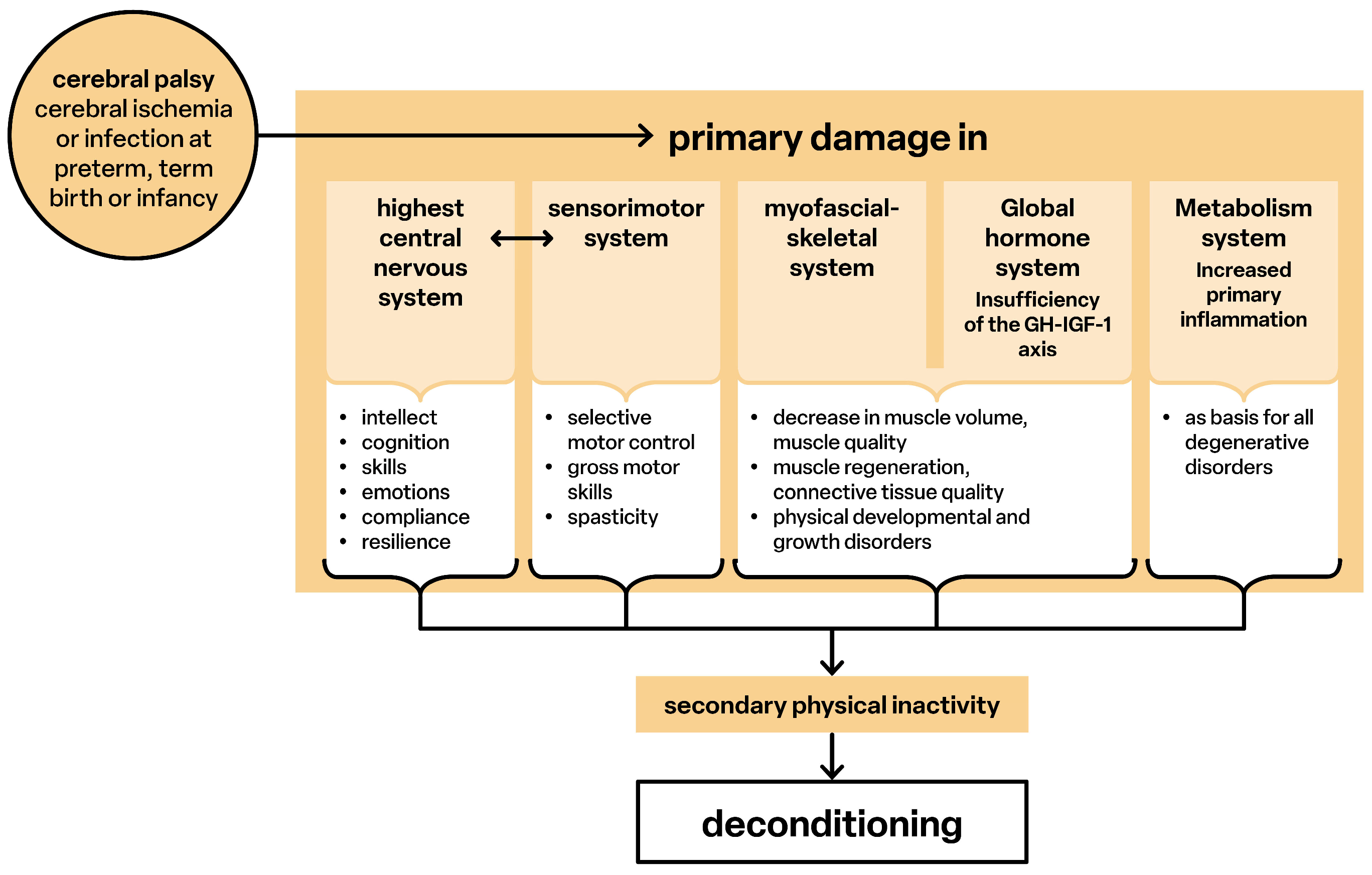
4. CP and Link to Damage to All Brain Functions
5. CP and Link to Sensorimotor Function and Cognition
6. CP and Link to Sensorimotor Function and Emotion
7. CP Link to Pain Syndromes
- -
- Nociceptive: Primarily based on peripheral processes in which mechanically, thermally and/or chemically induced afferents are generated (inflammation, degeneration and chronic relative ischaemia) [47];
- -
- Neuropathic: Traumatic or metabolic peripheral and or central nerve damage (grading system according to IASP) [48];
- -
8. CP Damage to the Brain Structure and Pathogenesis of Chronic Pain Syndromes
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CP | Cerebral palsy |
| fMRI | Functional magnetic resonance imaging |
| CNS | Central nervous system |
| SMS | Sensorimotor system |
References
- Slater, H.; Hush, J. Pain Terminology: Introduction of a Third Clinical Descriptor. Pain Terminol. 2018, 3, 7–8. [Google Scholar]
- Mineyko, A.; Nettel-Aguirre, A.; de Jesus, P.; Benseler, S.; Yusuf, K.; Narendran, A.; Kirton, A. Association of neonatal inflammatory markers and perinatal stroke subtypes. Neurology 2020, 95, e1163–e1173. [Google Scholar] [CrossRef] [PubMed]
- Goracke-Postle, C.J.; Burkitt, C.C.; Panoskaltsis-Mortari, A.; Ehrhardt, M.; Wilcox, G.L.; Graupman, P.; Partington, M.; Symons, F.J. Expression of and correlational patterns among neuroinflammatory, neuropeptide, and neuroendocrine molecules from cerebrospinal fluid in CP. BMC Neurol. 2021, 21, 384. [Google Scholar] [CrossRef] [PubMed]
- Lien, R. Neurocritical care of premature infants. Biomed. J. 2020, 43, 259–267. [Google Scholar] [CrossRef]
- Özek, E.; Kersin, S.G. Intraventricular hemorrhage in preterm babies. Turk Pediatri Ars. 2020, 55, 215–221. [Google Scholar] [CrossRef]
- Leifsdottir, K.; Jost, K.; Siljehav, V.; Thelin, E.P.; Lassarén, P.; Nilsson, P.; Haraldsson, Á.; Eksborg, S.; Herlenius, E. The cerebrospinal fluid proteome of preterm infants predicts neurodevelopmental outcome. Front. Pediatr. 2022, 10, 921444. [Google Scholar] [CrossRef]
- Kobesova, A.; Kolar, P. Developmental kinesiology: Three levels of motor control in the assessment and treatment of the motor system. J. Bodyw. Mov. Ther. 2014, 18, 23–33. [Google Scholar] [CrossRef]
- Božanić Urbančič, N.; Battelino, S.; Vozel, D. Appropriate Vestibular Stimulation in Children and Adolescents-A Prerequisite for Normal Cognitive, Motor Development and Bodily Homeostasis—A Review. Children 2023, 11, 2. [Google Scholar] [CrossRef]
- Maciak, M.; Koszela, K.; Beniuk, A.; Woldańska-Okońska, M. The Assessment of Postural-Motor, Coordination, and Reflex Functions in Children and Adolescents with a History of Premature Verticalization and Ontogeny Disorders in Their First Year of Life. Children 2024, 11, 1071. [Google Scholar] [CrossRef]
- Dieterich, M.; Brandt, T. Central vestibular networking for sensorimotor control, cognition, and emotion. Curr. Opin. Neurol. 2024, 37, 74–82. [Google Scholar] [CrossRef]
- Laube, W. Sensomotorik und Schmerz; Springer: Berlin/Heidelberg, Germany, 2020. [Google Scholar]
- Ostojic, K.; Paget, S.; Kyriagis, M.; Morrow, A. Acute and Chronic Pain in Children and Adolescents With CP: Prevalence, Interference, and Management. Arch. Phys. Med. Rehabil. 2020, 101, 213–219. [Google Scholar] [CrossRef]
- McKinnon, C.T.; Morgan, P.E.; Antolovich, G.C.; Clancy, C.H.; Fahey, M.C.; Harvey, A.R. Pain in children with dyskinetic and mixed dyskinetic/spastic CP. Dev. Med. Child Neurol. 2020, 62, 1294–1301. [Google Scholar] [CrossRef]
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour; World Health Organization: Geneva, Switzerland, 2020; ISBN 978-92-4-001513-5/978-92-4-001512-8. (electronic version). [Google Scholar]
- Pedersen, B.K. The Diseasome of Physical Inactivity and the role of myokines in muscle-fat cross talk. J. Physiol. 2009, 587, 5559–5568. [Google Scholar] [CrossRef] [PubMed]
- Shraim, M.A.; Massé-Alarie, H.; Farrell, M.J.; Cavaleri, R.; Loggia, M.L.; Hodges, P.W. Neuroinflammatory activation in sensory and motor regions of the cortex is related to sensorimotor function in individuals with low back pain maintained by nociplastic mechanisms: A preliminary proof-of-concept study. Eur. J. Pain 2024, 28, 1607–1626. [Google Scholar] [CrossRef] [PubMed]
- Safdar, A.; Tarnopolsky, M.A. Exosomes as Mediators of the Systemic Adaptations to Endurance Exercise. Cold Spring Harb. Perspect. Med. 2018, 8, a029827. [Google Scholar] [CrossRef] [PubMed]
- Fuller, O.K.; Whitham, M.; Mathivanan, S.; Febbraio, M.A. The Protective Effect of Exercise in Neurodegenerative Diseases: The Potential Role of Extracellular Vesicles. Cells 2020, 9, 2182. [Google Scholar] [CrossRef]
- Darragh, I.A.J.; O’Driscoll, L.; Egan, B. Exercise Training and Circulating Small Extracellular Vesicles: Appraisal of Methodological Approaches and Current Knowledge. Front. Physiol. 2021, 12, 738333. [Google Scholar] [CrossRef]
- Treede, R.D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. Chronic pain as a symptom or a disease: The IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain 2019, 160, 19–27. [Google Scholar] [CrossRef]
- Kosek, E.; Clauw, D.; Nijs, J.; Baron, R.; Gilron, I.; Harris, R.E.; Mico, J.A.; Rice, A.S.C.; Sterling, M. Chronic nociplastic pain affecting the musculoskeletal system: Clinical criteria and grading system. Pain 2021, 162, 2629–2634. [Google Scholar] [CrossRef]
- Nijs, J.; George, S.Z.; Clauw, D.J.; Fernández-de-Las-Peñas, C.; Kosek, E.; Ickmans, K.; Fernández-Carnero, J.; Polli, A.; Kapreli, E.; Huysmans, E.; et al. Central sensitisation in chronic pain conditions: Latest discoveries and their potential for precision medicine. Lancet Rheumatol. 2021, 3, e383–e392. [Google Scholar] [CrossRef]
- Clauw, D.J. From fibrositis to fibromyalgia to nociplastic pain: How rheumatology helped get us here and where do we go from here? Ann. Rheum. Dis. 2024, 83, 1421–1427. [Google Scholar] [CrossRef] [PubMed]
- Fang, W.; Liu, Y.; Wang, L. Multisensory Integration in Body Representation. Adv. Exp. Med. Biol. 2024, 1437, 77–89. [Google Scholar] [CrossRef] [PubMed]
- Shimada, S. Multisensory and Sensorimotor Integration in the Embodied Self: Relationship between Self-Body Recognition and the Mirror Neuron System. Sensors 2022, 22, 5059. [Google Scholar] [CrossRef]
- Bremner, A.J. Developing body representations in early life: Combining somatosensation and vision to perceive the interface between the body and the world. Dev. Med. Child Neurol. 2016, 58 (Suppl. 4), 12–16. [Google Scholar] [CrossRef]
- Gauduel, T.; Blondet, C.; Gonzalez-Monge, S.; Bonaiuto, J.; Gomez, A. Alteration of body representation in typical and atypical motor development. Dev. Sci. 2024, 27, e13455. [Google Scholar] [CrossRef] [PubMed]
- Melillo, R.; Leisman, G.; Machado, C.; Machado-Ferrer, Y.; Chinchilla-Acosta, M.; Kamgang, S.; Melillo, T.; Carmeli, E. Retained Primitive Reflexes and Potential for Intervention in Autistic Spectrum Disorders. Front. Neurol. 2022, 13, 922322. [Google Scholar] [CrossRef]
- Patel, D.R.; Bovid, K.M.; Rausch, R.; Ergun-Longmire, B.; Goetting, M.; Merrick, J. CP in children: A clinical practice review. Curr. Probl. Pediatr. Adolesc. Health Care 2024, 54, 101673. [Google Scholar] [CrossRef]
- Krägeloh-Mann, I.; Horber, V. The role of magnetic resonance imaging in elucidating the pathogenesis of CP: A systematic review. Dev. Med. Child Neurol. 2007, 49, 144–151. [Google Scholar] [CrossRef]
- Jacobs, N.P.T.; Pouwels, P.J.W.; van der Krogt, M.M.; Meyns, P.; Zhu, K.; Nelissen, L.; Schoonmade, L.J.; Buizer, A.I.; van de Pol, L.A. Brain structural and functional connectivity and network organization in CP: A scoping review. Dev. Med. Child Neurol. 2023, 65, 1157–1173. [Google Scholar] [CrossRef]
- Laube, W. Bewegungsmangel: Dekonditionierung, Krankheit, Schmerzen, Alter; Springer: Berlin/Heidelberg, Germany, 2023. [Google Scholar]
- Laube, W. (Hrsg): Sensomotorisches System; Thieme: Stuttgart, Germany; New York, NY, USA, 2009. [Google Scholar]
- Mailleux, L.; Simon-Martinez, C.; Radwan, A.; Blommaert, J.; Gooijers, J.; Wenderoth, N.; Klingels, K.; Ortibus, E.; Sunaert, S.; Feys, H. White matter characteristics of motor, sensory and interhemispheric tracts underlying impaired upper limb function in children with unilateral CP. Brain Struct. Funct. 2020, 225, 1495–1509. [Google Scholar] [CrossRef]
- Holmström, L.; Vollmer, B.; Tedroff, K.; Islam, M.; Persson, J.K.; Kits, A.; Forssberg, H.; Eliasson, A.C. Hand function in relation to brain lesions and corticomotor-projection pattern in children with unilateral CP. Dev. Med. Child Neurol. 2010, 52, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Scheck, S.M.; Pannek, K.; Fiori, S.; Boyd, R.N.; Rose, S.E. Quantitative comparison of cortical and deep grey matter in pathological subtypes of unilateral CP. Dev. Med. Child Neurol. 2014, 56, 968–975. [Google Scholar] [CrossRef]
- Scheck, S.M.; Boyd, R.N.; Rose, S.E. New insights into the pathology of white matter tracts in CP from diffusion magnetic resonance imaging: A systematic review. Dev. Med. Child Neurol. 2012, 54, 684–696. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.; Pae, C.; Lee, J.D.; Park, E.S.; Cho, S.R.; Um, M.H.; Lee, S.K.; Oh, M.K.; Park, H.J. Analysis of structure-function network decoupling in the brain systems of spastic diplegic CP. Hum. Brain Mapp. 2017, 38, 5292–5306. [Google Scholar] [CrossRef]
- Mailleux, L.; Franki, I.; Emsell, L.; Peedima, M.L.; Fehrenbach, A.; Feys, H.; Ortibus, E. The relationship between neuroimaging and motor outcome in children with CP: A systematic review-Part B diffusion imaging and tractography. Res. Dev. Disabil. 2020, 97, 103569. [Google Scholar] [CrossRef]
- Tsao, H.; Pannek, K.; Boyd, R.N.; Rose, S.E. Changes in the integrity of thalamocortical connections are associated with sensorimotor deficits in children with congenital hemiplegia. Brain Struct. Funct. 2015, 220, 307–318. [Google Scholar] [CrossRef]
- Ballester-Plané, J.; Schmidt, R.; Laporta-Hoyos, O.; Junqué, C.; Vázquez, É.; Delgado, I.; Zubiaurre-Elorza, L.; Macaya, A.; Póo, P.; Toro, E.; et al. Whole-brain structural connectivity in dyskinetic CP and its association with motor and cognitive function. Hum. Brain Mapp. 2017, 38, 4594–4612. [Google Scholar] [CrossRef] [PubMed]
- Caldú, X.; Reid, L.B.; Pannek, K.; Fripp, J.; Ballester-Plané, J.; Leiva, D.; Boyd, R.N.; Pueyo, R.; Laporta-Hoyos, O. Tractography of sensorimotor pathways in dyskinetic CP: Association with motor function. Ann. Clin. Transl. Neurol. 2024, 11, 2609–2622. [Google Scholar] [CrossRef]
- Hebert, J.R.; Filley, C.M. Multisensory integration and white matter pathology: Contributions to cognitive dysfunction. Front. Neurol. 2022, 13, 1051538. [Google Scholar] [CrossRef]
- Laporta-Hoyos, O.; Pannek, K.; Ballester-Plané, J.; Reid, L.B.; Vázquez, É.; Delgado, I.; Zubiaurre-Elorza, L.; Macaya, A.; Póo, P.; Meléndez-Plumed, M.; et al. White matter integrity in dyskinetic CP: Relationship with intelligence quotient and executive function. Neuroimage Clin. 2017, 12, 789–800. [Google Scholar] [CrossRef]
- Saini, A.G.; Sankhyan, N.; Malhi, P.; Ahuja, C.; Khandelwal, N.; Singhi, P. Dyskinetic CP in Children: Clinical Perspectives on Common Comorbidities and Health-Related Quality of Life. J. Autism Dev. Disord. 2024. [Google Scholar] [CrossRef]
- Ding, J.Y.; Cleary, S.L.; Morgan, P.E. Health literacy (Gesundheitskompetenz) in adolescents and young adults with CP: A mixed methods systematic review. Disabil. Rehabil. 2024, 46, 5717–5729. [Google Scholar] [CrossRef]
- IASP. Terminology International Association for the Study of Pain. Available online: https://www.iasp-pain.org/resources/terminology/ (accessed on 8 February 2025).
- Finnerup, N.B.; Haroutounian, S.; Kamerman, P.; Baron, R.; Bennett, D.L.H.; Bouhassira, D.; Cruccu, G.; Freeman, R.; Hansson, P.; Nurmikko, T.; et al. Neuropathic pain: An updated grading system for research and clinical practice. Pain 2016, 157, 1599–1606. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.; Quintner, J.; Weisman, A. “Nociplastic Pain”: A Challenge to Nosology and to Nociception. J. Pain 2023, 12, 2131–2139. [Google Scholar] [CrossRef]
- Nijs, J.; Kosek, E.; Chiarotto, A.; Cook, C.; Danneels, L.A.; Fernández-de-Las-Peñas, C.; Hodges, P.W.; Koes, B.; Louw, A.; Ostelo, R.; et al. Nociceptive, neuropathic, or nociplastic low back pain? The low back pain phenotyping (BACPAP) consortium’s international and multidisciplinary consensus recommendations. Lancet Rheumatol. 2024, 6, e178–e188. [Google Scholar] [CrossRef] [PubMed]
- Peterson, M.D.; Haapala, H.; Kamdar, N.; Lin, P.; Hurvitz, E.A. Pain phenotypes among adults living with CP and spina bifida. Pain 2021, 162, 2532–2538. [Google Scholar] [CrossRef]
- Heinen, F.; Bonfert, M.; Kaňovský, P.; Schroeder, A.S.; Chambers, H.G.; Dabrowski, E.; Geister, T.L.; Hanschmann, A.; Althaus, M.; Banach, M.; et al. Spasticity-related pain in children/adolescents with CP. Part 1: Prevalence and clinical characteristics from a pooled analysis. J. Pediatr. Rehabil. Med. 2022, 15, 129–143. [Google Scholar] [CrossRef] [PubMed]
- Peterson, M.D.; Haapala, H.J.; Kratz, A. Pain Phenotypes in Adults Living With CP. Neurol. Clin. Pract. 2021, 11, e848–e855. [Google Scholar] [CrossRef]
- Jarlman, E.; Hägglund, G.; Alriksson-Schmidt, A.I. Foot and lower leg pain in children and adults with CP: A population-based register study on 5,122 individuals. BMC Musculoskelet. Disord. 2024, 25, 391. [Google Scholar] [CrossRef]
- Yoo, Y.M.; Kim, K.H. Current understanding of nociplastic pain. Korean J. Pain 2024, 37, 107–118. [Google Scholar] [CrossRef]
- Kaplan, C.M.; Kelleher, E.; Irani, A.; Schrepf, A.; Clauw, D.J.; Harte, S.E. Deciphering nociplastic pain: Clinical features, risk factors and potential mechanisms. Nat. Rev. Neurol. 2024, 20, 347–363. [Google Scholar] [CrossRef]
- Bułdyś, K.; Górnicki, T.; Kałka, D.; Szuster, E.; Biernikiewicz, M.; Markuszewski, L.; Sobieszczańska, M. What Do We Know about Nociplastic Pain? Healthcare 2023, 11, 1794. [Google Scholar] [CrossRef]
- Wirth, B.; Schweinhardt, P. Personalized assessment and management of non-specific low back pain. Eur. J. Pain 2024, 28, 181–198. [Google Scholar] [CrossRef]
- Handsfield, G.G.; Williams, S.; Khuu, S.; Lichtwark, G.; Stott, N.S. Muscle architecture, growth, and biological remodelling in CP: A narrative review. BMC Musculoskelet. Disord. 2022, 23, 233. [Google Scholar] [CrossRef] [PubMed]
- Schless, S.H.; Cenni, F.; Bar-On, L.; Hanssen, B.; Goudriaan, M.; Papageorgiou, E.; Aertbeliën, E.; Molenaers, G.; Desloovere, K. Combining muscle morphology and neuromotor symptoms to explain abnormal gait at the ankle joint level in CP. Gait Posture 2019, 68, 531–537. [Google Scholar] [CrossRef] [PubMed]
- Hanssen, B.; Peeters, N.; Vandekerckhove, I.; De Beukelaer, N.; Bar-On, L.; Molenaers, G.; Van Campenhout, A.; Degelaen, M.; Van den Broeck, C.; Calders, P.; et al. The Contribution of Decreased Muscle Size to Muscle Weakness in Children with Spastic CP. Front. Neurol. 2021, 12, 692582. [Google Scholar] [CrossRef] [PubMed]
- Laube, W. Die Muskulatur—Das „signalstoffgestützte periphere Zentrum“ adaptiver Wirkungen. Man. Med. 2022, 60, 104–106. [Google Scholar] [CrossRef]
- Haapala, H.J.; Schmidt, M.; Lin, P.; Kamdar, N.; Mahmoudi, E.; Peterson, M.D. Musculoskeletal Morbidity Among Adults Living With Spina Bifida and CP. Top. Spinal Cord Inj. Rehabil. 2022, 28, 73–84. [Google Scholar] [CrossRef] [PubMed]
- Harvey, A.; Smith, N.; Smith, M.; Ostojic, K.; Berryman, C. Chronic pain in children and young people with CP: A narrative review of challenges, advances, and future directions. BMC Med. 2024, 22, 238. [Google Scholar] [CrossRef]
- Carozza, L.; Anderson-Mackay, E.; Blackmore, A.M.; Kirkman, H.A.; Ou, J.; Smith, N.; Love, S. Chronic Pain in Young People With CP: Activity Limitations and Coping Strategies. Pediatr. Phys. Ther. 2022, 34, 489–495. [Google Scholar] [CrossRef]
- Lee, J.; Protsenko, E.; Lazaridou, A.; Franceschelli, O.; Ellingsen, D.M.; Mawla, I.; Isenburg, K.; Berry, M.P.; Galenkamp, L.; Loggia, M.L.; et al. Encoding of Self-Referential Pain Catastrophizing in the Posterior Cingulate Cortex in Fibromyalgia. Arthritis Rheumatol. 2018, 70, 1308–1318. [Google Scholar] [CrossRef]
- Blackman, J.A.; Svensson, C.I.; Marchand, S. Pathophysiology of chronic pain in CP: Implications for pharmacological treatment and research. Dev. Med. Child Neurol. 2018, 60, 861–865. [Google Scholar] [CrossRef] [PubMed]
- Malfliet, A.; Coppieters, I.; Van Wilgen, P.; Kregel, J.; De Pauw, R.; Dolphens, M.; Ickmans, K. Brain changes associated with cognitive and emotional factors in chronic pain: A systematic review. Eur. J. Pain 2017, 21, 769–786. [Google Scholar] [CrossRef] [PubMed]
- Wirtz, M.A. (Hrsg.): Dorsch—Lexikon der Pscyhologie; Hofgrebe AG: Bern, Switzerland, 2022. [Google Scholar]
- Rose, J.; McGill, K.C. The motor-unit in CP. Dev. Med. Child Neurol. 1998, 40, 270–277. [Google Scholar] [CrossRef]
- Noble, J.J.; Gough, M.; Shortland, A.P. Selective motor control and gross motor function in bilateral spastic CP. Dev. Med. Child Neurol. 2019, 61, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Aisen, M.L.; Kerkovich, D.; Mast, J.; Mulroy, S.; Wren, T.A.; Kay, R.; Rethlefsen, S.A. CP: Clinical care and neurological rehabilitation. Lancet Neurol. 2011, 10, 844–852. [Google Scholar] [CrossRef]
- Vitrikas, K.; Dalton, H.; Breish, D. CP: An Overview. Am. Fam. Physician 2020, 101, 213–220. [Google Scholar]
- Devesa, J.; Casteleiro, N.; Rodicio, C.; López, N.; Reimunde, P. Growth hormone deficiency and CP. Ther. Clin. Risk Manag. 2010, 6, 413–418. [Google Scholar] [CrossRef]
- Hegazi, M.A.; Soliman, O.E.; Hasaneen, B.M.; El-Arman, M.; El-Galel, N.A.; El-Deek, B.S. Growth hormone/insulin-like growth factor-1 axis: A possible non-nutritional factor for growth retardation in children with CP. J. Pediatr. 2012, 88, 267–274. [Google Scholar] [CrossRef]
- Hoon, A.H.; Stashinko, E.E.; Nagae, L.M.; Lin, D.D.M.; Keller, J.; Bastian, A.; Campell, M.L.; Levey, E.; Mori, S.; Johnston, M.V. Sensory and motor deficits in children with CP born preterm correlate with diffusion tenso imaging abnormalities in thalamocortical pathways. Dev. Med. Child Neurol. 2009, 51, 697–704. [Google Scholar] [CrossRef]
- Fridèn, J.; Lieber, R.L. Spastic muscle cells are shorter and stiffer than normal cells. Muscle Nerve 2003, 27, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Bax, M.; Tydeman, C.; Flodmark, O. Clinical and MRI correlates for CP: The European CP Study. JAMA 2006, 296, 1602–1608. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laube, W.; Sengoelge, M. Cerebral Palsy Link to Sensorimotor System, Cognition, Emotion and Nociplastic Pain. Children 2025, 12, 702. https://doi.org/10.3390/children12060702
Laube W, Sengoelge M. Cerebral Palsy Link to Sensorimotor System, Cognition, Emotion and Nociplastic Pain. Children. 2025; 12(6):702. https://doi.org/10.3390/children12060702
Chicago/Turabian StyleLaube, Wolfgang, and Mathilde Sengoelge. 2025. "Cerebral Palsy Link to Sensorimotor System, Cognition, Emotion and Nociplastic Pain" Children 12, no. 6: 702. https://doi.org/10.3390/children12060702
APA StyleLaube, W., & Sengoelge, M. (2025). Cerebral Palsy Link to Sensorimotor System, Cognition, Emotion and Nociplastic Pain. Children, 12(6), 702. https://doi.org/10.3390/children12060702