
Exploring Conscious Sedation in Pediatric Oral Surgery: A Non-Randomized Clinical Trial on Safety and Efficacy



Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Viinikangas, A.; Lahti, S.; Yuan, S.; Pietilä, I.; Freeman, R.; Humphris, G. Evaluating a single dental anxiety question in Finnish adults. Acta Odontol. Scand. 2007, 65, 236–240. [Google Scholar] [CrossRef] [PubMed]
- Al-Zahrani, A.M.; Wyne, A.H.; Sheta, S.A. Comparison of Oral Midazolam with a Combination of Oral Midazolam and Nitrous Oxide-Oxygen Inhalation in the Effectiveness of Dental Sedation for Young Children. J. Indian. Soc. Pedod. Prev. Dent. 2009, 27, 9–16. [Google Scholar] [PubMed]
- Appukuttan, D.P. Strategies to manage patients with dental anxiety and dental phobia: Literature review. Clin. Cosmet. Investig. Dent. 2016, 8, 35–50. [Google Scholar] [CrossRef] [PubMed]
- Primozic, J.; Canova, F.F.; Rizzo, F.A.; Marzo, G.; Quinzi, V. Diagnostic ability of the primary second molar crown-to-root length ratio and the corresponding underlying premolar position in estimating future expander anchoring teeth exfoliation. Orthod. Craniofac Res. 2021, 24, 561–567. [Google Scholar] [CrossRef]
- Singh, J.; Hegde, S.; Rao, D.; Panwar, S.; Pal, S.; Rathore, N. Assessment of pain in paediatric dental patients during administration of local anesthesia with and without the use of audiovisual distraction. Dent. Res. J. 2023, 20, 7. [Google Scholar] [CrossRef]
- Sharma, M.; Sahu, A.K.; Kaila, P.; Hassan, A.A.H.A.; Mansy, M.; Thakur, R.; Homeida, H.E. Retrospective Evaluation of Sedation Techniques for Tooth Extraction in Paediatric Patients. J. Pharm. Bioallied Sci. 2024, 16 (Suppl. S4), S3150–S3152. [Google Scholar] [CrossRef]
- D‘ettorre, G.; Farronato, M.; Candida, E.; Quinzi, V.; Grippaudo, C. A comparison between stereophotogrammetry and smartphone structured light technology for three-dimensional face scanning. Angle Orthod. 2022, 92, 358–363. [Google Scholar] [CrossRef]
- Nelson, T.; Nelson, G. The role of sedation in contemporary paediatric dentistry. Dent. Clin. North. Am. 2013, 57, 145–161. [Google Scholar] [CrossRef]
- Corah, N.L.; O’Shea, R.M. Patient and Dentist selection in general practice. In The President’s Conference on the Dentist-Patient Relationships and the Management of Fear, Anxiety and Pain; Moretti, R., Ayer, W.A., Eds.; American Dental Association: Chicago, IL, USA, 1983. [Google Scholar]
- Klingberg, G.; Broberg, A.G. Dental fear/anxiety and dental behavior management problems in children and adolescents: A review of prevalence and concomitant psychological factors. Int. J. Paediatr. Dent. 2007, 17, 391–406. [Google Scholar] [CrossRef]
- Asl, A.N.; Shokravi, M.; Jamali, Z.; Shirazi, S. Barriers and drawbacks of the assessment of dental fear, dental anxiety and dental phobia in children: A critical literature review. J. Clin. Pediatr. Dent. 2017, 41, 399–423. [Google Scholar] [CrossRef]
- Kothari, S.; Gurunathan, D. Factors influencing anxiety levels in children undergoing dental treatment in an undergraduate clinic. J. Fam. Med. Prim. Care 2019, 8, 2036–2041. [Google Scholar]
- Cohen, S.M.; Fiske, J.; Newton, J.T. The impact of dental anxiety on daily living. Br. Dent. J. 2000, 189, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Yuwannisa, M.; Runkat, J.; Indrivanti, R. Dental anxiety level of children patient during dental treatment using CFSS-DS questionnaire. Padjadjaran J. Dent. 2013, 25, 1–9. [Google Scholar] [CrossRef]
- Cianetti, S.; Lombardo, G.; Lupatelli, E.; Pagano, S.; Abraha, I.; Montedori, A.; Caruso, S.; Gatto, R.; de Giorgio, S.; Salvato, R. Dental fear/anxiety among children and adolescents. A systematic review. Eur. J. Paediatr. Dent. 2017, 18, 121–130. [Google Scholar]
- Porritt, J.; Buchanan, H.; Hall, M.; Gilchrist, F.; Marshman, Z. Assessing children’s dental anxiety: A systematic review of current measures. Community Dent. Oral Epidemiol. 2013, 41, 130–142. [Google Scholar] [CrossRef]
- Attri, J.P.; Sharan, R.; Makkar, V.; Gupta, K.K.; Khetarpal, R.; Kataria, A.P. Conscious sedation: Emerging trends in pediatric dentistry. Anesth. Essays Res. 2017, 11, 277–281. [Google Scholar] [CrossRef]
- Lanza, V.; Mercadante, S.; Pignataro, A. Effects of halothane, enflurane, and nitrous oxide on oxyhemoglobin affinity. Anesthesiology 1988, 68, 591–594. [Google Scholar] [CrossRef]
- Field, L.M.; Dorrance, D.E.; Krzeminska, E.K.; Barsoum, L.Z. Effect of nitrous oxide on cerebral blood flow in normal humans. Br. J. Anaesth. 1993, 70, 154–159. [Google Scholar] [CrossRef]
- Cassetta, M.; Guarnieri, R.; Mezio, M.; Altieri, F.; Brandetti, G.; Padalino, G.; Di Giorgio, R.; Barbato, E. Comparison of profile macro-esthetic perception among orthodontists, dentistry students, orthodontic patients and surgical orthodontic patients. J. Clin. Exp. Dent. 2020, 12, e1109–e1116. [Google Scholar] [CrossRef]
- Mistry, R.B.; Nahata, M.C. Ketamine for conscious sedation in pediatric emergency care. Pharmacotherapy 2005, 25, 1104–1111. [Google Scholar] [CrossRef]
- Salerno, C.; Cirio, S.; Zambon, G.; D’avola, V.; Parcianello, R.G.; Maspero, C.; Campus, G.; Cagetti, M.G. Conscious sedation for dental treatments in subjects with intellectual disability: A systematic review and meta-analysis. Int. J. Environ. Res. Public. Health 2023, 20, 1779. [Google Scholar] [CrossRef] [PubMed]
- Zommick, J.; Leveillee, R.; Zabbo, A.; Colasanto, L.; Barrette, D. Comparison of general anesthesia and intravenous sedation-analgesia for SWL. J. Endourol. 1996, 10, 489–491. [Google Scholar] [CrossRef] [PubMed]
- Saccomanno, S.; Mummolo, S.; Laganà, D.; Greco, F.; Fiasca, F.; Marzo, G.; Quinzi, V. The Digital Diagnostic Approach to Stafne’s Bone Cavity [SBC]: From a Review of the Literature to the Description of a Clinical Case. Open Dent. J. 2021, 15, 1. [Google Scholar] [CrossRef]
- Agarwal, M.; Das, U. Dental anxiety prediction using Venham Picture test: A preliminary cross-sectional study. J. Indian. Soc. Pedod. Prev. Dent. 2013, 31, 22–24. [Google Scholar] [CrossRef]
- Hosey, M.T.; Blinkhorn, A.S. An evaluation of four methods of assessing the behaviour of anxious child dental patients. Int. J. Paediatr. Dent. 1995, 5, 87–95. [Google Scholar] [CrossRef]
- Vasakova, J.; Duskova, J.; Lunackova, J.; Drapalova, K.; Zuzankova, L.; Starka, L.; Duskova, M.; Broukal, Z. Midazolam and its effect on vital signs and behavior in children under conscious sedation in dentistry. Physiol. Res. 2020, 69 (Suppl. S2), S305–S314. [Google Scholar] [CrossRef]
- Wang, Z.; Ma, J.; Dong, B.; Song, Y.; Hu, P.J.; Zhang, B. Comparison of blood pressure levels among four age groups of Chinese children matched by height. J. Hum. Hypertens. 2012, 26, 437–442. [Google Scholar] [CrossRef]
- Behrman, R.E.; Kliegman, R.; Jenson, H.B. Nelson Textbook of Pediatrics; Saunders: Philadelphia, PA, USA, 2004; pp. 278, 1482–1483, 1487. [Google Scholar]
- Maspero, C.; Cenzato, N.; Inchingolo, F.; Cagetti, M.G.; Isola, G.; Sozzi, D.; Del Fabbro, M.; Tartaglia, G.M. The Maxilla-Mandibular Discrepancies through Soft-Tissue References: Reliability and Validation of the Anteroposterior Measurement. Children 2023, 10, 459. [Google Scholar] [CrossRef]
- Cazzolla, A.P.; Lovero, R.; Muzio, L.L.; Testa, N.F.; Schirinzi, A.; Palmieri, G.; Pozzessere, P.; Procacci, V.; Di Comite, M.; Ciavarella, D.; et al. Taste and Smell Disorders in COVID-19 Patients: Role of Interleukin-6. ACS Chem. Neurosci. 2020, 11, 2774–2781. [Google Scholar] [CrossRef]
- Mourad, M.S.; Santamaria, R.M.; Splieth, C.H.; Schwahn, C.; Midani, R.; Schmoeckel, J. Impact of operators’ experience and patients’ age on the success of nitrous oxide sedation for dental treatment in children. Eur. J. Paediatr. Dent. 2022, 23, 183–188. [Google Scholar]
- Cenzato, N.; Crispino, R.; Galbiati, G.; Giannini, L.; Bolognesi, L.; Lanteri, V.; Maspero, C. Premature loss of primary molars in children: Space recovery through molar distalisation. A literature review. Eur. J. Paediatr. Dent. 2024, 25, 1. [Google Scholar]
- Lourenço-Matharu, L.; Roberts, G.J. Oral sedation for dental treatment in young children in a hospital setting. Br. Dent. J. 2010, 209, E12. [Google Scholar] [CrossRef] [PubMed]
- Lenahan, M.; Wells, M.; Scarbecz, M. A Retrospective Study of 248 Paediatric Oral Sedations Utilizing the Combination of Meperidine and Hydroxyzine for Dental Treatment. J. Clin. Paediatr. Dent. 2015, 39, 481–487. [Google Scholar] [CrossRef] [PubMed]
- Wan, K.; Jing, Q.; Zhao, J.Z. Evaluation of oral midazolam as conscious sedation for pediatric patients in oral restoration. Chin. Med. Sci. J. 2006, 21, 163–166. [Google Scholar]
- Antunes, D.E.; Viana, K.A.; Costa, P.S.; Costa, L.R. Moderate sedation helps improve future behavior in paediatric dental patients—A prospective study. Braz. Oral. Res. 2016, 30, e107. [Google Scholar] [CrossRef]
- Ashley, P.F.; Anand, P.; Andersson, K. Best Clinical Practice Guidance for Conscious Sedation of Children Undergoing Dental Treatment: An EAPD Policy Document. Eur. Arch. Paediatr. Dent. 2021, 22, 989–1002. [Google Scholar] [CrossRef]
- Venham, L.L.; Gaulin-Kremer, E. A self-report measure of situational anxiety for young children. Pediatr. Dent. 1979, 1, 91–96. [Google Scholar]
- Tortora, G.; Farronato, M.; Gaffuri, F.; Carloni, P.; Occhipinti, C.; Tucci, M.; Cenzato, N.; Maspero, C. Survey of Oral Hygiene Habits and Knowledge among School Children: A cross-sectional study from Italy. Eur. J. Paediatr. Dent. 2023, 24, 194. [Google Scholar]
- Paglia, L. Oral prevention starts with the mother. Eur. J. Paediatr. Dent. 2019, 20, 173. [Google Scholar]
- Esposito, L.; Poletti, L.; Maspero, C.; Porro, A.; Pietrogrande, M.C.; Pavesi, P.; Dellepiane, R.M.; Farronato, G. Hyper-IgE syndrome: Dental implications. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. 2012, 114, 147–153. [Google Scholar] [CrossRef]
- Farronato, G.; Maspero, C.; Farronato, D. Orthodontic movement of a dilacerated maxillary incisor in mixed dentition treatment. Dent. Traumatol. 2009, 25, 451–456. [Google Scholar] [CrossRef] [PubMed]
- Akinmoladun, J.A.; Akinyemi, O.O.; Olanlokun, T.M. Assessing the Safety of Ketamine as a Procedural Sedative in Paediatric Dental Patients: A Randomized Clinical Trial. Niger. J. Clin. Pract. 2024, 27, 123–129. [Google Scholar]
- Maspero, C.; Fama, A.; Cavagnetto, D.; Abate, A.; Farronato, M. Treatment of dental dilacerations. J. Biol. Regul. Homeost. Agents 2019, 33, 1623–1627. [Google Scholar] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | N | % |
|---|---|---|
| Total | 43 | 100 |
| Age, mean [DS] | 9.4 [2.2] | |
| Gender | ||
| Male | 20 | 47 |
| Female | 23 | 53 |
| Type of sedation | ||
| Basic | 8 | 19 |
| Advanced | 35 | 81 |
| Benzodiazepine dose, mean [DS] | 10.8 [4.5] | |
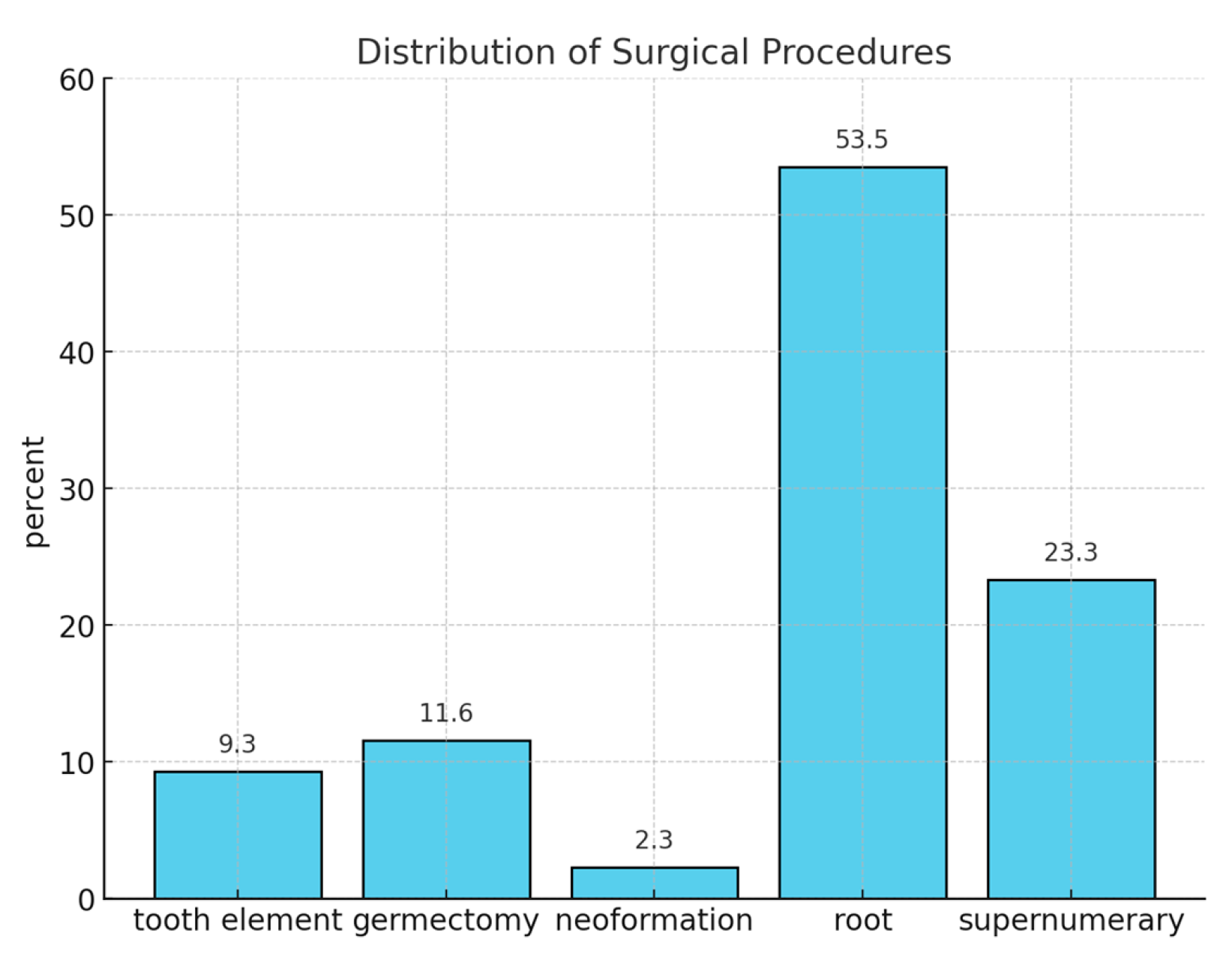
| Type of surgery | ||
| Root residual | 23 | 53 |
| Supernumerary teeth | 10 | 23 |
| Germectomy | 5 | 12 |
| Tooth extraction | 4 | 9 |
| Lesion removal | 1 | 2 |
| Variable | N [%] | Pre-Sedation Mean [DS] | Post-Sedation Mean [DS] | p-Value a |
|---|---|---|---|---|
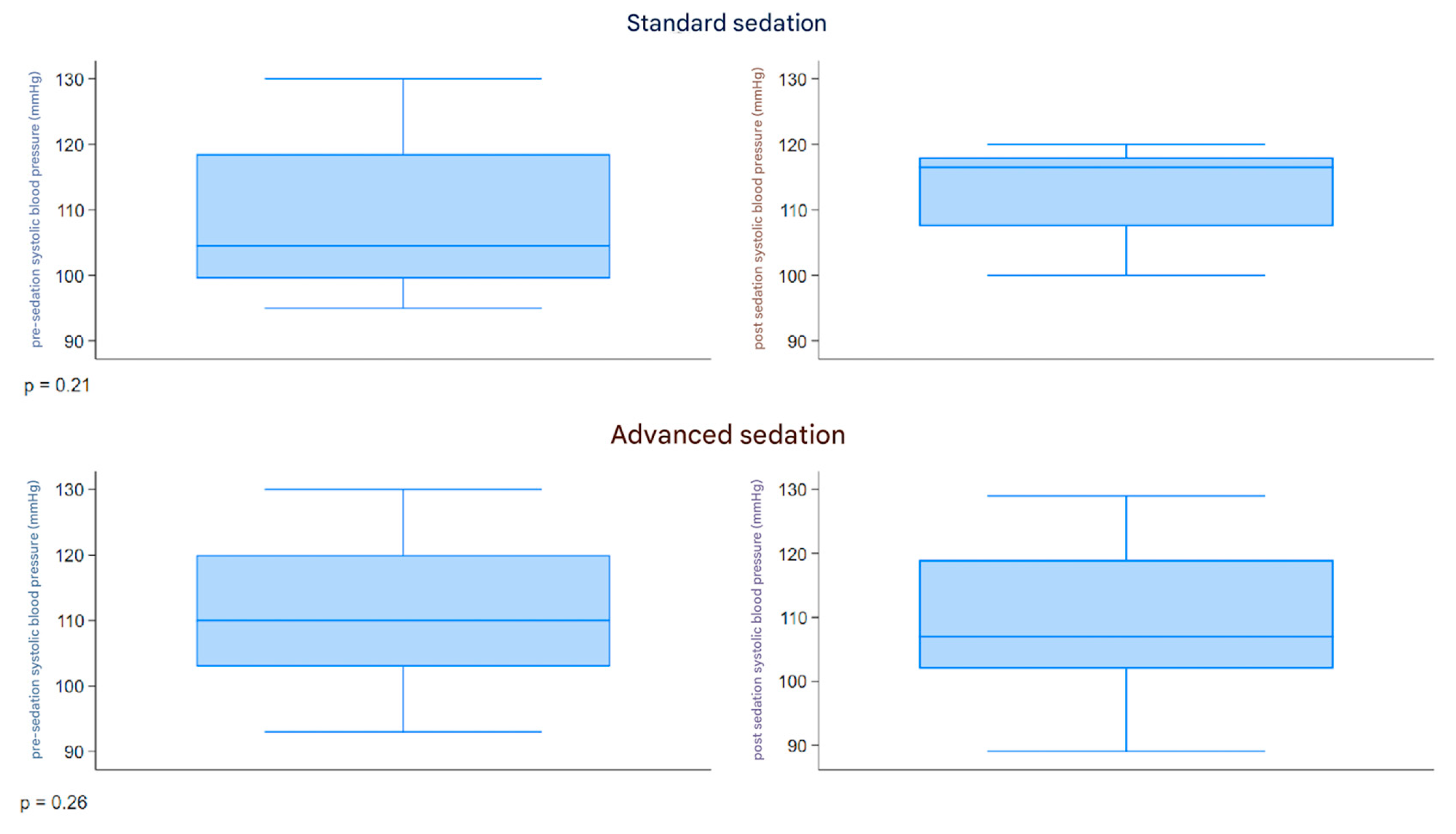
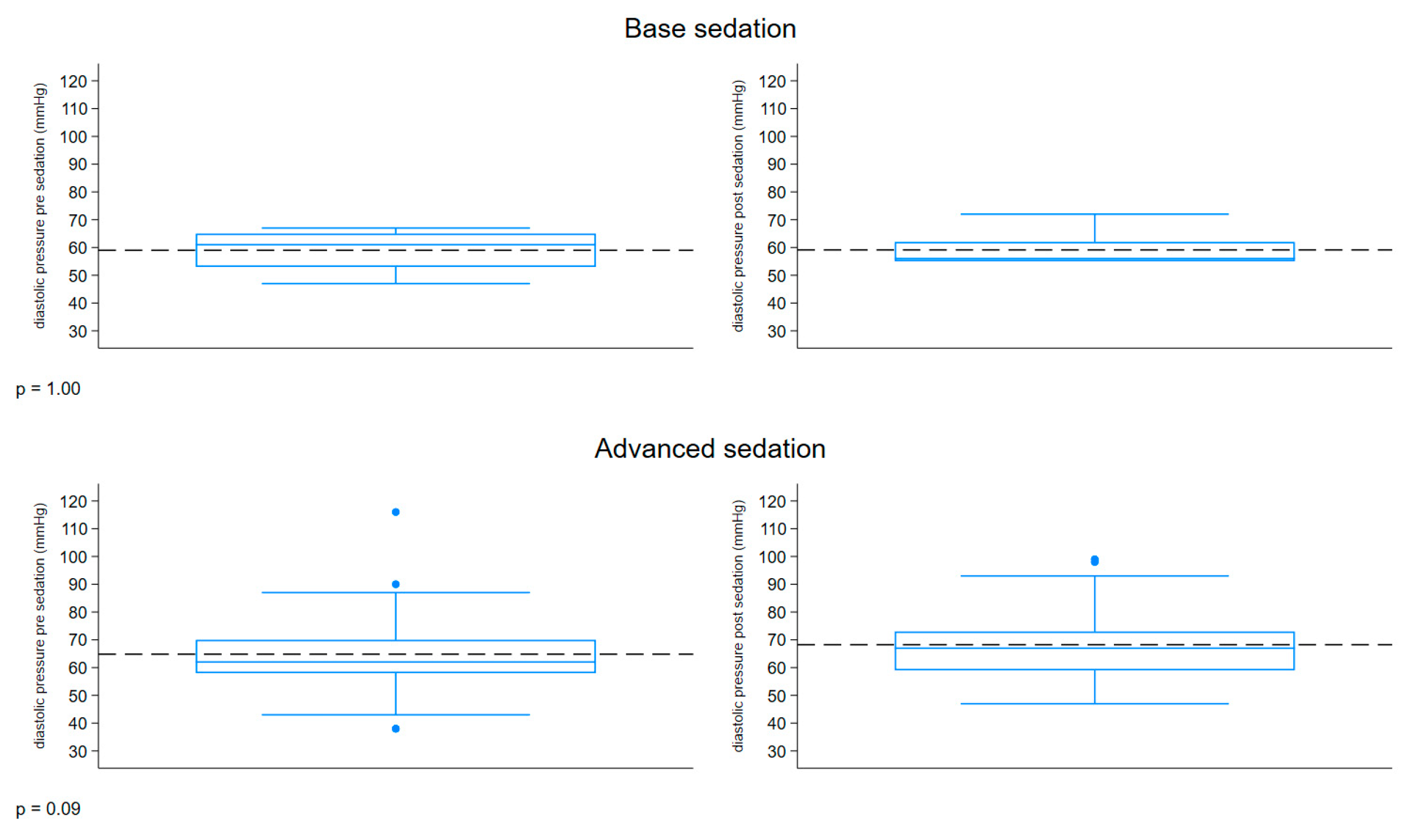
| Base Sedation | 8 (9) | |||
| Clinical Parameter | ||||
| Systolic pressure [mmHg] | 108.8 [12.2] | 113 [7.2] | 0.21 | |
| Diastolic pressure [mmHg] | 59 [7.4] | 59.1 [6.1] | 1.00 | |
| Heart rate [bpm] | 87 [10.6] | 86.1 [11.1] | 0.72 | |
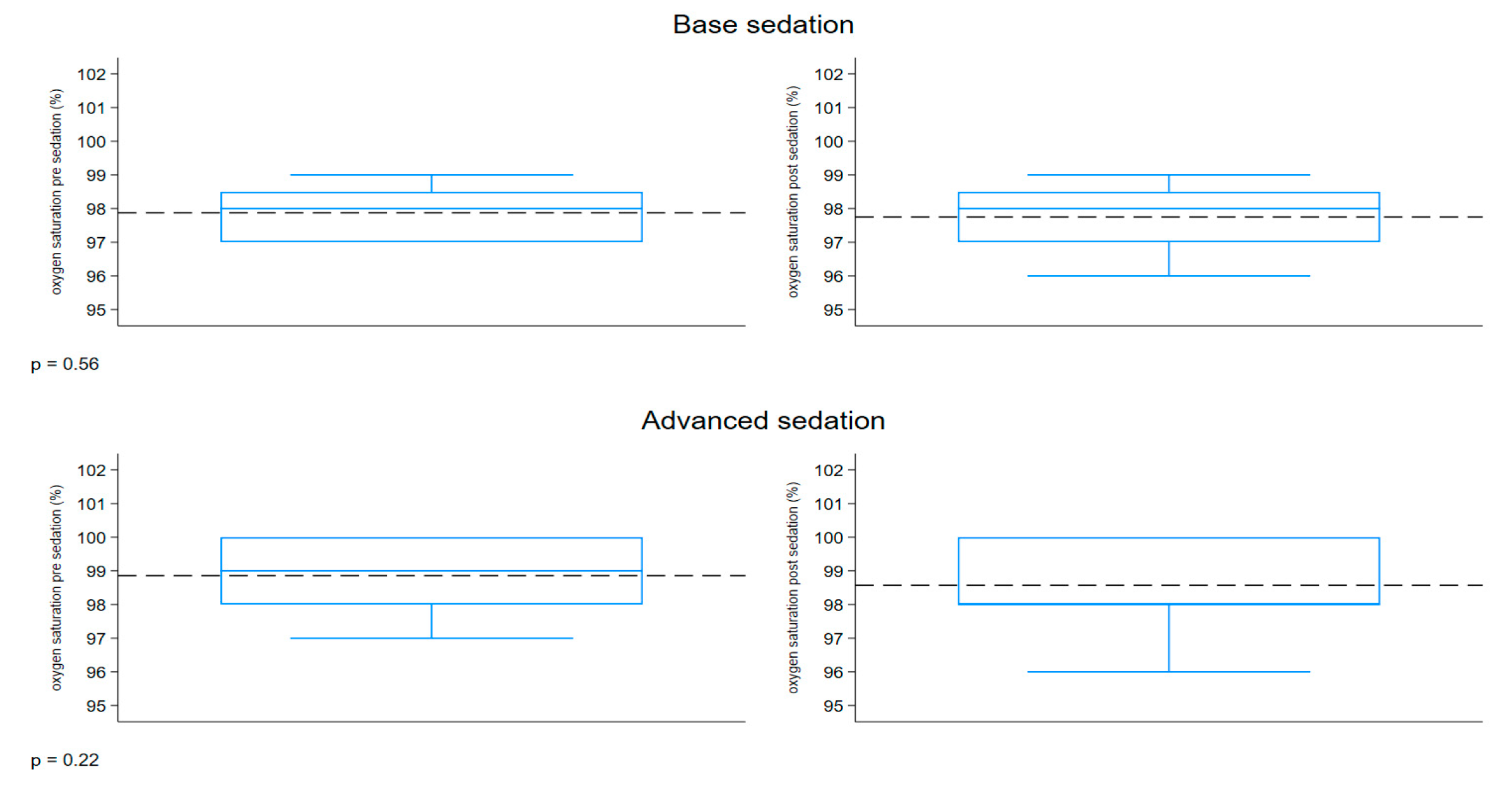
| Oxygen saturation [%] | 97.9 [0.8] | 97.8 [1.0] | 0.56 | |
| Venham score | 6.7 [0.5] | 4.4 [1.0] | 0.01 | |
| Advanced Sedation | 35 (81) | |||
| Clinical Parameter | ||||
| Systolic pressure [mmHg] | 111.8 [10.9] | 108.7 [10.7] | 0.26 | |
| Diastolic pressure [mmHg] | 64.8 [14.5] | 68.2 [12.4] | 0.09 | |
| Heart rate [bpm] | 95.6 [18.9] | 97.8 [11.2] | 0.47 | |
| Oxygen saturation [%] | 98.9 [1.00] | 98.6 [1.1] | 0.22 | |
| Venham score | 6.9 [0.3] | 4.9 [0.3] | <0.01 |
| Variable | N [%] | Advanced Mean [DS] | N [%] | Base Mean [DS] | p-Value a |
|---|---|---|---|---|---|
| Pre-sedation | 35 [81] | 8 [19] | |||
| Clinical Parameter | |||||
| Systolic pressure [mmHg] | 111.8 [10.9] | 108.8 [12.2] | 0.43 | ||
| Diastolic pressure [mmHg] | 64.8 [15.4] | 59 [7.4] | 0.36 | ||
| Heart rate [bpm] | 95.6 [18.9] | 87 [10.6] | 0.21 | ||
| Oxygen saturation [%] | 98.9 [1.0] | 97.9 [0.8] | 0.02 | ||
| Venham score | 9 [56] | 6.9 [0.3] | 7 [44] | 6.7 [0.5] | 0.01 |
| Post-sedation | 35 [81] | 8 [19] | |||
| Clinical Parameter | |||||
| Systolic pressure [mmHg] | 108.7 [10.7] | 113 [7.2] | 0.33 | ||
| Diastolic pressure [mmHg] | 68.2 [12.4] | 59.1 [6.1] | 0.02 | ||
| Heart rate [bpm] | 97.8 [11.2] | 86.1 [11.1] | 0.06 | ||
| Oxygen saturation [%] | 98.6 [1.1] | 97.8 [1.0] | 0.07 | ||
| Venham score | 9 [56] | 4.9 [0.3] | 7 [44] | 4.4 [1.0] | <0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cenzato, N.; Pasquali, L.; Menozzi, G.; Maspero, C. Exploring Conscious Sedation in Pediatric Oral Surgery: A Non-Randomized Clinical Trial on Safety and Efficacy. Children 2025, 12, 604. https://doi.org/10.3390/children12050604
Cenzato N, Pasquali L, Menozzi G, Maspero C. Exploring Conscious Sedation in Pediatric Oral Surgery: A Non-Randomized Clinical Trial on Safety and Efficacy. Children. 2025; 12(5):604. https://doi.org/10.3390/children12050604
Chicago/Turabian StyleCenzato, Niccolò, Lorenzo Pasquali, Gregorio Menozzi, and Cinzia Maspero. 2025. "Exploring Conscious Sedation in Pediatric Oral Surgery: A Non-Randomized Clinical Trial on Safety and Efficacy" Children 12, no. 5: 604. https://doi.org/10.3390/children12050604
APA StyleCenzato, N., Pasquali, L., Menozzi, G., & Maspero, C. (2025). Exploring Conscious Sedation in Pediatric Oral Surgery: A Non-Randomized Clinical Trial on Safety and Efficacy. Children, 12(5), 604. https://doi.org/10.3390/children12050604