

Examining Preschoolers’ Emotion Regulation Strategies: Psychometric Properties of the Translated Dutch Early Emotion Regulation Behavior Questionnaire (EERBQ-Dutch)


Abstract
1. Introduction
1.1. Emotion Regulation in Early Childhood
1.2. Emotion Regulation and (Psycho)pathology
1.3. Measuring Emotion Regulation in Early Childhood
2. Methods
2.1. Participants
2.2. EERBQ Translation
2.3. Structure of EERBQ-Dutch
2.4. Procedures
2.5. Data Analyses
3. Results
3.1. Internal Reliability
3.2. Item–Total Correlation
3.3. Test–Retest Reliability
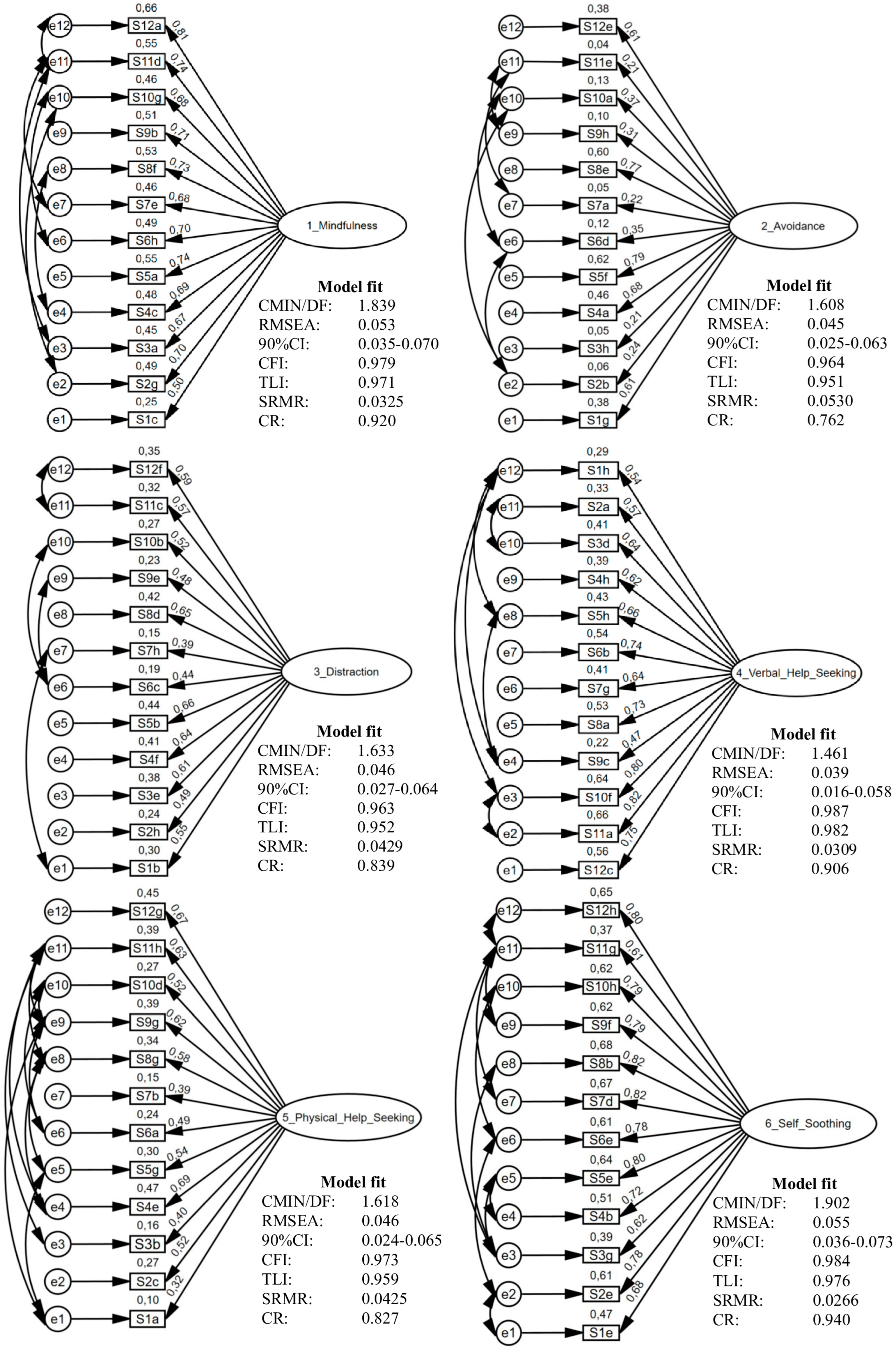
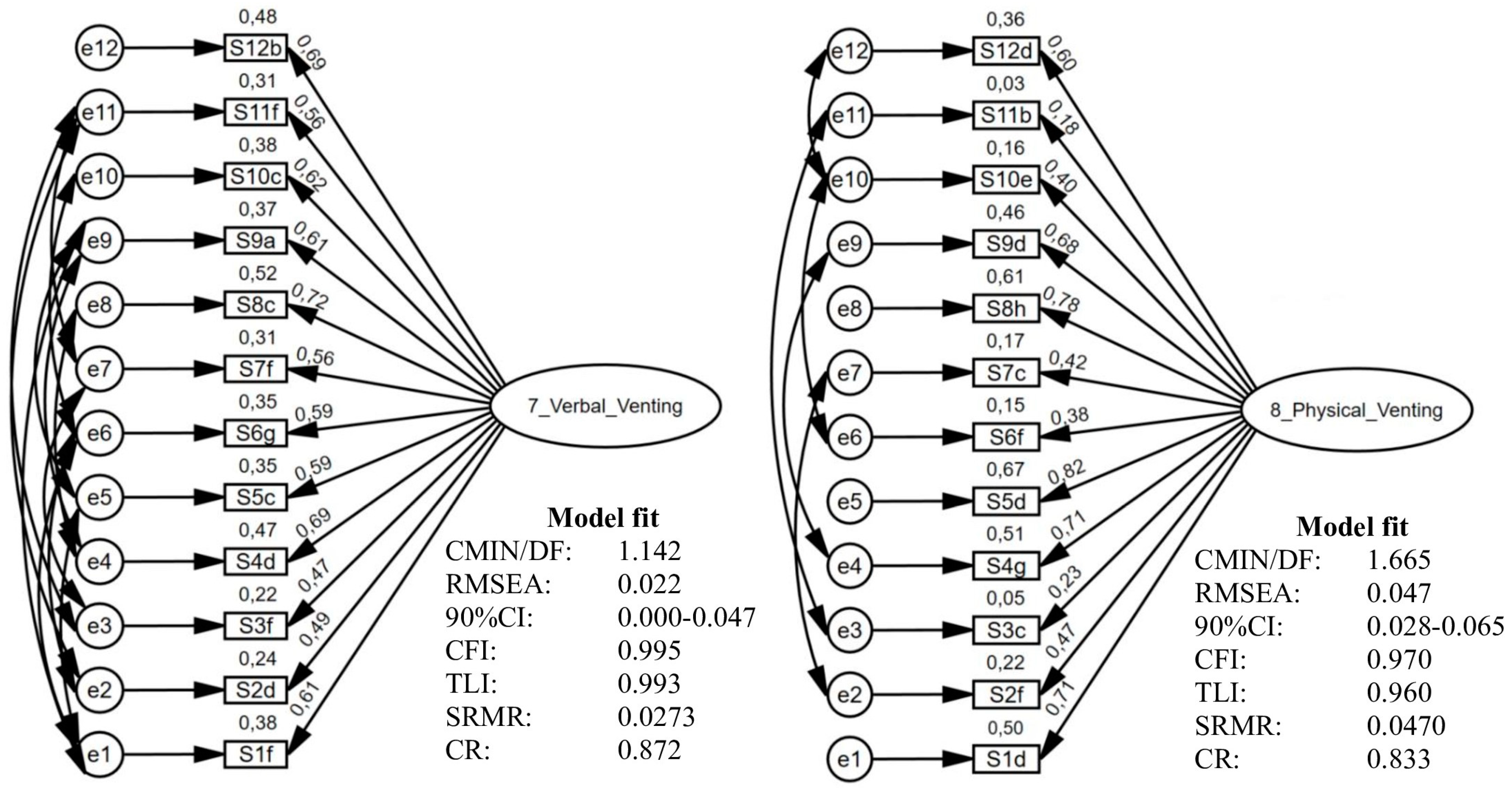
3.4. EERBQ-Dutch Factor Structure
3.5. Relation Between EERBQ and Demographic Variables
4. Discussion
4.1. Psychometric Properties
4.2. Confirmatory Factor Analysis
4.3. Demographic Predictors for ER Strategies
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gross, J.J. The emerging field of emotion regulation: An integrative review. Rev. Gen. Psychol. 1998, 2, 271–299. [Google Scholar] [CrossRef]
- Gross, J.J. Emotion regulation: Past, present, future. Cogn. Emot. 1999, 13, 551–573. [Google Scholar] [CrossRef]
- Gross, J.J.; Levenson, R.W. Emotional suppression: Physiology, self-report, and expressive behavior. J. Personal. Soc. Psychol. 1993, 64, 970–986. [Google Scholar] [CrossRef]
- Gross, J.J.; Levenson, R.W. Hiding feelings: The acute effects of inhibiting negative and positive emotion. J. Abnorm. Psychol. 1997, 106, 95–103. [Google Scholar] [CrossRef]
- Gross, J.J.; Thompson, R.A. Emotion Regulation: Conceptual Foundations. In Handbook of Emotion Regulation; Gross, J.J., Ed.; Guilford Press: New York, NY, USA, 2007; pp. 3–24. [Google Scholar]
- Thompson, R.A. Emotion regulation: A theme in search of definition. Monogr. Soc. Res. Child Dev. 1994, 59, 25–52. [Google Scholar] [CrossRef] [PubMed]
- Gross, J.J.; John, O.P. Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. J. Personal. Soc. Psychol. 2003, 85, 348–362. [Google Scholar] [CrossRef] [PubMed]
- Kring, A.M.; Sloan, D.M. Emotion Regulation and Psychopathology: A Transdiagnostic Approach to Etiology and Treatment; Guilford Press: New York, NY, USA, 2009. [Google Scholar]
- Grolnick, W.S.; McMenamy, J.M.; Kurowski, C.O. Emotional self-regulation in infancy and toddlerhood. In Child Psychology: A Handbook of Contemporary Issues, 2nd ed.; Balter, L., Tamis-LeMonda, C.S., Eds.; Psychology Press: Hove, UK, 2006; pp. 3–25. [Google Scholar]
- Grolnick, W.S.; Bridges, L.J.; Connell, J.P. Emotion regulation in two-year-olds: Strategies and emotional expression in four contexts. Child Dev. 1996, 67, 928–941. [Google Scholar] [CrossRef] [PubMed]
- Gross, J.J. Emotion regulation: Current status and future prospects. Psychol. Inq. 2015, 26, 1–26. [Google Scholar] [CrossRef]
- Cole, P.M.; Martin, S.E.; Dennis, T.A. Emotion regulation as a scientific construct: Methodological challenges and directions for child development research. Child Dev. 2004, 75, 317–333. [Google Scholar] [CrossRef]
- Campos, J.J.; Mumme, D.; Kermoian, R.; Campos, R.G. A functionalist perspective on the nature of emotion. Jpn. J. Res. Emot. 1994, 2, 1–20. [Google Scholar] [CrossRef]
- Kagan, J. On the nature of emotion. Monogr. Soc. Res. Child Dev. 1994, 59, 7–24. [Google Scholar] [CrossRef] [PubMed]
- Rothbart, M.K.; Derryberry, D. Theoretical issues in temperament. In Developmental Disabilities; Lewis, M., Taft, L.T., Eds.; Springer: Berlin, Germany, 1981; pp. 383–400. [Google Scholar] [CrossRef]
- Rothbart, M.K. Becoming Who We Are: Temperament and Personality in Development; Guilford Press: New York, NY, USA, 2011. [Google Scholar]
- Rothbart, M.K.; Derryberry, D.; Hershey, K. Stability of temperament in childhood: Laboratory infant assessment to parent report at seven years. In Temperament and Personality Development Across the Life Span; Molfese, V.J., Molfese, D.L., McCrae, R.R., Eds.; Psychology Press: New York, USA, 2000; pp. 85–119. [Google Scholar]
- Rothbart, M.K.; Ahadi, S.A.; Hershey, K.L.; Fisher, P. Investigations of temperament at three to seven years: The Children’s Behavior Questionnaire. Child Dev. 2001, 72, 1394–1408. [Google Scholar] [CrossRef]
- Rothbart, M.K.; Hwang, J. Measuring infant temperament. Infant Behav. Dev. 2002, 25, 113–116. [Google Scholar] [CrossRef]
- Brummer, L.; Stopa, L.; Bucks, R. The influence of age on emotion regulation strategies and psychological distress. Behav. Cogn. Psychother. 2014, 42, 668–681. [Google Scholar] [CrossRef]
- Cole, P.M.; Lougheed, J.P.; Ram, N. The Development of Emotion Regulation in Early Childhood: A Matter of Multiple Time Scales1. In Emotion Regulation: A Matter of Time; Cole, P.M., Lougheed, J.P., Ram, N., Eds.; Routledge: London, UK, 2018; pp. 52–69. [Google Scholar]
- Ekas, N.V.; Braungart-Rieker, J.M.; Messinger, D.S. The development of infant emotion regulation: Time is of the essence. In Emotion Regulation; Pamela, M., Cole, T.H., Eds.; Routledge: London, UK, 2018; pp. 31–51. [Google Scholar]
- Fuchs, D.; Thelen, M.H. Children’s expected interpersonal consequences of communicating their affective state and reported likelihood of expression. Child Dev. 1988, 59, 1314–1322. [Google Scholar] [CrossRef] [PubMed]
- Harrington, E.M.; Trevino, S.D.; Lopez, S.; Giuliani, N.R. Emotion regulation in early childhood: Implications for socioemotional and academic components of school readiness. Emotion 2020, 20, 48–53. [Google Scholar] [CrossRef]
- Ratcliff, K.A.; Vazquez, L.C.; Lunkenheimer, E.S.; Cole, P.M. Longitudinal changes in young children’s strategy use for emotion regulation. Dev. Psychol. 2021, 57, 1471–1486. [Google Scholar] [CrossRef] [PubMed]
- Zeman, J.; Shipman, K. Children’s expression of negative affect: Reasons and methods. Dev. Psychol. 1996, 32, 842–849. [Google Scholar] [CrossRef]
- Baird, J.A.; Moses, L.J. Do preschoolers appreciate that identical actions may be motivated by different intentions? J. Cogn. Dev. 2001, 2, 413–448. [Google Scholar] [CrossRef]
- Bartsch, K.; Wellman, H.M. Children Talk About the Mind; Oxford University Press: Oxford, UK, 1995. [Google Scholar]
- Bretherton, I.; Fritz, J.; Zahn-Waxler, C.; Ridgeway, D. Learning to talk about emotions: A functionalist perspective. Child Dev. 1986, 57, 529–548. [Google Scholar] [CrossRef]
- Denham, S.A.; Kochanoff, A. “Why is she crying?”: Children’s understanding of emotion from preschool to preadolescence. In The Wisdom in Feeling: Psychological Processes in Emotional Intelligence; Barrett, L.F., Salovey, P., Eds.; The Guilford Press: New York, NY, USA, 2002; pp. 239–270. [Google Scholar]
- Stipek, D.J.; DeCotis, K.M. Children’s understanding of the implications of causal attributions for emotional experiences. Child Dev. 1988, 59, 1601–1610. [Google Scholar] [CrossRef] [PubMed]
- Wellman, H.M.; Cross, D.; Watson, J. Meta-analysis of theory-of-mind development: The truth about false belief. Child Dev. 2001, 72, 655–684. [Google Scholar] [CrossRef]
- Blankson, A.N.; Weaver, J.M.; Leerkes, E.M.; O’Brien, M.; Calkins, S.D.; Marcovitch, S. Cognitive and emotional processes as predictors of a successful transition into school. Early Educ. Dev. 2017, 28, 1–20. [Google Scholar] [CrossRef]
- Calkins, S.D.; Dedmon, S.E. Physiological and behavioral regulation in two-year-old children with aggressive/destructive behavior problems. J. Abnorm. Child Psychol. 2000, 28, 103–118. [Google Scholar] [CrossRef] [PubMed]
- Perry, N.B.; Dollar, J.M. Measurement of behavioral emotion regulation strategies in early childhood: The early emotion regulation behavior questionnaire (EERBQ). Children 2021, 8, 779. [Google Scholar] [CrossRef]
- Sanchis-Sanchis, A.; Grau, M.D.; Moliner, A.-R.; Morales-Murillo, C.P. Effects of age and gender in emotion regulation of children and adolescents. Front. Psychol. 2020, 11, 946. [Google Scholar] [CrossRef] [PubMed]
- Silvers, J.A. Adolescence as a pivotal period for emotion regulation development. Curr. Opin. Psychol. 2022, 44, 258–263. [Google Scholar] [CrossRef]
- Zeman, J.; Cassano, M.; Perry-Parrish, C.; Stegall, S. Emotion regulation in children and adolescents. J. Dev. Behav. Pediatr. 2006, 27, 155–168. [Google Scholar] [CrossRef]
- López-Pérez, B.; Pacella, D. Interpersonal emotion regulation in children: Age, gender, and cross-cultural differences using a serious game. Emotion 2021, 21, 17–27. [Google Scholar] [CrossRef]
- Matthews, M.; Webb, T.L.; Shafir, R.; Snow, M.; Sheppes, G. Identifying the determinants of emotion regulation choice: A systematic review with meta-analysis. Cogn. Emot. 2021, 35, 1056–1084. [Google Scholar] [CrossRef]
- Sala, M.N.; Pons, F.; Molina, P. Emotion regulation strategies in preschool children. Brit. J. Dev. Psychol. 2014, 32, 440–453. [Google Scholar] [CrossRef] [PubMed]
- Zahn-Waxler, C.; Shirtcliff, E.A.; Marceau, K. Disorders of childhood and adolescence: Gender and psychopathology. Annu. Rev. Clin. Psychol. 2008, 4, 275–303. [Google Scholar] [CrossRef] [PubMed]
- Liben, L.S.; Bigler, R.S. The developmental course of gender differentiation: Conceptualizing, measuring, and evaluating constructs and pathways. Monogr. Soc. Res. Child Dev. 2002, 67, 1–147. [Google Scholar] [CrossRef]
- Martin, C.L.; Halverson, C.F., Jr. A schematic processing model of sex typing and stereotyping in children. Child Dev. 1981, 52, 1119–1134. [Google Scholar] [CrossRef]
- Deaux, K.; Major, B. Putting gender into context: An interactive model of gender-related behavior. Psychol. Rev. 1987, 94, 369. [Google Scholar] [CrossRef]
- Nolen-Hoeksema, S. Emotion regulation and psychopathology: The role of gender. Annu. Rev. Clin. Psychol. 2012, 8, 161–187. [Google Scholar] [CrossRef]
- Tamres, L.K.; Janicki, D.; Helgeson, V.S. Sex differences in coping behavior: A meta-analytic review and an examination of relative coping. Personal. Soc. Psychol. Rev. 2002, 6, 2–30. [Google Scholar] [CrossRef]
- Nolen-Hoeksema, S.; Aldao, A. Gender and age differences in emotion regulation strategies and their relationship to depressive symptoms. Personal. Individ. Differ. 2011, 51, 704–708. [Google Scholar] [CrossRef]
- Preston, T.; Carr, D.C.; Hajcak, G.; Sheffler, J.; Sachs-Ericsson, N. Cognitive reappraisal, emotional suppression, and depressive and anxiety symptoms in later life: The moderating role of gender. Aging Ment. Health 2022, 26, 2390–2398. [Google Scholar] [CrossRef]
- Rogier, G.; Garofalo, C.; Velotti, P. Is emotional suppression always bad? A matter of flexibility and gender differences. Curr. Psychol. 2019, 38, 411–420. [Google Scholar] [CrossRef]
- Zhang, Y.; Bian, Y. Emotion Regulation Questionnaire for Cross-Gender Measurement Invariance in Chinese University Students. Front. Psychol. 2020, 11, 569438. [Google Scholar] [CrossRef] [PubMed]
- Cuartas, J.; Hanno, E.; Lesaux, N.K.; Jones, S.M. Executive function, self-regulation skills, behaviors, and socioeconomic status in early childhood. PLoS ONE 2022, 17, e0277013. [Google Scholar] [CrossRef]
- Lin, S.C.; Kehoe, C.; Pozzi, E.; Liontos, D.; Whittle, S. Research Review: Child emotion regulation mediates the association between family factors and internalizing symptoms in children and adolescents—A meta-analysis. J. Child Psychol. Psychiatry Allied Discip. 2024, 65, 260–274. [Google Scholar] [CrossRef]
- Ma, X.; Yang, N.; Huang, M.; Zhan, S.; Cao, H.; Jiang, S. Relationships between gross motor skills, psychological resilience, executive function, and emotional regulation among Chinese rural preschoolers: A moderated mediation model. Heliyon 2024, 10, e38039. [Google Scholar] [CrossRef]
- Paley, B.; Hajal, N.J. Conceptualizing Emotion Regulation and Coregulation as Family-Level Phenomena. Clin. Child Fam. Psychol. Rev. 2022, 25, 19–43. [Google Scholar] [CrossRef]
- Singh, S.; Shankar, B. Socio-economic status of family as a factor of emotion regulation and well-being. Indian J. Health Wellbeing 2013, 4, 1521–1524. [Google Scholar]
- Zitzmann, J.; Rombold-George, L.; Rosenbach, C.; Renneberg, B. Emotion Regulation, Parenting, and Psychopathology: A Systematic Review. Clin. Child Fam. Psychol. Rev. 2024, 27, 1–22. [Google Scholar] [CrossRef]
- Zysberg, L.; Raz, S. Emotional intelligence and emotion regulation in self-induced emotional states: Physiological evidence. Personal. Individ. Differ. 2019, 139, 202–207. [Google Scholar] [CrossRef]
- De France, K.; Evans, G.W. Expanding context in the role of emotion regulation in mental health: How socioeconomic status (SES) and developmental stage matter. Emotion 2021, 21, 772–782. [Google Scholar] [CrossRef]
- Kim, J.; Cicchetti, D. Longitudinal pathways linking child maltreatment, emotion regulation, peer relations, and psychopathology. J. Child Psychol. Psychiatry Allied Discip. 2010, 51, 706–716. [Google Scholar] [CrossRef]
- Bijttebier, P.; Roeyers, H. Temperament and vulnerability to psychopathology: Introduction to the special section. J. Abnorm. Child Psychol. 2009, 37, 305–308. [Google Scholar] [CrossRef]
- Fernández-Berrocal, P.; Extremera, N. Ability emotional intelligence, depression, and well-being. Emot. Rev. 2016, 8, 311–315. [Google Scholar] [CrossRef]
- Garnefski, N.; Kraaij, V.; van Etten, M. Specificity of relations between adolescents’ cognitive emotion regulation strategies and Internalizing and Externalizing psychopathology. J. Adolesc. 2005, 28, 619–631. [Google Scholar] [CrossRef] [PubMed]
- Lincoln, T.M.; Schulze, L.; Renneberg, B. The role of emotion regulation in the characterization, development and treatment of psychopathology. Nat. Rev. Psychol. 2022, 1, 272–286. [Google Scholar] [CrossRef]
- Paulus, F.W.; Ohmann, S.; Möhler, E.; Plener, P.; Popow, C. Emotional dysregulation in children and adolescents with psychiatric disorders. A narrative review. Front. Psychiatry 2021, 12, 628252. [Google Scholar] [CrossRef]
- Schäfer, J.; Naumann, E.; Holmes, E.A.; Tuschen-Caffier, B.; Samson, A.C. Emotion Regulation Strategies in Depressive and Anxiety Symptoms in Youth: A Meta-Analytic Review. J. Youth Adolesc. 2017, 46, 261–276. [Google Scholar] [CrossRef]
- Schneider, R.L.; Arch, J.J.; Landy, L.N.; Hankin, B.L. The longitudinal effect of emotion regulation strategies on anxiety levels in children and adolescents. J. Clin. Child Adolesc. Psychol. 2018, 47, 978–991. [Google Scholar] [CrossRef]
- Kim-Spoon, J.; Cicchetti, D.; Rogosch, F.A. A longitudinal study of emotion regulation, emotion lability-negativity, and internalizing symptomatology in maltreated and nonmaltreated children. Child Dev. 2013, 84, 512–527. [Google Scholar] [CrossRef]
- Hill, A.L.; Degnan, K.A.; Calkins, S.D.; Keane, S.P. Profiles of externalizing behavior problems for boys and girls across preschool: The roles of emotion regulation and inattention. Dev. Psychol. 2006, 42, 913–928. [Google Scholar] [CrossRef]
- Supplee, L.H.; Skuban, E.M.; Shaw, D.S.; Prout, J. Emotion regulation strategies and later externalizing behavior among European American and African American children. Dev. Psychopathol. 2009, 21, 393–415. [Google Scholar] [CrossRef]
- Garber, J.; Dodge, K.A. The Development of Emotion Regulation and Dysregulation; Cambridge University Press: Cambridge, UK, 1991. [Google Scholar]
- Kovacs, M.; Joormann, J.; Gotlib, I.H. Emotion (Dys)regulation and Links to Depressive Disorders. Child Dev. Perspect. 2008, 2, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Ollendick, T.H.; Horsch, L.M. Fears in clinic-referred children: Relations with child anxiety sensitivity, maternal overcontrol, and maternal phobic anxiety. Behav. Ther. 2007, 38, 402–411. [Google Scholar] [CrossRef]
- Zeman, J.; Shipman, K.; Suveg, C. Anger and sadness regulation: Predictions to internalizing and externalizing symptoms in children. J. Clin. Child Adolesc. Psychol. 2002, 31, 393–398. [Google Scholar] [CrossRef]
- Aldao, A.; Nolen-Hoeksema, S.; Schweizer, S. Emotion-regulation strategies across psychopathology: A meta-analytic review. Clin. Psychol. Rev. 2010, 30, 217–237. [Google Scholar] [CrossRef] [PubMed]
- Aldao, A.; Nolen-Hoeksema, S. When are adaptive strategies most predictive of psychopathology? J. Abnorm. Psychol. 2012, 121, 276–281. [Google Scholar] [CrossRef]
- Sheppes, G.; Gross, J.J. Emotion regulation effectiveness: What works when. In Handbook of Psychology; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2012; Volume 2, pp. 391–406. [Google Scholar] [CrossRef]
- Billings, A.G.; Moos, R.H. The role of coping responses and social resources in attenuating the stress of life events. J. Behav. Med. 1981, 4, 139–157. [Google Scholar] [CrossRef]
- Carver, C.S.; Scheier, M.F.; Weintraub, J.K. Assessing coping strategies: A theoretically based approach. J. Personal. Soc. Psychol. 1989, 56, 267–283. [Google Scholar] [CrossRef] [PubMed]
- Folkman, S.; Lazarus, R.S. Stress-processes and depressive symptomatology. J. Abnorm. Psychol. 1986, 95, 107–113. [Google Scholar] [CrossRef]
- Garnefski, N.; Rieffe, C.; Jellesma, F.; Terwogt, M.M.; Kraaij, V. Cognitive emotion regulation strategies and emotional problems in 9–11-year-old children: The development of an instrument. Eur. Child Adolesc. Psychiatry 2007, 16, 1–9. [Google Scholar] [CrossRef]
- Hannesdottir, D.K.; Ollendick, T.H. The role of emotion regulation in the treatment of child anxiety disorders. Clin. Child Fam. Psychol. Rev. 2007, 10, 275–293. [Google Scholar] [CrossRef]
- Braet, C.; Theuwis, L.; Van Durme, K.; Vandewalle, J.; Vandevivere, E.; Wante, L.; Moens, E.; Verbeken, S.; Goossens, L. Emotion regulation in children with emotional problems. Cogn. Ther. Res. 2014, 38, 493–504. [Google Scholar] [CrossRef]
- Silk, J.S.; Steinberg, L.; Morris, A.S. Adolescents’ emotion regulation in daily life: Links to depressive symptoms and problem behavior. Child Dev. 2003, 74, 1869–1880. [Google Scholar] [CrossRef] [PubMed]
- Garber, J.; Weiss, B.; Shanley, N. Cognitions, depressive symptoms, and development in adolescents. J. Abnor. Psychol. 1993, 102, 47–57. [Google Scholar] [CrossRef]
- Schwartz-Mette, R.A.; Lawrence, H.R.; Shankman, J.; Fearey, E.; Harrington, R. Intrapersonal emotion regulation difficulties and maladaptive interpersonal behavior in adolescence. Res. Child Adolesc. Psychopathol. 2021, 49, 749–761. [Google Scholar] [CrossRef]
- Velotti, P.; Bruno, S.; Rogier, G.; Beomonte Zobel, S.; Vacchino, M.; Garofalo, C.; Kosson, D.S. Psychopathy and Impairments in Emotion Regulation: A systematic review and Meta-analysis. Clin. Psychol. Rev. 2024, 113, 102482. [Google Scholar] [CrossRef]
- Aslan, I.H.; Dorey, L.; Grant, J.E.; Chamberlain, S.R. Emotion regulation across psychiatric disorders. CNS Spectr. 2024, 29, 215–220. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, K.A.; Mennin, D.S.; Farach, F.J. The contributory role of worry in emotion generation and dysregulation in generalized anxiety disorder. Behav. Res. Ther. 2007, 45, 35–52. [Google Scholar] [CrossRef]
- Nolen-Hoeksema, S.; Wisco, B.E.; Lyubomirsky, S. Rethinking Rumination. Perspect. Psychol. Sci. 2008, 3, 400–424. [Google Scholar] [CrossRef]
- Rottenberg, J.; Clift, A.; Bolden, S.; Salomon, K. RSA fluctuation in major depressive disorder. Psychophysiology 2007, 44, 450–458. [Google Scholar] [CrossRef]
- Linehan, M. Cognitive-Behavioral Treatment of Borderline Personality Disorder; Guilford Press: New York, NY, USA, 1993. [Google Scholar]
- Linehan, M.M.; Schmidt, H.; Dimeff, L.A., 3rd; Craft, J.C.; Kanter, J.; Comtois, K.A. Dialectical behavior therapy for patients with borderline personality disorder and drug-dependence. Am. J. Addict. 1999, 8, 279–292. [Google Scholar] [CrossRef]
- Lynch, T.R.; Trost, W.T.; Salsman, N.; Linehan, M.M. Dialectical behavior therapy for borderline personality disorder. Annu. Rev. Clin. Psychol. 2007, 3, 181–205. [Google Scholar] [CrossRef]
- Johnson, S.L. Mania and dysregulation in goal pursuit: A review. Clin. Psychol. Rev. 2005, 25, 241–262. [Google Scholar] [CrossRef]
- Oliva, V.; De Prisco, M.; Fico, G.; Possidente, C.; Bort, M.; Fortea, L.; Montejo, L.; Anmella, G.; Hidalgo-Mazzei, D.; Murru, A.; et al. Highest correlations between emotion regulation strategies and mood symptoms in bipolar disorder: A systematic review and Bayesian network meta-analysis. Neurosci. Biobehav. Rev. 2025, 169, 105967. [Google Scholar] [CrossRef]
- Bydlowski, S.; Corcos, M.; Jeammet, P.; Paterniti, S.; Berthoz, S.; Laurier, C.; Chambry, J.; Consoli, S.M. Emotion-processing deficits in eating disorders. Int. J. Eat. Disord. 2005, 37, 321–329. [Google Scholar] [CrossRef] [PubMed]
- Clyne, C.; Blampied, N.M. Training in emotion regulation as a treatment for binge eating: A preliminary study. Behav. Change 2004, 21, 269–281. [Google Scholar] [CrossRef]
- Czaja, J.; Rief, W.; Hilbert, A. Emotion regulation and binge eating in children. Int. J. Eat. Disord. 2009, 42, 356–362. [Google Scholar] [CrossRef] [PubMed]
- Goossens, L.; Van Malderen, E.; Van Durme, K.; Braet, C. Loss of control eating in adolescents: Associations with adaptive and maladaptive emotion regulation strategies. Eat. Behav. 2016, 22, 156–163. [Google Scholar] [CrossRef]
- Polivy, J.; Herman, C.P. Causes of eating disorders. Annu. Rev. Psychol. 2002, 53, 187–213. [Google Scholar] [CrossRef]
- Nigg, J.T. Parsing ADHD with temperament traits. Curr. Dir. Psychol. Sci. 2022, 31, 324–332. [Google Scholar] [CrossRef]
- Eggers, K.; Heselmans, I. Delay frustration in children who do and do not stutter: A preliminary study. J. Commun. Disord. 2024, 107, 106403. [Google Scholar] [CrossRef]
- Berking, M.; Wupperman, P. Emotion regulation and mental health: Recent findings, current challenges, and future directions. Curr. Opin. Psychiatry 2012, 25, 128–134. [Google Scholar] [CrossRef]
- Gross, J.J. Emotion regulation. In Handbook of Emotions; Lewis, M., Haviland-Jones, J.M., Barrett, L.F., Eds.; Guilford Press: New York, NY, USA, 2008; pp. 497–513. [Google Scholar]
- Jones, R.; Choi, D.; Conture, E.; Walden, T. Temperament, emotion, and childhood stuttering. Semin. Speech Lang. 2014, 35, 114–131. [Google Scholar] [CrossRef] [PubMed]
- Sheppes, G.; Suri, G.; Gross, J.J. Emotion regulation and psychopathology. Annu. Rev. Clin. Psychol. 2015, 11, 379–405. [Google Scholar] [CrossRef] [PubMed]
- Kahle, S.; Miller, J.G.; Helm, J.L.; Hastings, P.D. Linking autonomic physiology and emotion regulation in preschoolers: The role of reactivity and recovery. Dev. Psychobiol. 2018, 60, 775–788. [Google Scholar] [CrossRef] [PubMed]
- Philpott-Robinson, K.; Johnson, T.; Evans, L.; Wales, K.; Leonard, C.; Lane, A.E. Measurement of Self-regulation in Preschool and Elementary Children: A Scoping Review. Phys. Occup. Ther. Pediatr. 2023, 43, 403–429. [Google Scholar] [CrossRef]
- McDevitt, S.C.; Carey, W.B. The measurement of temperament in 3–7 year old children. Child Psychol. Psychiatry Allied Discip. 1978, 19, 245–253. [Google Scholar] [CrossRef]
- Cole, P.M.; Zahn-Waxler, C.; Fox, N.A.; Usher, B.A.; Welsh, J.D. Individual differences in emotion regulation and behavior problems in preschool children. J. Abnorm. Psychol. 1996, 105, 518–529. [Google Scholar] [CrossRef]
- Dennis, T.A.; Hajcak, G. The late positive potential: A neurophysiological marker for emotion regulation in children. J. Child Psychol. Psychiatry 2009, 50, 1373–1383. [Google Scholar] [CrossRef]
- Fabes, R.A.; Eisenberg, N.; Karbon, M.; Troyer, D.; Switzer, G. The relations of children’s emotion regulation to their vicarious emotional responses and comforting behaviors. Child Dev. 1994, 65, 1678–1693. [Google Scholar] [CrossRef]
- Sacrey, L.R.; Raza, S.; Armstrong, V.; Brian, J.A.; Kushki, A.; Smith, I.M.; Zwaigenbaum, L. Physiological measurement of emotion from infancy to preschool: A systematic review and meta-analysis. Brain Behav. 2021, 11, e01989. [Google Scholar] [CrossRef]
- Schaan, L.; Schulz, A.; Nuraydin, S.; Bergert, C.; Hilger, A.; Rach, H.; Hechler, T. Interoceptive accuracy, emotion recognition, and emotion regulation in preschool children. Int. J. Psychophysiol. 2019, 138, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Adrian, M.; Zeman, J.; Veits, G. Methodological implications of the affect revolution: A 35-year review of emotion regulation assessment in children. J. Exp. Child Psychol. 2011, 110, 171–197. [Google Scholar] [CrossRef] [PubMed]
- Zentner, M.; Bates, J.E. Child temperament: An integrative review of concepts, research programs, and measures. Int. J. Dev. Sci. 2008, 2, 7–37. [Google Scholar] [CrossRef]
- Bishop, G.; Spence, S.H.; McDonald, C. Can parents and teachers provide a reliable and valid report of behavioral inhibition? Child Dev. 2003, 74, 1899–1917. [Google Scholar] [CrossRef] [PubMed]
- Shields, A.; Cicchetti, D. Emotion regulation among school-age children: The development and validation of a new criterion Q-sort scale. Dev. Psychol. 1997, 33, 906–916. [Google Scholar] [CrossRef]
- Zeman, J.; Cassano, M.; Suveg, C.; Shipman, K. Initial validation of the children’s worry management scale. J. Child Fam. Stud. 2010, 19, 381–392. [Google Scholar] [CrossRef]
- Zeman, J.; Shipman, K.; Penza-Clyve, S. Development and initial validation of the Children’s Sadness Management Scale. J. Nonverbal Behav. 2001, 25, 187–205. [Google Scholar] [CrossRef]
- MacNamara, A.; Joyner, K.; Klawohn, J. The psychophysiology of emotion regulation: Next generation approaches. Int. J. Psychophysiol. 2023, 188, 12–16. [Google Scholar] [CrossRef]
- Kwon, H.; Yoon, K.L.; Joormann, J.; Kwon, J.-H. Cultural and gender differences in emotion regulation: Relation to depression. Cogn. Emot. 2013, 27, 769–782. [Google Scholar] [CrossRef]
- Matsumoto, D.; Yoo, S.H.; Nakagawa, S. Culture, emotion regulation, and adjustment. J. Personal. Soc. Psychol. 2008, 94, 925–937. [Google Scholar] [CrossRef]
- Schunk, F.; Trommsdorff, G.; König-Teshnizi, D. Regulation of positive and negative emotions across cultures: Does culture moderate associations between emotion regulation and mental health? Cogn. Emot. 2022, 36, 352–363. [Google Scholar] [CrossRef] [PubMed]
- Song, H.; Chan, J.S.; Ryan, C. Differences and Similarities in the Use of Nine Emotion Regulation Strategies in Western and East-Asian Cultures: Systematic Review and Meta-Analysis. J. Cross-Cult. Psychol. 2024, 55, 865–885. [Google Scholar] [CrossRef]
- Henrich, J.; Heine, S.J.; Norenzayan, A. The weirdest people in the world? Behav. Brain Sci. 2010, 33, 61–135. [Google Scholar] [CrossRef] [PubMed]
- Hofstede, G. Culture’s Consequences: Comparing Values, Behaviors, Institutions, and Organizations Across Nations, 2nd ed.; Sage Publications: Thousand Oaks, CA, USA, 2001. [Google Scholar] [CrossRef]
- Van de Vijver, F.J.; Leung, K. Methods and Data Analysis for Cross-Cultural Research, 2nd ed.; Cambridge University Press: Cambridge, UK, 2021; Volume 116. [Google Scholar] [CrossRef]
- Fabes, R.A.; Eisenberg, N.; Bernzweig, J. Coping with Children’s Negative Emotions Scale (CCNES); APA PsycTests: Tempe, AZ, USA, 1990. [Google Scholar] [CrossRef]
- Qin, S.; Nelson, L.; McLeod, L.; Eremenco, S.; Coons, S.J. Assessing test–retest reliability of patient-reported outcome measures using intraclass correlation coefficients: Recommendations for selecting and documenting the analytical formula. Qual. Life Res. 2019, 28, 1029–1033. [Google Scholar] [CrossRef]
- Cheung, G.W.; Cooper-Thomas, H.D.; Lau, R.S.; Wang, L.C. Reporting reliability, convergent and discriminant validity with structural equation modeling: A review and best-practice recommendations. Asia Pac. J. Manag. 2024, 41, 745–783. [Google Scholar] [CrossRef]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis, 8th ed.; Cengage Learning EMEA: Andover, UK, 2019. [Google Scholar]
- Peterson, R.A.; Kim, Y. On the relationship between coefficient alpha and composite reliability. J. Appl. Psychol. 2013, 98, 194–198. [Google Scholar] [CrossRef]
- Raykov, T. Scale Reliability, Cronbach’s Coefficient Alpha, and Violations of Essential Tau-Equivalence with Fixed Congeneric Components. Multivar. Behav. Res. 1997, 32, 329–353. [Google Scholar] [CrossRef]
- Hollingshead, A.B. Four factor index of social status. Yale J. Sociol. 2011, 8, 21–51. [Google Scholar]
- Brown, T.A. Confirmatory Factor Analysis for Applied Research, 2nd ed.; Guilford publications: New York, NY, USA, 2015. [Google Scholar]
- Nunnally, J.C.; Bernstein, I.H. Psychometric Theory, 3rd ed.; McGraw-Hill: New York, NY, USA, 1994. [Google Scholar]
- Clark, L.A.; Watson, D. Constructing validity: Basic issues in objective scale development. In Methodological Issues and Strategies in Clinical Research, 4th ed.; Kazdin, A.E., Ed.; American Psychological Association: Washington, DC, USA, 2016; pp. 187–203. [Google Scholar] [CrossRef]
- Fornell, C.; Larcker, D.F. Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Gullone, E.; Hughes, E.K.; King, N.J.; Tonge, B. The normative development of emotion regulation strategy use in children and adolescents: A 2-year follow-up study. J. Child Psychol. Psychiatry Allied Discip. 2010, 51, 567–574. [Google Scholar] [CrossRef]
- Cracco, E.; Goossens, L.; Braet, C. Emotion regulation across childhood and adolescence: Evidence for a maladaptive shift in adolescence. Eur. Child Adolesc. Psychiatry 2017, 26, 909–921. [Google Scholar] [CrossRef] [PubMed]
- Liddell, B.J.; Williams, E.N. Cultural differences in interpersonal emotion regulation. Front. Psychol. 2019, 10, 999. [Google Scholar] [CrossRef] [PubMed]
- Jaramillo, J.M.; Rendón, M.I.; Muñoz, L.; Weis, M.; Trommsdorff, G. Children’s Self-Regulation in Cultural Contexts: The Role of Parental Socialization Theories, Goals, and Practices. Front. Psychol. 2017, 8, 923. [Google Scholar] [CrossRef] [PubMed]
- Goodman, R. The Strengths and Difficulties Questionnaire: A research note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| ER Strategy | Definition |
|---|---|
| Mindfulness | Self-awareness of one’s own feelings (e.g., acknowledging feeling sad) |
| Avoidance | Withdrawing from, hiding, or avoiding the source of arousal (e.g., becoming withdrawn, quiet, or retreating to a personal space) |
| Distraction | The child’s ability to independently avert attention away from the source of distress to an activity or object less arousing (e.g., find another activity to do or toy to play with) |
| Verbal Help-Seeking | Eliciting caregiver assistance in dampening emotional arousal through verbal communication such as conversation or questioning (e.g., initiating a conversation with the caregiver) |
| Physical Help-Seeking | Eliciting caregiver assistance in dampening emotional arousal through physical contact such as hugs or holding (e.g., holding caregiver’s hand when feeling scared) |
| Self-Soothing | Physical mechanism that is independently generated to calm oneself such as sucking or rubbing (e.g., sucking thumb or cuddling a blanket) |
| Verbal Venting | Releasing arousal in a verbal way such as yelling, screaming, or crying (e.g., screaming because caregiver refuses to buy candy at a grocery store) |
| Physical Venting | Releasing arousal in a physical way such as running, jumping, kicking, or hitting (e.g., hitting another child) |
| Strategy | M (SD) | Range | α |
|---|---|---|---|
| Mindfulness | 4.8 (1.4) | 1.1–7.0 | 0.92 |
| Avoidance | 2.2 (0.9) | 1.0–4.7 | 0.79 |
| Distraction | 3.9 (1.1) | 1.3–6.8 | 0.84 |
| Verbal Help-Seeking | 4.7 (1.3) | 1.0–7.0 | 0.90 |
| Physical Help-Seeking | 5.1 (1.0) | 2.0–7.0 | 0.81 |
| Self-Soothing | 2.1 (1.3) | 1.0–7.0 | 0.94 |
| Verbal Venting | 2.6 (1.2) | 1.0–6.3 | 0.88 |
| Physical Venting | 2.5 (0.9) | 1.0–5.6 | 0.83 |
| Emotional Reactivity | 3.6 (0.9) | 1.7–5.6 | 0.66 |
| Strategy | S1 | S2 | S3 | S4 | S5 | S6 | S7 | S8 | S9 | S10 | S11 | S12 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mindfulness | 0.49 | 0.69 | 0.65 | 0.65 | 0.70 | 0.66 | 0.65 | 0.68 | 0.66 | 0.67 | 0.74 | 0.77 |
| Avoidance | 0.47 | 0.42 | 0.23 | 0.53 | 0.58 | 0.49 | 0.32 | 0.63 | 0.29 | 0.45 | 0.31 | 0.48 |
| Distraction | 0.47 | 0.42 | 0.56 | 0.57 | 0.60 | 0.42 | 0.34 | 0.60 | 0.41 | 0.51 | 0.54 | 0.58 |
| Verbal Help-Seeking | 0.57 | 0.55 | 0.61 | 0.61 | 0.68 | 0.66 | 0.60 | 0.67 | 0.50 | 0.72 | 0.74 | 0.67 |
| Physical Help-Seeking | 0.33 | 0.42 | 0.39 | 0.58 | 0.54 | 0.43 | 0.33 | 0.53 | 0.57 | 0.45 | 0.55 | 0.58 |
| Self-Soothing | 0.67 | 0.79 | 0.63 | 0.71 | 0.77 | 0.79 | 0.79 | 0.79 | 0.76 | 0.76 | 0.65 | 0.78 |
| Verbal Venting | 0.60 | 0.43 | 0.51 | 0.61 | 0.60 | 0.55 | 0.58 | 0.67 | 0.61 | 0.58 | 0.57 | 0.61 |
| Physical Venting | 0.65 | 0.44 | 0.29 | 0.60 | 0.68 | 0.36 | 0.44 | 0.69 | 0.59 | 0.43 | 0.25 | 0.59 |
| Emotional Reactivity | Question 1 | Question 2 | Question 3 | Question 4 | Question 5 | Question 6 | ||||||
| 0.52 | 0.58 | 0.49 | 0.51 | 0.18 | 0.13 | |||||||
| Emotion Regulation Strategy | ICC | 95% CI | p |
|---|---|---|---|
| Mindfulness | 0.888 | [0.816, 0.931] | <0.001 |
| Avoidance | 0.760 | [0.606, 0.853] | <0.001 |
| Distraction | 0.804 | [0.678, 0.880] | <0.001 |
| Verbal Help-Seeking | 0.938 | [0.899, 0.962] | <0.001 |
| Physical Help-Seeking | 0.825 | [0.713, 0.893] | <0.001 |
| Self-Soothing | 0.923 | [0.874, 0.953] | <0.001 |
| Verbal Venting | 0.881 | [0.805, 0.927] | <0.001 |
| Physical Venting | 0.836 | [0.731, 0.900] | <0.001 |
| Emotional Reactivity | 0.855 | [0.763–0.912] | <0.001 |
| Variable | Mindfulness | Avoidance | Distraction | Verbal Help-Seeking | Physical Help-Seeking | Self-Soothing | Verbal Venting | Physical Venting | Emotional Reactivity |
|---|---|---|---|---|---|---|---|---|---|
| Constant | 2.09 *** | 1.81 *** | 4.17 *** | 1.55 *** | 5.41 *** | 1.73 *** | 3.68 *** | 3.48 *** | 3.45 *** |
| Age | 0.04 *** | 0.00 | 0.00 | 0.04 *** | −0.01 | −0.00 | −0.02 *** | −0.01 *** | 0.00 |
| Sex | 0.16 | −0.15 | 0.02 | 0.30 * | 0.11 | 0.06 | −0.27 | −0.43 *** | −0.28 * |
| SES | 0.01 | 0.01 | −0.01 | 0.01 | −0.00 | 0.01 | 0.00 | 0.20 | 0.01 * |
| R2 | 0.16 | 0.02 | 0.01 | 0.25 | 0.01 | 0.00 | 0.06 | 0.11 | 0.04 |
| Adj. R2 | 0.15 | 0.01 | 0.00 | 0.24 | 0.00 | −0.01 | 0.05 | 0.10 | 0.03 |
| F(df = 3) | 16.80 *** | 1.92 | 1.25 | 30.46 *** | 1.00 | 0.30 | 6.30 *** | 10.87 *** | 3.46 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heselmans, I.; Van Gaever, M.; Hoogers, H.; Eggers, K. Examining Preschoolers’ Emotion Regulation Strategies: Psychometric Properties of the Translated Dutch Early Emotion Regulation Behavior Questionnaire (EERBQ-Dutch). Children 2025, 12, 494. https://doi.org/10.3390/children12040494
Heselmans I, Van Gaever M, Hoogers H, Eggers K. Examining Preschoolers’ Emotion Regulation Strategies: Psychometric Properties of the Translated Dutch Early Emotion Regulation Behavior Questionnaire (EERBQ-Dutch). Children. 2025; 12(4):494. https://doi.org/10.3390/children12040494
Chicago/Turabian StyleHeselmans, Iris, Marie Van Gaever, Hana Hoogers, and Kurt Eggers. 2025. "Examining Preschoolers’ Emotion Regulation Strategies: Psychometric Properties of the Translated Dutch Early Emotion Regulation Behavior Questionnaire (EERBQ-Dutch)" Children 12, no. 4: 494. https://doi.org/10.3390/children12040494
APA StyleHeselmans, I., Van Gaever, M., Hoogers, H., & Eggers, K. (2025). Examining Preschoolers’ Emotion Regulation Strategies: Psychometric Properties of the Translated Dutch Early Emotion Regulation Behavior Questionnaire (EERBQ-Dutch). Children, 12(4), 494. https://doi.org/10.3390/children12040494