
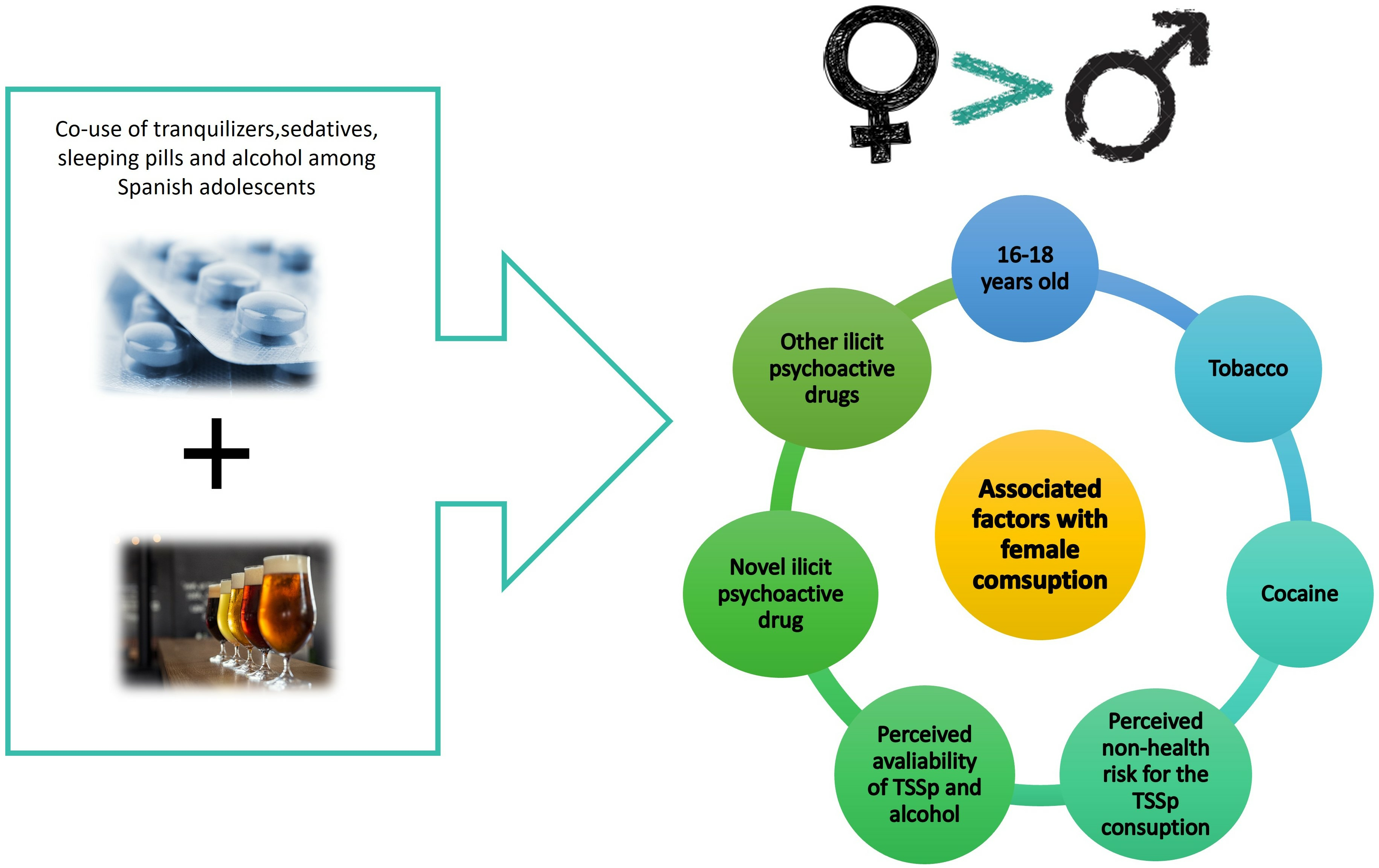
Gender Differences in the Co-Use of Tranquilizers, Sedatives, Sleeping Pills and Alcohol among Spanish Adolescents: A Nationwide Population-Based Study

 , ,
, ,  ,
,
Abstract

1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Study Design
2.3. Study Variables
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations Office on Drugs and Crime (UNODC). World Drug Report 2018. Available online: https://www.unodc.org/wdr2018/prelaunch/WDR18_Booklet_1_EXSUM.pdf (accessed on 18 March 2022).
- Ford, J.A. The prescription drug problem we are missing: Risks associated with the misuse of tranquilizers and sedatives. J. Adolesc. Health 2018, 63, 665–666. [Google Scholar] [CrossRef]
- Palacios-Ceña, D.; Jiménez-Trujillo, I.; Hernández-Barrera, V.; Florencio, L.L.; Carrasco-Garrido, P. Time trends in the co-use of cannabis and the misuse of tranquilizers, sedatives and sleeping pills among young adults in Spain between 2009 and 2015. Int. J. Env. Res. Public Health 2019, 16, 3423. [Google Scholar] [CrossRef]
- Goldstick, J.E.; Bonar, E.E.; Myers, M.; Bohnert, A.S.B.; Walton, M.A.; Cunningham, R.M. Within-person predictors of same-day alcohol and nonmedical prescription drug use among youth presenting to an urban emergency department. J. Stud. Alcohol. Drugs 2022, 83, 85–90. [Google Scholar] [CrossRef]
- Cabrera-Perona, V.; Ordoñez-Franco, A.; González-Galnares, I.; Civantos-Cantero, V.; Moriano-León, J.A.; Lloret-Irles, D. Evaluation of the effectiveness of a school-based alcohol and cannabis prevention programme among adolescents. Rev. Esp. Salud Publica. 2022, 96, e202201004. [Google Scholar]
- Barrense-Dias, Y.; Berchtold, A.; Akre, C.; Surís, J.C. Consuming energy drinks at the age of 14 predicted legal and illegal substance use at 16. Acta Paediatr. 2016, 105, 1361–1368. [Google Scholar] [CrossRef]
- Benkert, R.; Abel, T. Heavy energy drink consumption is associated with risky substance use in young Swiss men. Swiss Med. Wkly. 2020, 150, w20243. [Google Scholar] [CrossRef] [PubMed]
- Terry-McElrath, Y.M.; O’Malley, P.M.; Johnston, L.D. Energy drinks, soft drinks, and substance use among United States secondary school students. J. Addict Med. 2014, 8, 6–13. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Fact Sheet: Adolescent and Young Adult Health. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/adolescents-health-risks-and-solutions (accessed on 18 March 2022).
- Konefal, S.; Sherk, A.; Maloney-Hall, B.; Young, M.; Kent, P.; Biggar, E. Polysubstance use poisoning deaths in Canada: An analysis of trends from 2014 to 2017 using mortality data. BMC Public Health 2022, 22, 269. [Google Scholar] [CrossRef] [PubMed]
- Chiappini, S.; Mosca, A.; Miuli, A.; Santovito, M.C.; Orsolini, L.; Corkery, J.M.; Guirguis, A.; Pettorruso, M.; Martinotti, G.; Di Giannantonio, M.; et al. New psychoactive substances and suicidality: A systematic review of the current literature. Medicina 2021, 57, 580. [Google Scholar] [CrossRef] [PubMed]
- Jang, J.B.; Patrick, M.E.; Keyes, K.M.; Hamilton, A.D.; Schulenberg, J.E. Frequent binge drinking among US adolescents, 1991 to 2015. Pediatrics 2017, 139, e20164023. [Google Scholar] [CrossRef] [PubMed]
- Spanish Observatory on Drugs and Addictions. Nationwide Survey on Drug Use Among Secondary School Students (ESTUDES) 2016/2017. Madrid: Ministry of Health. Government Delegation for the National Plan on Drugs. 2018. Available online: https://pnsd.sanidad.gob.es/profesionales/sistemasInformacion/sistemaInformacion/pdf/2016_2017_ESTUDES.pdf (accessed on 4 March 2024).
- Miech, R.A.; Johnston, L.D.; O’Malley, P.M.; Bachman, J.G.; Schulenberg, J.E.; Patrick, M.E. Monitoring the Future National Survey Results on Drug Use, 1975–2020: Volume I, Secondary School Students. Ann Arbor: Institute for Social Research, The University of Michigan. 2021. Available online: http://monitoringthefuture.org/pubs/monographs/mtf-vol1_2020.pdf (accessed on 4 March 2024).
- Cobo, B.; Pulido, J.; Pascual, S.; Sáiz, A.; Carrasco-Garrido, P.; Carabantes-Alarcón, D.; Sordo, L. The effects of early onset tranquilizers, sedatives, and sleeping pills use on recent consumption among adolescents. J. Addict Med. 2022, 16, e23–e29. [Google Scholar] [CrossRef]
- Carrasco-Garrido, P.; Jiménez-Trujillo, I.; Hernández-Barrera, V.; García-Gómez-Heras, S.; Alonso-Fernández, N.; Palacios-Ceña, D. Trends in the misuse of tranquilizers, sedatives, and sleeping pills by adolescents in Spain, 2004–2014. J. Adolesc. Health 2018, 63, 709–716. [Google Scholar] [CrossRef]
- Carrasco-Garrido, P.; Jiménez-Trujillo, I.; Hernández-Barrera, V.; Alonso-Fernández, N.; García-Gómez-Heras, S.; Palacios-Ceña, D. Gender differences in the nonmedical use of psychoactive medications in the school population- national trends and related factors. BMC Pediatr. 2019, 19, 362. [Google Scholar] [CrossRef]
- Hladun, O.; Papaseit, E.; Martín, S.; Barriocanal, A.M.; Poyatos, L.; Farré, M.; Pérez-Mañá, C. Interaction of energy drinks with prescription medication and drugs of abuse. Pharmaceutics 2021, 13, 1532. [Google Scholar] [CrossRef]
- Perlmutter, A.S.; Rivera-Aguirre, A.E.; Mauro, P.M.; Castillo-Carniglia, A.; Rodriguez, N.; Cadenas, N.; Cerdá, M.; Martins, S.S. Sex differences in nonmedical prescription tranquilizer and stimulant use trends among secondary school students in Argentina, Chile, and Uruguay. Drug Alcohol. Depend. 2019, 205, 107607. [Google Scholar] [CrossRef]
- Alonso-Fernández, N.; Jiménez-Trujillo, I.; Hernández-Barrera, V.; Palacios-Ceña, D.; Carrasco-Garrido, P. Alcohol consumption among Spanish female adolescents: Related factors and national trends 2006–2014. Int. J. Environ. Res. Public Health 2019, 16, 4294. [Google Scholar] [CrossRef]
- Henkel, D.; Zemlin, U. Social inequality and substance use and problematic gambling among adolescents and young adults: A review of epidemiological surveys in Germany. Curr Drug Abus. Rev. 2016, 9, 26–48. [Google Scholar] [CrossRef]
- Donath, C.; Baier, D.; Graessel, E.; Hillemacher, T. Substance consumption in adolescents with and without an immigration background: A representative study-What part of an immigration background is protective against binge drinking? BMC Public Health 2016, 16, 1157. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Spanish Observatory on Drugs and Addictions. Nationwide Survey on Drug Use among Secondary School Students, ESTUDES. Available online: https://pnsd.sanidad.gob.es/profesionales/sistemasInformacion/sistemaInformacion/encuestas_ESTUDES.htm (accessed on 18 March 2022).
- Spanish Observatory on Drugs and Addictions. Madrid: Ministry of Health. Government Delegation for the National Plan on Drugs. 2019. Nationwide Survey on Drug Use among Secondary School Students (ESTUDES) 1994–2018. Available online: https://pnsd.sanidad.gob.es/profesionales/sistemasInformacion/sistemaInformacion/pdf/ESTUDES_2018-19_Informe.pdf (accessed on 18 March 2022).
- Hosmer, D.W.; Lemeshow, S. Applied Logistic Regression, 2nd ed.; John Wiley & Sons: Hoboken, NJ, USA, 2000. [Google Scholar]
- Opaleye, E.S.; Noto, A.R.; Sanchez, Z.M.; Amato, T.C.; Locatelli, D.P.; Gossop, M.; Ferri, C.P. Nonprescribed use of tranquilizers or sedatives by adolescents: A Brazilian national survey. BMC Public Health 2013, 13, 499. [Google Scholar] [CrossRef] [PubMed]
- Frobel, W.; Grafe, N.; Meigen, C.; Vogel, M.; Hiemisch, A.; Kiess, W.; Poulain, T. Substance use in childhood and adolescence and its associations with quality of life and behavioral strengths and difficulties. BMC Public Health 2022, 22, 275. [Google Scholar] [CrossRef] [PubMed]
- Bosque-Prous, M.; Kuipers, M.A.G.; Espelt, A.; Richter, M.; Rimpelä, A.; Perelman, J.; Federico, B.; Brugal, M.T.; Lorant, V.; Kunst, A.E. Adolescent alcohol use and parental and adolescent socioeconomic position in six European cities. BMC Public Health 2017, 17, 646. [Google Scholar] [CrossRef]
- Slade, T.; Chapman, C.; Swift, W.; Keyes, K.; Tonks, Z.; Teesson, M. Birth cohort trends in the global epidemiology of alcohol use and alcohol-related harms in men and women: Systematic review and metaregression. BMJ Open 2016, 6, e011827. [Google Scholar] [CrossRef]
- Fernandez-Mendoza, J.; Bourchtein, E.; Calhoun, S.; Puzino, K.; Snyder, C.K.; He, F.; Vgontzas, A.N.; Liao, D.; Bixler, E. Natural history of insomnia symptoms in the transition from childhood to adolescence: Population rates, health disparities, and risk factors. Sleep 2021, 44, zsaa187. [Google Scholar] [CrossRef]
- Breslau, J.; Gilman, S.E.; Stein, B.D.; Ruder, T.; Gmelin, T.; Miller, E. Sex differences in recent first-onset depression in an epidemiological sample of adolescents. Transl. Psychiaty. 2017, 7, e1139. [Google Scholar] [CrossRef] [PubMed]
- Belzunegui-Eraso, A.; Pastor-Gosálbez, I.; Raigal-Aran, L.; Valls-Fonayet, F.; Fernández-Aliseda, S.; Torres-Coronas, T. Substance use among Spanish adolescents: The information paradox. Int. J. Env. Res. Public Health 2020, 17, 627. [Google Scholar] [CrossRef] [PubMed]
- Deutsch, A.R.; Steinley, D.; Slutske, W.S. The role of gender and friends’ gender on peer socialization of adolescent drinking: A prospective multilevel social network analysis. J. Youth Adolesc. 2014, 43, 1421–1435. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Manrique, L.; Berasaluce, M.; Sureda, X.; Sandín Vázquez, M. Gender Matters: Identity, Risk Perception and Preventive Interventions for Alcohol Consumption among Adolescents Using a Qualitative Approach. Int. J. Environ. Res. Public Health 2022, 19, 16435. [Google Scholar] [CrossRef] [PubMed]
- Mosher, J.F. Joe Camel in a bottle: Diageo, the Smirnoff brand, and the transformation of the youth alcohol market. Am. J. Public Health 2012, 102, 56–63. [Google Scholar] [CrossRef]
- Atkinson, A.M.; Meadows, B.R.; Emslie, C.; Lyons, A.; Sumnall, H.R. ‘Pretty in Pink’ and ‘Girl Power’: An Analysis of the Targeting and Representation of Women in Alcohol Brand Marketing on Facebook and Instagram. Int. J. Drug Policy 2022, 101, 103547. [Google Scholar] [CrossRef]
- Sordo, L.; Indave, B.I.; Vallejo, F.; Belza, M.; Sanz-Barbero, B.; Rosales-Statkus, M.; Fernández-Balbuena, S.; Barrio, G. Effect of country-of-origin contextual factors and length of stay on ’immigrants’ substance use in Spain. Eur. J. Public Health 2015, 25, 930–936. [Google Scholar] [CrossRef] [PubMed]
- Carrasco-Garrido, P.; Díaz Rodríguez, D.R.; Jiménez-Trujillo, I.; Hernández-Barrera, V.; Florencio, L.L.; Palacios-Ceña, D. Nonmedical use of benzodiazepines among immigrant and native-born adolescents in Spain: National trends and related factors. Int. J. Environ. Res. Public Health 2021, 18, 1171. [Google Scholar] [CrossRef]
- Eslava, D.; Martínez-Vispo, C.; Villanueva-Blasco, V.J.; Errasti, J.M.; Al-Halabí, S. Dual alcohol and cannabis use in male and female adolescents: Relationships with family variables. Addict. Behav. 2023, 146, 107798. [Google Scholar] [CrossRef]
- Stewart, S.H.; McGonnell, M.; Wekerle, C.; Adlaf, E. Associations of personality with alcohol use behaviour and alcohol problems in adolescents receiving child welfare services. Int. J. Ment. Health Addict. 2011, 9, 492–506. [Google Scholar] [CrossRef]
- Stewart, S.H.; Chinneck, A.; Thompson, K.; Afzali, M.H.; Nogueira-Arjona, R.; Mahu, I.T.; Conrod, P.J. Personality to Prescription Drug Misuse in Adolescents: Testing Affect Regulation, Psychological Dysregulation, and Deviance Proneness Pathways. Front. Psychiatry 2021, 27, 640766. [Google Scholar] [CrossRef] [PubMed]
- González Moreno, A.; Molero Jurado, M.D.M. Prosocial behaviours and emotional intelligence as factors associated with healthy lifestyles and violence in adolescents. BMC Psychol. 2024, 12, 88. [Google Scholar] [CrossRef] [PubMed]
- De Andrés-Sánchez, J.; Belzunegui-Eraso, A.; Valls-Fonayet, F. The significance of information variables in polydrug use by adolescents: Insights from a cross-sectional study in Tarragona (Spain). PeerJ 2024, 12, e16801. [Google Scholar] [CrossRef] [PubMed]
- United Nations Office on Drugs and Crime (UNODC). International Standards on Drug Use Prevention 2018. Available online: https://www.unodc.org/documents/prevention/UNODC-WHO_2018_prevention_standards_E.pdf (accessed on 5 March 2024).
- Martinez-Montilla, J.M.; Mercken, L.; de Vries, H.; Candel, M.; Lima-Rodríguez, J.S.; Lima-Serrano, M. A Web-Based, Computer-Tailored Intervention to Reduce Alcohol Consumption and Binge Drinking Among Spanish Adolescents: Cluster Randomized Controlled Trial. J. Med. Internet Res. 2020, 22, e15438. [Google Scholar] [CrossRef]

{kind=link}
| Male | Female | Total | ||||||
|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | p-Value | ||
| Age | 14–15 years | 8005 | 43.09% | 8279 | 42.61% | 16,285 | 42.84% | 0.348 |
| 16–18 years | 10,574 | 56.91% | 11,151 | 57.39% | 21,725 | 57.16% | ||
| Total | 18,579 | 100.00% | 19,431 | 100.00% | 38,010 | 100.00% | ||
| Nationality | Spanish | 16,792 | 90.65% | 17,424 | 89.87% | 34,216 | 90.25% | 0.110 |
| Immigrants | 1733 | 9.35% | 1964 | 10.13% | 3697 | 9.75% | ||
| Occupational status of parents | Unemployed both | 551 | 3.03% | 671 | 3.50% | 1223 | 3.27% | 0.026 |
| Employed one | 6228 | 34.26% | 6616 | 34.53% | 12,844 | 34.40% | ||
| Employed both | 11,398 | 62.70% | 11,873 | 61.97% | 23,272 | 62.33% | ||
| Educational level of parents | No formal education | 317 | 1.93% | 327 | 1.82% | 644 | 1.87% | 0.000 |
| Primary school | 744 | 4.52% | 936 | 5.21% | 1680 | 4.88% | ||
| Secondary school | 7154 | 43.48% | 8166 | 45.52% | 15,320 | 44.55% | ||
| Higher education | 8237 | 50.07% | 8511 | 47.44% | 16,747 | 48.70% | ||
| Perceived family income | Above average | 3012 | 16.42% | 2071 | 10.80% | 5083 | 13.55% | 0.000 |
| Average | 14,519 | 79.18% | 16,249 | 84.71% | 30,768 | 82.01% | ||
| Below average | 807 | 4.40% | 861 | 4.49% | 1668 | 4.45% | ||
| Living environment | Rural (<10,000 inhabitants) | 2634 | 14.18% | 3074 | 15.82% | 5708 | 15.02% | 0.000 |
| Urban (≥10,000 inhabitants) | 15,945 | 85.82% | 16,357 | 84.18% | 32,302 | 84.98% | ||
| Any cigarette smoking in the past 12 months | No | 12,758 | 68.67% | 11,973 | 61.62% | 24,731 | 65.06% | 0.000 |
| Yes | 5821 | 31.33% | 7458 | 38.38% | 13,279 | 34.94% | ||
| Energy drink use in the past 12 months | No | 9436 | 50.79% | 13,420 | 69.07% | 22,857 | 60.13% | 0.000 |
| Yes | 9143 | 49.21% | 6010 | 30.93% | 15,153 | 39.87% | ||
| Marihuana use in the past 12 months | No | 13,712 | 73.80% | 14,957 | 76.98% | 28,670 | 75.43% | 0.000 |
| Yes | 4867 | 26.20% | 4473 | 23.02% | 9340 | 24.57% | ||
| Cocaine use in the last 12 months | No | 17,986 | 96.81% | 19,113 | 98.36% | 37,099 | 97.60% | 0.000 |
| Yes | 593 | 3.19% | 318 | 1.64% | 911 | 2.40% | ||
| Heroin use in the last 12 months | No | 18,456 | 99.33% | 19,382 | 99.75% | 37,838 | 99.55% | 0.000 |
| Yes | 124 | 0.67% | 48 | 0.25% | 172 | 0.45% | ||
| Other illicit psychoactive drug use in the last 12 months | No | 17,672 | 95.12% | 18,898 | 97.26% | 36,570 | 96.21% | 0.000 |
| Yes | 908 | 4.88% | 532 | 2.74% | 1440 | 3.79% | ||
| Novel psychoactive substances in the last 12 months | No | 18,071 | 97.26% | 19,067 | 98.13% | 37,138 | 97.70% | 0.000 |
| Yes | 508 | 2.74% | 364 | 1.87% | 872 | 2.30% | ||
| Perceived health risks for consumption of alcohol | No/few problems | 4034 | 26.77% | 3554 | 21.00% | 7588 | 23.72% | 0.000 |
| Quite a few/many problems | 11,035 | 73.23% | 13,368 | 79.00% | 24,402 | 76.28% | ||
| Perceived health risks for consumption of TSSps | No/few problems | 1366 | 10.28% | 1257 | 8.39% | 2623 | 9.28% | 0.000 |
| Quite a few/many problems | 11,920 | 89.72% | 13,713 | 91.61% | 25,633 | 90.72% | ||
| Perceived availability of alcohol | Impossible/very difficult to obtain | 859 | 5.56% | 819 | 4.75% | 1678 | 5.13% | 0.000 |
| Easy/very easy to obtain | 14,584 | 94.44% | 16,448 | 95.25% | 31,032 | 94.87% | ||
| Perceived availability of TSSps | Impossible/very difficult to obtain | 4864 | 52.73% | 5196 | 52.43% | 10,060 | 52.58% | 0.001 |
| Easy/very easy to obtain | 4360 | 47.27% | 4714 | 47.57% | 9074 | 47.42% | ||
| Sufficiently informed about drugs | Yes, perfectly | 5744 | 31.99% | 3885 | 20.41% | 9629 | 26.03% | 0.678 |
| Yes, sufficiently | 7322 | 40.77% | 7798 | 40.96% | 15,121 | 40.87% | ||
| Only halfway | 3619 | 20.15% | 5988 | 31.46% | 9607 | 25.97% | 0.000 | |
| No, I am misinformed | 1273 | 7.09% | 1365 | 7.17% | 2639 | 7.13% | ||
| TSSp co-use with alcohol in the last 12 months | No | 17,183 | 92.48% | 17,039 | 87.69% | 34,222 | 90.03% | 0.000 |
| Yes | 1396 | 7.52% | 2392 | 12.31% | 3788 | 9.97% | ||
| Male | Female | Both | OR Female | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | Categories | N | % | p-Value | N | % | p-Value | N | % | p-Value | |
| Age group | 14–15 years | 427 | 5.33 | 0.000 | 684 | 8.26 | 0.000 | 1111 | 6.82 | 0.000 | 1.60 (1.37–1-87) |
| 16–18 years | 970 | 9.17 | 1708 | 15.31 | 2677 | 12.32 | 1.80 (1.60–2.00) | ||||
| Total | 1396 | 7.52 | 2392 | 12.31 | 3788 | 9.97 | 1.72 (1.58–1.89) | ||||
| Nationality | Spanish | 1268 | 7.55 | 0.616 | 2156 | 12.38 | 0.293 | 3424 | 10.01 | 0.348 | 1.73 (1.57–1.90) |
| Immigrants | 125 | 7.24 | 227 | 11.54 | 352 | 9.53 | 1.67 (1.24–2.26) | ||||
| Occupational status of parents | Unemployed both | 56 | 10.15 | 0.042 | 96 | 14.23 | 0.253 | 151 | 12.39 | 0.019 | 1.47 (0.94–2.31) |
| Employed one | 450 | 7.22 | 820 | 12.39 | 1270 | 9.88 | 1.82 (1.55–2.13) | ||||
| Employed both | 865 | 7.59 | 1443 | 12.15 | 2308 | 9.92 | 1.68 (1.50–1.89) | ||||
| Educational level of parents | No formal education | 24 | 7.6 | 0.471 | 46 | 14.08 | 0.000 | 70 | 10.89 | 0.000 | 1.99 (0.96–4.11) |
| Primary school | 64 | 8.59 | 129 | 13.75 | 193 | 11.46 | 1.69 (1.10–2.60) | ||||
| Secondary school | 574 | 8.03 | 1100 | 13.47 | 1674 | 10.93 | 1.78 (1.55–2.05) | ||||
| Higher education | 614 | 7.45 | 970 | 11.4 | 1584 | 9.46 | 1.59 (1.40–1.82) | ||||
| Perceived family income | Above average | 287 | 9.53 | 0.000 | 282 | 13.61 | 0.008 | 569 | 11.19 | 0.000 | 1.49 (1.20–1.86) |
| Average | 1018 | 7.01 | 1962 | 12.08 | 2980 | 9.69 | 1.82 (1.64–2.02) | ||||
| Below average | 79 | 9.79 | 129 | 14.99 | 208 | 12.47 | 1.62 (1.09–2.41) | ||||
| Living environment | Rural (<10,000 inhabitants) | 178 | 6.75 | 0.109 | 387 | 12.58 | 0.608 | 565 | 9.89 | 0.850 | 1.98 (1.57–2.53) |
| Urban (≥10,000 inhabitants) | 1219 | 7.64 | 2005 | 12.26 | 3223 | 9.98 | 1.69 (1.53–1.86) | ||||
| Male | Female | Both | OR Female | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | Categories | N | % | p-Value | N | % | p-Value | N | % | p-Value | |
| Any cigarette smoking in the past 12 months | Yes | 810 | 13.91 | 0.000 | 1462 | 19.6 | 0.000 | 2272 | 17.11 | 0.000 | 1.51 (1.33–1.70) |
| Energy drink use in the past 12 months | Yes | 943 | 10.31 | 0.000 | 1084 | 18.04 | 0.000 | 2027 | 13.38 | 0.000 | 1.91 (1.69–2.17) |
| Marihuana use in the past 12 months | Yes | 760 | 15.61 | 0.000 | 1039 | 23.23 | 0.000 | 1799 | 19.26 | 0.000 | 1.63 (1.43–1.87) |
| Cocaine use in the last 12 months | Yes | 194 | 32.75 | 0.000 | 141 | 44.52 | 0.000 | 336 | 36.86 | 0.000 | 1.65 (1.14–2.38) |
| Heroin use in the last 12 months | Yes | 49 | 39.34 | 0.000 | 28 | 57.2 | 0.000 | 76 | 44.37 | 0.000 | 2.06 (0.84–5.05) |
| Other illicit psychoactive drug use in the last 12 months | Yes | 300 | 33.08 | 0.000 | 219 | 41.13 | 0.000 | 519 | 36.06 | 0.000 | 1.41 (1.06–1.87) |
| Novel psychoactive substances in the last 12 months | Yes | 181 | 35.51 | 0.000 | 143 | 39.17 | 0.000 | 323 | 37.04 | 0.000 | 1.17 (0.82–1.67) |
| Perceived health risks for consumption of alcohol | No/few problems | 348 | 8.63 | 0.031 | 552 | 15.53 | 0.000 | 900 | 11.86 | 0.031 | 1.94 (1.62–2.33) |
| Quite a few/many problems | 834 | 7.56 | 1618 | 12.11 | 2453 | 10.05 | 1.68 (1.50–1.89) | ||||
| Perceived health risk for consumption of TSSps | No/few problems | 184 | 13.46 | 0.000 | 330 | 26.22 | 0.000 | 513 | 19.57 | 0.000 | 2.29 (1.76–2.97) |
| Quite a few/many problems | 852 | 7.15 | 1580 | 11.52 | 2432 | 9.49 | 1.69 (1.51–1.89) | ||||
| Perceived availability of alcohol | Impossible/very difficult to obtain | 29 | 3.38 | 0.000 | 44 | 5.39 | 0.000 | 73 | 4.36 | 0.000 | 1.63 (0.90–2.93) |
| Easy/very easy to obtain | 1211 | 8.3 | 2235 | 13.59 | 3446 | 11.1 | 1.74 (1.58–1.91) | ||||
| Perceived availability of TSSps | Impossible/very difficult to obtain | 291 | 5.97 | 0.000 | 478 | 9.2 | 0.000 | 768 | 7.64 | 0.000 | 1.60 (1.30–1.94) |
| Easy/very easy to obtain | 654 | 15.01 | 1114 | 23.64 | 1769 | 19.49 | 1.75 (1.53–2.01) | ||||
| Sufficiently informed about drugs | Yes, perfectly | 530 | 9.22 | 0.000 | 592 | 15.23 | 0.000 | 1121 | 11.65 | 0.000 | 1.77 (1.50–2.08) |
| Yes, sufficiently | 505 | 6.9 | 954 | 12.23 | 1459 | 9.65 | 1.88 (1.62–2.18) | ||||
| Only halfway | 227 | 6.27 | 0.000 | 665 | 11.1 | 0.000 | 892 | 9.28 | 0.000 | 1.87 (1.53–2.28) | |
| No, I am misinformed | 71 | 5.58 | 120 | 8.79 | 191 | 7.24 | 1.63 (1.13–2.35) | ||||
| Male | Female | BOTH | ||
|---|---|---|---|---|
| Age | 16–18 Years | 1.26 (1–1.58) | 1.65 (1.39–1.95) | 1.49 (1.3–1.7) |
| Any cigarette smoking in the past 12 months | Yes | 1.61 (1.21–2.14) | 1.73 (1.42–2.12) | 1.68 (1.42–1.98) |
| Energy drink use in the past 12 months | Yes | 1.45 (1.15–1.82) | 1.4 (1.17–1.66) | 1.41 (1.23–1.61) |
| Marihuana use in the past 12 months | Yes | 1.67 (1.24–2.26) | 1.33 (1.08–1.64) | 1.44 (1.21–1.7) |
| Cocaine use in the last 12 months | Yes | 1.54 (1.03–2.3) | 1.84 (1.14–2.99) | 1.74 (1.27–2.37) |
| Other illicit psychoactive drug use in the last 12 months | Yes | 2.58 (1.86–3.58) | 1.89 (1.33–2.68) | 2.19 (1.72–2.8) |
| Novel psychoactive substances in the last 12 months | Yes | 1.52 (1–2.31) | 1.74 (1.08–2.79) | 1.56 (1.14–2.14) |
| Perceived health risk for consumption of TSSps | No/few problems | 1.52 (1.14–2.03) | 2.45 (1.98–3.03) | 2.05 (1.73–2.44) |
| Perceived availability of alcohol | Easy/very easy | NS | 2.09 (1.24–3.52) | 1.93 (1.32–2.82) |
| Perceived availability of TSSps | Easy/very easy | 2.04 (1.63–2.55) | 2.23 (1.88–2.65) | 2.12 (1.85–2.44) |
| Sex | Female | NA | NA | 2.09 (1.82–2.39) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carrasco-Garrido, P.; Jiménez-Trujillo, I.; Hernández-Barrera, V.; Florencio, L.L.; Yeamans, S.; Palacios-Ceña, D. Gender Differences in the Co-Use of Tranquilizers, Sedatives, Sleeping Pills and Alcohol among Spanish Adolescents: A Nationwide Population-Based Study. Children 2024, 11, 339. https://doi.org/10.3390/children11030339
Carrasco-Garrido P, Jiménez-Trujillo I, Hernández-Barrera V, Florencio LL, Yeamans S, Palacios-Ceña D. Gender Differences in the Co-Use of Tranquilizers, Sedatives, Sleeping Pills and Alcohol among Spanish Adolescents: A Nationwide Population-Based Study. Children. 2024; 11(3):339. https://doi.org/10.3390/children11030339
Chicago/Turabian StyleCarrasco-Garrido, Pilar, Isabel Jiménez-Trujillo, Valentín Hernández-Barrera, Lidiane Lima Florencio, Spencer Yeamans, and Domingo Palacios-Ceña. 2024. "Gender Differences in the Co-Use of Tranquilizers, Sedatives, Sleeping Pills and Alcohol among Spanish Adolescents: A Nationwide Population-Based Study" Children 11, no. 3: 339. https://doi.org/10.3390/children11030339
APA StyleCarrasco-Garrido, P., Jiménez-Trujillo, I., Hernández-Barrera, V., Florencio, L. L., Yeamans, S., & Palacios-Ceña, D. (2024). Gender Differences in the Co-Use of Tranquilizers, Sedatives, Sleeping Pills and Alcohol among Spanish Adolescents: A Nationwide Population-Based Study. Children, 11(3), 339. https://doi.org/10.3390/children11030339