
Inflammatory and Hematologic Liver and Platelet (HALP) Scores in Hypothermia-Treated Hypoxic–Ischemic Encephalopathy (HIE)

 , , ,
, , ,  and
and
Abstract
1. Introduction
2. Material and Methods
2.1. Overview and Ethical Consideration
2.2. Study Population and Inclusion/Exclusion Criteria
2.3. Treatment Protocol
2.4. Data Collection and Variables
- NLR (neutrophil-to-lymphocyte ratio): N/L.
- PLR (platelet-to-lymphocyte ratio), p/L.
- Monocyte-to-lymphocyte ratio (MLR) (M/L).
- Systemic immune-inflammation index (SII): P × N/L.
- SIRI (systemic inflammation response index): N × M/L.
- PIV (platelet, neutrophil, monocyte, and lymphocyte index): P × N × M/L.
- HALP score: hemoglobin (g/L) × albumin (g/L) levels × lymphocyte count (/L)/platelet count (/L).
2.5. Statistical Analysis
3. Results
3.1. Analysis of Clinical and Demographic Parameters in HIE and Control Cohorts
3.2. Temporal Changes and Associations in Systemic Inflammatory Markers and Hematological Parameters in Hypoxic–Ischemic Encephalopathy (HIE) and Control Groups
3.3. Comparative Analysis of Temporal Variations in Hematological and Systemic Inflammatory Parameters before the Therapeutic Hypothermia Treatment and during/or toward Finishing the Hypothermia Therapy in HIE Patients
3.4. Analysis of Hematological and Inflammatory Markers in HIE Patients according to Clinical Subgroups
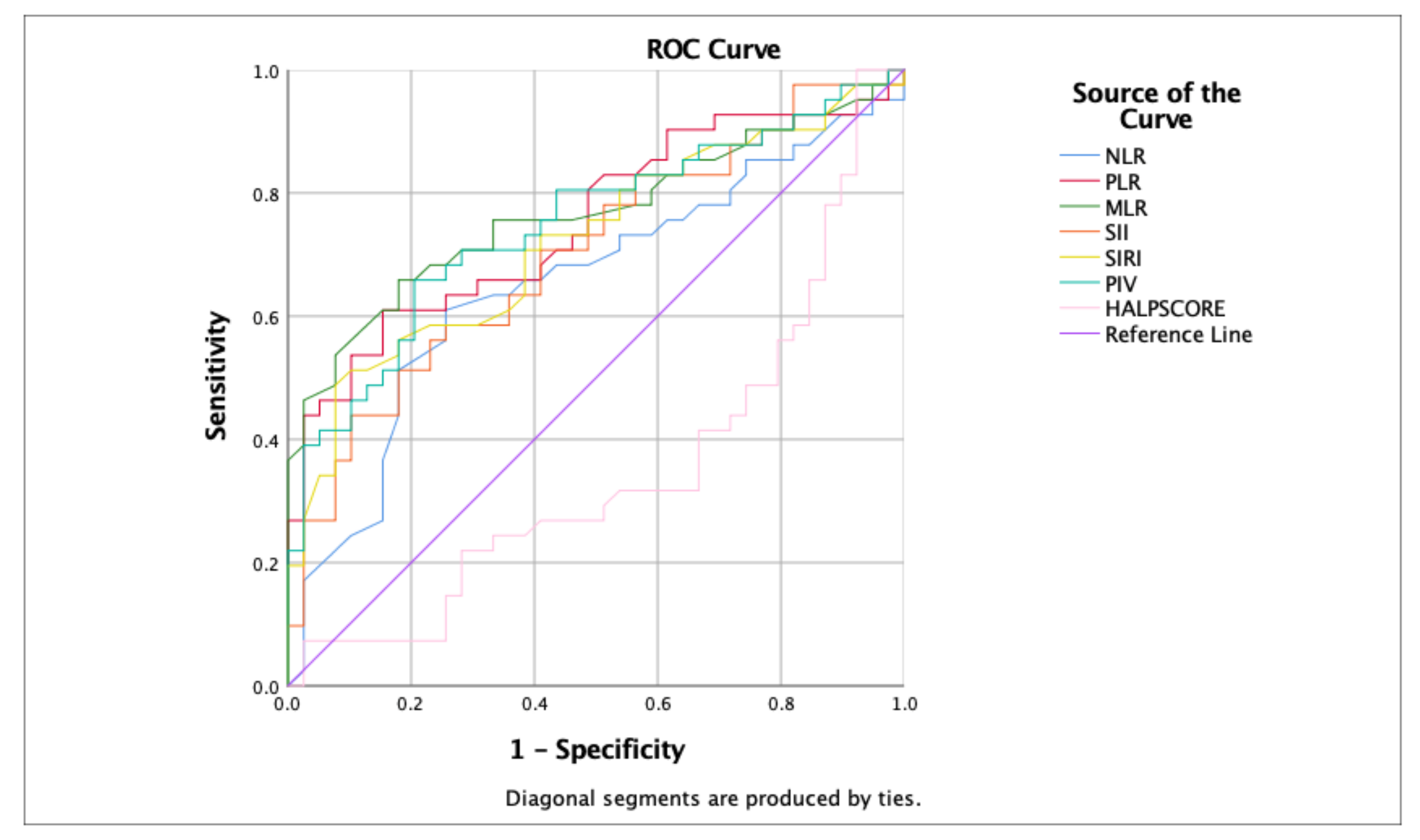
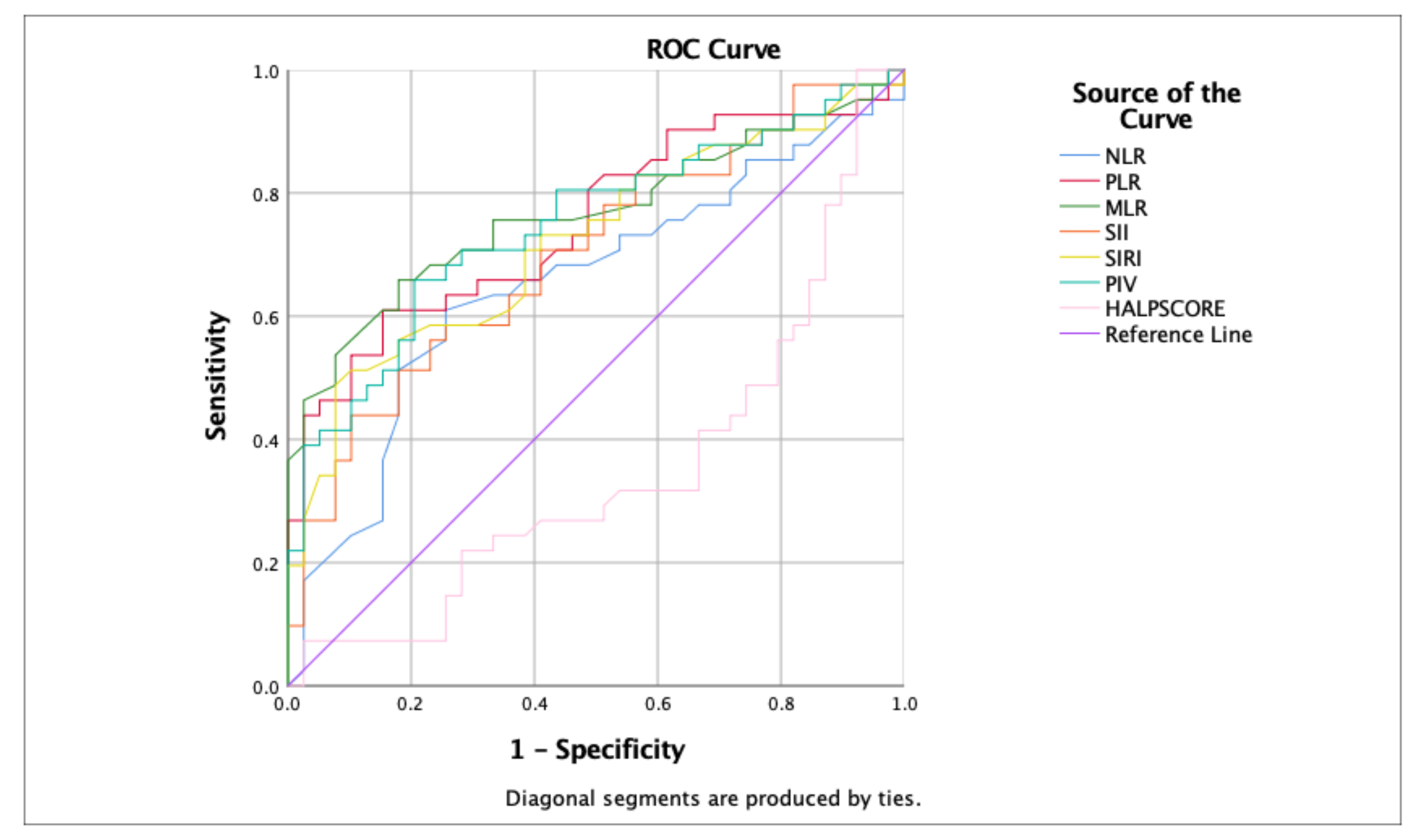
3.5. Predictive Value of Inflammatory Markers and HALP Score in HIE Patients
4. Discussion
4.1. Study Strengths
4.2. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- DeLaGarza-Pineda, O.; Mailo, J.A.; Boylan, G.; Chau, V.; Glass, H.C.; Mathur, A.M.; Shellhaas, R.A.; Soul, J.S.; Wusthoff, C.J.; Chang, T.; et al. (Eds.) Management of seizures in neonates with neonatal encephalopathy treated with hypothermia. In Seminars in Fetal and Neonatal Medicine; Elsevier: Amsterdam, The Netherlands, 2021. [Google Scholar]
- Kariholu, U.; Montaldo, P.; Markati, T.; Lally, P.J.; Pryce, R.; Teiserskas, J.; Liow, N.; Oliveira, V.; Soe, A.; Shankaran, S.; et al. Therapeutic hypothermia for mild neonatal encephalopathy: A systematic review and meta-analysis. Arch. Dis. Child. Fetal Neonatal Ed. 2020, 105, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Abate, B.B.; Bimerew, M.; Gebremichael, B.; Mengesha Kassie, A.; Kassaw, M.; Gebremeskel, T.; Alebachew Bayih, W. Effects of therapeutic hypothermia on death among asphyxiated neonates with hypoxic-ischemic encephalopathy: A systematic review and meta-analysis of randomized control trials. PLoS ONE 2021, 16, e0247229. [Google Scholar] [CrossRef] [PubMed]
- Victor, S.; Rocha-Ferreira, E.; Rahim, A.; Hagberg, H.; Edwards, D. New possibilities for neuroprotection in neonatal hypoxic-ischemic encephalopathy. Eur. J. Pediatr. 2022, 181, 875–887. [Google Scholar] [CrossRef]
- Mallard, C.; Tremblay, M.-E.; Vexler, Z.S. Microglia and neonatal brain injury. Neuroscience 2019, 405, 68–76. [Google Scholar] [CrossRef]
- Liu, F.; Mccullough, L.D. Inflammatory responses in hypoxic ischemic encephalopathy. Acta Pharmacol. Sin. 2013, 34, 1121–1130. [Google Scholar] [CrossRef] [PubMed]
- Jha, M.K.; Seo, M.; Kim, J.-H.; Kim, B.-G.; Cho, J.-Y.; Suk, K. The secretome signature of reactive glial cells and its pathological implications. Biochim. Biophys. Acta (BBA)-Proteins Proteom. 2013, 1834, 2418–2428. [Google Scholar] [CrossRef] [PubMed]
- Brombacher, T.; Berkiks, I.; Pillay, S.; Scibiorek, M.; Moses, B.; Brombacher, F. IL-4R alpha deficiency influences hippocampal-BDNF signaling pathway to impair reference memory. Sci. Rep. 2020, 10, 16506. [Google Scholar] [CrossRef]
- Hu, X.; Li, S.; Doycheva, D.M.; Huang, L.; Lenahan, C.; Liu, R.; Huang, J.; Xie, S.; Tang, J.; Zuo, G.; et al. Rh-CSF1 attenuates neuroinflammation via the CSF1R/PLCG2/PKCε pathway in a rat model of neonatal HIE. J. Neuroinflamm. 2020, 17, 1–18. [Google Scholar] [CrossRef]
- Riljak, V.; Kraf, J.; Daryanani, A.; Jiruška, P.; Otáhal, J. Pathophysiology of Perinatal Hypoxic-Ischemic Encephalopathy--Biomarkers, Animal Models and Treatment Perspectives. Physiol. Res. 2016, 65 (Suppl. S5), S533–S545. [Google Scholar] [CrossRef]
- Ceran, B.; Dizdar, E.A.; Beşer, E.; Karaçağlar, N.B.; Sarı, F.N. Diagnostic role of systemic inflammatory indices in infants with moderate-to-severe hypoxic ischemic encephalopathy. Am. J. Perinatol. 2021. Online ahead of print. [Google Scholar] [CrossRef]
- Zhai, B.; Chen, J.; Wu, J.; Yang, L.; Guo, X.; Shao, J.; Xu, H.; Shen, A. Predictive value of the hemoglobin, albumin, lymphocyte, and platelet (HALP) score and lymphocyte-to-monocyte ratio (LMR) in patients with non-small cell lung cancer after radical lung cancer surgery. Ann. Transl. Med. 2021, 9, 976. [Google Scholar] [CrossRef]
- Sarnat, H.B.; Flores-Sarnat, L.; Fajardo, C.; Leijser, L.M.; Wusthoff, C.; Mohammad, K. Sarnat grading scale for neonatal encephalopathy after 45 years: An update proposal. Pediatr. Neurol. 2020, 113, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Thompson, C.; Puterman, A.; Linley, L.; Hann, F.; Van der Elst, C.; Molteno, C.; Malan, A.F. The value of a scoring system for hypoxic ischaemic encephalopathy in predicting neurodevelopmental outcome. Acta Paediatr. 1997, 86, 757–761. [Google Scholar] [CrossRef] [PubMed]
- Cakir, U.; Tayman, C.; Tugcu, A.U.; Yildiz, D. Role of Systemic Inflammatory Indices in the Prediction of Moderate to Severe Bronchopulmonary Dysplasia in Preterm Infants. Arch. Bronconeumol. 2023, 59, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Mosalli, R. Whole body cooling for infants with hypoxic-ischemic encephalopathy. J. Clin. Neonatol. 2012, 1, 101–106. [Google Scholar] [CrossRef]
- Kawamura, N.; Schmeichel, A.M.; Wang, Y.; Schmelzer, J.D.; Low, P.A. Multiple effects of hypothermia on inflammatory response following ischemia–reperfusion injury in experimental ischemic neuropathy. Exp. Neurol. 2006, 202, 487–496. [Google Scholar] [CrossRef]
- Wang, G.; Deng, H.; Maier, C.; Sun, G.; Yenari, M. Mild hypothermia reduces ICAM-1 expression, neutrophil infiltration and microglia/monocyte accumulation following experimental stroke. Neuroscience 2002, 114, 1081–1090. [Google Scholar] [CrossRef] [PubMed]
- Yao, H.-W.; Kuan, C.-Y. Early neutrophil infiltration is critical for inflammation-sensitized hypoxic-ischemic brain injury in newborns. J. Cereb. Blood Flow Metab. 2020, 40, 2188–2200. [Google Scholar] [CrossRef]
- Lee, I.C.; Wong, S.H.; Wang, X.A.; Yu, C.S. Identifying early diagnostic biomarkers associated with neonatal hypoxic-ischemic encephalopathy. Diagnostics 2021, 11, 897. [Google Scholar] [CrossRef]
- Pimentel-Coelho, P.M. Monocytes in neonatal stroke and hypoxic-ischemic encephalopathy: Pathophysiological mechanisms and therapeutic possibilities. Neuroprotection 2023, 1, 20–33. [Google Scholar] [CrossRef]
- Marlow, N.; Shankaran, S.; Rogers, E.E.; Maitre, N.L.; Smyser, C.D.; Newborn Brain Society Guidelines and Publications Committee (Eds.) Neurological and developmental outcomes following neonatal encephalopathy treated with therapeutic hypothermia. In Seminars in Fetal and Neonatal Medicine; Elsevier: Amsterdam, The Netherlands, 2021. [Google Scholar]
- Chen, X.; Peng, W.; Zhang, Z.; Zhao, Q.; Zhou, Y.; Chen, L.; Pan, J. Efficacy and safety of selective brain hypothermia therapy on neonatal hypoxic-ischemic encephalopathy. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue 2018, 30, 1046–1050. [Google Scholar]
- Zhang, Y.; Lei, Y.; Jiang, H.; Li, X.; Feng, H. Analysis of the correlation between the severity of neonatal hypoxic ischemic encephalopathy and multiple organ dysfunction. Am. J. Transl. Res. 2022, 14, 311. [Google Scholar] [PubMed]
- Akdogan, M.; Ustundag, Y.; Cevik, S.G.; Dogan, P.; Dogan, N. Correlation between systemic immune-inflammation index and routine hemogram-related inflammatory markers in the prognosis of retinopathy of prematurity. Indian J. Ophthalmol. 2021, 69, 2182. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Liu, G.; Yang, X.; Liu, Q.; Li, Z. Effect of mild hypothermia on the expression of IL-10 and IL-18 in neonates with hypoxic ischemic encephalopathy. Exp. Ther. Med. 2019, 18, 2194–2198. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variable | HIE (n = 43) | Control (n = 50) | p-Value |
|---|---|---|---|
| Cesarean Section (C/S). n (%) | 27 (62.8%) | 39 (78.0%) | 0.117 |
| Female Gender. n (%) | 25 (58.1%) | 25 (50.0%) | 0.532 |
| Gestational Weeks (GW). mean ± sd | 38.19 ± 2.06 | 37.60 ± 1.65 | 0.132 |
| Birth Weight (BW). median. IQR | 3295.00. 2720.00–3565.00 | 3110.00. 2657.50–3445.00 | 0.339 |
| APGAR1 Score. median. IQR | 3.00. 1.00–4.75 | 8.00. 7.00–9.00 | <0.001 |
| APGAR5 Score. median. IQR | 5.00. 3.00–7.00 | 9.00. 8.00–10.00 | <0.001 |
| Cord Blood pH. mean ± sd | 6.82 ± 0.16 | 7.25 ± 0.09 | <0.001 |
| Base Deficit. median. IQR | −18.90. −23.80 to −17.00 | −5.00. −7.70 to −3.18 | <0.001 |
| Cord Blood Lactate. median. IQR | 16.00. 11.10–18.00 | 3.00. 2.45–4.35 | <0.001 |
| HIE (n = 43) | Control (n = 50) | ||||||
|---|---|---|---|---|---|---|---|
| Median | IQR | Median | IQR | p | |||
| Hb 0–6 | 17.00 | 15.60 | 18.10 | 18.90 | 17.08 | 19.83 | <0.001 |
| Hb 60–72 | 14.90 | 12.35 | 17.65 | 17.40 | 15.85 | 18.40 | 0.004 |
| Alb 0–6 | 3.50 | 3.05 | 3.90 | 3.70 | 3.50 | 3.90 | 0.163 |
| Alb 60–72 | 3.25 | 2.80 | 3.50 | 3.70 | 3.40 | 4.00 | <0.001 |
| Neu 0–6 | 11,100.00 | 7100.00 | 15,200.00 | 10,150.00 | 7300.00 | 14,500.00 | 0.844 |
| Neu 60–72 | 5500.00 | 3350.00 | 8650.00 | 5000.00 | 3850.00 | 7300.00 | 0.796 |
| L 0–6 | 5900.00 | 3900.00 | 9400.00 | 3800.00 | 3200.00 | 5375.00 | 0.001 |
| L 60–72 | 2300.00 | 1550.00 | 3250.00 | 3200.00 | 2850.00 | 4400.00 | 0.001 |
| M 0–6 | 1000.00 | 600.00 | 1800.00 | 1600.00 | 1100.00 | 2000.00 | 0.004 |
| M 60–72 | 400.00 | 200.00 | 800.00 | 1200.00 | 950.00 | 1450.00 | <0.001 |
| MPV 0–6 | 7.95 | 7.28 | 9.25 | 10.15 | 9.58 | 10.73 | <0.001 |
| MPV 60–72 | 8.30 | 7.55 | 9.95 | 10.40 | 9.70 | 11.10 | <0.001 |
| PLT 0–6 | 217,000.00 | 137,000.00 | 260,000.00 | 252,000.00 | 187,500.00 | 299,750.00 | 0.018 |
| PLT 60–72 | 141,000.00 | 68,500.00 | 187,500.00 | 248,000.00 | 175,000.00 | 322,500.00 | <0.001 |
| WBC 0–6 | 18,200.00 | 14,200.00 | 25,300.00 | 17,450.00 | 13,975.00 | 20,875.00 | 0.155 |
| WBC 60–72 | 10,100.00 | 6250.00 | 12,400.00 | 10,200.00 | 8500.00 | 12,850.00 | 0.245 |
| PLT index 0–6 | 1638.00 | 1132.20 | 2109.70 | 2539.80 | 2002.20 | 2967.50 | <0.001 |
| PLT index 60–72 | 1.099.80 | 681.60 | 1585.40 | 2551.10 | 1856.70 | 3351.75 | <0.001 |
| NLR 0–6 | 1.53 | 1.04 | 3.67 | 2.64 | 1.64 | 4.15 | 0.021 |
| NLR 60–72 | 2.79 | 1.47 | 4.85 | 1.68 | 1.21 | 2.10 | 0.002 |
| PLT/L 0–6 | 33.24 | 19.39 | 61.30 | 58.40 | 43.14 | 80.24 | <0.001 |
| PLT/L 60–72 | 51.00 | 41.51 | 91.52 | 64.59 | 50.17 | 94.22 | 0.108 |
| MLR 0–6 | 0.18 | 0.09 | 0.38 | 0.38 | 0.25 | 0.53 | <0.001 |
| MLR 60–72 | 0.22 | 0.09 | 0.40 | 0.33 | 0.29 | 0.39 | 0.021 |
| SII 0–6 | 331.02 | 161.17 | 592.00 | 548.68 | 361.20 | 1002.61 | 0.004 |
| SII 60–72 | 327.13 | 175.15 | 681.52 | 340.00 | 240.18 | 583.28 | 0.485 |
| PIV 0–6 | 351.54 | 111.31 | 729.64 | 816.93 | 531.11 | 1925.78 | <0.001 |
| PIV 60–72 | 124.03 | 36.43 | 461.54 | 462.04 | 230.16 | 607.67 | 0.001 |
| SIRI 0–6 | 1.69 | 0.69 | 4.66 | 3.82 | 2.00 | 6.84 | 0.001 |
| SIRI 60–72 | 0.85 | 0.42 | 2.76 | 1.89 | 1.27 | 2.62 | 0.062 |
| HALP score 0–6 | 181.09 | 96.94 | 283.01 | 112.96 | 75.86 | 173.71 | 0.02 |
| HALP score 60–72 | 99.39 | 51.15 | 138.61 | 95.62 | 69.22 | 132.67 | 0.382 |
| HIE (n = 43) | |||||||
|---|---|---|---|---|---|---|---|
| Parameter | 0–6 h | 60–72 h | |||||
| Median | IQR | Median | IQR | p | |||
| Hb (g/dL) | 17.00 | 15.60 | 18.10 | 14.90 | 12.35 | 17.65 | 0.003 |
| Alb (g/dL) | 3.50 | 3.05 | 3.90 | 3.25 | 2.80 | 3.50 | 0.005 |
| Neu (cells/μL) | 11,100.00 | 7100.00 | 15,200.00 | 5500.00 | 3350.00 | 8650.00 | <0.001 |
| L (cells/μL) | 5900.00 | 3900.00 | 9400.00 | 2300.00 | 1550.00 | 3250.00 | <0.001 |
| M (cells/μL) | 1000.00 | 600.00 | 1800.00 | 400.00 | 200.00 | 800.00 | <0.001 |
| MPV | 7.95 | 7.28 | 9.25 | 8.30 | 7.55 | 9.95 | 0.221 |
| PLT (cells/μL) | 217,000.00 | 137,000.00 | 26,000.00 | 141,000.00 | 68,500.00 | 187,500.00 | <0.001 |
| WBC (cells/μL) | 18,200.00 | 14,200.00 | 25,300.00 | 10,100.00 | 6250.00 | 12,400.00 | <0.001 |
| PLT Index | 1638.00 | 1132.20 | 2109.70 | 1099.80 | 681.60 | 1585.40 | <0.001 |
| NLR | 1.53 | 1.04 | 3.67 | 2.79 | 1.47 | 4.85 | 0.019 |
| PLT/L | 33.24 | 19.39 | 61.30 | 51.00 | 41.51 | 91.52 | 0.002 |
| MLR | 0.18 | 0.09 | 0.38 | 0.22 | 0.09 | 0.40 | 0.166 |
| SII | 331.02 | 161.17 | 592.00 | 327.13 | 175.15 | 681.52 | 0.908 |
| PIV | 351.54 | 111.31 | 729.64 | 124.03 | 36.43 | 461.54 | 0.048 |
| SIRI | 1.69 | 0.69 | 4.66 | 0.85 | 0.42 | 2.76 | 0.246 |
| HALP Score | 181.09 | 96.94 | 283.01 | 99.39 | 51.15 | 138.61 | <0.001 |
| HIE (n = 43) | |||
|---|---|---|---|
| Seizures | |||
| No (n = 21) | Yes (n = 22) | p | |
| Median (IQR) | Median (IQR) | ||
| PLT index 0–6 | 1743 (1122.25–2157.15) | 1511.6 (1126.58–2186.35) | 0.706 |
| PLT index 60–72 | 1099.8 (805.6–1630) | 1209.3 (613.55–1605.05) | 0.885 |
| NLR 0–6 | 1.74 (1.24–3.91) | 1.45 (0.74–3.21) | 0.325 |
| NLR 60–72 | 2.56 (1.46–4.07) | 3.52 (1.46–5.19) | 0.270 |
| PLT/LENF 0–6 | 49.25 (29.23–63.4) | 22.45 (14–50.01) | 0.055 |
| PLT/LENF 60–72 | 44.05 (42.19–65.68) | 55.42 (39.31–100.96) | 0.278 |
| MLR 0–6 | 0.23 (0.1–0.41) | 0.12 (0.09–0.23) | 0.142 |
| MLR6 0–72 | 0.16 (0.08–0.38) | 0.25 (0.1–0.47) | 0.406 |
| SII 0–6 | 473.12 (205.52–795.48) | 300.22 (130.82–507.11) | 0.285 |
| SII 60–72 | 257.39 (170.63–442.43) | 382.38 (173.3–725.32) | 0.406 |
| PIV 0–6 | 385.5 (113.56–1267.83) | 274.2 (100.21–665.48) | 0.528 |
| PIV 60–72 | 124.03 (34.13–216.73) | 213.66 (36.65–561.91) | 0.492 |
| SIRI 0–6 | 1.89 (0.72–5.52) | 1.31 (0.58–3.33) | 0.466 |
| SIRI 60–72 | 0.65 (0.4–1.58) | 1.46 (0.56–3.5) | 0.214 |
| HALP score 0–6 | 130.5 (85.94–200.65) | 251.85 (152.55–443.99) | 0.022 |
| HALP score 60–72 | 110.89 (72.23–173.51) | 58.68 (42.2–128.83) | 0.160 |
| IVH | |||
| No (n = 35) | Yes (n = 7) | p | |
| Median (IQR) | Median (IQR) | ||
| PLT index 0–6 | 1743 (1201.2–2512.3) | 1207.8 (908.8–2024) | 0.133 |
| PLT index 60–72 | 1138.2 (685.8–1563.1) | 1277.4 (414.15–1956.05) | 0.772 |
| NLR 0–6 | 1.49 (1.04–3.54) | 1.75 (0.77–6.94) | 0.353 |
| NLR 60–72 | 2.74 (1.38–4.19) | 4.25 (1.16–11.01) | 0.359 |
| PLT/LENF 0–6 | 33.24 (20.44–61.19) | 32.11 (9.04–118.13) | 0.933 |
| PLT/LENF 60–72 | 49.88 (40.32–91.2) | 73.84 (35.97–116.52) | 0.469 |
| MLR 0–6 | 0.18 (0.08–0.38) | 0.13 (0.11–0.23) | 0.826 |
| MLR 60–72 | 0.19 (0.09–0.39) | 0.27 (0.13–0.66) | 0.530 |
| SII 0–6 | 317.71 (161.17–569.25) | 362.67 (79.51–1311.19) | 0.853 |
| SII 60–72 | 269.69 (166.52–460.43) | 520.91 (142.23–1114.03) | 0.385 |
| PIV 0–6 | 385.5 (111.75–729.64) | 262.24 (42–544) | 0.489 |
| PIV 60–72 | 94.97 (35.53–325.08) | 377.52 (41.17–584.82) | 0.359 |
| SIRI 0–6 | 1.75 (0.69–4.66) | 1.39 (0.6–4.25) | 0.748 |
| SIRI 60–72 | 0.69 (0.37–1.81) | 2.89 (1–8.47) | 0.041 |
| HALPSCORE 012 | 168.03 (104.22–283.01) | 181.09 (49.17–589.54) | 0.735 |
| HALPSCORE 60–72 | 101.35 (53.15–148.13) | 81.55 (38.65–148.89) | 0.653 |
| PVL | |||
| No (n = 29) | Yes (n = 10) | p | |
| Median (IQR) | Median (IQR) | ||
| PLT index 0–6 | 1743 (1215.7–2367.7) | 1325.6 (973.08–2140.08) | 0.260 |
| PLT index 60–72 | 1138.2 (650.25–1810.35) | 1399.75 (494.25–1607.7) | 0.925 |
| NLR 0–6 | 1.69 (1.24–3.91) | 1.22 (0.73–3.46) | 0.288 |
| NLR 60–72 | 2.79 (1.48–4.6) | 2.62 (1.06–8.22) | 0.851 |
| PLT/LENF 0–6 | 49.25 (24.21–64.19) | 19.92 (11.45–40.65) | 0.022 |
| PLT/LENF 60–72 | 53.18 (40.26–100.96) | 46.03 (41.17–88.65) | 0.639 |
| MLR 0–6 | 0.18 (0.08–0.35) | 0.22 (0.13–0.47) | 0.234 |
| MLR 60–72 | 0.19 (0.09–0.35) | 0.27 (0.09–0.65) | 0.336 |
| SII 0–6 | 439.42 (206–795.48) | 289.42 (98.05–502.84) | 0.234 |
| SII 60–72 | 318.43 (177.66–538.61) | 253.4 (107.49–756.95) | 0.778 |
| PIV 0–6 | 309.79 (121.27–654.07) | 638.96 (105.45–940.54) | 0.260 |
| PIV 60–72 | 115.99 (35.53–325.08) | 280.15 (28.01–665.49) | 0.482 |
| SIRI 0–6 | 1.5 (0.59–3.96) | 2.78 (1–4.96) | 0.234 |
| SIRI 60–72 | 0.78 (0.4–2.08) | 1.1 (0.23–3.66) | 0.838 |
| HALP core 0–6 | 136.19 (84.4–238.98) | 327.32 (218.88–583.45) | 0.004 |
| HALP core 60–72 | 109.68 (47.21–135.54) | 88.22 (48.41–150.02) | 0.884 |
| Kidney Injury | |||
| No (n = 28) | Yes (n = 15) | ||
| Median (IQR) | Median (IQR) | p | |
| PLT index 0–6 | 230,000 (185,000–228,350) | 137,000 (117,000–218,000) | 0.006 |
| PLT index 60–72 | 169,500 (114,000–207,250) | 92,000 (50,000–139,500) | 0.013 |
| NLR 0–6 | 1.70 (1.25–4.27) | 1.20 (0.6–1.8) | 0.083 |
| NLR 60–72 | 2.45 (1.2–3.85) | 4.1 (2.7–6.25) | 0.022 |
| PLT/L 0–6 | 53.35 (23.85–64.62) | 20.8 (11.9–32.1) | 0.004 |
| PLT/L 60–72 | 58.7 (43.65–97.67) | 42.40 (33.80–69.15) | 0.173 |
| MLR 0–6 | 0.21 (0.1–0.40) | 0.11 (0.04–0.23) | 0.092 |
| MLR 60–72 | 0.19 (0.08–0.35) | 0.25 (0.13–0.63) | 0.217 |
| SII 0–6 | 475 (242–801) | 199 (79.5–334.6) | 0.012 |
| SII 60–72 | 304 (174–624) | 354 (159–717) | 0.941 |
| PIV 0–6 | 438 (226–821) | 111 (39.4–544) | 0.037 |
| PIV 60–72 | 125 (34.8–311) | 82 (42.5–625) | 0.73 |
| SIRI 0–6 | 2.25 (1.05–5.07) | 0.8 (0.3–4.3) | 0.12 |
| SIRI 60–72 | 0.8 (0.35–1.8) | 1.1 (0.5–7.3) | 0.126 |
| HALP score 0–6 | 124 (83.5–265) | 245 (200–566) | 0.003 |
| HALP score 60–72 | 109 (47.6–129) | 97.4 (52.8–148) | 0.985 |
| Marker | Cut-Off Value | Sensitivity | Specificity | Area under the Curve (AUC) | Lower 95% CI | Upper 95% CI | p |
|---|---|---|---|---|---|---|---|
| NLR | 2 | 0.634 | 0.641 | 0.654 | 0.532 | 0.776 | 0.018 |
| PLR | 54.75 | 0.659 | 0.643 | 0.751 | 0.644 | 0.859 | 0.001 |
| MLR | 0.305 | 0.707 | 0.718 | 0.766 | 0.659 | 0.873 | 0.001 |
| SII | 458.35 | 0.634 | 0.641 | 0.700 | 0.585 | 0.814 | 0.002 |
| SIRI | 2.7 | 0.634 | 0.615 | 0.722 | 0.61 | 0.834 | 0.001 |
| PIV | 603.5 | 0.707 | 0. 723 | 0.749 | 0.641 | 0.857 | 0.001 |
| HALP Score | 140.7 | 0.39 | 0.333 | 0.349 | 0.226 | 0.472 | 0.020 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toptan, H.H.; Tezel, K.G.; Tezel, O.; Ataç, Ö.; Vardar, G.; Gülcan Kersin, S.; Özek, E. Inflammatory and Hematologic Liver and Platelet (HALP) Scores in Hypothermia-Treated Hypoxic–Ischemic Encephalopathy (HIE). Children 2024, 11, 72. https://doi.org/10.3390/children11010072
Toptan HH, Tezel KG, Tezel O, Ataç Ö, Vardar G, Gülcan Kersin S, Özek E. Inflammatory and Hematologic Liver and Platelet (HALP) Scores in Hypothermia-Treated Hypoxic–Ischemic Encephalopathy (HIE). Children. 2024; 11(1):72. https://doi.org/10.3390/children11010072
Chicago/Turabian StyleToptan, Handan Hakyemez, Kübra Gökçe Tezel, Oğuzhan Tezel, Ömer Ataç, Gonca Vardar, Sinem Gülcan Kersin, and Eren Özek. 2024. "Inflammatory and Hematologic Liver and Platelet (HALP) Scores in Hypothermia-Treated Hypoxic–Ischemic Encephalopathy (HIE)" Children 11, no. 1: 72. https://doi.org/10.3390/children11010072
APA StyleToptan, H. H., Tezel, K. G., Tezel, O., Ataç, Ö., Vardar, G., Gülcan Kersin, S., & Özek, E. (2024). Inflammatory and Hematologic Liver and Platelet (HALP) Scores in Hypothermia-Treated Hypoxic–Ischemic Encephalopathy (HIE). Children, 11(1), 72. https://doi.org/10.3390/children11010072