
Parenting Styles and Psychosocial Factors of Mother–Child Dyads Participating in the ENDORSE Digital Weight Management Program for Children and Adolescents during the COVID-19 Pandemic

 , , , and
, , , and 
Abstract
1. Introduction
2. Methodology
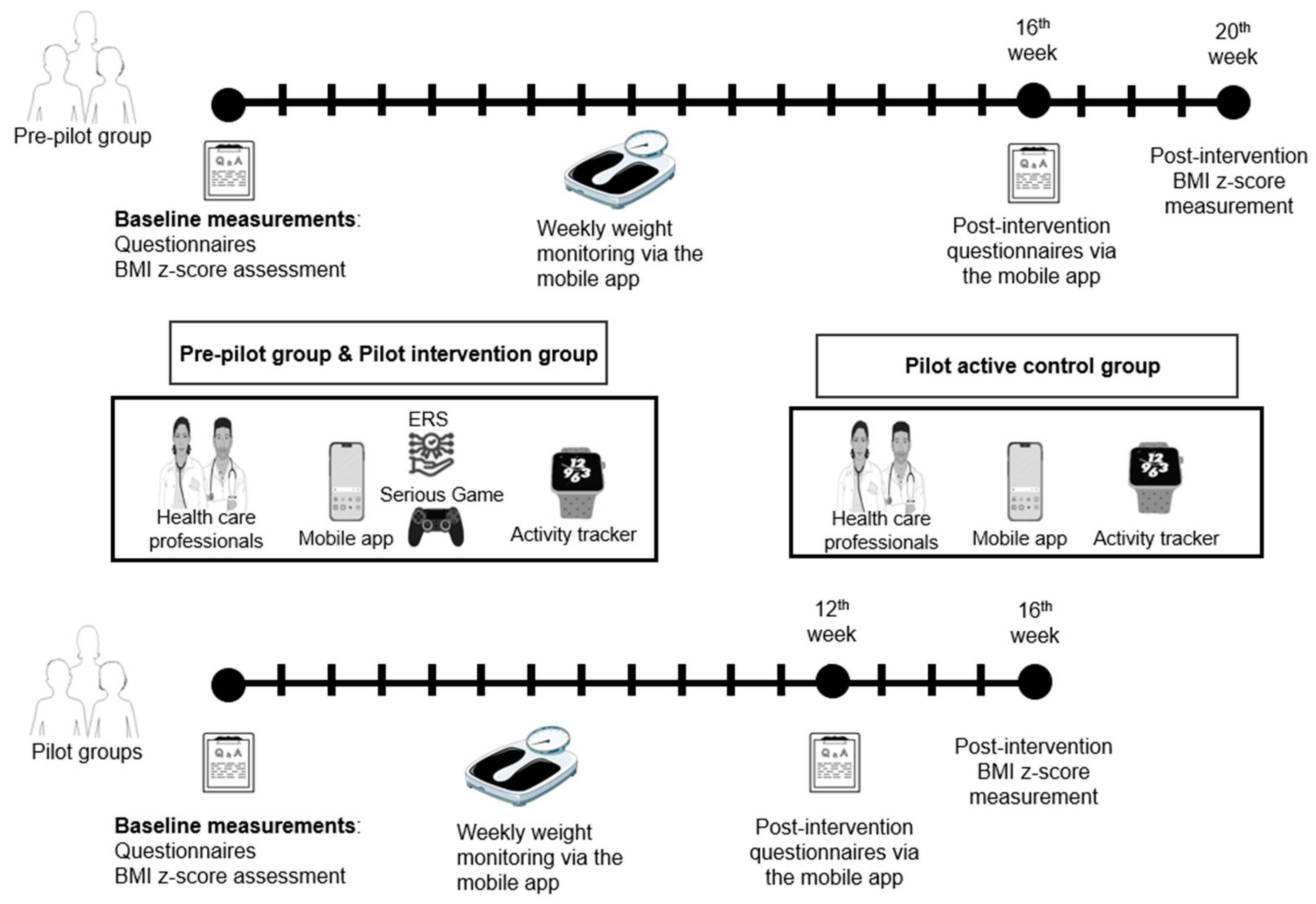
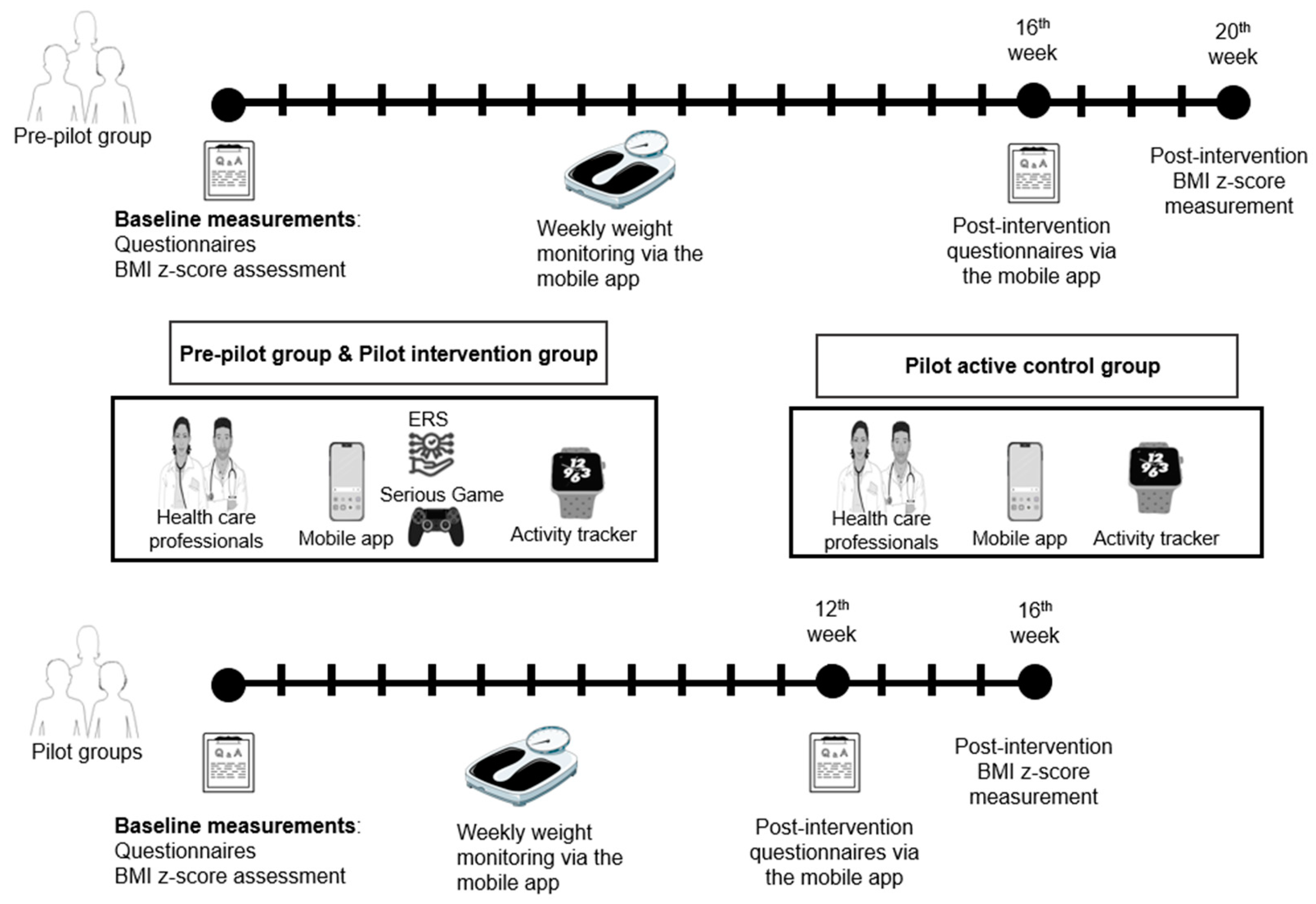
2.1. Study Design
2.2. Participants and Settings
2.3. Measures
2.3.1. Clinical and Nutritional Assessments
2.3.2. Psychological Assessment
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Changes in Parenting Styles
3.3. Changes in Psychosocial Functioning
3.4. Associations between Parenting Styles and BMI z-Scores
4. Discussion
5. Conclusions and Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hampl, S.E.; Hassink, S.G.; Skinner, A.C.; Armstrong, S.C.; Barlow, S.E.; Bolling, C.F.; Avila Edwards, K.C.; Eneli, I.; Hamre, R.; Joseph, M.M.; et al. Clinical Practice Guideline for the Evaluation and Treatment of Children and Adolescents with Obesity. Pediatrics 2023, 151, e2022060640. [Google Scholar] [CrossRef]
- Styne, D.M.; Arslanian, S.A.; Connor, E.L.; Farooqi, I.S.; Murad, M.H.; Silverstein, J.H.; Yanovski, J.A. Pediatric Obesity-Assessment, Treatment, and Prevention: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2017, 102, 709–757. [Google Scholar] [CrossRef] [PubMed]
- Kelly, A.S.; Marcus, M.D.; Yanovski, J.A.; Yanovski, S.Z.; Osganian, S.K. Working toward Precision Medicine Approaches to Treat Severe Obesity in Adolescents: Report of an NIH Workshop. Int. J. Obes. 2018, 42, 1834–1844. [Google Scholar] [CrossRef]
- Yanovski, S.Z.; Yanovski, J.A. Toward Precision Approaches for the Prevention and Treatment of Obesity. JAMA 2018, 319, 223–224. [Google Scholar] [CrossRef]
- World Obesity Atlas 2023. Available online: https://www.worldobesity.org/resources/resource-library/world-obesity-atlas-2023 (accessed on 18 May 2023).
- Bakaloudi, D.R.; Barazzoni, R.; Bischoff, S.C.; Breda, J.; Wickramasinghe, K.; Chourdakis, M. Impact of the First COVID-19 Lockdown on Body Weight: A Combined Systematic Review and a Meta-Analysis. Clin. Nutr. Edinb. Scotl. 2022, 41, 3046–3054. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Guo, B.; Ao, L.; Yang, C.; Zhang, L.; Zhou, J.; Jia, P. Obesity and Activity Patterns before and during COVID-19 Lockdown among Youths in China. Clin. Obes. 2020, 10, e12416. [Google Scholar] [CrossRef]
- Chang, T.-H.; Chen, Y.-C.; Chen, W.-Y.; Chen, C.-Y.; Hsu, W.-Y.; Chou, Y.; Chang, Y.-H. Weight Gain Associated with COVID-19 Lockdown in Children and Adolescents: A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 3668. [Google Scholar] [CrossRef] [PubMed]
- Jenssen, B.P.; Kelly, M.K.; Powell, M.; Bouchelle, Z.; Mayne, S.L.; Fiks, A.G. COVID-19 and Changes in Child Obesity. Pediatrics 2021, 147, e2021050123. [Google Scholar] [CrossRef]
- Woolford, S.J.; Sidell, M.; Li, X.; Else, V.; Young, D.R.; Resnicow, K.; Koebnick, C. Changes in Body Mass Index Among Children and Adolescents During the COVID-19 Pandemic. JAMA 2021, 326, 1434–1436. [Google Scholar] [CrossRef]
- Azrak, M.Á.; Fasano, M.V.; Avico, A.J.; Sala, M.; Casado, C.; Padula, M.; Kruger, A.L.; Malpeli, A.; Andreoli, M.F. Prolonged Body Weight Gain, Lifestyle Changes and Health-Related Quality of Life in Children during the COVID-19 Pandemic Lockdown: A Follow-up Study. Eur. J. Clin. Nutr. 2022, 77, 460–467. [Google Scholar] [CrossRef] [PubMed]
- Androutsos, O.; Perperidi, M.; Georgiou, C.; Chouliaras, G. Lifestyle Changes and Determinants of Children’s and Adolescents’ Body Weight Increase during the First COVID-19 Lockdown in Greece: The COV-EAT Study. Nutrients 2021, 13, 930. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Luo, B.; Zhao, L.; Liao, S. Influences of the COVID-19 Pandemic on Obesity and Weight-Related Behaviors among Chinese Children: A Multi-Center Longitudinal Study. Nutrients 2022, 14, 3744. [Google Scholar] [CrossRef] [PubMed]
- Neshteruk, C.D.; Zizzi, A.; Suarez, L.; Erickson, E.; Kraus, W.E.; Li, J.S.; Skinner, A.C.; Story, M.; Zucker, N.; Armstrong, S.C. Weight-Related Behaviors of Children with Obesity during the COVID-19 Pandemic. Child. Obes. Print 2021, 17, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Pietrobelli, A.; Pecoraro, L.; Ferruzzi, A.; Heo, M.; Faith, M.; Zoller, T.; Antoniazzi, F.; Piacentini, G.; Fearnbach, S.N.; Heymsfield, S.B. Effects of COVID-19 Lockdown on Lifestyle Behaviors in Children with Obesity Living in Verona, Italy: A Longitudinal Study. Obesity 2020, 28, 1382–1385. [Google Scholar] [CrossRef]
- Firth, J.; Solmi, M.; Wootton, R.E.; Vancampfort, D.; Schuch, F.B.; Hoare, E.; Gilbody, S.; Torous, J.; Teasdale, S.B.; Jackson, S.E.; et al. A Meta-Review of “Lifestyle Psychiatry”: The Role of Exercise, Smoking, Diet and Sleep in the Prevention and Treatment of Mental Disorders. World Psychiatry 2020, 19, 360–380. [Google Scholar] [CrossRef]
- Mental Health and Psychosocial Considerations during the COVID-19 Outbreak. Available online: https://www.who.int/publications-detail-redirect/WHO-2019-nCoV-MentalHealth-2020.1 (accessed on 18 May 2023).
- Nikolaidis, A.; Paksarian, D.; Alexander, L.; Derosa, J.; Dunn, J.; Nielson, D.M.; Droney, I.; Kang, M.; Douka, I.; Bromet, E.; et al. The Coronavirus Health and Impact Survey (CRISIS) Reveals Reproducible Correlates of Pandemic-Related Mood States across the Atlantic. Sci. Rep. 2021, 11, 8139. [Google Scholar] [CrossRef]
- Nikolaidis, A.; DeRosa, J.; Kass, M.; Droney, I.; Alexander, L.; Di Martino, A.; Bromet, E.; Merikangas, K.; Milham, M.P.; Paksarian, D. Heterogeneity in COVID-19 Pandemic-Induced Lifestyle Stressors Predicts Future Mental Health in Adults and Children in the US and UK. J. Psychiatr. Res. 2022, 147, 291–300. [Google Scholar] [CrossRef]
- Clinical Practice Guideline for the Treatment of Obesity and Overweight in Children and Adolescents. Available online: https://www.apa.org/obesity-guideline (accessed on 29 December 2022).
- Rankin, J.; Matthews, L.; Cobley, S.; Han, A.; Sanders, R.; Wiltshire, H.D.; Baker, J.S. Psychological Consequences of Childhood Obesity: Psychiatric Comorbidity and Prevention. Adolesc. Health Med. Ther. 2016, 7, 125–146. [Google Scholar] [CrossRef]
- Rao, W.-W.; Zong, Q.-Q.; Zhang, J.-W.; An, F.-R.; Jackson, T.; Ungvari, G.S.; Xiang, Y.; Su, Y.-Y.; D’Arcy, C.; Xiang, Y.-T. Obesity Increases the Risk of Depression in Children and Adolescents: Results from a Systematic Review and Meta-Analysis. J. Affect. Disord. 2020, 267, 78–85. [Google Scholar] [CrossRef]
- Pervanidou, P.; Chrousos, G.P. Emotional/Behavioral Disorders and Obesity in Childhood: A Clinician’s Perspective. Eur. Health Psychol. 2011, 13, 48–52. [Google Scholar]
- Pont, S.J.; Puhl, R.; Cook, S.R.; Slusser, W.; Section on Obesity; Obesity Society. Stigma Experienced by Children and Adolescents with Obesity. Pediatrics 2017, 140, e20173034. [Google Scholar] [CrossRef] [PubMed]
- Cheng, S.; Kaminga, A.C.; Liu, Q.; Wu, F.; Wang, Z.; Wang, X.; Liu, X. Association between Weight Status and Bullying Experiences among Children and Adolescents in Schools: An Updated Meta-Analysis. Child Abuse Negl. 2022, 134, 105833. [Google Scholar] [CrossRef]
- Schwimmer, J.B.; Burwinkle, T.M.; Varni, J.W. Health-Related Quality of Life of Severely Obese Children and Adolescents. JAMA 2003, 289, 1813–1819. [Google Scholar] [CrossRef] [PubMed]
- Halliday, J.A.; Palma, C.L.; Mellor, D.; Green, J.; Renzaho, A.M.N. The Relationship between Family Functioning and Child and Adolescent Overweight and Obesity: A Systematic Review. Int. J. Obes. 2014, 38, 480–493. [Google Scholar] [CrossRef]
- O’Connor, E.A.; Evans, C.V.; Burda, B.U.; Walsh, E.S.; Eder, M.; Lozano, P. Screening for Obesity and Intervention for Weight Management in Children and Adolescents: Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2017, 317, 2427–2444. [Google Scholar] [CrossRef] [PubMed]
- Fowler, L.A.; Grammer, A.C.; Staiano, A.E.; Fitzsimmons-Craft, E.E.; Chen, L.; Yaeger, L.H.; Wilfley, D.E. Harnessing Technological Solutions for Childhood Obesity Prevention and Treatment: A Systematic Review and Meta-Analysis of Current Applications. Int. J. Obes. 2021, 45, 957–981. [Google Scholar] [CrossRef]
- Kouvari, M.; Karipidou, M.; Tsiampalis, T.; Mamalaki, E.; Poulimeneas, D.; Bathrellou, E.; Panagiotakos, D.; Yannakoulia, M. Digital Health Interventions for Weight Management in Children and Adolescents: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2022, 24, e30675. [Google Scholar] [CrossRef]
- DeSilva, S.; Vaidya, S.S. The Application of Telemedicine to Pediatric Obesity: Lessons from the Past Decade. Telemed. J. e-Health 2021, 27, 159–166. [Google Scholar] [CrossRef]
- Park, J.; Park, M.-J.; Seo, Y.-G. Effectiveness of Information and Communication Technology on Obesity in Childhood and Adolescence: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2021, 23, e29003. [Google Scholar] [CrossRef]
- Gow, M.L.; Tee, M.S.Y.; Garnett, S.P.; Baur, L.A.; Aldwell, K.; Thomas, S.; Lister, N.B.; Paxton, S.J.; Jebeile, H. Pediatric Obesity Treatment, Self-Esteem, and Body Image: A Systematic Review with Meta-Analysis. Pediatr. Obes. 2020, 15, e12600. [Google Scholar] [CrossRef]
- Jebeile, H.; Gow, M.L.; Baur, L.A.; Garnett, S.P.; Paxton, S.J.; Lister, N.B. Association of Pediatric Obesity Treatment, Including a Dietary Component, With Change in Depression and Anxiety. JAMA Pediatr. 2019, 173, e192841. [Google Scholar] [CrossRef] [PubMed]
- Jebeile, H.; Gow, M.L.; Baur, L.A.; Garnett, S.P.; Paxton, S.J.; Lister, N.B. Treatment of Obesity, with a Dietary Component, and Eating Disorder Risk in Children and Adolescents: A Systematic Review with Meta-Analysis. Obes. Rev. 2019, 20, 1287–1298. [Google Scholar] [CrossRef]
- Darling, N.; Steinberg, L. Parenting Style as Context: An Integrative Model. Psychol. Bull. 1993, 113, 487–496. [Google Scholar] [CrossRef]
- Baumrind, D. Effects of Authoritative Parental Control on Child Behavior. Child Dev. 1966, 37, 887–907. [Google Scholar] [CrossRef]
- Maccoby, E.E.; Martin, J.A. Socialization in the Context of the Family: Parent-Child Interaction. In Handbook of Child Psychology; Mussen, P.H., Hetherington, E.M., Eds.; Wiley: New York, NY, USA, 1983. [Google Scholar]
- Balantekin, K.N.; Anzman-Frasca, S.; Francis, L.A.; Ventura, A.K.; Fisher, J.O.; Johnson, S.L. Positive Parenting Approaches and Their Association with Child Eating and Weight: A Narrative Review from Infancy to Adolescence. Pediatr. Obes. 2020, 15, e12722. [Google Scholar] [CrossRef]
- Sokol, R.L.; Qin, B.; Poti, J.M. Parenting Styles and Body Mass Index: A Systematic Review of Prospective Studies among Children. Obes. Rev. 2017, 18, 281–292. [Google Scholar] [CrossRef]
- Hughes, S.O.; Power, T.G.; Papaioannou, M.A.; Cross, M.B.; Nicklas, T.A.; Hall, S.K.; Shewchuk, R.M. Emotional Climate, Feeding Practices, and Feeding Styles: An Observational Analysis of the Dinner Meal in Head Start Families. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 60. [Google Scholar] [CrossRef]
- Hughes, S.O.; Power, T.G.; O’Connor, T.M.; Fisher, J.O.; Micheli, N.E.; Papaioannou, M.A. Maternal Feeding Style and Child Weight Status among Hispanic Families with Low-Income Levels: A Longitudinal Study of the Direction of Effects. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 30. [Google Scholar] [CrossRef]
- Shloim, N.; Edelson, L.R.; Martin, N.; Hetherington, M.M. Parenting Styles, Feeding Styles, Feeding Practices, and Weight Status in 4–12 Year-Old Children: A Systematic Review of the Literature. Front. Psychol. 2015, 6, 1849. [Google Scholar] [CrossRef]
- Ventura, A.K.; Birch, L.L. Does Parenting Affect Children’s Eating and Weight Status? Int. J. Behav. Nutr. Phys. Act. 2008, 5, 15. [Google Scholar] [CrossRef]
- Wrotniak, B.H.; Epstein, L.H.; Paluch, R.A.; Roemmich, J.N. The Relationship Between Parent and Child Self-Reported Adherence and Weight Loss. Obes. Res. 2005, 13, 1089–1096. [Google Scholar] [CrossRef] [PubMed]
- Wilfley, D.E.; Saelens, B.E.; Stein, R.I.; Best, J.R.; Kolko, R.P.; Schechtman, K.B.; Wallendorf, M.; Welch, R.R.; Perri, M.G.; Epstein, L.H. Dose, Content, and Mediators of Family-Based Treatment for Childhood Obesity: A Multisite Randomized Clinical Trial. JAMA Pediatr. 2017, 171, 1151–1159. [Google Scholar] [CrossRef]
- Epstein, L.H.; McKenzie, S.J.; Valoski, A.; Klein, K.R.; Wing, R.R. Effects of Mastery Criteria and Contingent Reinforcement for Family-Based Child Weight Control. Addict. Behav. 1994, 19, 135–145. [Google Scholar] [CrossRef] [PubMed]
- Gow, M.L.; Baur, L.A.; Ho, M.; Chisholm, K.; Noakes, M.; Cowell, C.T.; Garnett, S.P. Can Early Weight Loss, Eating Behaviors and Socioeconomic Factors Predict Successful Weight Loss at 12- and 24-Months in Adolescents with Obesity and Insulin Resistance Participating in a Randomised Controlled Trial? Int. J. Behav. Nutr. Phys. Act. 2016, 13, 43. [Google Scholar] [CrossRef] [PubMed]
- Sato, A.F.; Jelalian, E.; Hart, C.N.; Lloyd-Richardson, E.E.; Mehlenbeck, R.S.; Neill, M.; Wing, R.R. Associations between Parent Behavior and Adolescent Weight Control. J. Pediatr. Psychol. 2011, 36, 451–460. [Google Scholar] [CrossRef] [PubMed]
- Holland, J.C.; Kolko, R.P.; Stein, R.I.; Welch, R.R.; Perri, M.G.; Schechtman, K.B.; Saelens, B.E.; Epstein, L.H.; Wilfley, D.E. Modifications in Parent Feeding Practices and Child Diet during Family-Based Behavioral Treatment Improve Child zBMI. Obesity 2014, 22, E119–E126. [Google Scholar] [CrossRef] [PubMed]
- Stein, R.I.; Epstein, L.H.; Raynor, H.A.; Kilanowski, C.K.; Paluch, R.A. The Influence of Parenting Change on Pediatric Weight Control. Obes. Res. 2005, 13, 1749–1755. [Google Scholar] [CrossRef]
- Rhee, K.E.; Jelalian, E.; Boutelle, K.; Dickstein, S.; Seifer, R.; Wing, R. Warm Parenting Associated with Decreasing or Stable Child BMI during Treatment. Child. Obes. Print 2016, 12, 94–102. [Google Scholar] [CrossRef]
- Wilson, D.K.; Sweeney, A.M.; Quattlebaum, M.; Loncar, H.; Kipp, C.; Brown, A. The Moderating Effects of the Families Improving Together (FIT) for Weight Loss Intervention and Parenting Factors on Family Mealtime in Overweight and Obese African American Adolescents. Nutrients 2021, 13, 1745. [Google Scholar] [CrossRef]
- Pervanidou, P.; Chatzidaki, E.; Nicolaides, N.C.; Voutetakis, A.; Polychronaki, N.; Chioti, V.; Kitani, R.-A.; Kyrkopoulou, E.; Zarkogianni, K.; Kalafatis, E.; et al. The Impact of the ENDORSE Digital Weight Management Program on the Metabolic Profile of Children and Adolescents with Overweight and Obesity and on Food Parenting Practices. Nutrients 2023, 15, 1777. [Google Scholar] [CrossRef]
- Zarkogianni, K.; Chatzidaki, E.; Polychronaki, N.; Kalafatis, E.; Nicolaides, N.C.; Voutetakis, A.; Chioti, V.; Kitani, R.-A.; Mitsis, K.; Perakis, Κ.; et al. The ENDORSE Feasibility Study: Exploring the Use of M-Health, Artificial Intelligence and Serious Games for the Management of Childhood Obesity. Nutrients 2023, 15, 1451. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Self-Determination Theory and the Facilitation of Intrinsic Motivation, Social Development, and Well-Being. Am. Psychol. 2000, 55, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Di Pasquale, R.; Rivolta, A. A Conceptual Analysis of Food Parenting Practices in the Light of Self-Determination Theory: Relatedness-Enhancing, Competence-Enhancing and Autonomy-Enhancing Food Parenting Practices. Front. Psychol. 2018, 9, 2373. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a Standard Definition for Child Overweight and Obesity Worldwide: International Survey. BMJ 2000, 320, 1240–1243. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Lobstein, T. Extended International (IOTF) Body Mass Index Cut-Offs for Thinness, Overweight and Obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef]
- Kuczmarski, R.J.; Ogden, C.L.; Guo, S.S.; Grummer-Strawn, L.M.; Flegal, K.M.; Mei, Z.; Wei, R.; Curtin, L.R.; Roche, A.F.; Johnson, C.L. 2000 CDC Growth Charts for the United States: Methods and Development. Vital Health Stat. 2002, 11, 1–190. [Google Scholar]
- Freedman, D.S.; Berenson, G.S. Tracking of BMI z Scores for Severe Obesity. Pediatrics 2017, 140, e20171072. [Google Scholar] [CrossRef]
- Kastorini, C.-M.; Critselis, E.; Zota, D.; Coritsidis, A.L.; Nagarajan, M.K.; Papadimitriou, E.; Belogianni, K.; Benetou, V.; Linos, A. Greek National Dietary Guidelines Scientific Team National Dietary Guidelines of Greece for Children and Adolescents: A Tool for Promoting Healthy Eating Habits. Public Health Nutr. 2019, 22, 2688–2699. [Google Scholar] [CrossRef]
- Spear, B.A.; Barlow, S.E.; Ervin, C.; Ludwig, D.S.; Saelens, B.E.; Schetzina, K.E.; Taveras, E.M. Recommendations for Treatment of Child and Adolescent Overweight and Obesity. Pediatrics 2007, 120 (Suppl. S4), S254–S288. [Google Scholar] [CrossRef]
- Robinson, C.C.; Mandleco, B.; Olsen, S.F.; Hart, C.H. Authoritative, Authoritarian, and Permissive Parenting Practices: Development of a New Measure. Psychol. Rep. 1995, 77, 819. [Google Scholar] [CrossRef]
- Antonopoulou, K.; Tsitsas, G. An Exploration of Greek Mothers Parental Typology: Adaptation of Parenting Styles & Dimensions Questionnaire (PSDQ). Epistimes Agogis 2011, 2, 51–60. [Google Scholar]
- Goodman, R. The Strengths and Difficulties Questionnaire: A Research Note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef]
- Bibou-Nakou, I.; Kiosseoglou, G.; Stogiannidou, A. Strengths and Difficulties of School-Aged Children in the Family and School Context. Psychol. J. Hell. Psychol. Soc. 2001, 8, 506–525. [Google Scholar]
- Available online: https://www.sdqinfo.org/ (accessed on 4 April 2023).
- Kohn, J.S. Michael Sample Size for Before-after Study (Paired T-Test)|Sample Size Calculators. Available online: https://sample-size.net/sample-size-study-paired-t-test/ (accessed on 9 March 2023).
- Austin, P.C.; Steyerberg, E.W. The Number of Subjects per Variable Required in Linear Regression Analyses. J. Clin. Epidemiol. 2015, 68, 627–636. [Google Scholar] [CrossRef]
- Welcome to Python.Org. Available online: https://www.python.org/ (accessed on 20 November 2023).
- Harriger, J.A.; Thompson, J.K. Psychological Consequences of Obesity: Weight Bias and Body Image in Overweight and Obese Youth. Int. Rev. Psychiatry 2012, 24, 247–253. [Google Scholar] [CrossRef]
- Reiss, F. Socioeconomic Inequalities and Mental Health Problems in Children and Adolescents: A Systematic Review. Soc. Sci. Med. 1982 2013, 90, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Drukker, M.; Wojciechowski, F.; Feron, F.J.M.; Mengelers, R.; Van Os, J. A Community Study of Psychosocial Functioning and Weight in Young Children and Adolescents. Int. J. Pediatr. Obes. 2009, 4, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Boneberger, A.; von Kries, R.; Milde-Busch, A.; Bolte, G.; Rochat, M.K.; Rückinger, S.; GME Study Group. Association between Peer Relationship Problems and Childhood Overweight/Obesity. Acta Paediatr. 2009, 98, 1950–1955. [Google Scholar] [CrossRef]
- Maltezou, H.C.; Krumbholz, B.; Mavrouli, M.; Tseroni, M.; Gamaletsou, M.N.; Botsa, E.; Anastassopoulou, C.; Gikas, A.; Fournarakou, E.; Kavieri, M.; et al. A Study of the Evolution of the Third COVID-19 Pandemic Wave in the Athens Metropolitan Area, Greece, through Two Cross-Sectional Seroepidemiological Surveys: March, June 2021. J. Med. Virol. 2022, 94, 1465–1472. [Google Scholar] [CrossRef]
- Maltezou, H.C.; Basoulis, D.; Bonelis, K.; Gamaletsou, M.N.; Giannouchos, T.V.; Karantoni, E.; Karapanou, A.; Kounouklas, K.; Livanou, M.E.; Zotou, M.; et al. Effectiveness of Full (Booster) COVID-19 Vaccination against Severe Outcomes and Work Absenteeism in Hospitalized Patients with COVID-19 during the Delta and Omicron Waves in Greece. Vaccine 2023, 41, 2343–2348. [Google Scholar] [CrossRef]
- Theberath, M.; Bauer, D.; Chen, W.; Salinas, M.; Mohabbat, A.B.; Yang, J.; Chon, T.Y.; Bauer, B.A.; Wahner-Roedler, D.L. Effects of COVID-19 Pandemic on Mental Health of Children and Adolescents: A Systematic Review of Survey Studies. SAGE Open Med. 2022, 10, 20503121221086712. [Google Scholar] [CrossRef] [PubMed]
- Wilson, D.K.; Sweeney, A.M.; Van Horn, M.L.; Kitzman, H.; Law, L.H.; Loncar, H.; Kipp, C.; Brown, A.; Quattlebaum, M.; McDaniel, T.; et al. The Results of the Families Improving Together (FIT) for Weight Loss Randomized Trial in Overweight African American Adolescents. Ann. Behav. Med. Publ. Soc. Behav. Med. 2022, 56, 1042–1055. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristics | Total (n = 50) | Pre-Pilot Group (n = 20) | Pilot Group (n = 30) | p-Value (between Groups) |
|---|---|---|---|---|
| Age | 10.49 (1.99) | 10.94 (1.85) | 10.19 (2.05) | 0.193 |
| Sex: Female Male | 26 (52) 24 (48) | 8 (40) 12 (60) | 18 (60) 12 (40) | 0.248 |
| Pubertal stage: Prepubertal Pubertal | 21 (42) 29 (58) | 8 (40) 12 (60) | 13 (43.3) 17 (56.7) | 1.00 |
| Weight | 69.82 (22.53) | 76.94 (22.48) | 65.08 (21.64) | 0.068 |
| Height | 1.49 (0.13) | 1.51 (0.13) | 1.48 (0.14) | 0.349 |
| BMI | 30.65 (6.22) | 33.02 (6.51) | 29.06 (5.58) | 0.026 1 |
| BMI z-score | 2.85 (2.23, 4.07) | 2.85 (2.57, 4.38) | 2.79 (1.95, 3.47) | 0.104 |
| Weight Status: (IOTF criteria) [59] Overweight Simple obesity Severe obesity | 4 (8) 25 (50) 21 (42) | 0 11 (55) 9 (45) | 4 (13.3) 14 (46.7) 12 (40) | 0.234 |
| Weight stigma experience at school: 1 Yes No | 28 (56) 22 (44) | 11 (55) 9 (45) | 17 (56.7) 13 (43.3) | 1.00 |
| Body image concerns: 1 Yes No | 33 (66) 17 (34) | 12 (60) 8 (40) | 21 (70) 9 (30) | 0.548 |
| SDQ scales in scores: Total difficulties Emotional problems Conduct problems Hyperactivity Peer relationships Prosocial behavior | 10.66 (6.16) 3.10 (2.39) 2.62 (1.61) 3.42 (2.50) 1.52 (1.57) 8.82 (1.21) | 10.95 (6.24) 2.75 (2.15) 2.90 (1.83) 3.90 (2.79) 1.40 (1.39) 8.40 (1.27) | 10.47 (6.21) 3.33 (2.55) 2.43 (1.45) 3.10 (2.28) 1.60 (1.69) 9.10 (1.09) | 0.789 0.404 0.322 0.272 0.663 0.043 2 |
| Characteristics | Total (n = 50) | Pre-Pilot Group (n = 20) | Pilot Group (n = 30) | p-Value (between Groups) |
|---|---|---|---|---|
| Age | 43.90 (5.34) | 44.35 (5.08) | 43.6 (5.57) | 0.632 |
| BMI | 30.01 (6.07) | 30.71 (6.35) | 29.55 (5.94) | 0.514 |
| Ethnicity: Greek Albanian Romanian | 48 (96) 1 (2) 1 (2) | 19 (95) 0 1 (5) | 29 (96.7) 1 (3.3) 0 | 0.338 |
| Marital status: Married Single Divorced Widowed | 39 (78) 3 (6) 7 (14) 1 (2) | 14 (70) 1 (5) 4 (20) 1 (5) | 25 (83.3) 1 (3.3) 4 (13.3) 0 | 0.413 |
| Educational level: Primary Secondary Tertiary | 4 (8) 27 (54) 19 (38) | 3 (15) 12 (60) 5 (25) | 1 (3.3) 15 (50) 14 (46.7) | 0.154 |
| Occupation: Employed Unemployed | 39 (78) 11 (22) | 14 (70) 6 (30) | 25 (83.3) 5 (16.7) | 0.311 |
| Maternal annual income: EUR <10,000 EUR 10,000–20,000 EUR >200,000 Omission | 12 (24) 12 (24) 4 (8) 21 (42) | 7 (35) 7 (35) 1 (5) 5 (25) | 5 (16.7) 5 (16.7) 3 (10) 16 (53.3) | 0.113 |
| Parenting style (PSDQ): (5-point Likert scale) Authoritative Strict Permissive Authoritarian | 4.27 (0.47) 3.56 (0.55) 2.86 (0.77) 1.61 (0.58) | 4.28 (0.55) 3.46 (0.47) 2.81 (0.89) 1.57 (0.57) | 4.26 (0.42) 3.62 (0.59) 2.89 (0.70) 1.64 (0.60) | 0.924 0.334 0.735 0.681 |
| Family functioning: 1 No concerns Mother–child difficulties Sibling rivalry/teasing Multi-level difficulties (parents and siblings) | 26 (52) 11 (22) 8 (16) 5 (10) | 13 (65) 4 (20) 1 (5) 2 (10) | 13 (43.3) 7 (23.3) 7 (23.3) 3 (10) | 0.300 |
| Number of children: One child Two children Three children Four or five children | 11 (22) 30 (60) 4 (8) 5 (10) | 6 (30) 10 (50) 1 (5) 3 (15) | 5 (16.7) 20 (66.7) 3 (10) 2 (6.7) | 0.435 |
| Total (n = 43) | Pre-Pilot Group (n = 16) | Pilot Group (n = 27) | p-Value (between Groups) | |
|---|---|---|---|---|
| Authoritative | 0.02 (0.31) | 0.07 (0.22) | −0.003 (0.35) | 0.961 |
| Strict | −0.05 (0.38) | −0.06 (0.40) | −0.04 (0.36) | 0.513 |
| Permissive | 0.07 (0.61) | 0.06 (0.53) | 0.08 (0.66) | 0.140 |
| Authoritarian | −0.02 (0.36) | 0.05 (0.22) | −0.06 (0.42) | 0.060 |
| SDQ Scores | Total (n = 43) | Pre-Pilot Group (n = 16) | Pilot Group (n = 27) | p-Value (between Groups) |
|---|---|---|---|---|
| Total difficulties | 0.74 (4.76) | 0.19 (4.26) | 1.07 (5.08) | 0.553 |
| Emotional problems | 0.28 (2.13) | 0.06 (2.21) | 0.41 (2.12) | 0.838 |
| Conduct problems | 0.02 (1.16) | −0.69 1 (0.70) | 0.44 (1.19) | 0.002 2 |
| Hyperactivity/ inattention | 0.35 (2.06) | 0.69 (1.85) | 0.15 (2.18) | 0.407 |
| Peer problems | 0.33 (1.38) | 0.56 (1.46) | 0.19 (1.33) | 0.262 |
| Prosocial behavior | 0.12 (1.18) | 0.50 (1.10) | −0.11 (1.19) | 0.150 |
| Independent Variables | Dependent Variable: BMI z-Score Change (n = 41) | ||
|---|---|---|---|
| Beta | SE | p-Value | |
| Child age | 0.315 | 0.019 | 0.052 |
| Child sex | −0.014 | 0.074 | 0.924 |
| Child baseline BMI z-score | −0.010 | 0.027 | 0.946 |
| Maternal marital status | 0.274 | 0.080 | 0.044 |
| Maternal education | 0.331 | 0.076 | 0.033 |
| Baseline strict parenting style | −0.015 | 0.065 | 0.918 |
| Strict parenting style change | 0.468 | 0.098 | 0.003 |
| Group | 0.107 | 0.075 | 0.464 |
| Adherence | −0.307 | 0.071 | 0.032 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chatzidaki, E.; Chioti, V.; Mourtou, L.; Papavasileiou, G.; Kitani, R.-A.; Kalafatis, E.; Mitsis, K.; Athanasiou, M.; Zarkogianni, K.; Nikita, K.; et al. Parenting Styles and Psychosocial Factors of Mother–Child Dyads Participating in the ENDORSE Digital Weight Management Program for Children and Adolescents during the COVID-19 Pandemic. Children 2024, 11, 107. https://doi.org/10.3390/children11010107
Chatzidaki E, Chioti V, Mourtou L, Papavasileiou G, Kitani R-A, Kalafatis E, Mitsis K, Athanasiou M, Zarkogianni K, Nikita K, et al. Parenting Styles and Psychosocial Factors of Mother–Child Dyads Participating in the ENDORSE Digital Weight Management Program for Children and Adolescents during the COVID-19 Pandemic. Children. 2024; 11(1):107. https://doi.org/10.3390/children11010107
Chicago/Turabian StyleChatzidaki, Evi, Vassiliki Chioti, Lidia Mourtou, Georgia Papavasileiou, Rosa-Anna Kitani, Eleftherios Kalafatis, Kostas Mitsis, Maria Athanasiou, Konstantia Zarkogianni, Konstantina Nikita, and et al. 2024. "Parenting Styles and Psychosocial Factors of Mother–Child Dyads Participating in the ENDORSE Digital Weight Management Program for Children and Adolescents during the COVID-19 Pandemic" Children 11, no. 1: 107. https://doi.org/10.3390/children11010107
APA StyleChatzidaki, E., Chioti, V., Mourtou, L., Papavasileiou, G., Kitani, R.-A., Kalafatis, E., Mitsis, K., Athanasiou, M., Zarkogianni, K., Nikita, K., Kanaka-Gantenbein, C., & Pervanidou, P. (2024). Parenting Styles and Psychosocial Factors of Mother–Child Dyads Participating in the ENDORSE Digital Weight Management Program for Children and Adolescents during the COVID-19 Pandemic. Children, 11(1), 107. https://doi.org/10.3390/children11010107